On This Page – Quick Medical Summary
You had a colonoscopy, and now there’s a colonoscopy pathology report full of words like adenoma, dysplasia, and tubulovillous — and your stomach dropped. Take a breath. For most people, this report describes a polyp that was found, removed, and is either benign or precancerous — not a cancer diagnosis.
Where you are right now points you to what you need:
- Your report lists a polyp that was removed and you want to know what it was — start with the polyp-types and dysplasia sections below.
- You’re still waiting on results — the next section explains how the report is made and the timeline.
- You see high-grade dysplasia and you’re frightened — the dysplasia section explains, plainly, why that is not cancer.
- Your report mentions carcinoma or invasive cells — the red-flags section tells you exactly what to ask, and to call your doctor promptly.
This guide translates every line into plain English and tells you what happens next.
ℹ️ Medical Disclaimer: This article is general health education — not medical advice, a diagnosis, or a treatment or screening recommendation for any individual. The pathology terms and surveillance intervals described here are general guidelines; only your gastroenterologist can interpret your report and set your personal follow-up schedule, accounting for your full findings, bowel-prep quality, and personal and family history. If your report mentions cancer or invasive cells, contact your doctor promptly. Always consult a board-certified gastroenterologist or your care team before acting on your results.
What a colonoscopy pathology report actually is
A pathology report is the written, microscopic analysis of any tissue your doctor removed or sampled during the procedure. It is separate from the verbal “everything looked fine” you may have heard in recovery — that was the visual finding; this is the microscopic one.
How your tissue becomes a report
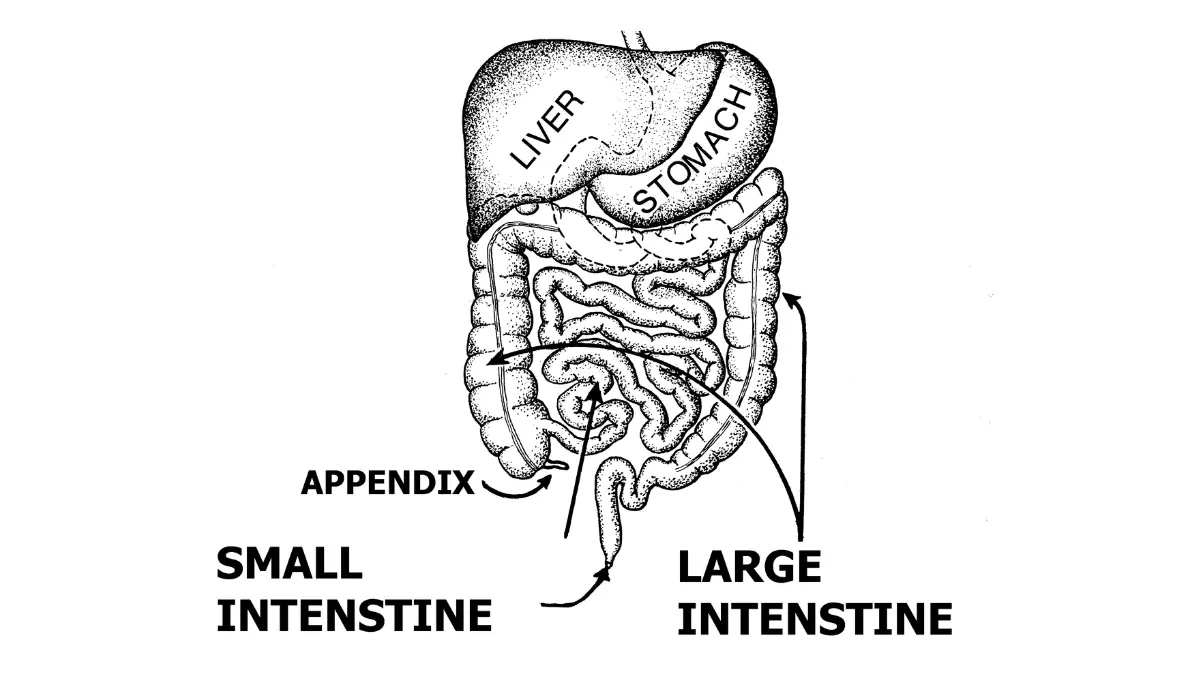
During the colonoscopy, the doctor removes polyps or takes a biopsy, then sends the tissue to a pathologist — a physician who reads it under a microscope. The pathologist identifies what each piece of tissue is and writes it up, which is the report now in your hands. For a refresher on the procedure itself, see what happens during the colonoscopy.
