On This Page – Quick Medical Summary
For most adults at average risk whose colonoscopy comes back clean, the standard interval is one colonoscopy every 10 years. But that “10-year rule” rests on two conditions many people don’t realize are part of it: you’re at average risk, and your last exam was normal. Change either one and your interval changes too.
Find your situation below:
- Normal result, average risk? The 10-year rule is for you — here’s why a full decade is safe.
- Polyps were removed? Your next colonoscopy is likely sooner — see the interval-by-finding guide.
- Family history, a hereditary syndrome, or IBD? You’re on a different schedule entirely.
- Wondering when to start or stop? Screening now begins at 45 and usually runs through 75.
- Having symptoms? Don’t wait for a scheduled exam — see why below.
This guide walks each path using current US screening guidelines, so you can see exactly where you fit. It builds on our complete guide to colonoscopy prep, cost, and results.
ℹ️ Medical Disclaimer: This article is general health education, not medical advice, and does not replace a diagnosis, screening recommendation, or care plan from a licensed clinician. Colonoscopy intervals, surveillance after polyps, hereditary-risk schedules, and decisions about screening after age 75 must be individualized — talk with your primary care provider or a board-certified gastroenterologist before acting on anything here. If you have symptoms such as rectal bleeding or a change in bowel habits, seek timely medical evaluation rather than waiting for a scheduled screening.
Why 10 years — the science behind the interval
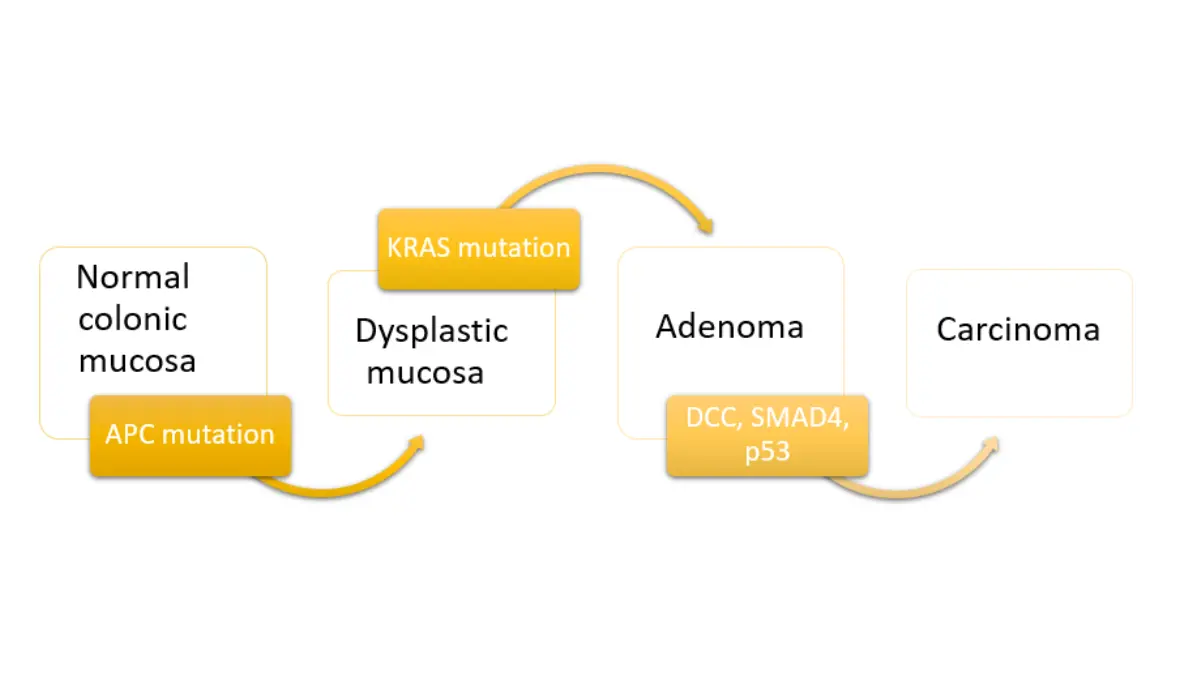
A colonoscopy can buy you a full decade because of how slowly most colorectal cancers begin. Nearly all start as a small growth called an adenoma — a precancerous polyp — that usually takes years to turn into cancer. A high-quality colonoscopy finds and removes those polyps during the same exam, which is why the test both detects cancer and helps prevent it.
