On This Page – Quick Medical Summary
A colonoscopy is the test most people dread and least understand, and that gap is where avoidable mistakes happen. This guide closes it: what the test is for, how to get through the prep, what every result means, what it should cost, and which of the six screening options actually fits your situation.
If you just turned 45 and aren’t sure what to do
Screening for colorectal cancer now starts at age 45 for average-risk adults, not 50 — the recommendation changed in 2021. A colonoscopy is one of several valid options, not the only one. The section below on which test you need lays out the trade-offs before you commit to anything.
If your colonoscopy is already scheduled
The preparation is the hard part, and most of the fear comes from not knowing what to expect. Move ahead to the prep walkthrough and the section on what actually happens during the procedure. Both are written to make an unfamiliar day feel predictable.
If you’re worried about the cost
A screening colonoscopy is usually covered with no out-of-pocket cost for average-risk adults — but a “free” screening can still produce a bill in specific, avoidable situations. The cost section explains exactly when that happens and how to prevent it.
If you have symptoms or a family history right now
If you’re having rectal bleeding, a lasting change in bowel habits, or unexplained weight loss, this is not routine screening — call a doctor. The symptoms section explains why, and the higher-risk section covers what changes if colorectal cancer runs in your family.
Here is what this guide does that most others don’t. It corrects the screening age that many pages still get wrong. It compares every test honestly, including how well each one catches precancerous growths rather than only established cancer. It walks through the prep and the results without alarm, and it explains the cost rules plainly, because fear of an unexpected bill keeps people from a test that prevents one of the most preventable cancers there is.
Every number here is tied to a named source you can check — the FDA, CDC, the National Cancer Institute, the U.S. Preventive Services Task Force, the American Cancer Society, and the US Multi-Society Task Force. Where a figure is genuinely uncertain or varies between studies, this guide says so rather than inventing false precision. That honesty is the point: a screening decision deserves accurate information, not confident guesswork.
You do not need to read all of this. Use the routing above to jump to what you need today, and come back to the rest when it matters.
ℹ️ Medical Disclaimer: This guide explains colorectal cancer screening decisions, the colonoscopy procedure and its risks, bowel preparation and pre-procedure medication adjustments, sedation, how results and polyp findings are interpreted, and insurance and billing rules. It is general education, not personal medical or financial advice. Your own situation depends on your age, health history, medications, family history, and your clinician’s and insurer’s guidance — talk with a board-certified gastroenterologist or your primary care clinician before acting on anything here.
What a colonoscopy is and why doctors recommend it
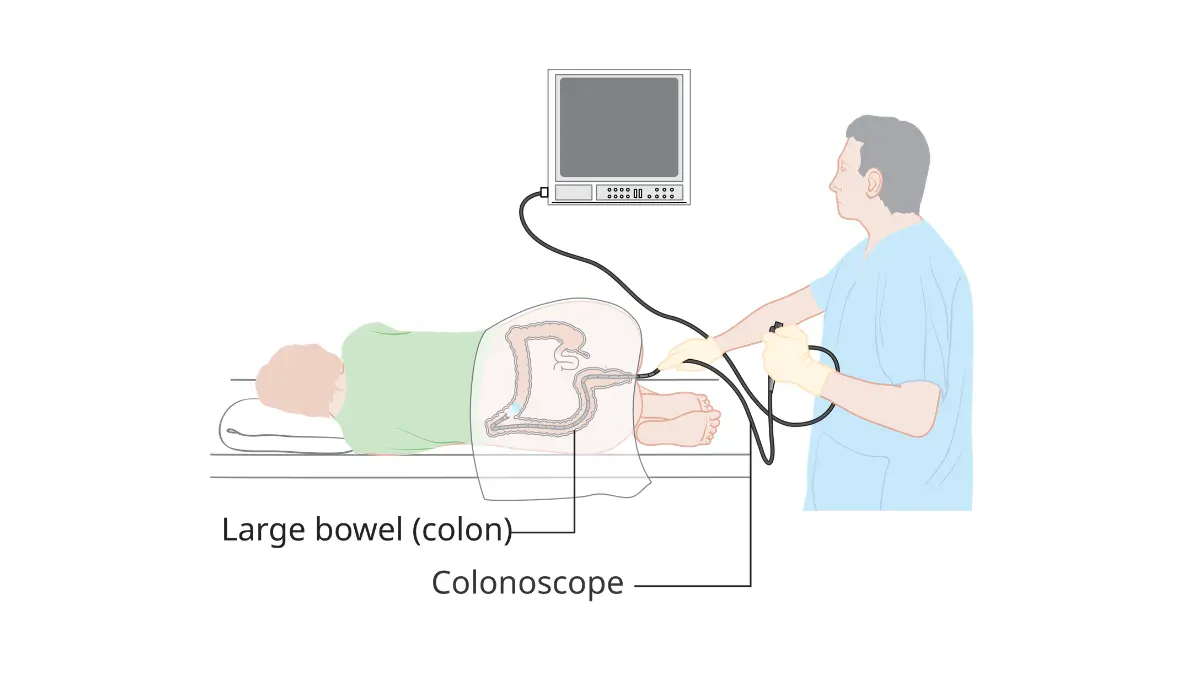
A colonoscopy is an exam that lets a doctor look at the entire lining of your large intestine using a thin, flexible tube with a camera on the end. It can find and remove polyps — small growths that can slowly turn into cancer — during the same procedure. That ability to both detect and prevent is what sets it apart from most other tests.
