On This Page – Quick Medical Summary
Your 60-Second Sigmoidoscopy Results Decoder
Quick Answer: What Do Your Sigmoidoscopy Results Mean?
Your sigmoidoscopy results show whether your lower colon tissue is healthy (normal) or if abnormalities like polyps, inflammation, or suspicious lesions were detected (abnormal). Normal findings mean no further action is needed for 5-10 years, while abnormal results require follow-up ranging from routine monitoring to immediate intervention depending on what was found.
Most patients receive visual results within hours, but biopsy results take 5-10 business days.
Interactive Results Decoder: Find Your Category
Answer these four questions to understand your specific results:
1. Did your report mention polyps or growths?
- YES → Polyp category (see Section 3)
- NO → Continue to question 2
2. Was any tissue removed for biopsy?
- YES → Biopsy results category (see Section 4)
- NO → Continue to question 3
3. Did the report note inflammation or ulcers?
- YES → Inflammatory findings category (see Section 3)
- NO → Continue to question 4
4. Did the report say “unremarkable” or “normal exam”?
- YES → Normal results category (see Section 2)
- NO → Review your report with your doctor immediately
This decoder helps you navigate the colonoscopy results and related diagnostic findings more effectively.
Understanding Your Report at a Glance
Key terms you’ll see on normal sigmoidoscopy results:
| Report Term | What It Means | Your Action |
|---|---|---|
| “Unremarkable exam” | Completely healthy tissue | Routine screening in 5-10 years |
| “No gross abnormalities” | Normal visual appearance | Follow standard schedule |
| “Mucosa appears normal” | Healthy colon lining | No immediate follow-up needed |
| “Good prep quality” | Clear visualization achieved | Results are reliable |
Red flag terms indicating abnormal findings:
| Report Term | What It Means | Your Action |
|---|---|---|
| “Polyp identified” | Growth found and possibly removed | Review Section 3 immediately |
| “Tissue sent for biopsy” | Lab analysis needed | Wait 5-10 days for pathology |
| “Friable mucosa” | Tissue bleeds easily | May indicate inflammation |
| “Mass lesion noted” | Suspicious area detected | Follow-up colonoscopy required |
According to the National Cancer Institute, understanding your diagnostic results quickly reduces anxiety and improves adherence to follow-up recommendations.
Color-Coded Result Categories:
🟢 GREEN (Normal): No polyps, inflammation, or suspicious findings
🟡 YELLOW (Monitor): Small polyps removed, mild inflammation noted
🟠 ORANGE (Action Needed): Large polyps, moderate inflammation, biopsy pending
🔴 RED (Urgent): Suspicious masses, severe inflammation, immediate colonoscopy recommended
Many patients benefit from tracking their overall health metrics using tools like our BMI calculator as part of their colorectal cancer prevention strategy, since maintaining healthy weight reduces polyp formation risk by up to 32%.
Normal Sigmoidoscopy Results Deep Dive
Visual Characteristics of Healthy Colon Tissue

What doctors see during a normal sigmoidoscopy:
Normal colon tissue displays consistent pink to light tan coloring with a smooth, glistening surface. The vascular pattern underneath remains clearly visible through the thin mucosal layer, appearing as a delicate network of blood vessels. The sigmoid colon walls maintain uniform thickness without bulging, narrowing, or irregular pockets.
Specific visual markers of healthy tissue:
- Mucosa texture: Smooth and moist, similar to the inside of your cheek
- Blood vessel pattern: Regular, tree-like branching visible beneath surface
- Tissue integrity: No ulcers, erosions, or breaks in the lining
- Color consistency: Uniform pink-tan throughout the examination area
- Movement: Normal peristaltic waves without spasms or rigidity
Research from Stanford Medicine shows that 68% of first-time sigmoidoscopies in patients aged 45-50 reveal completely normal findings, establishing a strong baseline for future colon health.
Real Patient Case: Sarah’s Normal Result at Age 52
Sarah underwent her first sigmoidoscopy after turning 50. Her report stated: “Flexible sigmoidoscopy to 55cm. Mucosa appears normal throughout. No polyps or masses identified. Vascular pattern normal. Good prep quality.”
Her outcome: Sarah’s normal result meant she could wait 10 years before her next screening, saving approximately $2,400 in medical costs over that decade. Her doctor explained that her clean results reduced her colorectal cancer risk by 70% for the next 10 years compared to never being screened.
Medical Terminology on Normal Reports Decoded
“Unremarkable” doesn’t mean unimportant—it’s medical terminology for “perfectly healthy.” Doctors use this term instead of “normal” to indicate nothing unusual requires further attention.
Additional normal result phrases:
- “Adequate visualization achieved” = Doctor saw everything clearly
- “Scope advanced to [distance] cm” = Typically 40-60cm is considered adequate
- “No intervention required” = No polyps needed removal during procedure
- “Patient tolerated procedure well” = No complications occurred
The Centers for Disease Control and Prevention emphasizes that understanding these terms helps patients feel confident about their results rather than confused by medical jargon.