The main parts of the report
Most reports cover four things: the type of polyp or tissue, its growth pattern, whether it shows dysplasia (abnormal cells), and whether it was completely removed (the margins). To see how this fits your overall picture, read how each finding fits your colonoscopy results.
How long results take
Results usually take a few days to about two weeks, depending on the lab and the complexity of your case. If you haven’t heard back within the window your clinic gave you, call and ask — and see the typical biopsy-results timeline for what to expect.
🔬 How It Works: A pathologist stains thin slices of your tissue and examines the shape and arrangement of the cells under magnification. That microscopic view — not the camera during your colonoscopy — is what determines whether a polyp was benign, precancerous, or cancerous.
Polyp types on your report, explained in plain English
Does an adenoma on your report mean you have cancer? No. An adenoma is a precancerous polyp — it can slowly turn into cancer over years, which is exactly why finding and removing it lowers your risk. For the bigger picture, see how colon polyps relate to cancer risk.
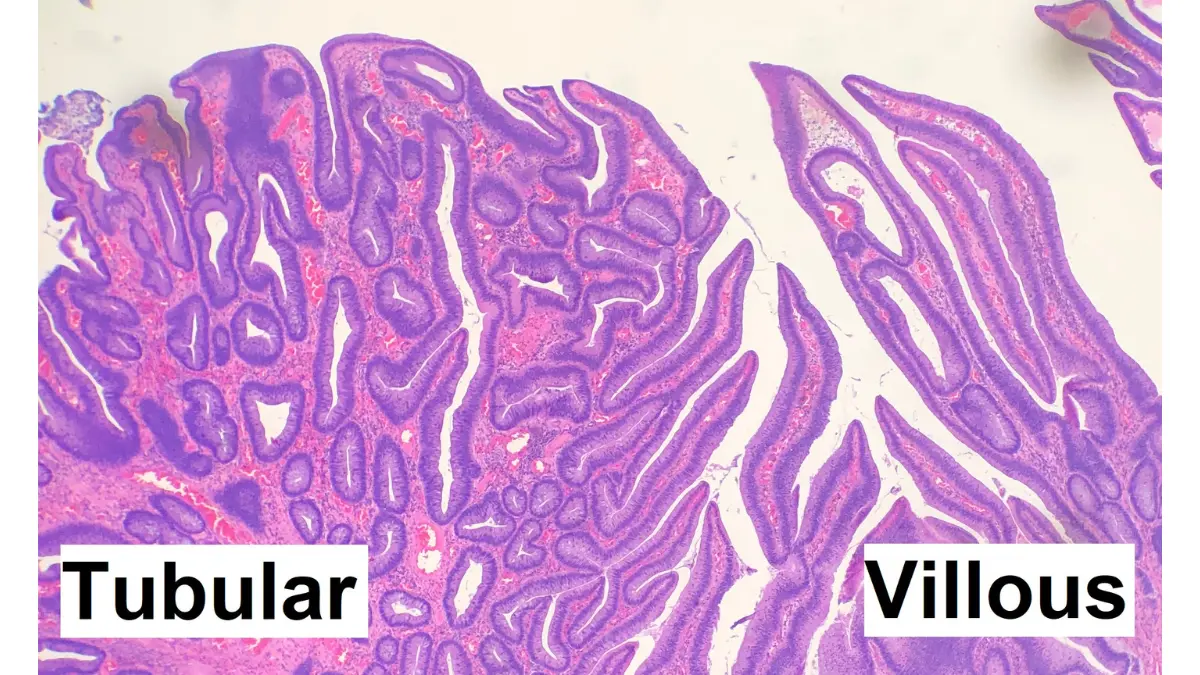
Adenomas: tubular, tubulovillous, villous
These words describe a polyp’s growth pattern under the microscope. Most small adenomas are tubular; larger ones are more often villous (a finger- or leaf-like pattern), and many are a mix called tubulovillous. Villous and larger adenomas are more likely to contain cancer cells — but once a polyp is fully removed, the growth pattern mainly affects when your next colonoscopy is due. This is per the American Cancer Society’s guide to colon polyp pathology.
Serrated polyps: sessile serrated and traditional serrated
Serrated polyps have a saw-tooth look under the microscope. The two precancerous kinds — sessile serrated and traditional serrated adenomas — are not cancer, but they need to be removed completely. A hyperplastic polyp, by contrast, is typically benign and usually not a cause for concern, especially the small ones in the lower colon. For a plain-language primer, see an overview of colon polyps from MedlinePlus.