The scope enters through the rectum and is guided through the full length of the colon. As the doctor slowly withdraws it, they examine the lining for polyps, inflammation, and other changes. If a polyp is found, it is usually removed on the spot in a step called a polypectomy, then sent to a lab.
What the procedure actually examines
The colon and rectum together form the last several feet of the digestive tract. A colonoscopy is the only routine screening test that views all of it directly, which is why it can catch growths in parts of the colon that shorter or indirect tests miss. The National Cancer Institute’s overview of how each screening test finds cancer and polyps explains why some tests can prevent cancer, not just detect it.
🔬 How It Works: Most colorectal cancers begin as a benign growth called an adenoma. Over a span that often runs 10 to 15 years in an average-risk person, a small fraction of these adenomas accumulate genetic changes that can make them cancerous. A colonoscopy interrupts that timeline — when the polyp is removed before it transforms, the cancer it might have become never develops.
Why it’s considered the gold-standard test
A colonoscopy is the most sensitive of the screening options, and it is the only one that finds and removes precancerous polyps in a single visit. It also has the longest interval between tests: a normal result for an average-risk adult means the next colonoscopy is typically 10 years away. No other screening test combines that completeness with that durability.
That does not make it the right test for everyone, and the other options have real advantages in cost, convenience, and avoiding sedation. The point is that colonoscopy is the reference standard the others are measured against, not that it is automatically the best choice for you.
Screening vs. diagnostic colonoscopy — an important difference
This distinction sounds technical, but it affects both your care and your bill. A screening colonoscopy is done for an average-risk adult with no symptoms, on a routine schedule. A diagnostic colonoscopy is done because something prompted it — symptoms like bleeding, or a positive result from a stool or blood test.
The two are the same procedure but are coded and covered differently, which is why the same exam can be free in one situation and generate a bill in another. Hold on to that difference; the cost section returns to it in detail, because it is the single most common reason people are surprised by a charge.
Symptoms that mean you should call a doctor now
Some symptoms shouldn’t wait for routine screening. If you notice any of the following, contact a doctor promptly rather than scheduling a standard screening down the road:
- Blood in your stool or rectal bleeding, whether bright red or dark and tarry
- A change in bowel habits — diarrhea, constipation, or narrower stools — lasting more than a few weeks
- Unexplained weight loss
- Persistent abdominal pain, cramping, or bloating
- A feeling that your bowel doesn’t empty completely
- Fatigue or iron-deficiency anemia found on a blood test
Most of these symptoms have causes far more common and less serious than cancer — hemorrhoids, infections, dietary changes, and inflammatory conditions among them. But they all deserve evaluation, because the only way to know what’s causing them is to be seen.
⚠️ Clinical Warning: Do not try to diagnose rectal bleeding yourself, and do not assume it’s “just hemorrhoids” because you’ve had them before. Bleeding has overlapping causes that look identical from the outside, and a brief evaluation is the only way to separate the harmless from the serious.
Why symptoms mean a diagnostic — not screening — colonoscopy
If you have symptoms, a colonoscopy done to investigate them is diagnostic, not screening. That changes nothing about the procedure itself, but it changes how it’s classified, and it changes the urgency: a symptom-driven evaluation shouldn’t be delayed to fit a screening calendar. Tell whoever schedules it that you have symptoms, so it’s ordered and coded correctly.
A symptom you can describe precisely helps your doctor act faster. Our guide to bowel cancer symptoms people tend to dismiss covers what’s worth tracking — when the bleeding started, how your stools have changed, and how long it’s been going on.
✅ Patient Action: If you’ve had rectal bleeding or a lasting change in bowel habits for more than two to three weeks, book an appointment with your primary care clinician or a gastroenterologist and ask directly: “Do these symptoms warrant a diagnostic colonoscopy?”
Symptoms in younger adults are being missed
Colorectal cancer is rising in people under 50, and younger patients are too often reassured that they’re “too young” for it to be a concern. That delay matters: about three out of four adults under 50 who are diagnosed already have advanced-stage disease by the time it’s found.
You can use our symptom checker to organize what you’re experiencing before a visit, though it’s a preparation tool, not a diagnosis. If you’re under 45 with persistent symptoms, the takeaway is simple — being young lowers the odds, but it does not rule cancer out, and persistent symptoms still warrant a real evaluation.
When to start screening and how often you need it
Average-risk adults should begin colorectal cancer screening at age 45 and continue through 75, according to the U.S. Preventive Services Task Force and the American Cancer Society. For adults 76 to 85, screening becomes an individual decision based on overall health and prior screening. The recommended starting age dropped from 50 to 45 in 2021.
That five-year change is the single most important thing many people — and some outdated web pages — still get wrong. If you’re between 45 and 49 and have been told you can wait, that guidance is out of date.
📊 Clinical Data Point: The U.S. Preventive Services Task Force lowered the average-risk screening start age from 50 to 45 in May 2021, citing rising colorectal cancer rates in younger adults. (Source: U.S. Preventive Services Task Force, 2021.)
Why screening now starts at 45
The change was driven by a clear, measurable trend: colorectal cancer incidence has been climbing steadily in adults under 50. Starting at 45 captures the front edge of that rise, and notably, about half of people diagnosed before 50 fall in the 45-to-49 window — exactly the group the new guidance now reaches.
Screening this age group earlier does two things at once. It finds and removes precancerous polyps before they can become cancer, and it catches cancers earlier, when treatment works best.