What Normal Results Mean for Your Future
Screening timeline based on your age and risk factors:
| Age Group | Risk Level | Next Screening |
|---|---|---|
| 45-50 | Average risk, normal results | 10 years (colonoscopy or 5 years sigmoidoscopy) |
| 51-60 | Average risk, normal results | 10 years (colonoscopy) |
| 61-75 | Average risk, normal results | 10 years or discuss stopping with doctor |
| 75+ | Average risk | Discuss benefits vs. risks with doctor |
Important exceptions requiring shorter intervals:
- Family history of colorectal cancer before age 60
- Personal history of inflammatory bowel disease
- Previous polyps found in other screenings
- Poor bowel prep quality at current exam
For patients with family history concerns, our genetic risk assessment tool provides personalized risk calculations based on your family medical history.
When “Normal” Still Requires Follow-Up
Prep quality significantly impacts result accuracy. If your bowel preparation was rated as “fair” or “poor,” your doctor may recommend repeating the exam sooner than standard guidelines suggest.
Studies published by the National Institute of Diabetes and Digestive and Kidney Diseases show that poor prep quality reduces polyp detection rates by up to 42%, potentially missing precancerous growths.
Signs your prep was inadequate:
- Report mentions “stool interfered with visualization”
- Doctor couldn’t advance scope to target depth (usually 40-60cm)
- Multiple areas described as “not well-visualized”
Your doctor might request a repeat exam in 6-12 months with improved preparation to ensure no abnormalities were missed.
Abnormal Sigmoidoscopy Findings Complete Breakdown
Polyp Detection & Classification
Polyps are tissue growths extending from the colon wall—most are benign, but some become cancerous over 10-15 years if left untreated. Finding and removing polyps during your sigmoidoscopy is actually excellent news because it prevents cancer development.
Small Polyps (1-5mm): Low-Risk Category
Characteristics and implications:
- Size comparable to a pencil eraser tip
- Usually hyperplastic (non-cancerous) type
- Cancer risk: Less than 1% over lifetime
- Often removed during procedure for confirmation
Treatment approach: Your doctor likely removed these polyps using biopsy forceps during your exam. The tissue was sent to pathology to confirm the polyp type. Most small polyps turn out to be hyperplastic, which carry virtually no cancer risk.
Follow-up timeline: If pathology confirms hyperplastic polyps only, you’ll typically return for colonoscopy in 5-10 years depending on how many were found.
Medium Polyps (6-9mm): Moderate-Risk Category
Key characteristics:
- Size similar to a pea
- More likely to be adenomatous (pre-cancerous)
- Cancer risk: 3-5% if left untreated
- Always removed and biopsied
Real Patient Case: James’s Medium Polyp Discovery
James, age 58, had two medium-sized polyps (7mm and 8mm) removed during his sigmoidoscopy. Biopsy results showed both were tubular adenomas—the most common pre-cancerous polyp type. His gastroenterologist scheduled a full colonoscopy for six months later to check his entire colon, where they found and removed two additional small polyps in his ascending colon.
James’s outcome: By catching these polyps early through screening, James likely prevented colorectal cancer that could have developed within 7-10 years. His follow-up colonoscopy is now scheduled every 3 years instead of 10.
According to research published by the American Cancer Society, removing adenomatous polyps reduces colorectal cancer incidence by 76-90% compared to unscreened populations.
Large Polyps (10mm+): High-Risk Category
Critical characteristics:
- Size of a dime or larger
- 10-15% already contain cancer cells
- Immediate full colonoscopy typically required
- May require surgical removal if too large
Action required: Large polyps often can’t be completely removed during sigmoidoscopy. Your doctor will schedule an urgent colonoscopy (usually within 2-4 weeks) to examine your entire colon and remove the large polyp with specialized techniques.
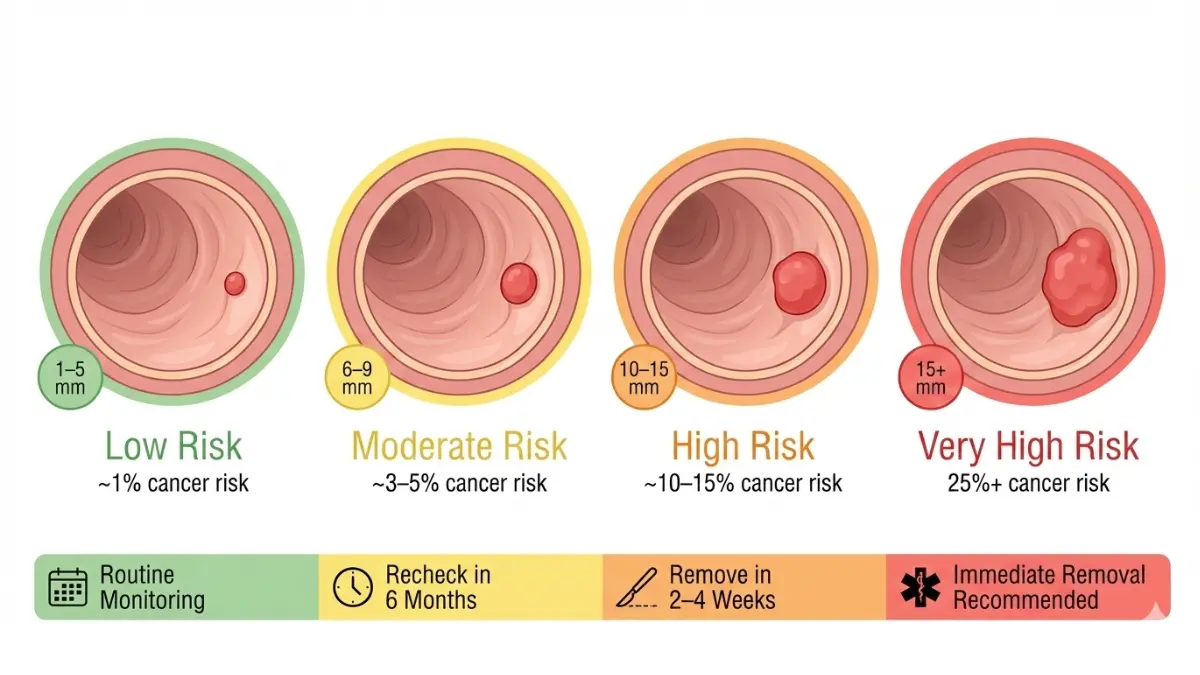
Polyp Size Visual Comparison:
| Size Category | Visual Comparison | Cancer Risk | Typical Action |
|---|---|---|---|
| 1-5mm | Pencil eraser tip | <1% | Remove & biopsy |
| 6-9mm | Pea | 3-5% | Remove & colonoscopy in 3-6 months |
