On This Page – Quick Medical Summary
If you have seen a map ranking the “worst states” for prostate cancer and wondered whether your address puts you at risk, the honest answer is reassuring: where you live matters far less than who you are. Prostate cancer risk is shaped mostly by age, race, and family history — not by state lines.
This guide is built for three readers. If a state ranking alarmed you, Section 2 gives the verified numbers and Section 3 explains why they are easy to misread. If you are a Black man or have a father or brother with prostate cancer, Sections 4 and 5 cover what genuinely raises your risk. If you are deciding whether to get screened, Sections 6 and 7 walk through your next step.
Prostate cancer is the most common cancer in men in the United States other than skin cancer, and about 1 in 8 men will be diagnosed during their lifetime. Knowing your real risk profile is how you act on it.
ℹ️ Medical Disclaimer: This article explains prostate cancer risk patterns, screening guidance, and genetic risk factors for general education only. It does not diagnose disease, recommend treatment, or replace individualized screening decisions. Decisions about PSA testing, genetic testing, and your personal screening schedule should be made with a board-certified urologist or your primary care physician, who can weigh your age, race, family history, and overall health.
Which US states have the highest prostate cancer rates?
The states with the highest prostate cancer death rates are Washington, D.C. and Mississippi. Mortality rate — deaths per 100,000 men — is the most reliable way to compare states, because it reflects real outcomes rather than how aggressively a state screens.
📊 Clinical Data Point: Washington, D.C. (27.5 deaths per 100,000 men) and Mississippi (24.8) have the highest prostate cancer mortality in the country — Source: American Cancer Society, Prostate Cancer Statistics 2025.
A separate CDC analysis using 2018–2022 data ranks the 50 states slightly differently, with Mississippi highest nationally.
| State | Death rate (per 100,000 men) | How it compares to the U.S. average |
|---|---|---|
| Mississippi | 24.2 | ~25% above average |
| Vermont | 21.9 | ~13% above average |
| Utah | 21.8 | ~13% above average |
| Alaska | 21.5 | ~11% above average |
Source: CDC mortality data, 2018–2022; the U.S. average is about 19.3 deaths per 100,000 men. The ACS 2025 report, using mortality data through 2023, ranks Washington, D.C. highest (27.5), followed by Mississippi (24.8).
Incidence rate — new cases per 100,000 — tells a different story. In 2022, Louisiana had the highest prostate cancer incidence rate at 157 cases per 100,000, per CDC data. Nationally, the ACS estimated about 313,780 new cases and 35,770 deaths in 2025. For the wider picture, see our overview of prostate cancer statistics and trends.
Why incidence and mortality tell different state stories
Living in a “high-incidence” state does not mean your personal risk is high. Much of the variation between states reflects how often men get PSA testing, not how often the disease truly occurs.
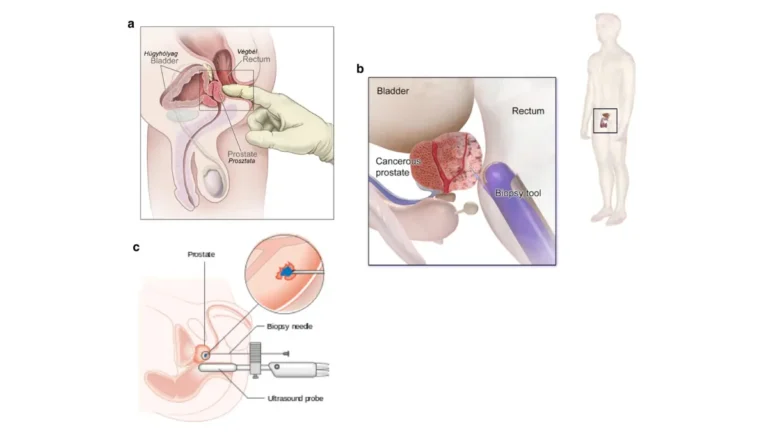
🔬 How It Works: A prostate cancer case is only counted when it is found. States and eras that screen more men with the PSA blood test detect more cancers — including many slow-growing ones that would never have caused harm. When PSA screening patterns shifted, U.S. diagnoses declined sharply from 2007 to 2014, then incidence rose about 3% per year from 2014 through 2022. The true cancer rate did not swing that much; the detection rate did.
Mortality is harder to distort, which is why it better reflects true burden. The clearest example is Washington, D.C.: it has the highest overall prostate cancer mortality yet ranks 37th in incidence, with Black men there having the second-highest mortality rate of any state (45.0 per 100,000) while White men have the lowest (10.7). The same place sends opposite signals depending on who is counted.
This matters because most prostate cancers grow slowly, and the majority of men diagnosed do not die from the disease. A high case count is not the same as a high chance of dying. That distinction also shapes how to read prostate cancer survival rates, which you can explore further in the linked guide. The CDC’s U.S. Cancer Statistics prostate data breaks these patterns down in detail.
