On This Page – Quick Medical Summary
If your doctor has recommended colon cancer screening — or you’ve been avoiding the standard colonoscopy because of the sedation, the scope, or a rough past experience — a virtual colonoscopy can sound like an easier path. It’s a real, guideline-accepted option, not a shortcut. But “easier” and “right for you” aren’t always the same thing.
Here’s how to use this guide:
- Weighing both tests for routine screening? Start with the pros and cons side by side.
- Worried mainly about accuracy? Skip to how accurate it is.
- Focused on cost and coverage? A 2025 Medicare change may affect you — see cost and coverage.
- Researching for an older or frail parent, or someone on blood thinners? The decision and risk sections are for you.
Our complete guide to colonoscopy covers prep, cost, and results in full. The honest answer to “which is better” is: it depends on you — and the sections below make that concrete.
ℹ️ Medical Disclaimer: This article is general education about colorectal cancer screening options, accuracy, cost and coverage, and procedure risks. It isn’t a diagnosis, a treatment recommendation, or advice for your situation, and it doesn’t replace your own clinician. Which test to have, how often, and what to do about any finding should be decided with a board-certified gastroenterologist or primary care provider who knows your personal and family history. Insurance coverage varies by plan — confirm your benefits before scheduling.
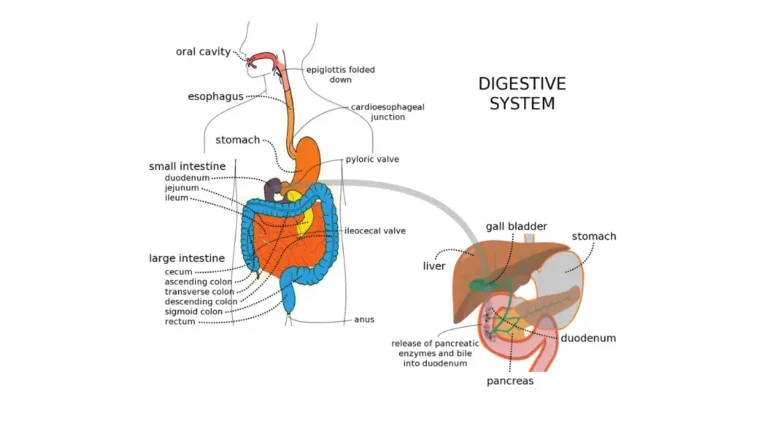
How a virtual colonoscopy works — and how it differs from the traditional test
A virtual colonoscopy and a traditional colonoscopy examine the same thing — the lining of your colon and rectum — but reach it in completely different ways.
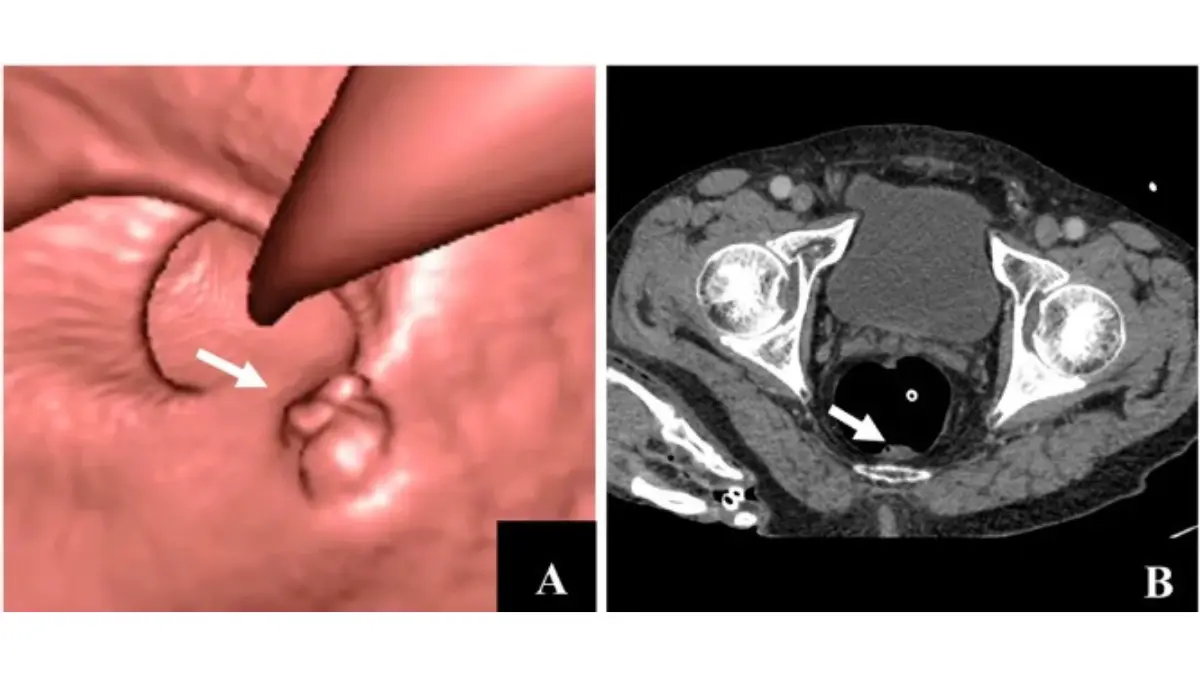
Adapted from Wikimedia Commons CT colonography of a rectal mass, licensed under CC BY 4.0.
