On This Page – Quick Medical Summary
Your colonoscopy found polyps — here’s what that actually means
If your results say a colon polyp was found, the first thing to know is that most polyps are not cancer, and yours was very likely removed during the same procedure. Where you go next depends on your situation. If you just saw “polyp” on a patient portal and no one has explained it, the next two sections decode the types. If your report names a type — adenoma, sessile serrated, or hyperplastic — skip to which polyps are precancerous. If you mainly want to know when your next scope is due, the surveillance section covers that. And if a relative had polyps and you’re weighing your own risk, the risk-factor and warning-sign sections are for you.
Finding a polyp is exactly what screening is designed to do, and a polypectomy — removing it during the colonoscopy — is usually the entire treatment. This guide explains what your type means, how likely it is to matter, and when you’ll return. For the full picture, see your complete colonoscopy results guide; if this was your first procedure, here’s what actually happens during a colonoscopy.
ℹ️ Medical Disclaimer: This article is general health education, not medical advice, diagnosis, or treatment. Decisions about your diagnosis, follow-up testing, treatment, any procedure, and insurance coverage depend on your individual pathology and medical history. Always follow the specific guidance of a board-certified gastroenterologist before acting on anything here, and never delay or change recommended screening based on this article.
The main types of colon polyps, explained simply
Colon polyps fall into two groups, and the difference is the whole story for cancer risk:
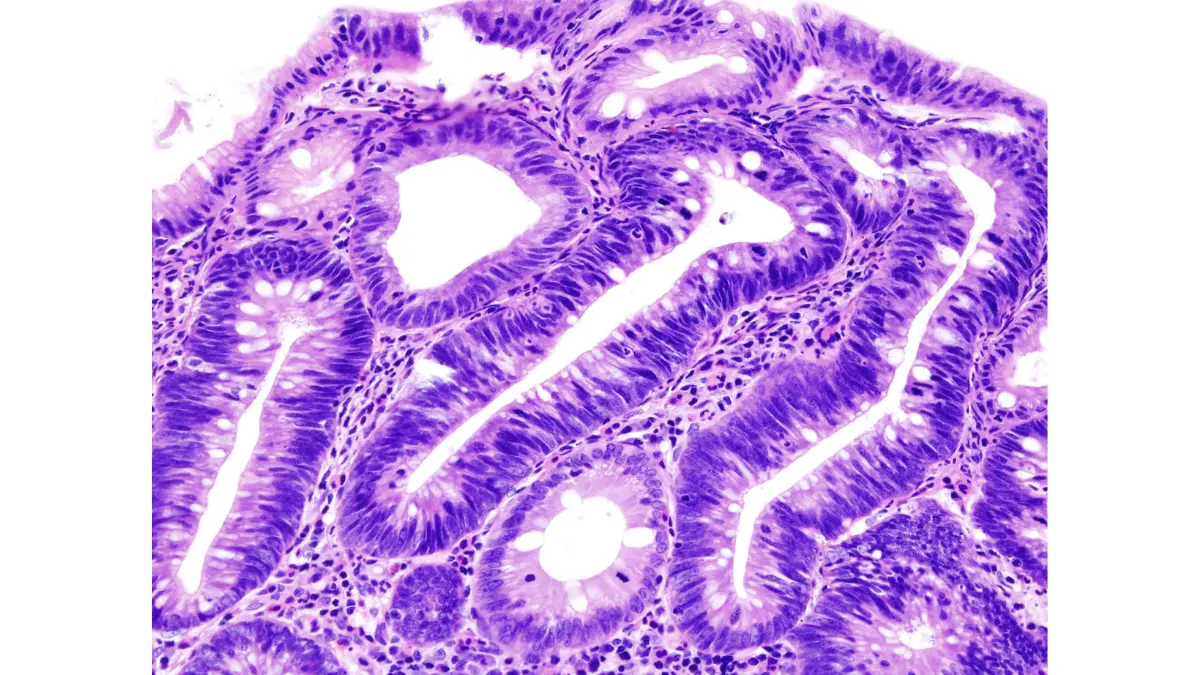
- Neoplastic polyps can, over time, turn into cancer. This group includes all adenomas, sessile serrated lesions, and traditional serrated adenomas.
- Non-neoplastic polyps generally cannot. This group includes hyperplastic polyps, juvenile polyps, and inflammatory pseudopolyps.
