On This Page – Quick Medical Summary
If a parent, brother, or sister has been diagnosed with colon cancer — or you keep seeing headlines about it striking younger adults — the question underneath the worry is simple: when do you need to be screened?
Here is the short answer this guide expands on. Most adults at average risk start screening at age 45. A family history of colorectal cancer can move that start date earlier, sometimes to 40 or younger, and can change how often you are screened.
Find your situation:
- One close relative diagnosed, or several affected relatives — your timeline likely changes; see exactly when to start below.
- A relative diagnosed very young, or a known syndrome like Lynch — you may need much earlier, more frequent screening.
- Not sure what even counts as “family history” — start by mapping who had cancer, what kind, and at what age.
What family history changes is when you start and how often you screen — not whether you are destined to get the disease.
ℹ️ Medical Disclaimer: This article is general education about colorectal cancer screening and family history. It does not diagnose disease, prescribe a specific test or treatment for you, or replace personalized care. Screening ages, intervals, and decisions about genetic testing should be set with a board-certified gastroenterologist or your primary care physician, who can weigh your individual history. If you have symptoms such as rectal bleeding, seek medical evaluation rather than waiting for routine screening.
How much does a family history of colon cancer raise your risk?
Having one first-degree relative — a parent, sibling, or child — with colorectal cancer roughly doubles your risk compared with someone who has no family history. That is a real increase, but “doubled” is far from a certainty.
📊 Clinical Data Point: One affected first-degree relative is associated with roughly 1.7–1.9 times the risk of colorectal cancer; two or more raise it to about 2.75 times. — Source: New England Journal of Medicine and a 2019 meta-analysis in Clinical Gastroenterology and Hepatology.
In plainer terms, a lifetime risk of about 1 in 20 rises to roughly 1 in 10 with a first-degree relative. It is also worth knowing that most colorectal cancers occur in people with no family history at all, per the CDC — which is why everyone is advised to screen at 45.
One relative versus several — and why their age at diagnosis matters
The numbers climb with more affected relatives and with younger diagnoses. A relative diagnosed under 50, or several relatives across the family, pushes your risk higher and can move your screening earlier. The age your youngest affected relative was diagnosed is one of the few facts that directly changes your timeline.
Does a grandparent, aunt, or cousin count?
They count for less. Grandparents, aunts, and uncles are second-degree relatives; cousins are third-degree. A single second- or third-degree relative usually means standard screening, though several affected relatives can still matter. You can estimate how your family history affects your risk before your appointment, then confirm it with your doctor.
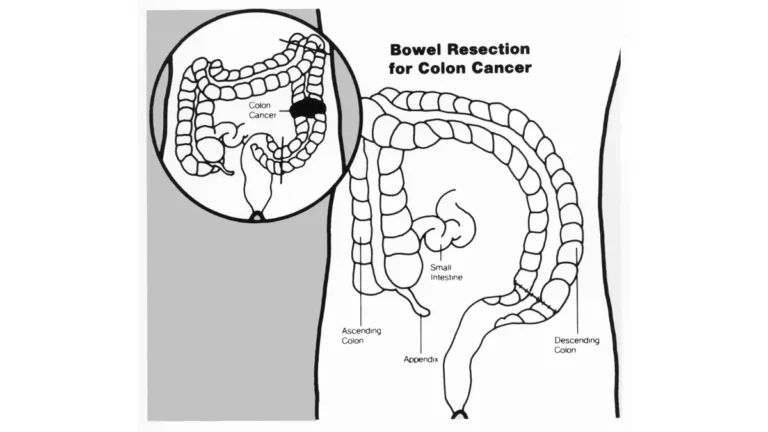
🔬 How It Works: Colorectal cancer usually begins as a polyp — a small growth in the colon lining. Some, called advanced adenomas, can slowly turn cancerous over years. That is why finding and removing them early matters, and why understanding how polyps relate to cancer risk is central to screening.
When should you start screening based on your family history?
For most adults at average risk, screening starts at 45. A family history can move that earlier — and the two facts that decide your timeline are how closely you are related to the affected person and how old they were at diagnosis.