What actually drives prostate cancer risk
The strongest drivers of prostate cancer risk are not geographic. In rough order of impact, they are age, race and ethnicity, and family history or inherited genes.
- Age is the single biggest factor. About 6 in 10 prostate cancers are diagnosed in men 65 or older, and the disease is rare before age 40.
- Race and ethnicity matter substantially. Black men have about 67% higher incidence than White men, while the disease is less common in Asian American and Pacific Islander men.
- Family history roughly doubles risk. Having a father or brother with prostate cancer more than doubles a man’s risk.
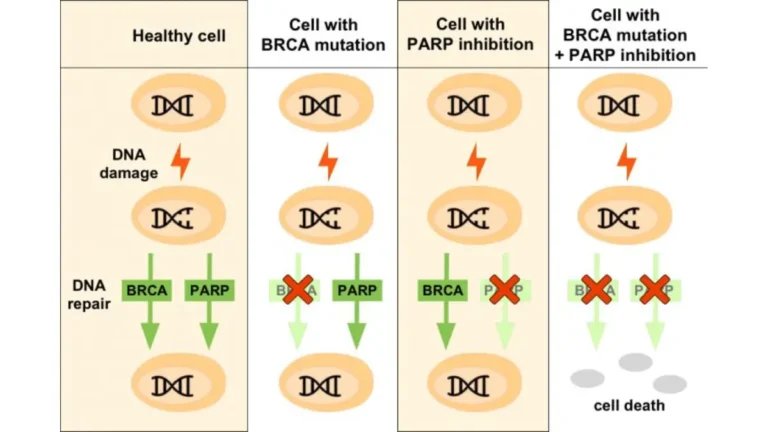
- Inherited gene changes, especially BRCA2, raise risk sharply.
🔬 How It Works: BRCA2 is a gene that helps repair damaged DNA. When it carries a harmful change, cells accumulate more genetic errors, raising cancer risk. Men with a BRCA2 variant have roughly a threefold to sevenfold increased risk of prostate cancer, and these cancers appear more aggressive than typical cases.
📊 Clinical Data Point: About 19% to 61% of men with a harmful BRCA2 change develop prostate cancer by age 80, versus about 10.6% of men in the general population — Source: National Cancer Institute.
✅ Patient Action: If a close relative had prostate, breast, ovarian, or pancreatic cancer, ask a genetic counselor whether testing for BRCA2 and related genes is appropriate for you.
For the complete picture, see the full list of prostate cancer risk factors and our guide to genetic testing for BRCA and prostate cancer. National baseline rates are tracked by the NCI’s SEER program, and the NCI’s BRCA fact sheet covers inherited risk in depth.
How race and demographics explain the state gap
The state-level differences you saw earlier are largely a reflection of who lives in each state and the care they can access — not a hazard built into the geography itself.
The states with the highest prostate cancer mortality, including D.C. and Mississippi, have large Black populations, and the disparity is real and serious. Black men have about double the prostate cancer mortality of White men — 36.9 versus 18.4 deaths per 100,000 — despite incidence being about 67% higher. Native American men have about 12% higher mortality than White men despite 13% lower incidence, a sign that outcomes, not just case counts, drive the gap.
🩺 Physician Note: Researchers attribute these disparities to a mix of factors — differences in access to screening and treatment, socioeconomic conditions, later-stage diagnosis, and some genetic differences in risk. Current understanding frames disparity as a reflection of circumstances and access, not an individual’s destiny.
For an individual reader, the takeaway is empowering rather than frightening: if you are in a higher-risk group, earlier screening conversations are the lever that most improves outcomes. Our dedicated guide covers prostate cancer risk in Black men in more depth.
✅ Patient Action: If you are Black or have a family history, ask your primary care physician about beginning PSA screening discussions at age 45 rather than 50.
How to assess your own prostate cancer risk
You can build a clear picture of your own risk in three steps, before any appointment.
- Map your family history. Note any father, brother, or son with prostate cancer, and any relatives with breast, ovarian, or pancreatic cancer, which can signal an inherited risk gene. The age at their diagnosis matters; younger ages raise your risk more.
- Identify your risk-based starting age. Average-risk men typically discuss screening at 50; Black men and those with a close relative diagnosed before 65 at 45; men with more than one such relative at 40.
- Decide whether genetic counseling fits. A strong family history, or a known BRCA2 mutation in the family, is a reason to ask about genetic testing.
✅ Patient Action: Before your visit, write down which relatives had which cancers and at what ages, and bring that list to your primary care physician or urologist.
To estimate where you stand, you can estimate your personal risk profile with our risk tool, and review how PSA levels are interpreted by age. You can also look up your own state’s and county’s prostate cancer rates through the National Cancer Institute’s State Cancer Profiles tool.
When to talk to your doctor about screening
The right time to start prostate cancer screening depends on your risk group, and the American Cancer Society frames it as a conversation with your provider — not an automatic test.
The ACS recommends starting that discussion at:
- Age 50 for men at average risk with at least a 10-year life expectancy.