What ‘sessile’ and ‘pedunculated’ mean
These describe shape, not danger. Sessile means flat and broad-based; pedunculated means growing on a stalk. Your report may use either to describe how a polyp sat against the colon wall. One common mix-up is confusing a polyp’s type (adenoma, serrated, hyperplastic) with its growth pattern (tubular, villous) — they answer different questions, and your report may list both.
What ‘dysplasia’ and ‘clear margins’ mean on your report
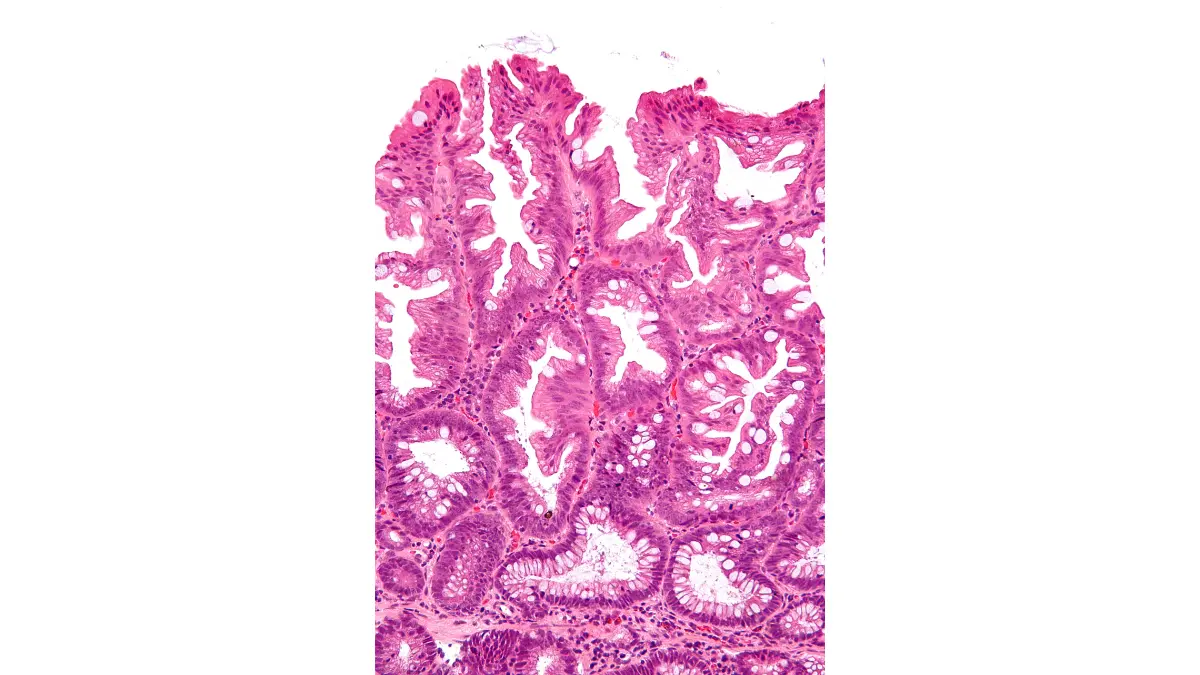
Dysplasia is one of the most misread words on a pathology report. It means cells look abnormal under the microscope — not that they are cancer.
Low-grade vs high-grade dysplasia
Dysplasia is graded by how abnormal the cells look. Low-grade dysplasia is mildly abnormal and does not look much like cancer. High-grade dysplasia is more abnormal and usually means your next colonoscopy will be sooner.
Why high-grade dysplasia is not cancer
This is worth saying plainly: high-grade dysplasia is an advanced precancerous change, not cancer. It means the polyp was caught and removed at exactly the stage screening is designed to catch. For how this and other results read, see what each colonoscopy finding means.
‘Margins’ and ‘completely removed’ — the line that matters most
The single most reassuring phrase on your report is that the polyp was removed completely with clear margins — meaning no polyp tissue was seen at the cut edges. If a polyp could not be fully removed, your doctor may recommend a repeat procedure.
If your report mentions cancer
If you see adenocarcinoma, invasive, or infiltrating, those words need a doctor’s interpretation, not an internet search — they do not reveal your outlook on their own.
✅ Patient Action: Ask your gastroenterologist two specific questions: “Was every polyp removed completely?” and “Does any finding on my report change when I need my next colonoscopy?”
🩺 Physician Note: Patients often read “high-grade dysplasia” as a cancer diagnosis. Current guidance treats it as a high-risk precancerous finding — managed with a shorter follow-up interval, not cancer treatment.