📊 Clinical Data Point: The American Cancer Society’s 2026 guideline reaffirms that average-risk adults begin colorectal cancer screening at age 45 and continue through 75 (for those with at least 10 years of life expectancy). — Source: American Cancer Society, 2026.
Guideline-based starting points are summarized below. These reflect published recommendations, not a personalized plan — your doctor sets your actual timeline.
| Your family history | When guidelines suggest starting | How often | Preferred test |
|---|---|---|---|
| One first-degree relative with colorectal cancer or advanced polyps, diagnosed before 60 — or two or more first-degree relatives at any age | Age 40, or 10 years before your youngest affected relative’s diagnosis, whichever comes first | Every 5 years | Colonoscopy |
| A single first-degree relative diagnosed at 60 or older | Around age 40 | Average-risk intervals may apply (colonoscopy every 10 years, or annual stool testing) | Colonoscopy or stool-based test |
| One second- or third-degree relative only | Age 45 (standard) | Standard intervals | Any recommended test |
| A known hereditary syndrome | Much earlier — see the next section | More frequent | Colonoscopy |
Source: based on guidance from the American Cancer Society, the NCCN, and the American College of Gastroenterology. Confirm the specifics with your physician.
One relative diagnosed before 60, or two or more relatives at any age
This is the higher-risk group. Guidelines point to starting colonoscopy at 40, or 10 years before the earliest colorectal cancer in your family — whichever is sooner — and repeating it every 5 years rather than the standard 10. You can read how repeat screening intervals are set once your first result is in.
A single relative diagnosed at 60 or older
A later diagnosis in one relative raises your risk more modestly. Many guidelines still suggest beginning around age 40, but average-risk testing options may be appropriate in this situation. Your physician can tell you which applies.
Colonoscopy or a stool test — which is appropriate?
For higher family-history risk, colonoscopy is preferred because it both finds and removes polyps in a single procedure. Stool-based tests like FIT can play a role in lower-risk situations, but any positive stool test must be followed by a colonoscopy. See how stool-based tests compare to colonoscopy, and the full colonoscopy preparation, cost, and results walkthrough.
🩺 Physician Note: Family-history guidelines vary between organizations and are partly based on expert opinion, so two doctors may suggest slightly different timelines. Bringing the American Cancer Society’s current screening guideline to the conversation can help.
✅ Patient Action: Ask your primary care doctor or a gastroenterologist: “Given that my [relative] was diagnosed at [age], what start age and screening interval do you recommend for me?”
When a family pattern points to a hereditary syndrome
Most family history is not a hereditary syndrome. Inherited syndromes account for only about 5% of colorectal cancers; the rest of family-linked risk comes from a mix of genes and shared environment without a single identified mutation.
Lynch syndrome: the most common inherited cause
Lynch syndrome (also called HNPCC) is the most common inherited colorectal cancer syndrome.
📊 Clinical Data Point: Lynch syndrome accounts for about 2–4% of all colorectal cancers, and a carrier’s lifetime colorectal cancer risk ranges from roughly 10% to 80% depending on which gene is involved. — Source: American Cancer Society.
It is caused by changes in DNA mismatch repair (MMR) genes — MLH1, MSH2, MSH6, PMS2, or EPCAM. People with confirmed Lynch syndrome typically need colonoscopy every 1–2 years starting far earlier than usual, often in their twenties.
Familial adenomatous polyposis (FAP)
FAP is rarer — under 1% of colorectal cancers — and is caused by mutations in the APC gene. It produces hundreds to thousands of polyps, and without treatment the lifetime risk of colorectal cancer approaches 100%. Screening for those affected begins in childhood.
Red-flag family patterns worth raising with your doctor
Patterns that suggest an inherited syndrome include several affected relatives, colorectal cancer diagnoses before 50, or the same person or family having multiple related cancers. The American Cancer Society’s overview of inherited syndromes that raise colorectal cancer risk explains the criteria doctors use.
🩺 Physician Note: A hereditary syndrome is confirmed through genetic counseling and testing, not from family history alone. If your pattern fits, the next step is a referral — not a self-diagnosis.
How to map your family history before your appointment
The single most useful thing you can do before your appointment is arrive with your family history written down. Doctors set your screening timeline from a few specific facts, and “I think someone had it” is not enough to act on.