How often you need each test
The right interval depends on which test you choose and what it finds. For average-risk adults with normal results, the standard schedules are:
- Colonoscopy: every 10 years
- FIT (fecal immunochemical test): every year
- Multi-target stool DNA test (Cologuard): every 3 years
- CT colonography (virtual colonoscopy): every 5 years
- Flexible sigmoidoscopy: every 5 years, or every 10 years combined with a yearly FIT
- Blood-based test (Shield): every 3 years
A normal colonoscopy buys the longest interval because polyps generally take years to develop and the exam removes any that are present. The CDC’s summary of how often to have each screening test reflects the current age-45 recommendation and the schedules above.
When you may need to start earlier
The age-45 rule is for average-risk adults. You may need to start sooner, screen more often, or use colonoscopy specifically rather than a home test if you have a family history of colorectal cancer or advanced polyps, an inherited syndrome such as Lynch syndrome or familial adenomatous polyposis, or inflammatory bowel disease. The higher-risk section covers each of these in detail.
✅ Patient Action: Ask your primary care clinician: “Based on my age, family history, and health, when should I start screening, and which test is the best fit for me?”
Which colon cancer screening test do you actually need?
There are six recommended ways to screen for colorectal cancer, and the best one is the one you’ll actually complete. They differ in how thoroughly they see the colon, how often you repeat them, whether they catch precancerous polyps or only established cancer, and what they cost. The table below compares them at a glance; the sections after it explain the trade-offs that matter most.
| Test | What it detects | How often | Finds precancerous polyps? | Best for |
|---|---|---|---|---|
| Colonoscopy | Cancer and polyps, and removes them | Every 10 years | Yes — the most of any test | A complete, one-and-done option |
| Multi-target stool DNA (Cologuard) | ~92–94% of cancers; some polyps | Every 3 years | Some | At-home testing; avoiding a scope if normal |
| FIT (fecal immunochemical test) | ~80% of cancers | Every year | Limited | Low-cost, simple yearly home screening |
| CT colonography (virtual) | Cancer and larger polyps | Every 5 years | Larger polyps only | Avoiding sedation or a standard scope |
| Flexible sigmoidoscopy | Cancer and polyps in the lower colon | Every 5 years (or 10 with yearly FIT) | Lower colon only | A shorter, limited-scope visual exam |
| Blood test (Shield) | ~83% of cancers | Every 3 years | Very limited (~13%) | Those who decline every other option |
Source note: sensitivity figures reflect FDA labeling and the ECLIPSE trial for Shield (New England Journal of Medicine, 2024), 2024 New England Journal of Medicine data for the latest multi-target stool DNA test, and the American Cancer Society and US Multi-Society Task Force for intervals. Colonoscopy is the most sensitive option; exact percentages vary by study.
🔬 How It Works: Stool DNA tests look for abnormal DNA and tiny amounts of blood shed into the stool by cancers and some polyps. Blood-based tests detect fragments of tumor DNA circulating in the bloodstream. Both can flag a cancer, but neither sees the colon directly — so any positive result still requires a colonoscopy to confirm and treat what’s there.
Colonoscopy vs. Cologuard (stool DNA)
Cologuard is a multi-target stool DNA test you do at home, mailing a sample to a lab. The latest version detects roughly 92 to 94 percent of colorectal cancers, which is high — but it catches fewer precancerous polyps than a colonoscopy, and it’s repeated every three years rather than every ten. A normal result is reassuring; a positive result means you’ll need a colonoscopy next.
The honest trade-off is convenience versus completeness. Cologuard avoids prep and sedation and can be done from home, but it doesn’t remove anything, and it’s less sensitive than a scope for the precancerous growths that screening is meant to catch early.
The FIT test: simple, cheap, yearly
The fecal immunochemical test is the most accessible option — inexpensive, done at home, with no prep — and it detects about 80 percent of colorectal cancers in a single round. Its strength comes from repetition: done every year as recommended, FIT becomes a strong screening strategy over time. Its limitation is that any one test catches fewer cancers than a colonoscopy or Cologuard, and like all stool tests, a positive result must be followed by a colonoscopy.
📊 Clinical Data Point: A normal stool-based test only counts if it’s repeated on schedule — FIT every year, multi-target stool DNA every three years — and any positive result is followed by a colonoscopy. (Source: American Cancer Society; US Multi-Society Task Force.)
The Shield blood test: what it can and can’t catch
Shield, approved by the FDA in July 2024, is the first blood test cleared as a primary screening option for colorectal cancer. Its appeal is obvious — a blood draw instead of a stool sample or a scope. But its performance comes with an important asterisk that the convenience can obscure.
📊 Clinical Data Point: In its pivotal trial, the Shield blood test detected about 83% of colorectal cancers but only about 13% of advanced precancerous polyps. (Source: FDA; ECLIPSE trial, New England Journal of Medicine, 2024.)
That 13 percent is the catch. Screening’s greatest value is finding and removing polyps before they become cancer, and a test that catches almost none of them works mainly to detect cancer that’s already present. For that reason, the American Cancer Society’s current screening recommendations state that blood-based tests are not a preferred option, and should be used only by people unwilling to do a stool test or a visual exam.
⚠️ Clinical Warning: A normal stool or blood test does not rule out a polyp that isn’t yet bleeding or shedding DNA. And any positive non-colonoscopy result must be followed by a colonoscopy — skipping that step defeats the entire purpose of screening.