When you’ll need your next colonoscopy
When your next colonoscopy is due depends on exactly what your pathology report shows. The table below reflects current U.S. surveillance guidelines for average-risk patients.
Your finding and your next colonoscopy
| Finding on your report | Typical next colonoscopy | What it means |
|---|---|---|
| Normal exam, no polyps | 10 years | Routine screening continues |
| 1–2 small tubular adenomas (<10 mm, low-grade) | 7–10 years | Low-risk finding |
| 3–4 small tubular adenomas (<10 mm) | 3–5 years | Slightly higher risk |
| 5–10 adenomas | 3 years | Higher risk |
| Any adenoma ≥10 mm | 3 years | “Advanced” adenoma |
| Adenoma with villous/tubulovillous features | 3 years | “Advanced” adenoma |
| Adenoma with high-grade dysplasia | 3 years | “Advanced” adenoma |
| More than 10 adenomas | Within 1 year | Doctor may check for a hereditary syndrome |
| Large polyp removed in pieces (piecemeal, ≥20 mm) | About 6 months | Confirms nothing was left behind |
| 1–2 small sessile serrated polyps (<10 mm) | 5–10 years | Lower-risk serrated finding |
| Sessile serrated polyp ≥10 mm or with dysplasia; or a traditional serrated adenoma | 3 years | Higher-risk serrated finding |
| Small hyperplastic polyps (lower colon, <10 mm) | 10 years | Typically benign |
Source: U.S. Multi-Society Task Force on Colorectal Cancer post-polypectomy surveillance recommendations (Gupta et al., 2020). See the U.S. Multi-Society Task Force recommendations.
What ‘advanced’ and ‘low-risk’ adenoma mean for timing
An advanced adenoma is one that is 10 mm or larger, has villous features, or contains high-grade dysplasia — any of these generally means a 3-year interval. A low-risk adenoma is one or two tubular adenomas under 10 mm with low-grade dysplasia, which can usually wait 7–10 years.
Why your doctor’s date may be different
These are guideline ranges, not your personal schedule. Your gastroenterologist may choose a sooner date based on how complete your bowel prep was, whether every polyp was fully removed, and your family history — so good bowel prep genuinely affects your results. Dreading the next one? Here’s what your next colonoscopy actually involves.
✅ Patient Action: Confirm your interval directly. Ask: “Based on my exact findings and how complete my prep and removal were, what is my recommended date — and should it be sooner than the general guideline?”
What your results mean for your colorectal cancer risk
Polyps are among the most common findings at colonoscopy — finding and removing them is the whole point of the test. A precancerous polyp on your report usually means the screening did its job.
Why removing polyps lowers your risk
Most colorectal cancer develops slowly, over years, from a precancerous adenoma — a process called the adenoma-carcinoma sequence. Removing the polyp interrupts that path before cancer can form, which is the mechanism behind the CDC’s colorectal cancer screening basics.
Why your next-scope date matters at any age
Screening matters across adulthood now, not just after 65.
📊 Clinical Data Point: About 158,850 new colorectal cancer cases and 55,230 deaths are projected in the U.S. in 2026, and incidence in adults under 50 has been rising roughly 3% per year — Source: American Cancer Society, Colorectal Cancer Statistics, 2026. See current colorectal cancer statistics.
That rising trend in younger adults is why keeping your follow-up date matters, whatever your age — and why it helps to know colon cancer symptoms in younger adults. To weigh your personal and family-history risk, you can estimate your colorectal cancer risk factors.
Disclosure: some links on this site are affiliate links. Between recommended colonoscopies, average-risk adults sometimes use at-home stool-based screening tests — a general option, not a substitute for the surveillance colonoscopy a polyp finding calls for. Ask your doctor what fits your situation.
Red flags and questions to ask your doctor
Most reports describe benign or precancerous findings that were fully handled during your colonoscopy. A few results, though, warrant a prompt call.
Report phrases that mean ‘call your doctor’
Reach out to your gastroenterologist soon if your pathology report includes any of these: a polyp that could not be completely removed; a large polyp removed in pieces (piecemeal); the phrase indefinite for dysplasia; or any mention of carcinoma or invasive cells.
What an incomplete or piecemeal removal means
If a polyp wasn’t fully removed, or a large one came out in fragments, your doctor may schedule an earlier repeat colonoscopy to confirm nothing was left behind. This is routine caution, not a sign something went wrong.
⚠️ Clinical Warning: A report that mentions carcinoma, adenocarcinoma, or invasive cells needs in-person interpretation by your doctor. Do not try to estimate your stage or outlook from the report alone — those words do not carry that information by themselves.
