On This Page – Quick Medical Summary
Opening a patient portal to find your Cologuard or FIT result marked “positive” or “abnormal” is frightening — but a positive stool test is not a cancer diagnosis. It means the test detected something that needs a closer look, and that closer look is a colonoscopy.
Where you are right now shapes what matters most on this page:
- Just got the result and scared it means cancer → start with what a positive actually means; most are not cancer.
- Worried about the cost → skip to coverage; since 2023, the follow-up colonoscopy is covered with no cost-sharing under Medicare and most plans.
- Wondering how urgently to act → see how soon to schedule, and the one point every study agrees on.
- Caring for a parent on Medicare → the Medicare details are written for exactly that situation.
This guide walks through each step, with every figure tied to a named, checkable source, and fits inside our complete guide to colonoscopy prep, cost, and results.
ℹ️ Medical Disclaimer: This article is general health education, not medical or insurance advice. It covers screening-result interpretation, a medical procedure (colonoscopy), and insurance coverage — areas where specifics depend on your health and your plan. For decisions about your result, your procedure, or your costs, consult a board-certified gastroenterologist and confirm coverage directly with your insurer or plan. If you have urgent symptoms such as rectal bleeding, contact a clinician promptly rather than waiting.
What a positive Cologuard or FIT result actually means
No — a positive Cologuard or FIT result does not mean you have cancer. It means the test found traces of blood, or abnormal DNA, that warrant a colonoscopy to find the cause. Most positive results are not cancer; they are often caused by polyps or other minor bleeding in the digestive tract.
What the test detected — and what it didn’t
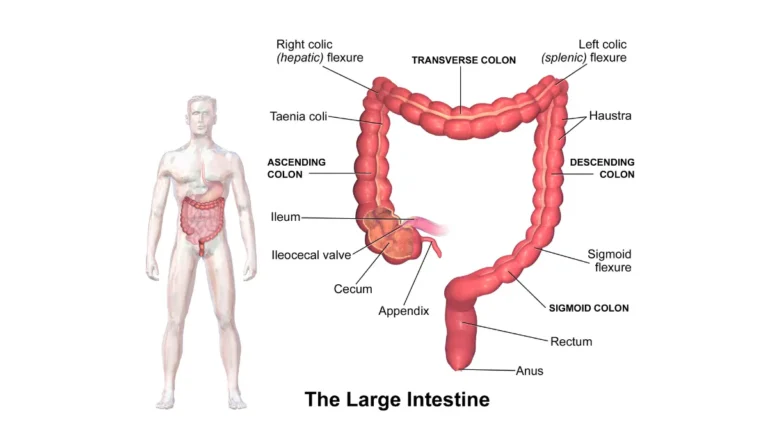
A fecal immunochemical test detects hidden blood in the stool. A stool DNA test like Cologuard looks for both blood and altered DNA markers. Neither test sees inside your colon — that is what the colonoscopy does.
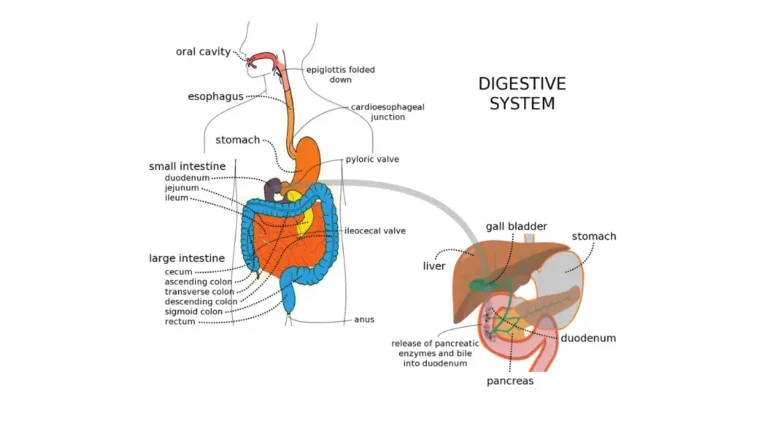
🔬 How It Works: A FIT detects human hemoglobin — blood — in a stool sample, even amounts too small to see. A stool DNA test adds a search for altered DNA that polyps and tumors can shed into stool. A positive means one of these signals was found; it cannot tell where the signal came from, which is why a colonoscopy follows.