CT colonography and flexible sigmoidoscopy
CT colonography, sometimes called a virtual colonoscopy, uses a CT scanner to build images of the colon. It still requires bowel prep but no sedation, and it’s repeated every five years; larger polyps show up well, but small ones may not, and anything found means a follow-up colonoscopy. Flexible sigmoidoscopy examines only the lower third of the colon with a shorter scope, which makes it quicker and lower-risk but leaves the upper colon unseen.
Both are valid, guideline-recommended choices for the right person, particularly someone who can’t have or strongly prefers to avoid a full colonoscopy. If you’ve had a sigmoidoscopy, our guide to reading sigmoidoscopy results explains what normal and abnormal findings mean.
The honest bottom line: the best test is the one you’ll complete
Colonoscopy is the most thorough option and the only one that detects and prevents in a single visit. Stool tests are excellent, evidence-backed alternatives, and a test you’ll actually do beats a more thorough one you keep putting off. Cost-effectiveness research published in 2025 found that colonoscopy and stool tests were both more effective and less costly than the first-generation blood test — a useful reality check against the newest, most convenient option.
The blood test sits at the bottom of that hierarchy for a reason, but it is still far better than no screening at all. If the choice for you is realistically between a blood test and skipping screening entirely, the blood test wins.
✅ Patient Action: If you’re choosing between tests, ask your clinician: “Given my risk level, is a stool or blood test reasonable for me, or should I have a colonoscopy — and if I pick a home test, what happens if it comes back positive?”
How to prep for a colonoscopy without the misery
The prep is the part people remember, and the part that scares them most — but it’s manageable once you know what’s coming and why it matters. The goal is simple: empty the colon completely so the doctor can see every part of the lining clearly. A clean colon means a more accurate exam and fewer missed polyps.
Your clinic will give you a specific prep sheet with exact products, doses, and timing. Follow that sheet, not a general guide — including this one — because the details vary by the prep you’re prescribed and by your own health. What follows is the shape of the process, so none of it catches you off guard.
The week before: what to expect
A few days out, most prep instructions ask you to ease off foods that leave residue — nuts, seeds, popcorn, and high-fiber items — so the colon clears more easily. This is also when you confirm logistics: who’s driving you home, and time off work for the procedure day. Read your prep sheet early, not the night before, so you have time to ask questions and pick up what you need.
✅ Patient Action: When you book the colonoscopy, ask the scheduler two things: “When exactly do I stop eating and start the prep?” and “Do I need to change any of my regular medications beforehand?”
The day before: clear-liquid diet and split-dose prep
The day before, you’ll typically switch to a clear-liquid diet — broth, water, clear juices without pulp, plain gelatin, and similar — and avoid anything red or purple, which can be mistaken for blood. Then you’ll start the bowel prep itself, a liquid laxative regimen that empties the colon.
Most clinics now use a split-dose approach: half the prep the evening before, the other half several hours before the procedure. Split dosing isn’t there to inconvenience you — it produces a cleaner colon and better polyp detection than taking it all at once, which is why guidelines favor it.
🔬 How It Works: The prep solution pulls water into the colon and stimulates it to flush its contents. That’s why the instructions stress drinking the full amount and staying near a bathroom — the volume of fluid is what clears the lining, and stopping early can leave residue that hides polyps.
Medications you may need to adjust
Some routine medications need attention before a colonoscopy, but the specifics depend entirely on what you take and why. Blood thinners and antiplatelet drugs, diabetes medications including insulin and GLP-1 drugs, and certain other prescriptions may need to be paused or adjusted — but only your prescribing clinician can tell you whether, how, and when.
Do not stop or change any prescription on your own based on a general article. Bring a full list of everything you take, including over-the-counter products and supplements, to whoever is arranging the procedure.
⚠️ Clinical Warning: Never stop a blood thinner or adjust insulin without explicit instructions from the clinician who prescribed it. Stopping some medications carries its own risks, and the right plan is individual — not something to guess at from a checklist.
Tips to make the prep easier
The prep is unpleasant, but a few practical steps make it more tolerable: chill the prep solution if your instructions allow, use a straw, keep clear electrolyte drinks and flushable wipes on hand, and stay near a bathroom once you start. Plan a quiet evening — you won’t want to leave the house, and that’s normal.
The morning of your procedure
You’ll finish the second half of your prep in the early hours before your appointment, then stop all liquids at the time your clinic specifies — usually a couple of hours before, to keep sedation safe. Wear comfortable clothes, leave valuables at home, and bring your ID, insurance information, and the name of the person driving you. From here, the hard part is behind you.
What actually happens during a colonoscopy
Once the prep is done, the procedure itself is brief and, for most people, uneventful — you’re sedated, it takes well under an hour, and you won’t remember much of it. Knowing the steps ahead of time removes most of the remaining anxiety. Here’s what the day looks like from check-in to heading home.
Step by step, from check-in to recovery
After you check in, a nurse places a small IV line and reviews your history. You’ll receive sedation through that line, then lie on your side as the doctor gently advances the colonoscope through the colon. The scope is guided to the far end — the cecum, where the colon meets the small intestine — and then slowly withdrawn while the lining is examined.
If the doctor finds a polyp, they typically remove it during the same exam through the scope, a step called a polypectomy. Small tissue samples, or biopsies, may also be taken. You’re then moved to a recovery area to wake up from the sedation.