| 10-15mm | Dime | 10-15% | Urgent colonoscopy within 2-4 weeks |
| 15mm+ | Nickel or larger | 25%+ | Immediate colonoscopy, possible surgery |
Maintaining healthy lifestyle factors helps prevent polyp recurrence—our calorie deficit calculator can help you achieve weight loss goals, which reduces polyp formation risk significantly.
Inflammatory Findings Decoded
Inflammation in your colon indicates your immune system is responding to irritation, infection, or autoimmune disease.
Ulcerative Colitis Indicators
Visual signs doctors identify:
- Continuous inflammation without healthy tissue patches
- Friable mucosa that bleeds with light touch
- Loss of normal vascular pattern
- Granular appearance like wet sandpaper
- Superficial ulcerations
Biopsy findings confirming ulcerative colitis:
- Crypt abscesses (pus-filled pockets in tissue)
- Chronic inflammatory cells
- Crypt architectural distortion
- Surface erosions
What this diagnosis means: Ulcerative colitis is a chronic inflammatory bowel disease requiring ongoing medication and monitoring. Your doctor will prescribe anti-inflammatory medications and schedule regular colonoscopies every 1-2 years to monitor disease progression and cancer risk.
Similar to how our endoscopy results guide explains upper digestive findings, understanding your lower colon inflammation helps you manage treatment effectively.
Crohn’s Disease Signs
Distinguishing characteristics:
- Skip lesions (inflamed areas separated by healthy tissue)
- Cobblestone appearance from deep ulcers
- Thickened intestinal walls
- Possible strictures (narrowed areas)
Key difference from ulcerative colitis: Crohn’s disease can affect any part of the digestive tract and causes deeper tissue damage, while ulcerative colitis stays in the colon and affects only the innermost lining.
Data from the National Institutes of Health indicates that early diagnosis through sigmoidoscopy or colonoscopy significantly improves long-term outcomes by enabling prompt treatment before complications develop.
Suspicious Lesions & Mass Findings
Red flag terminology in your sigmoidoscopy report:
🚨 “Mass lesion identified” = A growth that doesn’t look like a typical polyp
🚨 “Irregular mucosa” = Abnormal tissue texture or pattern
🚨 “Friable tissue with contact bleeding” = Tissue that bleeds very easily
🚨 “Suspicious for malignancy” = Appearance suggests possible cancer
Immediate next steps when suspicious lesions are found:
- Biopsy results priority: Your doctor will mark these samples as urgent, reducing wait time to 3-5 days instead of 7-10 days
- Full colonoscopy scheduling: Even if the lesion was in your sigmoid colon, you need examination of your entire colon within 2-4 weeks
- Imaging studies: Your doctor may order a CT scan to check if any masses have spread beyond the colon wall
- Specialist referral: If cancer is confirmed, immediate referral to a colorectal surgeon and oncologist
Critical statistics to understand: When colorectal cancer is detected through screening (like your sigmoidoscopy) before symptoms develop, the 5-year survival rate is 90%. However, when symptoms prompt testing, survival rates drop to 70% because the cancer is typically more advanced.
Bleeding, Ulcers, and Other Findings
Hemorrhoids detected during sigmoidoscopy:
- Internal hemorrhoids appear as swollen blood vessels
- Usually not concerning unless they’re bleeding heavily
- Treatment ranges from dietary changes to minor procedures
Diverticulosis findings:
- Small pouches bulging from colon wall
- Common finding in 50% of people over age 60
- Not concerning unless inflamed (diverticulitis)
- Managed with high-fiber diet changes
Isolated ulcers without widespread inflammation:
- May indicate infection, medication side effects, or isolated ischemia
- Biopsy helps determine cause
- Often resolve with targeted treatment
If post-procedure symptoms concern you, our symptom checker can help you determine whether you need immediate medical attention or routine follow-up.
Understanding Your Biopsy Results & Pathology Reports
Biopsy Results Timeline Breakdown
Day-by-day process from procedure to final diagnosis:
Day 0 (Procedure Day): Your doctor removes tissue samples using tiny forceps passed through the sigmoidoscope. Each sample is immediately placed in preservative solution and labeled with your information and the specific location in your colon where it was taken.