That split is why your pathology report matters — it tells your physician which bucket your polyp falls into. Adenomas are the most common type and the classic precursor to colorectal cancer; nearly all cancerous colon polyps began as adenomatous tissue.
🔬 How It Works: The colon’s lining constantly sheds and replaces its cells, and each division carries a small chance of a DNA error. In a neoplastic polyp, those errors can accumulate over years until the growth’s cells behave abnormally — the early step toward cancer. Non-neoplastic polyps don’t follow this path.
Within the adenoma family, cells grow in tubular or villous patterns, and most small adenomas are the lower-risk tubular kind. To put your result in context, here’s how to read your colonoscopy results line by line.
Which colon polyps are precancerous — and which aren’t
Two polyp types carry meaningful cancer risk, and the rest generally don’t:
- Adenomas — the most common precancerous polyp. Risk rises with size and with villous (rather than tubular) features.
- Sessile serrated lesions and traditional serrated adenomas — these progress through a separate route called the serrated pathway, are often flat and found in the right colon, and can be easy to miss.
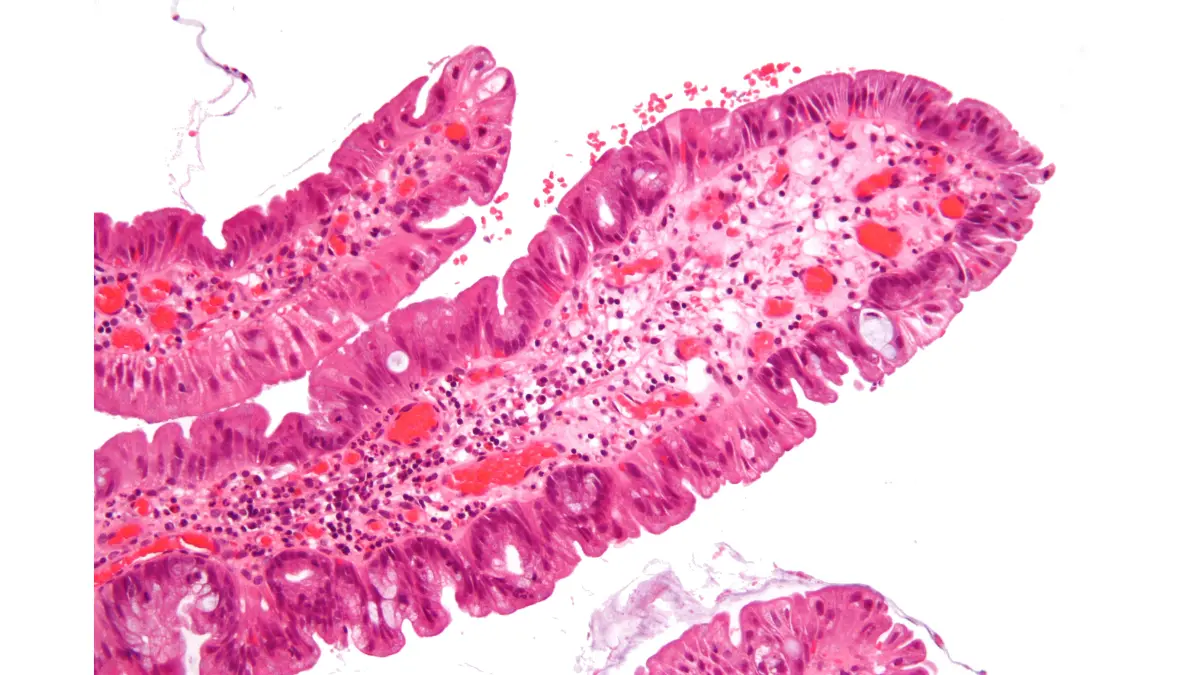
The polyps you usually don’t need to worry about are hyperplastic. Hyperplastic polyps are the most common serrated polyp — about three-quarters of them — are typically small and in the lower colon, and carry the lowest cancer potential, so they’re generally considered benign.
🩺 Physician Note: A common point of confusion is treating “I had a polyp” as one risk level. Current pathology guidance separates two very different processes: the classic adenoma-to-cancer sequence and the faster-moving serrated pathway, where some lesions are driven by BRAF gene changes. Your report’s specific wording defines your risk.