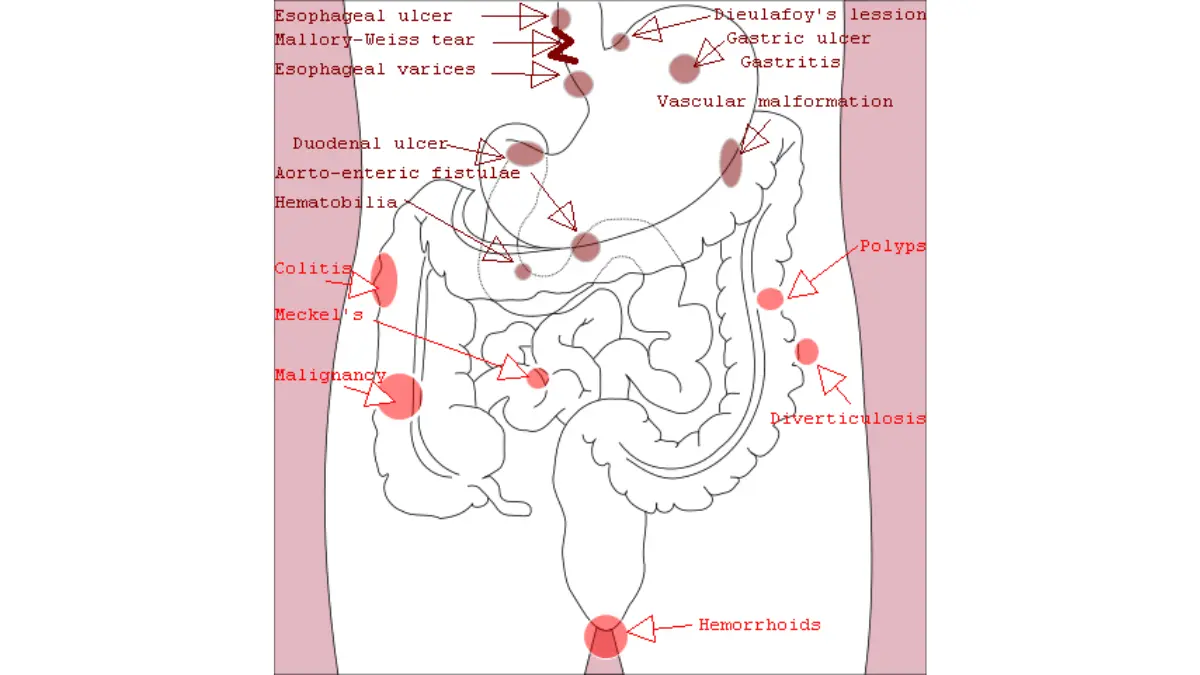
Adapted from Wikimedia Commons Causes of gastrointestinal bleeding.png, licensed under CC BY 4.0.
How accurate are these tests?
These tests catch most cancers but miss many precancerous polyps — a key reason colonoscopy remains the definitive step.
📊 Clinical Data Point: In its FDA approval study, the current Cologuard Plus test detected about 95% of colorectal cancers but only about 43% of advanced precancerous polyps, at roughly 94% specificity — Source: Exact Sciences / FDA approval (BLUE-C study, New England Journal of Medicine, 2024).
A single FIT detects roughly 70–80% of colorectal cancers, with lower sensitivity for advanced polyps. If you want to see how the stool test you took compares head-to-head, our guide on how Cologuard compares with colonoscopy lays it out.
Why a positive doesn’t mean cancer
A screening test is built to flag people who need a closer look, not to diagnose. A positive often traces back to what colon polyps mean for your cancer risk rather than to cancer. If you’re trying to understand why you were flagged, you can also gauge your personal colorectal risk factors.
Why a colonoscopy is the only recommended next step
After a positive stool test, repeating the test or switching to another at-home test is not the answer — a colonoscopy is the recommended follow-up. A positive result has already done its job: it flagged you for a closer look.
Why you can’t just re-test
A second stool test cannot rule out what the first one detected, and it delays the one procedure that can actually find and remove the cause.
🩺 Physician Note: Current guidance from major screening panels emphasizes a point patients often miss: a colorectal screening program is not “complete” until an abnormal stool-test result is followed up with a colonoscopy. The stool test starts the process; the colonoscopy finishes it.
What a colonoscopy does that a stool test can’t
A colonoscopy lets a doctor view the entire colon and remove polyps during the same procedure — finding and preventing in one step. The American Cancer Society’s overview of why colonoscopy is the diagnostic follow-up explains how it differs from a stool test.
Is the follow-up colonoscopy covered by insurance?
Yes. Since 2023, a colonoscopy after a positive stool test is treated as part of screening, and most people pay nothing for the procedure itself. This is where some online guides are out of date — so here is the current rule, by plan type.