🔬 How It Works: The colonoscope is a flexible tube with a light and a high-definition camera at the tip, plus channels that let the doctor pass instruments to remove polyps or take samples. Most of the careful looking happens on the way out — the doctor withdraws slowly and deliberately, because that’s when polyps are spotted and removed.
Will you be asleep? Sedation explained
Most people are sedated for a colonoscopy and feel little or nothing during it. The depth ranges from moderate sedation, where you’re very drowsy but breathing on your own, to monitored anesthesia care using a medication called propofol, where you’re more deeply asleep. Which one you receive depends on your clinic, your health, and sometimes your preference.
🩺 Physician Note: Sedation choice isn’t one-size-fits-all. Your health history, medications, and the practice’s standard approach all factor in, so it’s worth asking ahead of time what to expect and whether anything in your history affects the plan.
Either way, you won’t be able to drive, work, or make important decisions for the rest of the day, which is why a ride home is mandatory. The procedure is monitored throughout by trained staff watching your breathing, heart rate, and oxygen.
How long the whole thing takes
The colonoscopy itself usually takes about 30 to 60 minutes, though you should plan for two to three hours at the facility once you include check-in, sedation, and recovery. If polyps are removed, the exam may run slightly longer — but that’s time well spent, because it means something was found and dealt with. If you’ve had other scope procedures, our explainer on what doctors see during an endoscopy covers how these exams are read.
Colonoscopy risks and complications to know
A colonoscopy is a very safe procedure, but it’s still a medical one, and honest information means naming the risks rather than waving them away. Serious complications are uncommon — most people have nothing worse than temporary bloating — but knowing the warning signs afterward genuinely matters. This section covers both.
How common are complications, really?
The serious risks of a colonoscopy — a tear in the colon wall (perforation), significant bleeding after a polyp is removed, and reactions to sedation — are uncommon. They’re more likely when polyps are removed than during a look-only exam, and your individual risk depends on your health, your medications, and what’s found.
🩺 Physician Note: The small risks of a colonoscopy are weighed against a large benefit — finding and removing precancerous polyps before they can become cancer. For most average-risk adults, that trade-off strongly favors screening, but the right balance for you is a conversation worth having with your doctor if you have specific health concerns.
For most people, the after-effects are minor and short-lived: cramping, gas, and bloating that ease within hours as the air used during the exam clears.
Warning signs to call your doctor about
The rare complication usually shows up in the hours and first day or two afterward, when you’re already home — which is exactly why the warning signs are worth knowing. Contact your doctor or seek urgent care if you have:
- Severe or worsening abdominal pain that doesn’t ease
- Heavy or persistent rectal bleeding, or passing large amounts of blood
- A fever
- Dizziness, fainting, or a racing heart
A small amount of light spotting can be normal after a polyp removal, especially with your first bowel movement. The signs above are different — they’re your cue to act rather than wait.
⚠️ Clinical Warning: Don’t talk yourself out of calling because it’s after hours or you don’t want to be a bother. Severe abdominal pain or heavy bleeding after a colonoscopy needs prompt evaluation, and acting early is always the safer choice.
✅ Patient Action: Before you leave the facility, ask: “What’s normal in the next 24 hours, and what symptoms mean I should call you or go to the ER?” Write down the number to call.
Your results explained: polyps, biopsy, what’s next
Waiting on results is its own kind of stress, so here’s what the common findings actually mean — and why a polyp, the thing people fear most, is usually a sign the test did its job. Most findings are manageable, and many are reassuring. Let’s walk through them calmly.
What it means if they found a polyp
Finding a polyp is common, and on its own it is not a cancer diagnosis. A polyp is a small growth on the colon lining, and most are benign; screening exists precisely to find and remove them before any of them could become a problem. In most cases the doctor removes the polyp during the same colonoscopy, so by the time you hear “we found a polyp,” it’s usually already gone.
🔬 How It Works: A removed polyp is sent to a pathology lab, where it’s examined under a microscope to determine its type and whether it showed any concerning changes. That analysis is what tells your doctor how often you’ll need future colonoscopies — the polyp itself is handled during the exam; the report guides what comes next.
Types of polyps and why the type matters
Not all polyps carry the same risk, which is why the pathology report matters. Adenomatous polyps and sessile serrated lesions are the types that can, over years, progress toward cancer, so finding and removing them is the whole point of screening. Hyperplastic polyps, by contrast, are common and generally low-risk.
The number, size, and type of polyps found together determine your follow-up schedule. Our breakdown of what each colonoscopy finding means explains the terms you’ll see, so the report reads as information rather than alarm.
Understanding a biopsy result
If tissue was sampled or a polyp removed, the biopsy result is the lab’s read on exactly what it was. These results take time — often several days to two weeks — and that wait is routine, not a sign something is wrong. A pathologist examines the tissue and reports its type, and whether any cell changes were present.
If you want help making sense of the document itself, our guides to reading a biopsy report and decoding a pathology result walk through the language step by step.
When you’ll need your next colonoscopy
Your next colonoscopy isn’t a fixed date — it depends on what this one found. A completely normal exam in an average-risk adult typically means 10 years until the next one, while finding certain polyps shortens that interval to address the risk they represent. Your gastroenterologist sets the timing based on your specific pathology, so the surveillance plan is theirs to define, not something to estimate from a general rule.
✅ Patient Action: When you get your results, ask your gastroenterologist directly: “Based on what you found and the pathology, when exactly should my next colonoscopy be — and why that interval?”