✅ Patient Action: Bring three questions to your follow-up: “Was every polyp removed completely?” “Do my results change my next-scope date?” and “Do my findings suggest I need genetic or family screening?”
Colonoscopy pathology report: frequently asked questions
1. Is a colonoscopy pathology report the same as a biopsy result?
Essentially, yes. Your colonoscopy pathology report is the pathologist’s microscopic analysis of the polyp tissue or biopsy taken during your procedure. It describes what the tissue is, how it grows, whether it shows dysplasia, and whether it was completely removed. It’s separate from the visual “everything looked normal” your doctor may mention in recovery.
2. How long does it take to get colonoscopy pathology results?
Results usually take a few days to about two weeks, depending on the lab and how complex your case is. Your colonoscopy pathology report goes to your doctor, who then shares the findings with you. If you haven’t heard back within the timeframe your clinic gave you, call and ask for an update.
3. Does an adenoma on my colonoscopy pathology report mean I have cancer?
No. An adenoma is a precancerous polyp, not cancer — it can slowly turn into cancer over years, which is why removing it lowers your risk. Once it’s fully removed, the type mainly affects your follow-up timing. Discuss your specific colonoscopy pathology report with your gastroenterologist to confirm what it means for you.
4. What does high-grade dysplasia mean on a colonoscopy pathology report?
Dysplasia means cells look abnormal under the microscope. High-grade means more abnormal than low-grade — but high-grade dysplasia is still not cancer. It usually means an earlier follow-up colonoscopy rather than cancer treatment. If your colonoscopy pathology report lists high-grade dysplasia, ask your gastroenterologist which follow-up schedule they recommend for you.
5. Is a sessile serrated polyp dangerous?
A sessile serrated polyp is precancerous, so it’s removed completely, but it is not cancer. Guidelines generally suggest a 3-year follow-up if it’s 10 mm or larger or shows dysplasia, and longer intervals for small ones. Your doctor sets your exact timing based on your full colonoscopy pathology report and history.
6. Do hyperplastic polyps need follow-up?
Hyperplastic polyps are typically benign. For small ones in the lower colon, guidelines recommend the routine 10-year interval; larger hyperplastic polyps (10 mm or more) may warrant a 3–5-year follow-up. Your gastroenterologist confirms the timing that fits your colonoscopy pathology report and personal risk factors.
7. What does ‘clear margins’ or ‘completely removed’ mean on my report?
It’s the most reassuring line on the report. “Clear margins” or “completely removed” means the pathologist saw no polyp tissue at the cut edges, so the whole polyp was taken out. If your colonoscopy pathology report says a polyp wasn’t fully removed, your doctor may recommend a repeat procedure to finish the job.
8. When will I need my next colonoscopy after polyps are found?
It depends on your findings: roughly 7–10 years for one or two small tubular adenomas, and about 3 years for higher-risk findings like an adenoma 10 mm or larger, villous features, or high-grade dysplasia. These are guideline ranges — your gastroenterologist sets your personal date from your colonoscopy pathology report.
9. What is an ‘advanced adenoma’ on a pathology report?
An advanced adenoma is one that’s 10 mm or larger, has tubulovillous or villous features, or contains high-grade dysplasia. It’s still precancerous, not cancer, but it generally means a shorter follow-up — usually about 3 years. Ask your gastroenterologist how the finding on your colonoscopy pathology report affects your schedule.
10. What if my colonoscopy pathology report says no polyps were found?
That’s a normal, reassuring result. For average-risk people with a normal, high-quality colonoscopy, guidelines recommend the next exam in about 10 years, though personal and family history can shorten that. Confirm your interval with your doctor, since your colonoscopy pathology report is only one part of your overall risk picture.
11. Should I see a specialist about my colonoscopy pathology report?
For most benign or precancerous findings, the gastroenterologist who did your procedure manages follow-up. See them promptly if your colonoscopy pathology report mentions an incomplete or piecemeal removal, “indefinite for dysplasia,” or any cancer or invasive cells. When anything is unclear, ask them to walk you through the report line by line.
The bottom line on your report
A polyp found and removed is usually a prevention success, not a cancer diagnosis — and now you can read the words that describe it. You know what your polyp type means, that dysplasia is not cancer, and roughly when your next colonoscopy is due.
The one thing worth doing today: write down your recommended follow-up date and keep it somewhere you’ll see it. For the wider context, here’s the full colonoscopy guide. Then bring any remaining questions to your gastroenterologist — they have your complete picture.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.