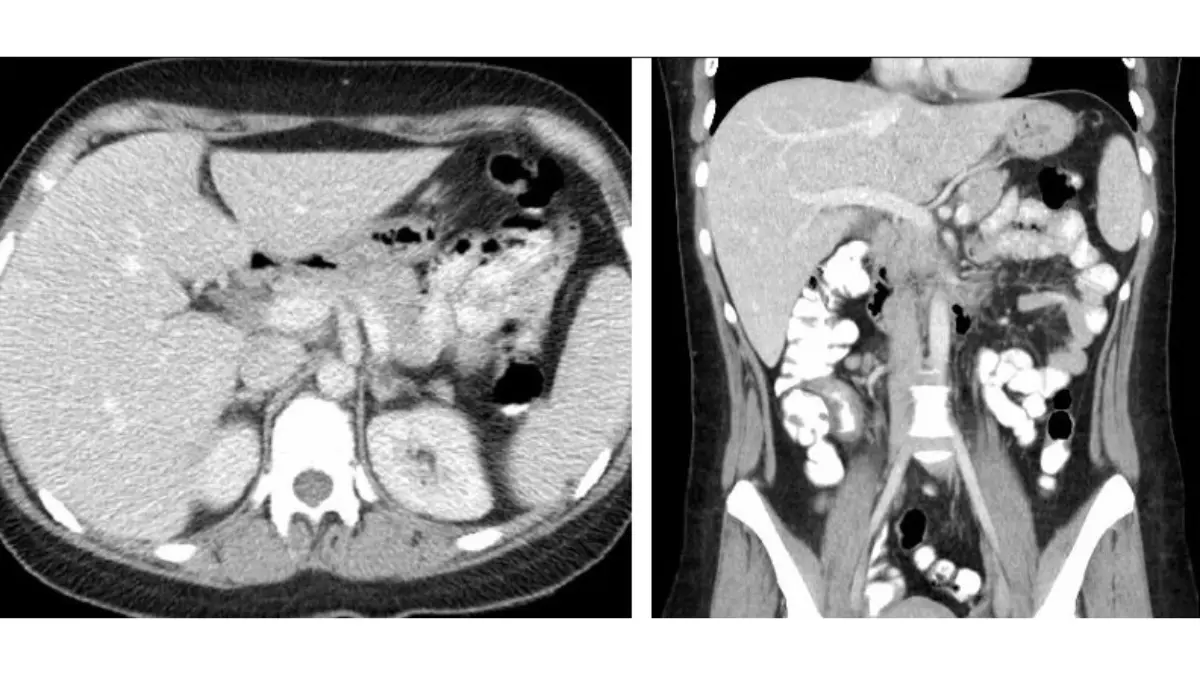
How a virtual colonoscopy (CT colonography) works
A CT colonography, the medical name for a virtual colonoscopy, uses a CT scanner to image your cleaned-out colon, then assembles the pictures into 2D and 3D views a radiologist reviews for polyps. No scope is passed through the colon — a thin tube just inside the rectum inflates it with carbon dioxide so the walls spread apart, and the scan takes only minutes.
🔬 How It Works: On a scan, leftover stool can look like a polyp. So the prep includes a “tagging” drink that makes any residue show up differently from tissue — letting the radiologist tell stool from a real growth. A plain-language overview from MedlinePlus walks through the options.