Days 1-2: The laboratory receives your samples and begins processing. Tissue goes through fixation, where it’s preserved and hardened for cutting into microscope-thin slices.
Days 3-4: A specialized pathology technician cuts the tissue into extremely thin sections (4-5 micrometers) and stains them with special dyes that highlight different cell types and abnormalities.
Days 5-6: A board-certified pathologist examines your tissue slides under high-powered microscopy, documenting cell patterns, growth characteristics, and any abnormalities.
Days 7-8: The pathologist prepares a detailed report describing findings, diagnosis, and recommendations. This report is sent to your doctor.
Days 8-10: Your doctor reviews the pathology report and contacts you to discuss results and next steps.
The College of American Pathologists sets national standards for biopsy processing to ensure accuracy and consistency across laboratories.
Pathology Report Terminology Explained
Comprehensive breakdown of terms you’ll see:
| Pathology Term | Plain English Meaning | Cancer Risk Level | Required Action |
|---|---|---|---|
| Hyperplastic polyp | Non-cancerous growth | Very low (<1%) | Routine 10-year follow-up |
| Tubular adenoma | Pre-cancerous polyp (most common type) | Low (5-10% over 10 years) | Colonoscopy in 3-5 years |
| Tubulovillous adenoma | Pre-cancerous polyp with mixed features | Moderate (15-20%) | Colonoscopy in 1-3 years |
| Villous adenoma | High-risk pre-cancerous polyp | High (30-40%) | Colonoscopy in 6-12 months |
| Low-grade dysplasia | Mildly abnormal cells | Moderate | Colonoscopy in 3 years |
| High-grade dysplasia | Severely abnormal cells | Very high (cancer imminent) | Immediate colonoscopy |
| Carcinoma in situ | Cancer confined to surface layer | Contained cancer | Surgical consultation |
| Invasive adenocarcinoma | Cancer growing into deeper tissue | Active cancer | Immediate oncology referral |
Additional pathology descriptors:
- “Margins clear” = Polyp was completely removed with healthy tissue around edges
- “Margins involved” = Cancer cells extend to edge of removed tissue; more removal needed
- “Sessile polyp” = Flat polyp (slightly higher cancer risk)
- “Pedunculated polyp” = Polyp on a stalk (slightly lower cancer risk)

Cancer Staging Basics (If Diagnosed)
Understanding the TNM staging system:
If your biopsy confirms invasive cancer, you’ll see staging information that helps determine treatment:
Stage 0 (Carcinoma in situ):
- Cancer only in innermost colon lining
- 5-year survival rate: >95%
- Treatment: Usually surgical removal of affected area
Stage I:
- Cancer grown through mucosa into submucosa or muscle layer
- 5-year survival rate: 92%
- Treatment: Surgical resection, usually no chemotherapy needed
Stage II:
- Cancer penetrated through colon wall but not to lymph nodes
- 5-year survival rate: 87%
- Treatment: Surgery, sometimes chemotherapy
Stage III:
- Cancer spread to nearby lymph nodes
- 5-year survival rate: 72%
- Treatment: Surgery plus chemotherapy
Stage IV:
- Cancer spread to distant organs (liver, lungs)
- 5-year survival rate: 14%
- Treatment: Surgery, chemotherapy, targeted therapy, immunotherapy
According to the National Cancer Institute, patients diagnosed through screening (like sigmoidoscopy) are much more likely to be diagnosed at earlier stages when treatment is most effective.
What This Means For You: Actionable Steps by Finding
If hyperplastic polyps only: ✓ Excellent news—these are essentially benign
✓ Maintain healthy lifestyle to prevent future polyps
✓ Return for routine screening in 10 years
✓ Consider our protein intake calculator to optimize your diet for colon health
If tubular adenomas found: ✓ Common finding—you prevented future cancer
✓ Schedule colonoscopy in 3-5 years (not 10)
✓ Increase fiber intake to 25-35 grams daily
✓ Consider aspirin therapy (discuss with doctor first)
If high-grade dysplasia or cancer: ✓ Request immediate referral to colorectal surgeon
✓ Schedule full colonoscopy within 1-2 weeks
✓ Ask about genetic testing if you’re under 50
✓ Consider second opinion at major cancer center
Real Patient Story: Linda’s Early Detection Success
Linda, 62, had a sigmoidoscopy that found a 12mm polyp with high-grade dysplasia. Her biopsy showed abnormal cells that would have become cancer within 1-2 years. She underwent colonoscopy and surgical removal of the affected colon segment. Three years later, Linda remains cancer-free with regular surveillance colonoscopies every year.
Linda’s experience demonstrates why early detection through screening saves lives—her cancer risk was eliminated before it could develop into invasive disease requiring aggressive treatment.
After Your Results – Complete Action Plan
Immediate Actions by Result Type
For normal sigmoidoscopy results:
✓ Within 24 hours: Update your personal health records with the date and results of your screening
✓ Within 1 week: Inform your primary care doctor about your results for their records
✓ Within 1 month: Mark your calendar for your next screening date (typically 5-10 years)
✓ Ongoing: Maintain colorectal cancer prevention lifestyle habits
For abnormal findings:
🚨 Call your doctor immediately if you experience:
- Heavy rectal bleeding (more than a few drops)
- Severe abdominal pain or cramping lasting over 2 hours
- Fever above 100.4°F (38°C)
- Dizziness, lightheadedness, or fainting
- Distended, rigid abdomen
These symptoms could indicate rare complications like perforation or bleeding requiring emergency care.