If you have commercial or marketplace insurance
📊 Clinical Data Point: Federal rules require most non-grandfathered health plans to cover a follow-up colonoscopy after a positive non-invasive stool-based screening test with no cost-sharing, for plan years beginning on or after May 31, 2022; and Medicare to do the same, effective January 1, 2023 — Sources: U.S. Departments of Labor, Health and Human Services, and Treasury (ACA Implementation FAQ Part 51, 2022); CMS, Calendar Year 2023 Physician Fee Schedule Final Rule.
Federal guidance also treats removing a polyp during that colonoscopy as part of the screening, so for commercial plans it should not trigger cost-sharing either. You can review the basics of colorectal cancer screening coverage on HealthCare.gov.
If you have Medicare
For traditional Medicare, a colonoscopy after a positive Cologuard or FIT is still billed as a screening colonoscopy, with no cost-sharing, under a CMS rule effective January 1, 2023. The provider applies a specific billing code — the KX modifier — so the claim is processed as screening. CMS describes the change in its 2023 Physician Fee Schedule materials.
What about a polyp found during the colonoscopy?
This is where traditional Medicare gets nuanced. Separately from the rule above, when a screening colonoscopy converts to diagnostic because a polyp is removed, Medicare’s coinsurance is being phased out.
📊 Clinical Data Point: For traditional Medicare, when a screening colonoscopy converts to diagnostic because a polyp is removed, coinsurance is 15% for 2023–2026, 10% for 2027–2029, and 0% from 2030, with the Part B deductible waived — Source: CMS / Medicare.
Sources differ on whether the screening-follow-up coding waives even this coinsurance, so don’t assume a guaranteed $0 if a polyp is removed under traditional Medicare. A Medigap policy covers any coinsurance that does apply. Medicare Advantage plans must cover at least what Original Medicare covers — confirm the specifics with your plan.
Make sure it’s billed correctly
✅ Patient Action: Before the procedure, ask both your doctor’s office and the facility to confirm the colonoscopy will be coded as a screening or complete-screening follow-up — with the KX modifier for Medicare. Incorrect coding is the most common cause of a surprise bill.
For more on out-of-pocket scenarios, see whether a colonoscopy is free and what a colonoscopy costs.
How soon should you schedule the colonoscopy?
Most guidelines recommend scheduling the follow-up colonoscopy promptly — commonly within one to three months of a positive stool test. How much delay actually matters has been debated, but every study agrees on one thing: getting the colonoscopy done is what counts most.
What the guidelines recommend
Screening panels advise arranging the colonoscopy soon after a positive result rather than waiting indefinitely.
What the research says about waiting
Older evidence found that long delays raised risk.
📊 Clinical Data Point: In a large Kaiser Permanente study, the risk of colorectal cancer rose significantly when colonoscopy was delayed beyond about 9–10 months after a positive FIT — odds ratios of roughly 1.48 for any colorectal cancer and 1.97 for advanced-stage disease at 10 months, rising further after 12 months — Source: Corley et al., JAMA, 2017.
By contrast, a 2025 study of more than 374,000 people found no increase in colorectal cancer risk with delays of up to 24 months, and concluded that ensuring every positive result leads to a colonoscopy matters more than hitting a strict deadline — Source: Grancher et al., Gut, 2025.
The bottom line on timing
Sooner is reasonable and shortens the stressful wait; letting it drift indefinitely is not.
✅ Patient Action: Ask your gastroenterologist how soon they recommend your colonoscopy given your specific result and any symptoms — then book it rather than letting it slide.
What the follow-up colonoscopy involves — and what your results mean
A follow-up colonoscopy works the same as any screening colonoscopy: preparation the day before, a short sedated procedure, and a recovery period afterward.
Before: the prep
The bowel must be completely empty for the doctor to see clearly, which is what the prep accomplishes. Our guide on how to prepare for your colonoscopy walks through the options.
During: what to expect
You’ll be sedated and comfortable while a thin, flexible scope examines the colon; if the doctor finds a polyp, they can usually remove it during the same procedure. Removing a polyp is a good outcome — it can prevent a cancer from ever forming. If this is your first time, here is what to expect at your first colonoscopy.
After: what your results mean
The doctor may share initial findings the same day; any tissue removed is sent to a lab, and pathology results follow. A clean colonoscopy generally resets your screening clock, though your doctor sets your next interval based on what they find. Our guide to what your colonoscopy results mean explains the common findings.
When not to wait — and what to do if you get a bill
Two situations deserve faster action than a routinely scheduled colonoscopy: troubling symptoms, and a bill you may not actually owe.
Symptoms that mean don’t wait
⚠️ Clinical Warning: Rectal bleeding, unexplained weight loss, a persistent change in bowel habits, or ongoing abdominal pain warrant prompt medical attention regardless of when your colonoscopy is scheduled. Don’t wait for a future appointment if these symptoms appear — contact your clinician promptly.