How it differs from a traditional colonoscopy
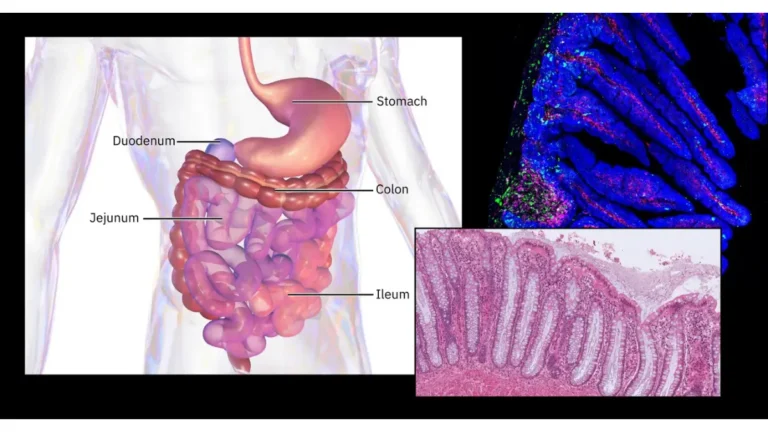
A traditional (optical) colonoscopy uses a flexible scope with a camera that a gastroenterologist advances through the colon while you’re sedated (here’s what that sedation involves). The defining difference: that scope can also remove polyps or take biopsies in the same session. A virtual colonoscopy can only see — it can’t sample or remove anything, a distinction that shapes nearly every pro and con below.
Adapted from Unsplash Human intestines and torso, licensed under the Unsplash License.
Virtual vs. traditional colonoscopy: the pros and cons side by side
The fastest way to weigh the two is to put every trade-off in one place.
| Factor | Virtual colonoscopy (CT colonography) | Traditional colonoscopy | Best for the patient who… |
|---|---|---|---|
| Sedation | None — you stay awake, drive yourself home | Sedation/anesthesia; you need a ride home | …can’t be sedated or wants no downtime |
| Time & recovery | ~Few-minute scan; back to normal the same day | Half-day visit plus recovery from sedation | …needs minimal time away |
| Removing polyps | Cannot remove or biopsy — see-only | Removes polyps and biopsies in the same visit | …wants one-and-done if a polyp is found |
| Large polyps & cancer | Strong — ~90% of patients with a ≥10 mm lesion flagged | Reference standard | …wants reliable detection of significant lesions |
| Small/flat polyps | Lower; lesions ≤5 mm usually aren’t reported | Higher | …wants the most sensitive small-polyp detection |
| Bowel prep | Same cleansing prep, plus a tagging drink | Same cleansing prep | (prep is similar either way) |
| Screening interval | Every 5 years if normal | Every 10 years if normal | …prefers a longer gap (favors the scope) |
| Radiation | Low-dose CT (~7–8 mSv) | None | …wants to avoid radiation (favors the scope) |
| Blood thinners | Usually no need to stop | May need to pause anticoagulants | …takes blood thinners |
| Perforation risk | Very low | About 1 in 1,000 | …wants the lowest procedural risk |
Sources: USPSTF (2021) for screening intervals; ACRIN National CT Colonography Trial (NEJM, 2008) for detection figures; AAFP review (2021) for radiation dose and perforation rate; RSNA/ACR RadiologyInfo.org for procedure details.
Where the virtual colonoscopy wins
If sedation, time off work, or blood thinners are your main obstacles, the virtual test has real advantages: no sedation (no IV, no grogginess, no ride home), a much lower risk of bowel perforation, and usually no need to stop anticoagulants first.
Where the traditional colonoscopy wins
The scope both finds and fixes in one visit — a polyp usually comes out then and there, with no second procedure. It’s also more sensitive for small and flat polyps, and a normal result buys ten years before the next screening instead of five. The American Cancer Society’s overview of screening tests shows where each fits.
How accurate is a virtual colonoscopy?
For the lesions that matter most — large polyps and cancers — a virtual colonoscopy performs well. In the large U.S. screening trial, it correctly flagged about 90% of patients who had a polyp 10 mm or larger.
📊 Clinical Data Point: Per-patient sensitivity for lesions ≥10 mm was about 90% — roughly 1 in 10 such patients was missed. For colorectal cancer specifically, pooled studies put sensitivity near 96%, comparable to optical colonoscopy. — Sources: ACRIN National CT Colonography Trial (NEJM, 2008); AAFP review of meta-analyses (2021).
What the accuracy numbers actually show
Out of 100 people with a large polyp, the scan flags about 90, and its cancer detection is close to a standard colonoscopy. Accuracy does depend on the radiologist’s skill and experience — this isn’t a fully automated read. You can see the underlying data in the national CT colonography trial.