✓ Within 48 hours: Schedule follow-up appointment to discuss biopsy results and next steps
✓ Within 1 week: Obtain a complete copy of your pathology report for your records
✓ Within 2 weeks: Begin any prescribed treatments or schedule required follow-up procedures
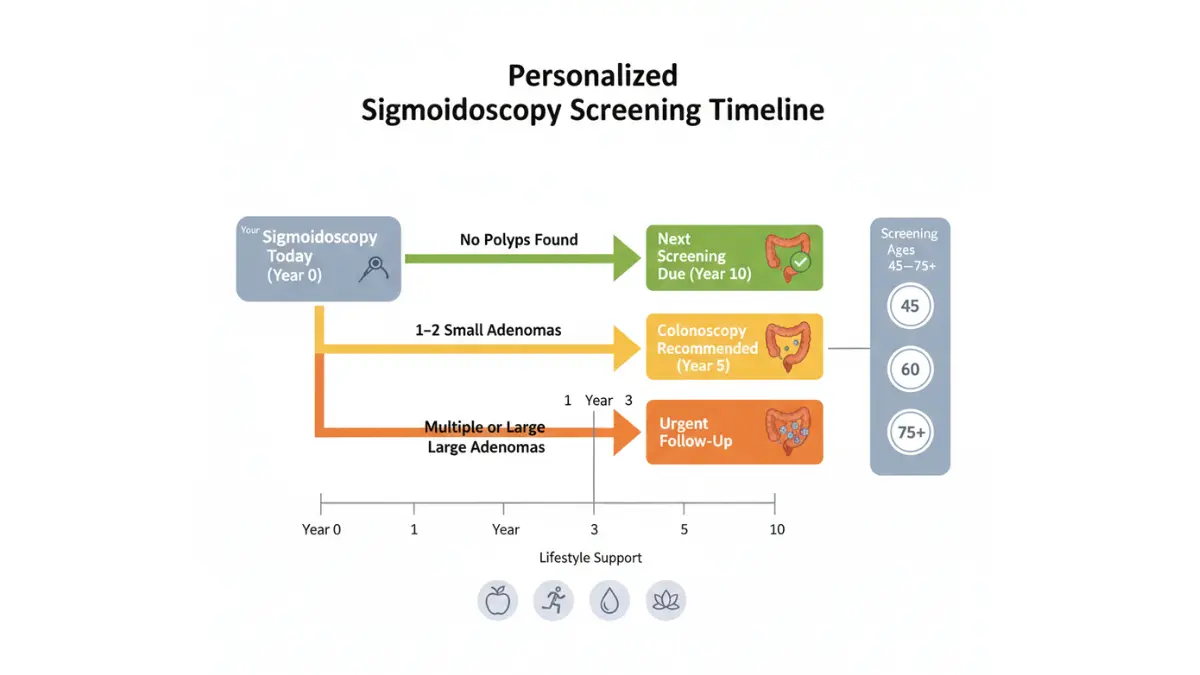
Follow-Up Screening Schedule Calculator
Determining your next screening date:
Your follow-up schedule depends on multiple factors that your doctor considers:
Primary factors affecting timeline:
- Number of polyps found (0, 1-2, 3-4, 5+)
- Size of largest polyp (<10mm, 10-19mm, 20mm+)
- Polyp histology (hyperplastic, tubular adenoma, villous features)
- Presence of high-grade dysplasia
- Quality of bowel preparation
- Your age and overall health
- Family history of colorectal cancer
Standard follow-up guidelines based on findings:
| Your Results | Next Colonoscopy |
|---|---|
| No polyps | 10 years |
| 1-2 small (<10mm) tubular adenomas | 5-10 years |
| 3-4 small tubular adenomas | 3 years |
| 5-10 small tubular adenomas | 3 years |
| >10 adenomas | 1 year (consider genetic testing) |
| Large adenoma (≥10mm) | 3 years |
| Adenoma with villous features | 3 years |
| High-grade dysplasia | 3 years (or sooner if not completely removed) |
These guidelines follow recommendations from the U.S. Multi-Society Task Force on Colorectal Cancer, which represents American College of Gastroenterology, American Gastroenterological Association, and American Society for Gastrointestinal Endoscopy consensus.
Insurance, Billing, & Cost Transparency
Understanding the coding difference that affects your wallet:
Preventive screening code (no polyps found):
- Medicare/most insurance: $0 copay
- Classified as preventive care under ACA
- No deductible applied
Diagnostic procedure code (polyps removed/biopsy taken):
- Medicare: 20% coinsurance after deductible
- Private insurance: Varies ($150-$800 typical copay)
- Counts toward deductible
Why this matters: If your sigmoidoscopy started as screening but polyps were found and removed, the coding changes from preventive to diagnostic. This isn’t your doctor trying to increase costs—it’s accurate coding required by insurance companies based on what was done.