If you’re unsure whether what you’re feeling needs urgent attention, you can check your symptoms as a starting point — not a substitute for a clinician.
If you receive a bill you don’t think you owe
If you’re billed for a follow-up colonoscopy that should carry no cost-sharing, you have options.
✅ Patient Action: Ask your plan to reprocess the claim with the correct screening coding. If it isn’t resolved, you can file a complaint with your state insurance commissioner. For commercial plans, federal guidance specifically prohibits cost-sharing for polyp removal during a screening colonoscopy — keep your test result and the billing codes used.
Positive Cologuard or FIT: frequently asked questions
1. Does a positive Cologuard mean I have cancer?
No. A positive Cologuard or FIT result means the test detected blood or abnormal DNA, not that cancer is present. Most positive results are caused by polyps or other minor bleeding, not cancer. A colonoscopy is needed to find the actual cause. Share your result with your clinician to arrange the follow-up.
2. Is the follow-up colonoscopy free after a positive Cologuard?
For most people, yes — the colonoscopy itself carries no cost-sharing. Federal rules require most commercial plans (plan years starting on or after May 31, 2022) and Medicare (since January 1, 2023) to cover a follow-up colonoscopy after a positive stool test as screening. Confirm your specific coverage with your insurer before the procedure.
3. Does Medicare cover a colonoscopy after a positive Cologuard?
Yes. Under a CMS rule effective January 1, 2023, traditional Medicare treats a colonoscopy after a positive stool test as a screening colonoscopy with no cost-sharing, billed with a KX modifier. If a polyp is removed, some coinsurance may apply during the phase-out period — confirm coding and any cost with your provider.
4. How accurate is Cologuard?
In its FDA approval study, the current Cologuard Plus test detected about 95% of colorectal cancers but only about 43% of advanced precancerous polyps, at roughly 94% specificity. That high cancer-detection rate is why a positive result is taken seriously — and why a colonoscopy, which also finds polyps the stool test can miss, is the next step.
5. How soon do I need a colonoscopy after a positive FIT?
Most guidelines recommend scheduling within about one to three months. Research on delay is mixed — older studies found higher risk beyond roughly 9–10 months, while a large 2025 study found no added risk up to 24 months. The consistent message is to complete the colonoscopy rather than let it drift. Ask your gastroenterologist about timing.
6. Can I just repeat the stool test instead of getting a colonoscopy?
No. Repeating a stool test cannot rule out what the first positive detected, and it delays the procedure that can find and remove the cause. After a positive FIT or Cologuard, a colonoscopy is the recommended follow-up. Discuss scheduling with your clinician or a gastroenterologist rather than re-testing.
7. What can cause a false-positive result?
A positive stool test doesn’t always mean cancer or even polyps. Bleeding from sources such as hemorrhoids or other irritation in the digestive tract can trigger a positive FIT, and stool DNA tests can flag abnormal markers that turn out to be benign. A colonoscopy clarifies what’s actually there. Your clinician can interpret your result.
8. If they find a polyp during the colonoscopy, will I be charged?
For commercial plans, federal guidance treats polyp removal during a screening colonoscopy as part of screening, with no cost-sharing. For traditional Medicare, a phase-out means some coinsurance may still apply when a polyp is removed (15% in 2023–2026, dropping to 0% by 2030), with the deductible waived. Confirm the billing with your provider.
9. What are the chances a positive result is actually cancer?
Most people with a positive Cologuard or FIT result do not have cancer. These tests are designed to flag anyone who needs a closer look, so they catch many people whose bleeding comes from polyps or other benign causes. Only a colonoscopy can determine the cause in your case. Your clinician will guide next steps.
10. Do I still need a colonoscopy if I feel completely fine?
Yes. Stool tests screen people who have no symptoms, so feeling fine doesn’t change a positive result — early colorectal cancer and precancerous polyps often cause no symptoms at all. The colonoscopy is what determines whether the positive reflects something that needs treatment. Don’t skip it because you feel well.
11. What should I do if I get a bill I don’t think I owe?
Ask your plan to reprocess the claim with the correct screening coding, since the follow-up colonoscopy should carry no cost-sharing for the procedure. If it isn’t resolved, you can file a complaint with your state insurance commissioner. Keep records of your test result and the billing codes used, and confirm coding with your provider’s office.
Your next step
A positive Cologuard or FIT result is a prompt, not a diagnosis. The colonoscopy that follows is the step that can find — and often prevent — a problem, and since 2023 it’s covered with no cost-sharing for the procedure under Medicare and most plans.
The most useful thing you can do today is schedule it, and confirm with the office that it will be coded as a screening follow-up. For the full picture of prep, cost, and results, see our complete colonoscopy guide.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.