Where virtual colonoscopy misses more
The test is weaker for small and flat polyps. Sensitivity for polyps 6 mm or larger ranges widely across studies (about 73% to 98%), and the smallest lesions — 5 mm and under — usually aren’t even reported, because they rarely turn dangerous and are hard to see reliably. The honest trade: very good at the lesions most likely to matter, less reliable for the tiny ones a scope would catch.
Cost, insurance, and what to expect on the day
A recent insurance change has made this question much easier to answer.
Does Medicare or insurance cover a virtual colonoscopy?
Yes — and this recently changed. As of January 1, 2025, Medicare covers screening CT colonography for beneficiaries 45 and older, with no deductible or coinsurance when your provider accepts assignment.
📊 Clinical Data Point: Medicare began covering screening CT colonography (CPT 74263) effective January 1, 2025, reversing long-standing non-coverage; it dropped the older barium-enema screening at the same time. There’s no patient cost-sharing for the screening exam when the provider accepts assignment. — Source: CMS 2025 Physician Fee Schedule final rule; Medicare’s CT colonography screening coverage.
For years Medicare didn’t pay for virtual colonoscopy as screening, so this is a real shift. Private coverage still varies by plan, and a scan ordered to investigate symptoms rather than for routine screening can carry standard cost-sharing.
What the appointment is like
You’ll do the same bowel-cleansing prep as a standard colonoscopy, plus the tagging drink (the prep options are the same — here’s how the common preps compare). At the imaging center the scan takes minutes, you stay awake, and you resume normal activities right after.
How often you need it
If normal, the standard interval is every 5 years for average-risk adults — versus every 10 years after a clear traditional colonoscopy (more on screening frequency). Higher-risk patients may be screened more often; Medicare allows every 2 years for high risk.
✅ Patient Action: Before scheduling, ask your insurer (or the imaging center) whether your plan covers CT colonography as a screening test, and what your out-of-pocket cost would be.
Which test is right for you?
There’s no single “better” test — there’s a better fit for your body, your risk, and what you’ll actually follow through on.
When a virtual colonoscopy may be the better fit
It’s often considered for people who can’t safely be sedated, take blood thinners, are frail or older, or had a traditional colonoscopy that couldn’t be completed. It’s also an option for someone who has skipped screening because the scope feels like too much — and the best test is ultimately one you’ll actually do.
When a traditional colonoscopy is usually preferred
It’s generally favored when finding-and-removing in one visit matters most, or for people more likely to have polyps — since a positive virtual result means coming back for a scope anyway. Your personal and family history weigh heavily, which is why this is a conversation, not a formula. You can gauge your colorectal cancer risk to frame it; if you’re also weighing stool-based options, see how a colonoscopy compares to Cologuard.
Questions to ask your doctor
🩺 Physician Note: Major guideline bodies treat both tests as acceptable options rather than ranking one universally above the other — which is why guidance emphasizes a shared decision based on your risk and preferences.
✅ Patient Action: Ask: “Given my age, family history, and whether I can tolerate sedation, which test do you recommend — and at what interval?” If virtual is on the table, also ask what happens, and how fast, if it finds something. See the National Cancer Institute’s screening guidance.
Risks and limits: radiation, missed polyps, and the second-procedure problem
A virtual colonoscopy is low-risk, but not risk-free, and it has real limits:
- Low-dose radiation from the CT scan
- Incidental findings outside the colon that may need follow-up
- Lower sensitivity for small and flat polyps
- A positive result usually means a second procedure — a traditional colonoscopy — to remove or biopsy what’s found
Radiation and extracolonic findings
The scan uses a low dose — roughly 7 to 8 mSv. Modeling suggests five-year screening still does far more good than harm, though the radiation consideration is greater for younger people screened repeatedly over decades.
📊 Clinical Data Point: A single CT colonography delivers about 7–8 mSv; one analysis estimated serial five-year screening prevents roughly 35–47 cancer deaths for every cancer it might cause, versus no screening. In the screening trial, incidental findings outside the colon appeared in about two-thirds of patients, and about 16% of participants had a finding judged to need further evaluation. — Sources: AAFP review (2021); ACRIN trial (NEJM, 2008).
Those findings cut both ways — occasionally catching something important early, but also leading to extra scans and worry over things that prove harmless.