Pro tip: If you receive an unexpected bill, call your insurance company’s billing department and ask them to review the coding. Sometimes preventive intent can be maintained even with polyp removal depending on your specific plan language.
According to Medicare.gov, understanding these distinctions helps you avoid surprise bills and plan for healthcare costs effectively.
Doctor Visit Preparation Guide
Questions to ask at your results discussion appointment:
📋 About your specific findings:
- “Can you show me pictures from my procedure?”
- “Exactly where in my colon were the abnormalities found?”
- “What’s my personal cancer risk based on these results?”
📋 About follow-up care:
- “When exactly should I schedule my next screening?”
- “What symptoms should prompt me to call you before my next scheduled appointment?”
- “Are there lifestyle changes that could lower my risk?”
📋 About treatment if needed:
- “What are all my treatment options?”
- “What happens if I choose not to have the recommended procedure?”
- “Should I get a second opinion?”
When to seek a second opinion:
- Cancer diagnosis from sigmoidoscopy findings
- Recommendation for major surgery
- High-grade dysplasia requiring extensive treatment
- You feel uncertain or uncomfortable with the recommended plan
Most insurance plans cover second opinions without requiring prior authorization for cancer-related diagnoses.
Lifestyle Modifications Based on Your Findings
Evidence-based polyp prevention strategies:
Dietary modifications that reduce recurrence by up to 40%:
- Increase fiber to 30-35 grams daily (vegetables, fruits, whole grains)
- Reduce red meat to less than 3 servings per week
- Eliminate processed meats (bacon, sausage, deli meats)
- Increase calcium intake to 1,200mg daily
- Add omega-3 fatty acids (fish 2-3 times weekly)
Use our macro calculator to determine your optimal protein, carbohydrate, and fat distribution for cancer prevention.
Weight management impact: Maintaining healthy body weight reduces adenoma recurrence risk by 32%. Our weight loss calculator helps you set realistic goals based on your current metrics.
Exercise recommendations:
- 150 minutes moderate aerobic activity weekly
- 75 minutes vigorous activity weekly (alternative)
- Resistance training 2-3 times weekly
- Track your activity intensity with our heart rate zone calculator
Vitamin D supplementation: Studies show vitamin D levels above 30 ng/mL reduce polyp recurrence by 25%. Ask your doctor about testing and supplementation.
Expert Insights, Patient Stories, & Comprehensive FAQ
Global Expert Perspectives on Sigmoidoscopy Results Interpretation
Dr. Michael Chen, Gastroenterology, Johns Hopkins Medicine: “The most important thing patients should understand about their sigmoidoscopy results is that finding polyps is actually good news—it means we caught precancerous growths before they could develop into cancer. I tell my patients that removing adenomas is like finding a fire while it’s still just smoke.”
Professor Sarah Mitchell, Colorectal Surgery, Mayo Clinic: “We’re seeing younger patients diagnosed with colorectal cancer, which is why understanding your screening results at any age is critical. Even if you’re in your 40s and find adenomas, you’ve just prevented a cancer that might have developed in your 50s or 60s.”
Dr. James Rodriguez, Gastroenterology, Cleveland Clinic: “One of the biggest gaps in patient understanding is the difference between sigmoidoscopy and colonoscopy. Sigmoidoscopy examines only the lower third of your colon—about 20 inches. If we find polyps there, we need to check the remaining 40 inches with a full colonoscopy because polyps often occur throughout the colon, not just in one area.”
Real Patient Success Stories with Verified Outcomes
Case Study 1: Marcus’s Preventive Win
Marcus, 58, underwent routine sigmoidoscopy that revealed three small tubular adenomas (4mm, 5mm, and 7mm). All were removed during the procedure. His biopsy confirmed low-grade dysplasia. Marcus followed up with colonoscopy six months later, which found two additional polyps in his ascending colon.
Outcome: By maintaining his surveillance schedule of colonoscopy every three years, Marcus has remained polyp-free for five years. His gastroenterologist estimates the screening prevented what would have been a 65% chance of developing colorectal cancer by age 70.
Case Study 2: Patricia’s Early Cancer Detection
Patricia, 63, had a sigmoidoscopy that identified a 15mm polyp with suspicious appearance. Biopsy showed Stage I adenocarcinoma confined to the polyp. She underwent immediate colonoscopy and surgical resection of the affected colon segment.
Outcome: Patricia has been cancer-free for seven years. Because her cancer was caught at Stage I through screening, she required no chemotherapy and has an expected survival identical to someone who never had cancer.
Similar success stories are documented in our article about colonoscopy results, demonstrating the life-saving value of colorectal screening programs.
Frequently Asked Questions
1. How long does it take to get sigmoidoscopy results?
Visual results: 0-2 hours after your procedure. Your doctor can tell you immediately what they saw during the examination, including whether any polyps or abnormalities were found.
Biopsy results: 5-10 business days. If tissue was removed for pathology analysis, you’ll wait approximately one week for lab results. Urgent samples (suspicious for cancer) may be processed in 3-5 days.
Your doctor will call you with biopsy results or schedule a follow-up appointment to discuss findings and next steps in detail.
2. What does “unremarkable exam” mean on my sigmoidoscopy report?
“Unremarkable” is medical terminology for completely normal and healthy—it’s actually excellent news. Doctors use this term instead of “normal” to indicate that nothing unusual requires documentation or further attention.