The four facts your doctor actually needs
For each relative who had cancer, try to find:
- Who they are and how you are related — parent, sibling, grandparent.
- What cancer it was — colon and rectal cancer count here; other cancers can still matter.
- What age they were diagnosed — the single fact that most often changes your start date.
- Which side of the family, and whether more than one relative was affected.
A simple worksheet with those four columns is enough to bring to your visit. (My Medicine Advisor offers a free downloadable Family Cancer History Worksheet built around exactly these fields.)
When to ask about genetic counseling
Genetic counseling is not for everyone with a family history. It is most worthwhile when the red-flag patterns appear: multiple affected relatives, early diagnoses, or several related cancers. A genetic counselor — not a search engine — can tell you whether testing makes sense. The CDC explains how genetic testing for Lynch syndrome works when a syndrome is suspected.
✅ Patient Action: Bring your completed history to your doctor and ask: “Based on this family history, do you recommend genetic counseling or earlier screening?” Once you have booked, review how to prepare for the procedure.
Why early-onset colon cancer makes family history matter more now
If your family history points to earlier screening, the timing matters more than it used to — because colorectal cancer is climbing in younger adults.
Colon cancer is rising in younger adults
📊 Clinical Data Point: Early-onset colorectal cancer (diagnosed before 50) has risen about 2% per year since the mid-1990s, including among adults in their twenties and thirties. — Source: American Cancer Society, 2025.
This trend is exactly why the American Cancer Society (2018) and the US Preventive Services Task Force (2021) lowered the average-risk start age from 50 to 45. For people with a family history, acting on the earlier timeline rather than waiting is the entire point.
Why catching it early changes everything
📊 Clinical Data Point: About 3 in 4 adults under 50 diagnosed with colorectal cancer are found at an advanced stage, while only about 1 in 5 adults aged 45–49 are up to date with screening. — Source: American Cancer Society, 2025–2026.
Caught early, colorectal cancer is far more treatable than when it is found late — which is the whole reason screening on the right schedule saves lives. The CDC’s colorectal cancer screening overview reinforces that screening is meant to find disease before symptoms appear. Younger readers can also see screening guidance for younger adults.
Don’t wait for your scheduled screening if you have these symptoms
Screening is designed for people who feel fine. If you already have symptoms, that is a different situation — it calls for evaluation now, not a wait for your next scheduled test.
⚠️ Clinical Warning: See a doctor promptly — regardless of your screening schedule — for rectal bleeding or blood in the stool, a persistent change in bowel habits, unexplained weight loss, or ongoing abdominal pain. These symptoms have many causes, but they warrant evaluation rather than waiting.
Symptoms that warrant prompt medical evaluation
The symptoms above do not mean you have cancer — most often they do not. But in a person with a family history, they are a reason to call a doctor and ask about a diagnostic colonoscopy rather than routine screening. You can review symptoms that warrant prompt evaluation and bring the results to your appointment.
Screening is for people without symptoms
Colorectal cancer often causes no symptoms early on, which is the whole reason screening on schedule matters — see why screening still matters without symptoms. When symptoms are present, doctors use diagnostic tests to find the cause. If you are under 50 with symptoms, colon cancer symptoms in younger adults is worth reading.
✅ Patient Action: If you have any of the warning symptoms, tell your doctor: “I have [symptom] and a family history of colon cancer — do I need a diagnostic colonoscopy now?”
Family history and colon cancer screening: common questions
1. At what age should I start colon cancer screening if I have a family history?
Guidelines generally recommend starting earlier than the average-risk age of 45. With one first-degree relative diagnosed before 60, or two or more at any age, the American Cancer Society and NCCN suggest beginning colonoscopy at 40 — or 10 years before your youngest affected relative’s diagnosis, whichever comes first. Confirm your exact timeline with your doctor.
2. Does a parent having colon cancer mean I will get it too?
No. A first-degree relative roughly doubles your risk, but doubled is far from certain — most people with a family history never develop colon cancer. Your risk rises with more affected relatives and younger diagnoses. A family history changes your screening timeline, not your fate. Discuss your personal risk with your doctor.