One more term to translate: dysplasia describes how much a polyp resembles cancer under the microscope. Low-grade dysplasia is mildly abnormal; high-grade looks more like cancer and may prompt an earlier follow-up. About one in four colon cancers arise from the serrated pathway, which is why flat serrated lesions get real attention even though most never become cancer.
✅ Patient Action: Ask your gastroenterologist: “Given my specific polyp type, size, and dysplasia grade, what is my individual cancer risk and follow-up plan?” For a finding-by-finding breakdown, review what each result on your report means.
You can match the exact terms on your report against the American Cancer Society’s pathology-report guide for colon polyps.
How likely is a polyp to turn into cancer?
Most adenomas take an estimated 10 to 15 years to progress to cancer, and the majority never do — which is exactly why regular screening catches them first. That slow timeline is your advantage: it gives your care team a wide window to find and remove a polyp long before it becomes dangerous.
Most colorectal cancers do develop from adenomas through the adenoma-carcinoma sequence, but the jump from an advanced adenoma to actual cancer is estimated at under roughly 10%. Size shifts the odds: in modeled estimates, the probability of cancer in a small adenoma is very low and rises as polyps grow past 10 and 20 millimeters.
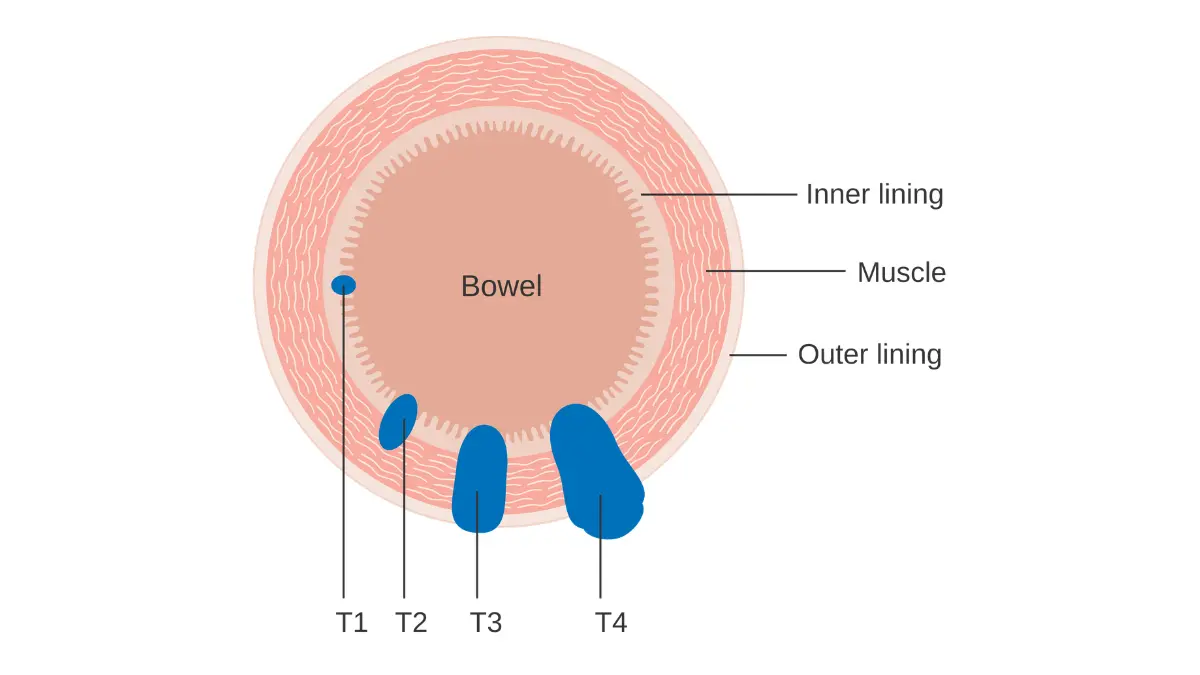
🔬 How It Works: A polyp doesn’t flip to cancer overnight. It accumulates specific genetic changes in a particular order over years — from normal lining, to adenoma, to advanced adenoma, to cancer — and most polyps stall well before the final step. Removing the polyp ends the sequence.
📊 Clinical Data Point: An estimated 158,850 new colorectal cancer cases and 55,230 deaths are projected in the US for 2026 — Source: American Cancer Society, Colorectal Cancer Statistics, 2026.