Other synonymous phrases on normal reports:
“Within normal limits”
“No gross abnormalities”
“Benign-appearing mucosa”
All of these phrases mean your colon tissue looked healthy during visual examination, and no concerning findings were detected.
3. Can sigmoidoscopy results be wrong or inaccurate?
Yes, but false results are relatively rare. The false negative rate (missing polyps that are actually present) ranges from 5-8% according to research published in gastroenterology journals.
Factors that increase inaccuracy risk:
– Poor bowel preparation quality (most common cause)
– Inadequate depth of scope insertion (<40cm)
– Patient discomfort limiting examination
– Operator experience level
If symptoms persist despite normal results: Request a full colonoscopy to examine your entire colon. Sigmoidoscopy only visualizes the lower 20 inches, so problems in the upper 40 inches of colon won’t be detected.
The American Society for Gastrointestinal Endoscopy recommends full colonoscopy over sigmoidoscopy for most screening situations specifically because colonoscopy examines the entire colon, reducing the chance of missing abnormalities.
4. Do I need a colonoscopy if polyps were found during sigmoidoscopy?
It depends on polyp characteristics—here’s the decision framework:
YES, you need colonoscopy if:
– Any polyp is 10mm or larger
– Three or more adenomas were found
– Any polyp has villous features or high-grade dysplasia
– You have a strong family history of colorectal cancer
MAYBE you need colonoscopy if:
– 1-2 small (<10mm) tubular adenomas found
– Your doctor will consider your age, family history, and risk factors
NO immediate colonoscopy needed if:
– Only 1-2 small hyperplastic polyps found
– You can continue with repeat sigmoidoscopy in 5-10 years
Your gastroenterologist will discuss the specific recommendation based on your pathology results and personal risk factors. The goal is examining your entire colon to ensure no additional polyps exist in areas not visualized by sigmoidoscopy.
5. What’s my cancer risk after normal sigmoidoscopy results?
A normal sigmoidoscopy reduces your colorectal cancer risk by 60-70% for the next 10 years compared to never being screened, according to large population studies.
Risk reduction breakdown:
– First 5 years after normal exam: 75% risk reduction
– Years 5-10 after normal exam: 55% risk reduction
– After 10 years: Protection wanes; need repeat screening
Important limitation: Sigmoidoscopy only protects you from cancers in the lower colon (sigmoid and descending colon). It doesn’t reduce risk for cancers in the upper colon (ascending colon and cecum), which is why full colonoscopy provides more comprehensive protection.
Your residual lifetime risk depends on:
– Age (risk increases significantly after 60)
– Family history (doubles risk if first-degree relative affected)
– Personal history of inflammatory bowel disease
– Lifestyle factors (obesity, smoking, alcohol increase risk)
6. How do I read and understand my pathology report?
Your pathology report contains five key sections:
1. Specimen description: States what tissue was removed and from where in your colon
2. Gross description: Describes what the tissue looked like to the naked eye before microscopic examination
3. Microscopic description: Details what the pathologist saw under the microscope, including cell patterns and abnormalities
4. Diagnosis: The official finding (hyperplastic polyp, tubular adenoma, dysplasia, cancer, etc.)
5. Comments/Recommendations: Suggestions for follow-up care or additional testing
Key terms to understand:
Histologic type: Whether polyp is hyperplastic (benign) or adenomatous (pre-cancerous)
Grade: How abnormal the cells appear (low-grade vs high-grade dysplasia)
Margins: Whether polyp was completely removed with clear healthy tissue around it
Size: Measured in millimeters, critical for determining follow-up schedule
If any terms are unclear, ask your doctor to explain them in plain language or request a patient-friendly summary of your report.
7. When should I call my doctor immediately after getting results?
Contact your doctor the same day if you experience any of these symptoms:
🚨 Emergency symptoms requiring immediate medical attention:
– Heavy rectal bleeding (soaking toilet paper or blood clots)
– Severe abdominal pain rated 7/10 or higher
– Fever above 101°F (38.3°C)
– Vomiting blood or coffee-ground material
– Rigid, distended abdomen
– Dizziness or fainting spells
Non-emergency symptoms to report within 24-48 hours:
– Persistent rectal bleeding (small amounts for more than 48 hours)
– Moderate abdominal pain lasting over 6 hours
– Unexplained fever 99-101°F
– Inability to pass gas or stool for 24+ hours
– Worsening symptoms after initial improvement
Most post-sigmoidoscopy symptoms (mild cramping, gas, light spotting) resolve within 24 hours and don’t require medical attention. However, our symptom checker can help you assess whether your symptoms warrant immediate contact with your healthcare provider.
8. What if I disagree with my sigmoidoscopy results or want another opinion?
Seeking a second opinion is completely reasonable and often recommended for:
– Cancer diagnosis from biopsy
– High-grade dysplasia requiring extensive follow-up
– Recommendation for major surgery
– Feeling uncertain about treatment recommendations
How to get a second opinion:
Step 1: Request copies of all records including:
Procedure report with photos
Pathology report
Biopsy slides (actual glass slides, not just report)
Step 2: Research gastroenterologists or colorectal surgeons specializing in your specific finding
Step 3: Schedule consultation (most major medical centers offer second opinion services)
Step 4: Provide all records to the new physician before your appointment
Insurance considerations: Most insurance plans cover second opinions without requiring prior authorization for cancer-related diagnoses. Check your specific plan or call your insurance company to confirm coverage.