3. How much does family history increase my colon cancer risk?
One first-degree relative with colorectal cancer is associated with roughly 1.7 to 1.9 times the risk in studies. Two or more affected relatives, or a relative diagnosed young, raise it further. In everyday terms, a lifetime risk of about 1 in 20 becomes roughly 1 in 10 with a first-degree relative, which is why family history shapes screening.
4. If my relative was diagnosed young, when do I start screening?
The “10 years before the earliest diagnosis” rule matters most here. If your youngest affected first-degree relative was diagnosed at 45, guidelines point to starting colonoscopy around 35 rather than waiting for 40. Earlier diagnoses also raise your risk more. Your doctor can confirm the precise start age for your family history.
5. Do I need a colonoscopy, or is a stool test enough?
For higher family-history risk, colonoscopy is the preferred screening test because it both finds and removes polyps. Stool-based tests like FIT are an option in some lower-risk situations, but any positive stool test must be followed by a colonoscopy. Ask your doctor which test fits your specific family history.
6. What is the difference between familial and hereditary colon cancer?
“Familial” means colon cancer clusters in a family without a single identified gene — this covers most family history. “Hereditary” means a specific inherited gene change, like Lynch syndrome or FAP, found in about 5% of colorectal cancers. The two are screened differently, so it helps to know which pattern your family fits.
7. What is Lynch syndrome and how is it screened?
Lynch syndrome is the most common inherited colorectal cancer syndrome, accounting for about 2 to 4% of cases, caused by changes in mismatch-repair genes. People with confirmed Lynch syndrome typically need colonoscopy every 1 to 2 years starting much earlier than usual. Genetic counseling determines whether it applies to you. Discuss testing with your doctor or a genetic counselor.
8. How often should I get a colonoscopy if colon cancer runs in my family?
For the higher-risk scenario — a first-degree relative diagnosed before 60, or two or more affected relatives — guidelines recommend repeating colonoscopy every 5 years rather than the average-risk 10. Your interval can shift based on what each colonoscopy finds. Your gastroenterologist will set the right schedule for you.
9. Does a grandparent or cousin with colon cancer count?
They count for less. Grandparents, aunts, and uncles (second-degree) and cousins (third-degree) raise risk far less than a parent, sibling, or child. A single second- or third-degree relative usually means standard average-risk screening at 45, though multiple affected relatives can change that. Map your full family history and review it with your doctor.
10. Should I get genetic testing for colon cancer?
Genetic testing is not needed for everyone with a family history. It is most worthwhile when patterns suggest a syndrome: multiple affected relatives, diagnoses before 50, or several related cancers in the family. A genetic counselor can assess whether testing makes sense for you. Ask your doctor for a referral if your family pattern fits.
11. Can I have colon cancer with no symptoms?
Yes — colorectal cancer, especially early on, often causes no symptoms, which is exactly why screening on the right timeline matters. That said, symptoms like rectal bleeding, a persistent change in bowel habits, or unexplained weight loss warrant prompt evaluation regardless of your screening schedule. See a clinician promptly if these appear.
Your next step
A family history of colorectal cancer changes two things — when you start screening and how often — not whether you will get the disease. Most people with a family history never develop colon cancer, and screening on the right timeline is what keeps the odds in your favor.
So make the next step concrete. Write down who in your family had cancer, what kind, and at what age, then bring that to your primary care doctor or a gastroenterologist and ask about your start age. If a pattern suggests an inherited syndrome, ask for a genetic counseling referral. And if you have symptoms now, do not wait for a scheduled test. Knowing your timeline — and acting on it — is what protects you.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Family Medicine (2007); Preventive Medicine (2011) Experience: 18 years | Location: Charlotte, North Carolina Education: BS Biology, Wake Forest University (1999); MD, Wake Forest School of…

Board Certifications: Preventive Medicine (2010); Public Health & General Preventive Medicine (2010) Experience: 15 years | Location: Washington, DC Education: BA Public Policy, Georgetown University (2001); MD, George…

Board Certifications: Internal Medicine (2010); Clinical Pharmacology (2013) Experience: 15 years | Location: San Francisco, California Education: BS Molecular Biology, Caltech (2000); MD/PhD, UCSF School of Medicine (2007);…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.