🔬 How It Works: Most colorectal cancers follow the “adenoma-to-carcinoma” path — a benign polyp slowly accumulates genetic changes over roughly a decade before it can become malignant. Removing the polyp interrupts that process before cancer forms, so a clean colonoscopy effectively resets the clock.
That slow timeline is the reason a 10-year gap is considered safe for people at average risk. Studies following adults after a normal colonoscopy have found their risk of colorectal cancer stays low for many years afterward, which is the evidence behind the interval.
📊 Clinical Data Point: When colorectal cancer is found at an early, localized stage, the 5-year relative survival rate is greater than 90% in the US — Source: American Cancer Society, 2026.
Finding disease early — or preventing it outright by removing polyps — is exactly what regular screening is built to do, which is why keeping to your interval matters more than the number itself.
When the 10-year rule applies — and when it doesn’t
The 10-year rule has a precise audience: adults at average risk whose exam showed no concerning findings. Average risk means you don’t carry the factors that raise your odds of colorectal cancer.
You’re generally considered average risk if you do not have any of the following:
- A personal history of colorectal cancer or certain types of polyps
- A first-degree relative (parent, sibling, or child) with colorectal cancer or advanced polyps
- Inflammatory bowel disease (ulcerative colitis or Crohn’s disease)
- A hereditary syndrome such as Lynch syndrome or familial adenomatous polyposis (FAP)
- A history of radiation to the abdomen or pelvis
Major US guideline bodies — including the U.S. Preventive Services Task Force and the American Cancer Society — set the average-risk screening window at ages 45 to 75. For people in that window whose colonoscopy is normal, repeat screening every 10 years is the standard documented across current CDC and Task Force guidance.
🩺 Physician Note: A common point of confusion is assuming “every 10 years” applies to all screening. It doesn’t — the 10-year interval is specific to colonoscopy. Stool-based tests (a FIT done yearly, or a stool-DNA test every 1–3 years) and CT colonography (every 5 years) each run on their own schedule.
If any average-risk criterion doesn’t fit you, your interval is set differently — that’s the next two sections.
How often if polyps were found
If your colonoscopy found and removed polyps, your next one is usually sooner than 10 years — and how much sooner depends on what was found. The U.S. Multi-Society Task Force on Colorectal Cancer sets these surveillance intervals based on the type, size, and number of polyps removed.
These intervals assume a high-quality baseline exam — adequate prep, a complete examination, and removal of all polyps found. Your pathology report and your endoscopist’s recommendation are what actually determine your timing; the table below is general education, not a personal schedule.
| What was found (average-risk adult) — key clinical detail | Typical interval to next colonoscopy |
|---|---|
| 1–2 small tubular adenomas (under 10 mm) | 7–10 years |
| 3–4 small tubular adenomas (under 10 mm) | 3–5 years |
| 5–10 small tubular adenomas (under 10 mm) | 3 years |
| An advanced adenoma (10 mm or larger, villous features, or high-grade dysplasia) | 3 years |
| More than 10 adenomas on a single exam | Within 1 year |
| 1–2 small sessile serrated polyps (under 10 mm) | 5–10 years |
Source: U.S. Multi-Society Task Force on Colorectal Cancer, 2020 post-polypectomy surveillance guidelines. Use as general guidance only — your individual interval is set by your care team.