- Age 45 for men at high risk — African American men, or those with a father or brother diagnosed before age 65.
- Age 40 for men at even higher risk, with more than one first-degree relative diagnosed with prostate cancer at an early age.
⚠️ Clinical Warning: Screening carries real benefits and real harms. The decision should be made after getting information about the possible benefits, risks, and uncertainties of screening, because a PSA test can flag slow-growing cancers that never needed treatment. Men with less than a 10-year life expectancy are generally not offered screening, because they aren’t likely to benefit.
Your state’s ranking should not drive this decision; your age, race, and family history should. For more, see our guide to prostate cancer screening by age and the American Cancer Society’s prostate cancer screening recommendations.
✅ Patient Action: Ask your primary care physician or a urologist directly: “Given my age, race, and family history, should I start PSA screening now, and how often?”
Frequently asked questions about prostate cancer risk by state
1. Which US state has the highest prostate cancer death rate?
Washington, D.C. has the highest prostate cancer death rate at 27.5 deaths per 100,000 men, followed by Mississippi at 24.8, according to the American Cancer Society’s 2025 report. A separate CDC analysis of 2018–2022 data ranked Mississippi highest among the 50 states. Both reflect states with large Black populations.
2. Does living in a certain state increase prostate cancer risk?
Largely, no. State rankings mostly reflect how often men are screened and the demographic makeup of each state, not a geographic hazard. Your prostate cancer risk by state matters far less than your age, race, and family history. Where you live can affect access to screening and care, but it does not change your biology.
3. Why do some states have higher prostate cancer mortality?
States with higher prostate cancer mortality tend to have larger Black populations and more barriers to early screening and treatment. Researchers link these differences to access to care, socioeconomic conditions, and later-stage diagnosis rather than geography itself. Outcomes — not just how many cancers are found — drive the gap between states.
4. Are Black men at higher risk of prostate cancer?
Yes. Black men have about 67% higher prostate cancer incidence than White men and roughly double the mortality (36.9 versus 18.4 deaths per 100,000). Because of this, guidelines suggest earlier screening discussions. If you are Black, ask your primary care physician about starting PSA screening conversations at age 45 rather than 50.
5. At what age should men start prostate cancer screening?
The American Cancer Society recommends discussing screening at age 50 for average-risk men, age 45 for high-risk men (Black men, or those with a father or brother diagnosed before 65), and age 40 for those with more than one such relative. Discuss your specific timing and frequency with your primary care physician or urologist.
6. Does family history affect prostate cancer risk?
Yes. Having a father or brother with prostate cancer more than doubles your risk, and breast, ovarian, or pancreatic cancer in the family can signal an inherited risk gene. The age at diagnosis matters — younger ages raise risk more. Share your full family history with your doctor to guide screening decisions.
7. Does a BRCA2 mutation increase prostate cancer risk?
Yes, substantially. Men with a harmful BRCA2 mutation have roughly a threefold to sevenfold higher prostate cancer risk, and these cancers tend to be more aggressive. An estimated 19% to 61% of BRCA2 carriers develop prostate cancer by age 80. If BRCA2 runs in your family, ask a genetic counselor whether testing is right for you.
8. Is prostate cancer incidence the same as prostate cancer risk?
No. Incidence counts how many cancers are diagnosed, which depends heavily on how many men get PSA testing. A state can have high incidence simply because it screens aggressively, detecting many slow-growing cancers. Mortality — the death rate — is a more reliable measure of true prostate cancer burden than incidence alone.
9. Which state has the highest prostate cancer incidence rate?
In 2022, Louisiana had the highest prostate cancer incidence rate at 157 new cases per 100,000 men, according to CDC data. High incidence reflects both real cases and how often men are screened, so a top incidence ranking does not necessarily mean men in that state face the highest true risk.
10. How common is prostate cancer in the US?
Prostate cancer is the most common cancer in American men other than skin cancer. About 1 in 8 men will be diagnosed in their lifetime, and the ACS estimated about 313,780 new cases and 35,770 deaths in 2025. Most men diagnosed do not die from it, as many cases grow slowly.
11. Can I look up prostate cancer rates for my own state?
Yes. The National Cancer Institute’s State Cancer Profiles tool lets you view prostate cancer incidence and mortality rates by state and county. Remember that a state’s rate describes its population, not your individual risk — your age, race, and family history are far more telling for your own prostate cancer risk by state.
The bottom line on prostate cancer risk by state
State rankings make compelling headlines, but they describe populations, not people. The data show that prostate cancer mortality clusters in states like D.C. and Mississippi largely because of demographics and access to care — while the factors that actually shape your personal risk are your age, your race, and your family history.
That is genuinely good news, because those factors point to a clear, controllable next step. Know your family history, learn your risk-based screening age, and have the screening conversation with your doctor at the right time for you.
Your zip code is not your destiny. Your risk profile — and what you do about it — is what counts.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.