Recovery: what to expect after your colonoscopy
Recovery from a colonoscopy is usually quick — most people are back to normal by the next day — but the sedation makes the first several hours their own small event. Here’s how the rest of the day and the day after typically go.
The first few hours (and why you need a ride)
Because you’ve been sedated, you can’t drive, return to work, or make important decisions for the rest of the day, even if you feel alert. That’s why arranging a ride home isn’t optional — it’s a safety requirement, and most facilities won’t discharge you without one. Plan to rest at home afterward; the medication can leave you groggy for hours.
Mild cramping, gas, and bloating are common right after, as the air used to inflate the colon during the exam works its way out. Walking around gently helps, and the discomfort usually passes within a few hours.
Eating, activity, and getting back to normal
Most people can eat normally and resume regular activity the next day, starting with a light meal once the sedation fully wears off. If a polyp was removed, your care team may give you specific instructions — a short list of foods to avoid or activities to skip for a day or two — and those instructions come from them, based on what was done.
The light spotting some people notice with the first bowel movement after a polyp removal is usually normal. The warning signs from the risks section — severe pain, heavy bleeding, fever — are what to watch for instead, and they’re your signal to call rather than wait.
What a colonoscopy costs and why “free” gets billed
A screening colonoscopy is one of the most-covered preventive services in the country — for most average-risk adults, it costs nothing out of pocket. Yet “free” screenings still generate surprise bills in a handful of specific, avoidable situations. Understanding the rules ahead of time is the difference between a $0 bill and a four-figure one.
What it costs with and without insurance
Without insurance, a colonoscopy typically runs about $2,000 to $3,500, a figure that can climb higher if polyps are removed and sent to pathology. The home-based and imaging tests cost less, which is part of their appeal. Here’s how the screening options compare on price.
| Test | Typical self-pay cost | Key cost detail |
|---|---|---|
| Colonoscopy | ~$2,000–$3,500 | Higher if polyps are removed (adds pathology fees) |
| CT colonography | ~$1,000–$2,000 | Still needs follow-up colonoscopy if abnormal |
| Cologuard (stool DNA) | ~$600–$900 | Repeated every 3 years |
| FIT | ~$100–$300 | Lowest cost; repeated yearly |
Source note: cost ranges reflect published 2025–2026 U.S. pricing analyses and the Kaiser Family Foundation; actual prices vary widely by region, facility, and whether a polyp is removed.
📊 Clinical Data Point: Even where screening is fully covered, some patients still face out-of-pocket charges for the bowel-prep medication itself — a gap documented despite the ACA’s coverage mandate. (Source: Shah et al., Gastroenterology, 2025.)
What the ACA covers at no cost
Under the Affordable Care Act, both private insurers and Medicare must cover the screening tests recommended by the U.S. Preventive Services Task Force with no copay or deductible, for average-risk adults aged 45 to 75. That’s the rule that makes a routine screening colonoscopy free for most people. The American Cancer Society’s summary of the coverage laws for screening lays out how this applies across plan types.
The catch is in the word “screening.” When the same procedure is classified as diagnostic instead, the no-cost-sharing rule may not apply — and that reclassification is where the surprise bills come from.
The screening-vs-diagnostic billing trap
This is the part that catches people, so it’s worth being precise. A colonoscopy can shift from “screening” to “diagnostic” in a few situations: when it’s done because you have symptoms, when it’s a follow-up to a positive stool or blood test, or, historically, when a polyp is removed during what began as a screening. A diagnostic classification can trigger your deductible, copay, or coinsurance.
⚠️ Clinical Warning: Don’t assume a colonoscopy is automatically free because it’s “preventive.” How it’s coded — screening versus diagnostic — determines what you owe, and that coding can hinge on symptoms, a prior positive test, or a polyp. Confirm the coding before the procedure, not after the bill arrives.
The good news is that two of these traps have been closed by recent federal action, which the next sections explain.
🩺 Physician Note: Medicare has clarified that removing a polyp during a screening colonoscopy is an integral part of the screening, not a separate diagnostic service — so polyp removal alone should not convert a Medicare screening into a cost-shared procedure. Coverage details still vary by plan, so confirm with your own insurer.
Follow-up colonoscopy after a positive test is now covered
If you do a stool test (FIT or Cologuard) or a blood test and it comes back positive, the follow-up colonoscopy you need next is now covered with no cost-sharing — a change that closed a long-standing gap. This protection applies to private plans for plan years beginning on or after May 31, 2022, and to Medicare beneficiaries as of January 1, 2023.
📊 Clinical Data Point: Federal guidance now requires private plans (for plan years beginning on or after May 31, 2022) and Medicare (effective January 1, 2023) to cover a follow-up colonoscopy after a positive non-invasive screening test, with no patient cost-sharing. (Source: U.S. Departments of Labor, Health and Human Services, and Treasury; Centers for Medicare & Medicaid Services.)
That means choosing a home test no longer risks a large bill for the colonoscopy it might lead to — the whole screening pathway is covered.
Medicare coverage and what you may still owe
Medicare covers a screening colonoscopy once every 120 months — every 10 years — for average-risk beneficiaries, and once every 24 months for those at high risk. For a straightforward screening with no findings, you pay nothing. If a polyp is removed, a small coinsurance may still apply in some cases, though the polyp-removal clarification above has narrowed when that happens.
✅ Patient Action: Before the procedure, call your insurer or the facility’s billing office and ask: “Will this be coded as screening or diagnostic, and if a polyp is removed, will I owe anything?” Get the answer in writing if you can.