One change worth knowing: in 2020 the interval for 1–2 small adenomas was lengthened from the older 5-year mark to 7–10 years, so a “5 years” you may remember from a past exam can be outdated. If you were told 3 or 5 years instead of 10, the type or number of your polyps is usually why — reading your colonoscopy pathology report and understanding what your polyp type means for cancer risk can help it make sense.
✅ Patient Action: Before you leave your follow-up appointment, ask your gastroenterologist: “Based on my polyp type, size, and number, what surveillance interval are you recommending, and why?” — then get that interval in writing.
How often if you’re at higher risk
Higher-risk readers shouldn’t apply the 10-year rule — these groups generally start earlier and screen more often, with colonoscopy specifically rather than stool tests. The exact schedule depends on the reason for the elevated risk.
Family history. If you have a first-degree relative who had colorectal cancer or advanced polyps, guidelines from the American College of Gastroenterology suggest beginning at age 40 — or 10 years before your relative’s age at diagnosis, whichever comes first — and screening more frequently than every 10 years.
Hereditary syndromes. Conditions like Lynch syndrome or familial adenomatous polyposis call for much earlier and far more frequent colonoscopy — sometimes starting in the teens or twenties, often roughly every 1–2 years. As the American Cancer Society’s screening recommendations note, the specifics depend on which syndrome you have.
Inflammatory bowel disease. People with ulcerative colitis or Crohn’s colitis generally begin surveillance colonoscopy about 8 years after diagnosis, then repeat every 1–3 years depending on prior findings and other risk factors.
⚠️ Clinical Warning: Higher-risk schedules are individualized and can shift with new findings or new family information. Don’t set your own interval from these general ranges — a gastroenterologist, and for hereditary syndromes a genetic counselor, should determine your plan.
✅ Patient Action: If colorectal cancer runs in your family, ask: “Given my family history, at what age should I start, and how often should I be screened?” You can also assess your inherited colorectal cancer risk before that conversation.
When to start — and when you can stop
Two more questions complete the picture: when to begin, and when you can stop. Both bookends shifted in recent years.
Starting age. Screening now begins at age 45 for adults at average risk — lowered from 50 by the U.S. Preventive Services Task Force in 2021, a change driven by rising colorectal cancer rates in younger adults. The American Cancer Society reaffirmed the age-45 start in its 2026 guideline update.
Stopping age. Routine screening generally continues through age 75 for people in good health. For ages 76 to 85, it becomes an individual decision weighing overall health, life expectancy, and prior screening history. The American Cancer Society advises that people over 85 no longer undergo colorectal cancer screening.
🩺 Physician Note: “When can I stop?” rarely has a single-age answer after 75. Guidelines frame it around whether you’re likely to live long enough to benefit — the payoff from removing a polyp generally takes 7 to 10 years to materialize, which is why the calculation changes with age and health.
Whenever your next colonoscopy comes due, knowing how to get ready for it makes the day far smoother.
Don’t wait for your next colonoscopy if this happens
Your screening interval assumes you feel well. New symptoms are a different situation — they call for evaluation now, not at your next scheduled exam, because a screening schedule is not the same as checking out a problem.
See a clinician promptly if you notice:
- Rectal bleeding or blood in the stool
- A persistent change in bowel habits — diarrhea, constipation, or a change in stool shape
- Unexplained weight loss
- Ongoing abdominal pain or cramping
- Unexplained iron-deficiency anemia
These symptoms have many possible causes, most of them not cancer — but they shouldn’t be filed away until a future colonoscopy. Learning the bowel cancer symptoms you should never ignore can help you decide how quickly to act.
⚠️ Clinical Warning: If you have rectal bleeding or a marked change in bowel habits, contact your doctor rather than waiting for a scheduled screening or trying to self-diagnose. A symptom evaluation may call for a colonoscopy sooner than your routine interval.
✅ Patient Action: If any of these symptoms appear, tell your provider directly: “I’m having [symptom] — should I be evaluated before my next scheduled colonoscopy?”