There’s an honest counterweight: people with high-risk adenomas carry a meaningfully higher future risk than those with low-risk findings — not a reason to panic over one small polyp, but a reason to keep your follow-up appointments. You can review the current ACS colorectal cancer statistics directly.
✅ Patient Action: Ask whether your findings place you in a low-risk or high-risk category, since that single distinction drives your follow-up timing more than any other factor.
When you’ll need your next colonoscopy after polyps
Your next colonoscopy interval depends on three things from your pathology: polyp type, size, and number. The table shows the general intervals gastroenterologists use across the US — but these are guidelines, and your doctor sets your personal interval based on your full results, prep quality, and history.
| Polyp Finding | General Follow-Up Interval | Key Clinical Detail |
|---|---|---|
| Normal exam / no polyps | 10 years | Standard interval for average-risk adults |
| Small hyperplastic polyps (rectosigmoid, <10mm) | 10 years | Lowest-risk type; treated like a normal exam |
| 1–2 small tubular adenomas (<10mm) | 7–10 years | Low-risk; interval lengthened in the 2020 update |
| 3–4 low-risk adenomas | 3–5 years | More polyps shortens the interval |
| 5–10 adenomas | 3 years | Higher polyp burden |
| Adenoma ≥10mm, villous, or high-grade dysplasia | 3 years | “Advanced” features raise risk |
| 1–2 sessile serrated polyps (<10mm) | 5–10 years | Serrated pathway, lower burden |
| 3–4 sessile serrated polyps | 3–5 years | Increasing serrated burden |
| >4 sessile serrated, or traditional serrated adenoma | 3 years | Highest-risk serrated findings |
Source: 2020 US Multi-Society Task Force on Colorectal Cancer recommendations (Gupta et al.). Intervals are general guidance; your gastroenterologist determines your individual schedule.
🩺 Physician Note: Current guidelines actually lengthened some intervals. After one or two small adenomas, the recommended return moved from the older 5-year mark toward 7 to 10 years, reflecting evidence that these patients carry a risk close to people with a normal exam. If you’re told to return much sooner for a low-risk finding, it’s reasonable to ask why.
A personal or family history of colorectal cancer can shorten these intervals. When your next scope is scheduled, here’s how to prepare for your follow-up colonoscopy.
✅ Patient Action: Before you leave, ask: “What follow-up interval did you set for me, and which specific finding drove that timing?” For broader context, the National Cancer Institute’s colorectal screening overview explains the available tests.
What raises your risk of colon polyps
Some risk factors for colon polyps you can’t change, and some you can. Outside your control are getting older — polyps become steadily more common with age — and family history, including inherited syndromes.
The factors you can influence are meaningful:
- Smoking
- Excess body weight, associated with a higher rate of adenomas and advanced adenomas
- Diet and alcohol intake
📊 Clinical Data Point: Colorectal cancer incidence is rising about 3% per year in adults aged 20–49, even as it falls in older adults — Source: American Cancer Society, Colorectal Cancer Statistics, 2026.
That rising trend is why average-risk screening now starts at age 45 rather than 50, and why symptoms in a younger person deserve attention rather than dismissal — here are the colorectal cancer warning signs in adults under 50.
If colorectal cancer runs in your family, that history is worth quantifying before you settle on a schedule. You can assess your hereditary colorectal risk and bring the result to your appointment, using the CDC’s guidance on talking with your doctor about screening as a starting point.
✅ Patient Action: If a first-degree relative had colorectal cancer or advanced polyps, ask your physician whether you should start screening earlier or repeat it more often than the standard schedule.
Warning signs, high-risk findings, and when family should screen
Most colon polyps cause no symptoms and are found only through screening — the central reason not to wait for symptoms before getting checked. When larger polyps do cause problems, the signs can include blood in the stool or a lasting change in bowel habits, though these more often have other, non-cancer causes.
⚠️ Clinical Warning: Don’t treat the absence of symptoms as reassurance, or ignore their presence. Rectal bleeding, blood in the stool, persistent changes in bowel habits, or unexplained abdominal pain warrant prompt evaluation — not because they usually mean cancer, but because they occasionally do, and early evaluation is when treatment works best.
A few findings raise the stakes. High-grade dysplasia may shorten your follow-up interval. Inherited conditions such as familial adenomatous polyposis cause very large numbers of polyps and a high cancer risk, and serrated polyposis syndrome carries elevated risk as well — both are uncommon and managed closely once identified.