Higher risk? Family history, Lynch syndrome, and IBD
The age-45 starting point is for people at average risk. If colorectal cancer runs in your family, or you have an inherited syndrome or a chronic bowel condition, your timeline is different — usually earlier, often more frequent, and frequently colonoscopy specifically rather than a home test. Here’s what changes, and why the specifics belong to a specialist.
Family history of colorectal cancer or polyps
A family history of colorectal cancer or advanced polyps — particularly in a parent, sibling, or child — raises your risk and generally means starting screening earlier than 45 and repeating it more often. How much earlier depends on who was affected and at what age they were diagnosed. This is a clear reason to use colonoscopy rather than a stool or blood test, because it both screens and removes polyps.
✅ Patient Action: Map your family history before your next appointment — who had colorectal cancer or polyps, and how old they were when diagnosed — and ask: “Given this, when should I start screening, and how often?”
Lynch syndrome and FAP
Some people inherit conditions that sharply increase colorectal cancer risk. Lynch syndrome and familial adenomatous polyposis (FAP) are the most well-known, and they call for specialized, earlier, and more frequent surveillance than standard screening.
🔬 How It Works: Lynch syndrome and FAP are caused by inherited gene changes that make the colon far more likely to develop polyps and cancer, often at a younger age. Because the lifetime risk is so much higher, management is built around starting colonoscopy early and repeating it on a tighter schedule — guided by genetics specialists, not a general rule.
If a hereditary syndrome is known or suspected in your family, genetic counseling can clarify your risk and the right surveillance plan. Our genetic risk assessment tool can help you organize your family history before that conversation.
Screening with inflammatory bowel disease
Long-standing inflammatory bowel disease — ulcerative colitis or Crohn’s disease affecting the colon — raises colorectal cancer risk and changes the surveillance schedule. People with IBD often need colonoscopies on a more frequent, individualized timeline set by their gastroenterologist, based on how long they’ve had the disease and how much of the colon is involved.
✅ Patient Action: If you have ulcerative colitis or Crohn’s, ask your gastroenterologist: “Given how long I’ve had IBD and how much of my colon is affected, how often do I need surveillance colonoscopies?”
Colorectal cancer by the numbers, and why 45 matters
The case for screening is easier to understand with the numbers in front of you — particularly the trend that drove the starting age down to 45. Colorectal cancer is common, increasingly affects younger adults, and is one of the most preventable cancers through screening. Here’s what the most recent data shows.
Colorectal cancer is the third most common cancer in the United States and the second-leading cause of cancer death overall — and, notably, it is now the leading cause of cancer death in adults under 50.
📊 Clinical Data Point: The American Cancer Society projects about 158,850 new colorectal cancer cases and roughly 55,230 deaths in the United States in 2026. (Source: American Cancer Society, Colorectal Cancer Statistics, 2026.)
How common colorectal cancer is in 2026
Of those new cases, roughly 108,860 are colon cancers and about 49,990 are rectal cancers. The lifetime risk works out to about 1 in 25 for men and 1 in 26 for women. Overall incidence has been declining for decades — largely thanks to screening — but that decline masks a sharp split by age.
📊 Clinical Data Point: Colorectal cancer incidence is rising about 3% per year in adults aged 20–49, even as it falls about 2.5% per year in adults 65 and older. (Source: American Cancer Society, Colorectal Cancer Statistics, 2026.)
Why cases are rising in younger adults
The increase in younger adults is the trend behind the age-45 recommendation, and it’s still not fully explained — though modifiable factors like diet, physical inactivity, obesity, smoking, and alcohol are thought to play a substantial role. The consequences are serious: about three out of four adults under 50 who develop colorectal cancer aren’t diagnosed until it’s already advanced. Our guide to colon cancer symptoms in people under 50 covers what younger adults should watch for.
Because obesity is one of the modifiable risk factors, knowing where you stand can be a useful starting point; our BMI calculator gives you that number in seconds, though it’s only one piece of overall risk.
What on-time screening actually prevents
Here’s the encouraging part. Screening works on two fronts — it finds and removes precancerous polyps before they can become cancer, and it catches cancer early, when treatment is most effective. And the age-45 change targets exactly the right group: about half of people diagnosed before 50 are between 45 and 49, the very window the new guidance now covers.
The American Cancer Society’s latest colorectal cancer statistics track these trends in detail. The simple takeaway is that on-time screening, starting at 45, is one of the most effective cancer-prevention steps available.
Colonoscopy FAQ: quick, sourced answers
1. At what age should you get a colonoscopy?
Average-risk adults should start colorectal cancer screening at age 45 and continue through 75, per the USPSTF and the American Cancer Society. The starting age was lowered from 50 to 45 in 2021 because of rising cancer rates in younger adults. If you have a family history or other risk factors, you may need to start earlier — ask your doctor.
2. How often do I need a colonoscopy?
For an average-risk adult with a normal result, the next colonoscopy is typically 10 years away — the longest interval of any screening test, because the exam removes polyps and they take years to develop. Finding certain polyps shortens that interval. Your gastroenterologist sets the timing based on what your colonoscopy actually finds.
3. How much does a colonoscopy cost without insurance?
A colonoscopy typically costs about $2,000 to $3,500 without insurance, and more if polyps are removed and sent to pathology. Home-based tests cost far less — FIT around $100 to $300, Cologuard around $600 to $900. With insurance, a screening colonoscopy is usually fully covered for average-risk adults aged 45 to 75.