Colonoscopy frequency: common questions
1. How often should you get a colonoscopy after 50?
For average-risk adults with a normal result, the interval is every 10 years, and that holds from age 45 through 75. Being over 50 doesn’t shorten it by itself — what changes the interval is finding polyps or having a higher-risk history. Confirm your personal timing with your clinician.
2. Is a colonoscopy every 10 years really enough?
For average-risk adults with a clean exam, yes. Most colorectal cancers grow from polyps over roughly a decade, and removing those polyps during colonoscopy resets the clock, with research showing risk stays low for years afterward. Polyps or higher-risk factors are what call for a shorter interval.
3. How often if you have a family history of colon cancer?
A first-degree relative with colorectal cancer or advanced polyps generally means starting earlier — around age 40, or 10 years before your relative’s diagnosis age — and screening by colonoscopy more often than every 10 years. The exact interval depends on your specifics, so have your gastroenterologist set it.
4. How soon do you need a repeat colonoscopy if polyps were found?
It depends on the type, size, and number. One or two small adenomas usually means 7–10 years; three or four means 3–5 years; an advanced adenoma means about 3 years; more than 10 means within a year. Your pathology report and endoscopist determine your interval.
5. At what age can you stop having colonoscopies?
Routine screening generally continues through 75 for healthy adults. Between 76 and 85 it’s an individual decision based on health, life expectancy, and prior screening, and the American Cancer Society advises stopping after 85. Discuss your own situation with your clinician.
6. Why did my doctor say 3 or 5 years instead of 10?
Almost always because polyps were found and removed. Three or four small adenomas point to a 3–5 year interval, and an advanced adenoma points to about 3 years, under current surveillance guidelines. The 10-year rule applies only to average-risk adults whose exam was completely normal.
7. How often with ulcerative colitis or Crohn’s disease?
People with inflammatory bowel disease affecting the colon generally start surveillance colonoscopy about 8 years after diagnosis, then repeat every 1–3 years depending on prior findings and risk factors. Stool tests aren’t a substitute here — colonoscopy is used specifically. A gastroenterologist should set your schedule.
8. Does the 10-year rule apply if I had a stool test instead?
No. The 10-year interval is specific to colonoscopy. Stool-based tests run more often — a FIT yearly, a stool-DNA test every 1–3 years — and CT colonography is every 5 years. A positive result on any non-colonoscopy test is followed by a colonoscopy to complete screening.
9. Can you safely wait longer than 10 years?
For average-risk adults with a normal colonoscopy, 10 years is the recommended maximum interval, not a minimum — going beyond it isn’t the standard. Your clinician may suggest a different interval based on your exam quality and findings, so confirm your timing rather than extending it on your own.
10. What symptoms mean I shouldn’t wait for my scheduled colonoscopy?
Rectal bleeding, a persistent change in bowel habits, unexplained weight loss, ongoing abdominal pain, or unexplained iron-deficiency anemia all warrant prompt evaluation regardless of when your next screening is due. Most causes aren’t cancer, but they need to be checked. Contact your provider rather than waiting.
11. How often should you have a colonoscopy after 75?
There’s no automatic interval after 75. Screening between 76 and 85 is decided case by case, weighing your health, life expectancy, and screening history, because the benefit of removing a polyp takes years to materialize. Your clinician can help you decide whether continuing makes sense.
Your next colonoscopy: the bottom line
The rule is simpler than it first looks. If you’re at average risk and your colonoscopy was normal, every 10 years is the standard. If polyps were found, expect a shorter interval set by what was removed. If you have a family history, a hereditary syndrome, or IBD, you’re on an earlier, more frequent schedule. And no matter when your next exam is due, new symptoms like rectal bleeding mean seeing a doctor now, not later.
The most useful next step is to confirm your own interval. Pull up your last colonoscopy results, note what they said, and ask your clinician exactly where you fit — because only your care team can set the schedule that’s right for you.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.