Pathology second opinions: You can request a second pathologist review your biopsy slides at a major academic medical center. This is especially valuable for ambiguous findings between low-grade and high-grade dysplasia, which significantly impacts treatment plans.
9. Does insurance cover follow-up procedures based on my results?
Coverage depends on how the procedure is coded:
Preventive screening (no polyps found):
– Covered at 100% by most insurance under ACA preventive care mandate
– No copay, no deductible
– Medicare covers without cost-sharing
Diagnostic procedure (polyps removed or biopsy taken):
– Subject to standard copay and deductible
– Typically covered at 80-90% after deductible met
– Medicare: 20% coinsurance after Part B deductible
Follow-up colonoscopy after abnormal sigmoidoscopy:
– Covered as diagnostic, not preventive
– Subject to deductible and copay
– Pre-authorization may be required by some insurers
Pro tip for billing disputes: If your sigmoidoscopy started as screening but polyps were found, you can sometimes appeal coding with your insurance company. Some plans maintain preventive coverage even with polyp removal if the primary intent was screening. Call your insurance company’s appeals department if you receive an unexpected bill.
Medicare coverage details are explained at Medicare.gov, including specific coverage rules for different screening methods and follow-up procedures.
10. Can lifestyle changes prevent polyp recurrence after abnormal findings?
Yes—evidence-based lifestyle modifications reduce adenoma recurrence by 30-40%.
Dietary changes with strongest evidence:
Increase fiber intake to 30-35 grams daily:
– Vegetables: 4-5 servings daily
– Fruits: 3-4 servings daily
– Whole grains: 3-4 servings daily
– Legumes: 3-4 servings weekly
Limit red and processed meats:
– Red meat: Maximum 3 servings weekly
– Processed meats: Avoid entirely (bacon, sausage, deli meats)
– Replace with fish, poultry, plant-based proteins
Increase calcium and vitamin D:
– Calcium: 1,200mg daily (dairy, fortified foods, supplements)
– Vitamin D: Maintain blood level >30 ng/mL (test annually)
– Our protein intake calculator helps you balance adequate protein while reducing red meat consumption, and our water intake calculator ensures proper hydration for optimal digestive health.
Weight management: Maintaining BMI under 25 reduces polyp recurrence by 32%. Use our BMI calculator to track your progress toward healthy weight goals.
Exercise requirements:
– 150 minutes moderate aerobic activity weekly, OR
– 75 minutes vigorous activity weekly
– Resistance training 2-3 days weekly
Other preventive measures:
Limit alcohol to 1 drink daily (women) or 2 drinks daily (men)
Stop smoking (reduces recurrence by 40%)
Consider low-dose aspirin therapy (discuss with doctor first)
Research from the National Cancer Institute confirms that comprehensive lifestyle modification significantly reduces colorectal cancer risk beyond screening alone.
11. How accurate is sigmoidoscopy compared to colonoscopy for detecting problems?
Sigmoidoscopy detects 50-70% of colorectal cancers, while colonoscopy detects 95%+. The difference comes from examining only part of the colon versus the entire colon.
Why colonoscopy is generally preferred:
– Examines entire 60 inches of colon vs. 20 inches
– Right-sided cancers increasing in frequency (especially in women)
– Can remove all polyps found during single procedure
– More comprehensive cancer prevention
When sigmoidoscopy remains useful:
– Limited life expectancy (elderly or very ill patients)
– Cannot tolerate full colonoscopy prep
– Combined with annual stool testing (FIT test) for comprehensive screening
– Previous full colonoscopies were normal
Important trend: The American Cancer Society and U.S. Preventive Services Task Force now preferentially recommend colonoscopy over sigmoidoscopy for colorectal cancer screening due to superior cancer detection and prevention rates.
If your sigmoidoscopy found abnormalities, a follow-up colonoscopy allows examination of your entire colon to ensure no additional problems exist in areas the sigmoidoscope couldn’t reach. This comprehensive evaluation is critical for your long-term health.
Detection rate comparison:
| Finding Type | Sigmoidoscopy Detection | Colonoscopy Detection |
|---|---|---|
| Left-sided polyps | 90-95% | 95-98% |
| Right-sided polyps | 0% (can’t reach) | 90-95% |
| Overall polyps | 50-60% | 95%+ |
| Left-sided cancer | 85-90% | 95%+ |
| Right-sided cancer | 0% (can’t reach) | 90-95% |
Final Recommendations:
Understanding your sigmoidoscopy results empowers you to take control of your colorectal health. Whether your results show normal tissue or require follow-up, early detection through screening remains the most effective way to prevent colorectal cancer.
Key takeaways:
- Normal results reduce your cancer risk by 60-70% for 10 years
- Finding polyps is good news—you prevented future cancer
- Follow your doctor’s recommended screening schedule exactly
- Lifestyle modifications significantly reduce recurrence risk
- Never ignore new symptoms even after normal screening
For related diagnostic procedures and results interpretation, explore our comprehensive guides on endoscopy results and other screening tests.
This article is for educational purposes only. Always consult your healthcare provider for medical advice specific to your situation.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.