4. Is a colonoscopy covered by insurance?
Yes — under the Affordable Care Act, private insurers and Medicare must cover screening colonoscopy with no copay or deductible for average-risk adults 45 to 75. The exception is when it’s classified as diagnostic rather than screening, which can trigger cost-sharing. Confirm how yours will be coded with your insurer before the procedure.
5. Why was I billed for a “free” screening colonoscopy?
Usually because it was coded as diagnostic rather than screening — for example, because you had symptoms, it followed a positive stool test, or, historically, because a polyp was removed. A diagnostic classification can trigger your deductible or coinsurance. Recent federal rules have closed some of these gaps; confirm coding with your provider beforehand.
6. What’s the prep for a colonoscopy?
The day before, you switch to a clear-liquid diet and take a liquid laxative prep, usually in a split dose — half the evening before and half a few hours before the procedure — to empty the colon completely. Follow your clinic’s specific prep sheet exactly, since products and timing vary, and ask which of your regular medications need adjusting.
7. Are you asleep during a colonoscopy?
Most people are sedated and feel little or nothing. Sedation ranges from moderate sedation, where you’re drowsy but breathing on your own, to monitored anesthesia care with propofol, where you’re more deeply asleep. Either way, you can’t drive or work for the rest of the day, so a ride home is required.
8. How long does a colonoscopy take?
The procedure itself usually takes about 30 to 60 minutes, but plan for two to three hours at the facility once check-in, sedation, and recovery are included. If polyps are removed, it may run a little longer. You’ll spend time in recovery afterward, waking up from the sedation before you’re discharged.
9. What happens if they find a polyp?
Finding a polyp is common and is not a cancer diagnosis — a polyp is a growth that, in some cases, could become cancer over years. In most cases it’s removed during the same colonoscopy and sent to a lab, where its type determines how soon you’ll need your next exam. Discuss your specific results with your gastroenterologist.
10. How accurate is a colonoscopy?
A colonoscopy is the most sensitive colorectal cancer screening test and the only one that both detects and removes precancerous polyps in a single exam. That’s why it’s considered the reference standard against which other tests are measured. No screening test is perfect, but colonoscopy offers the most complete view of the colon.
11. What are the risks of a colonoscopy?
Serious complications — a tear in the colon wall, significant bleeding after polyp removal, or sedation reactions — are uncommon, and most people have nothing worse than temporary bloating. Risks are slightly higher when polyps are removed. Call your doctor for severe abdominal pain, heavy bleeding, fever, or fainting afterward, as these can signal a rare complication.
12. Do I need a colonoscopy if my stool or blood test is positive?
Yes. A positive stool or blood test doesn’t confirm cancer — it signals that a colonoscopy is needed to look directly, find the cause, and remove anything present. Skipping that step defeats the purpose of screening. This follow-up colonoscopy is now covered with no cost-sharing under recent federal rules, so cost shouldn’t be a barrier.
13. Can I be screened without a colonoscopy?
Yes — recommended alternatives include the FIT stool test (yearly), the Cologuard stool DNA test (every 3 years), CT colonography (every 5 years), flexible sigmoidoscopy (every 5 years), and the Shield blood test (every 3 years). Each has trade-offs in accuracy and convenience, and any positive result requires a follow-up colonoscopy. Discuss the best fit with your clinician.
14. Is the Shield blood test as good as a colonoscopy?
No. The Shield blood test, FDA-approved in 2024, detected about 83% of colorectal cancers but only about 13% of advanced precancerous polyps in its trial. Because screening’s main value is catching polyps before they turn cancerous, major guidelines list blood tests as a non-preferred option — best reserved for people who won’t do a stool test or colonoscopy.
15. What’s the difference between colonoscopy and Cologuard?
A colonoscopy views the whole colon and removes polyps during the exam, repeated every 10 years. Cologuard is an at-home stool DNA test repeated every 3 years that detects roughly 92–94% of cancers but fewer precancerous polyps, and a positive result requires a colonoscopy. Colonoscopy is more thorough; Cologuard is more convenient. Your clinician can help you choose.
16. How long is recovery after a colonoscopy?
Most people are back to normal by the next day. The sedation means you can’t drive, work, or make important decisions for the rest of the procedure day, so a ride home is required. Mild bloating and gas are common for a few hours afterward. If a polyp was removed, follow any specific aftercare instructions from your care team.
Your next step before you book
If you’re 45 or older and haven’t been screened, or you’ve been putting off a colonoscopy you know you need, the most useful thing to know is this: the hardest part is the prep, the test itself is brief and sedated, and the payoff is real protection against one of the most preventable cancers there is. None of the fear around it — the prep, the cost, the results — holds up once you have accurate information, which is what this guide set out to give you.
Where to go from here depends on where you are. If you’re still deciding how to screen, revisit the six-test comparison above and weigh the trade-offs honestly, remembering that the best test is the one you’ll actually complete. If you’ve had your colonoscopy and are waiting on a report, our results and pathology guides walk through what the findings mean.
Before your next appointment, download our Colonoscopy Prep + Questions-for-Your-Doctor Checklist — a single page covering what to ask about prep, medication adjustments, sedation, cost coding, and results, so nothing important gets forgotten in the room.
The single most important conversation to have is about which test and when. Ask your primary care clinician or gastroenterologist directly: “Based on my age, family history, and health, which screening test should I do, when should I start, and will it be covered with no out-of-pocket cost?” That one question covers the decision, the timing, and the bill.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.