Your result can matter for relatives, too: a personal history of certain polyps can raise a first-degree relative’s risk, and a gastroenterologist or genetic counselor can advise whether they should screen earlier. Because fear of the procedure keeps many people away, it helps relatives to know what a colonoscopy actually feels like and which bowel symptoms are worth getting checked.
✅ Patient Action: If your pathology suggests a possible hereditary pattern, ask: “Do my findings warrant genetic counseling, and should my first-degree relatives start screening earlier than age 45?”
Colon polyps and cancer risk: frequently asked questions
1. Does finding colon polyps mean I have cancer?
No. Most colon polyps are benign and not cancer, and they’re usually removed during the same colonoscopy. Only certain types — adenomas and some serrated polyps — are precancerous, meaning they could turn cancerous over years if left in place. Your pathology report and gastroenterologist confirm which type you have.
2. Are hyperplastic polyps dangerous?
Usually not. Hyperplastic polyps are the most common serrated polyp, are typically small and found in the lower colon, and carry the lowest cancer potential, so they’re generally considered benign. Larger serrated lesions in the upper colon are a different, higher-risk category. Confirm your specific finding with your physician.
3. Which colon polyps are precancerous?
Two groups carry cancer risk: adenomas, the most common precursor, and sessile serrated lesions plus traditional serrated adenomas, which progress by a separate pathway. Hyperplastic, juvenile, and inflammatory polyps are generally not precancerous. The exact type is determined by pathology after the polyp is removed.
4. How likely is a polyp to become cancer?
Most adenomas never become cancer. The estimated jump from an advanced adenoma to colorectal cancer is under roughly 10%, and larger polyps carry higher odds than small ones. Because risk depends on type, size, and number, ask your gastroenterologist where your specific findings fall.
5. How long does a polyp take to turn into cancer?
Generally a long time. Most adenomas are estimated to take roughly 10 to 15 years to progress to cancer, which is why regular screening works so well — it finds and removes them well before that point. Some serrated-pathway polyps can progress faster than the typical adenoma.
6. When will I need my next colonoscopy after polyps?
It depends on your findings. Under the 2020 US Multi-Society Task Force guidelines, one or two small tubular adenomas typically mean a 7–10 year follow-up, while larger, villous, high-grade-dysplasia, or numerous polyps shorten that toward 3 years. Your gastroenterologist sets your personal interval.
7. Can colon polyps come back after they’re removed?
Yes. Even when every polyp is removed, you can develop new ones over time, which is why physicians recommend follow-up colonoscopies on a schedule rather than treating one clear exam as permanent. The interval is based on what was found and your overall risk.
8. Do colon polyps cause symptoms?
Usually none. Most colon polyps are silent and found only on screening. Rarely, larger polyps may bleed or change bowel habits — blood in the stool, or a lasting shift in bowel patterns — but these symptoms more often have other causes. Don’t wait for symptoms to get screened.
9. What causes colon polyps?
Risk rises with age and can run in families, and is also associated with modifiable factors like smoking, excess weight, diet, and alcohol. You can’t change age or genetics, but you can influence several lifestyle factors. Discuss your personal risk profile with your clinician.
10. Why is colorectal cancer rising in younger adults?
According to current American Cancer Society data, colorectal cancer incidence is increasing about 3% per year in adults aged 20–49, even as it declines in older adults. This trend is the reason average-risk screening now begins at age 45 instead of 50.
11. Should my family get screened if I have polyps?
Possibly. A personal history of certain polyps can raise a first-degree relative’s risk, and some findings point toward hereditary syndromes. If your results suggest higher familial risk, your gastroenterologist or a genetic counselor can advise whether relatives should screen earlier. Raise this at your next appointment.
The bottom line on your polyp results
Finding polyps is the screening system working as intended: most are benign or were removed before they could matter, and the type, size, and number on your report — not the word “polyp” alone — define your actual risk. The adenoma-to-cancer process is slow, which is why staying on your follow-up schedule is the single most protective thing you can do now.
Your clearest next step is to confirm two things with your gastroenterologist: which risk category your findings fall into, and the specific interval for your next colonoscopy. For the complete journey from prep through every possible result, return to your full colonoscopy results guide.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.