What happens if they find a polyp
This is the trade-off people most underestimate. A virtual colonoscopy can’t remove anything — so a significant polyp means a referral for a traditional colonoscopy to take it out, usually with another bowel prep (some centers do it same-day). Here’s what a polyp finding means for next steps.
Who should not get a virtual colonoscopy
⚠️ Clinical Warning: A virtual colonoscopy is generally not recommended during an active inflammatory bowel disease flare (Crohn’s or ulcerative colitis), or when a bowel perforation or acute colitis is known or suspected. If any apply, your doctor will steer you to a safer test.
✅ Patient Action: If your report lists a polyp or an “extracolonic finding,” ask your gastroenterologist exactly what follow-up is needed and how soon.
Frequently asked questions about virtual colonoscopy
1. What is a virtual colonoscopy?
A virtual colonoscopy, or CT colonography, uses a CT scanner to create 2D and 3D images of your colon and rectum that a radiologist reviews for polyps and cancer. No scope is passed through the colon — a small tube inflates it with gas, and the scan takes only minutes.
2. Is a virtual colonoscopy as accurate as a regular colonoscopy?
For large polyps (10 mm or more) and cancer, it’s quite accurate — flagging about 90% of patients with a large polyp, with cancer detection close to a standard colonoscopy. It’s less reliable for small and flat polyps. Discuss which test fits your risk with your doctor.
3. Does a virtual colonoscopy still require the prep?
Yes. It requires the same bowel-cleansing prep as a traditional colonoscopy, plus a contrast “tagging” drink that helps the radiologist tell leftover stool from real polyps. The prep is the part most people find hardest, and it’s essentially the same for both tests.
4. Do you need sedation for a virtual colonoscopy?
No. A virtual colonoscopy doesn’t use sedation — you stay awake during the few-minute scan and can drive yourself home and resume normal activities right away. A traditional colonoscopy uses sedation, so you’ll need someone to drive you home.
5. Can a virtual colonoscopy remove polyps?
No. It can only view the colon — it can’t remove polyps or take biopsies. If it finds a significant polyp, you’ll be referred for a traditional colonoscopy to remove it, usually repeating the bowel prep. Ask your doctor what follow-up a positive result would involve.
6. Does Medicare cover a virtual colonoscopy?
Yes. As of January 1, 2025, Medicare covers screening CT colonography for people 45 and older, with no deductible or coinsurance when the provider accepts assignment. This reversed years of non-coverage. Private insurance varies by plan, so confirm your benefits before scheduling.
7. How much does a virtual colonoscopy cost?
With Medicare, a screening virtual colonoscopy has no patient cost-sharing when the provider accepts assignment (effective 2025). For private insurance, cost depends on your plan, and a scan ordered for symptoms rather than screening may carry standard cost-sharing. Verify coverage with your insurer first.
8. What are the risks of a virtual colonoscopy?
The main risks and limits are low-dose radiation (about 7–8 mSv), incidental findings outside the colon that may need follow-up, lower detection of small or flat polyps, and the chance a positive result sends you for a traditional colonoscopy anyway.
9. Who should not get a virtual colonoscopy?
It’s generally not recommended during an active inflammatory bowel disease flare (Crohn’s or ulcerative colitis), or when a bowel perforation or acute colitis is known or suspected. If any apply to you, ask your doctor which screening test is safer for your situation.
10. How often do you need a virtual colonoscopy?
If normal, the standard interval is every 5 years for average-risk adults — versus every 10 years after a clear traditional colonoscopy. Higher-risk patients may be screened more often. Your doctor sets the right interval based on your risk and any findings.
11. What happens if they find a polyp on a virtual colonoscopy?
Because a virtual colonoscopy can’t remove tissue, a polyp means a referral for a traditional colonoscopy to take it out and test it — often with another bowel prep, though some centers offer same-day removal. Ask your gastroenterologist how quickly that follow-up should happen.
The bottom line: choosing your colorectal screening
A virtual colonoscopy is convenient, sedation-free, now covered by Medicare for adults 45 and up, and genuinely accurate for the large polyps and cancers that matter most. The costs are real too: it can’t remove anything, it’s less reliable for small polyps, it uses a little radiation, and a positive result sends you back for a scope.
A traditional colonoscopy asks more up front but finds and fixes in one visit and stretches to ten years between screenings.
Neither is universally better. The best test is the one you’ll actually complete, chosen with a clinician who knows your history. If you’ve been putting screening off, that conversation is the next step worth taking.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.