On This Page – Quick Medical Summary
Yes — if you are an average-risk adult age 45 or older, you need colonoscopy screening even with no symptoms. That is the whole point of screening: colorectal cancer and the polyps it grows from usually cause nothing you can feel until the disease is advanced, so waiting until you notice something often means waiting too long.
Use this guide based on where you are right now:
- Average risk, ages 45–75, no symptoms: Screening is recommended now. This guide explains why and walks through your options.
- Under 45 with no symptoms and no family history: Routine screening is not yet standard for you; the risk-factor section helps you decide with your doctor.
- Higher risk (family history of colorectal cancer, Lynch syndrome, inflammatory bowel disease): You may need to start earlier — see who qualifies below.
- You actually do have symptoms (rectal bleeding, a lasting change in bowel habits, unexplained weight loss): Do not wait for routine screening — contact your doctor promptly; you likely need a different kind of evaluation.
For preparation, cost, and reading your results, see our complete guide to colonoscopy.
ℹ️ Medical Disclaimer: This article is general health education about colorectal cancer screening — not a diagnosis, a treatment plan, or a recommendation for any specific test, procedure, medication, or insurance decision. The right test, timing, and follow-up depend on your personal risk and medical history. Consult a board-certified gastroenterologist or your primary care provider before acting on anything here.
Why colon cancer often causes no symptoms early on
Yes, you can have colon cancer with no symptoms — early on, that is the norm rather than the exception. Colorectal cancer grows slowly and quietly, which is exactly why a test done in healthy-feeling people catches it when it is most treatable.
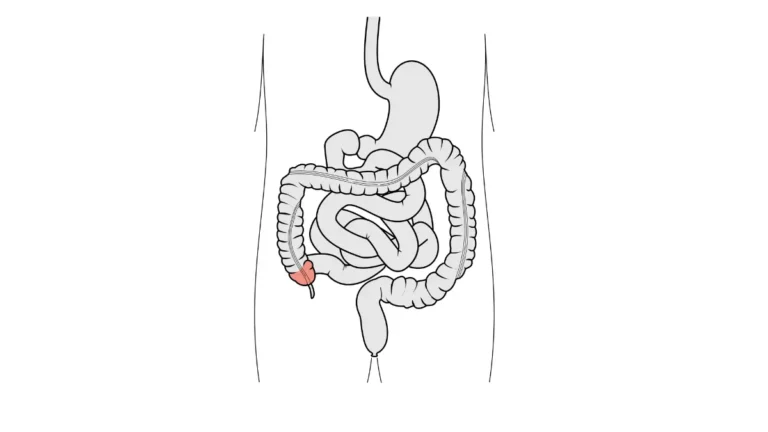
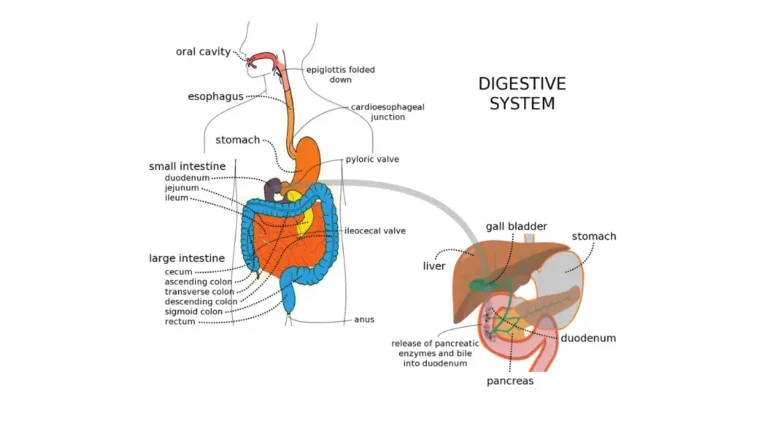
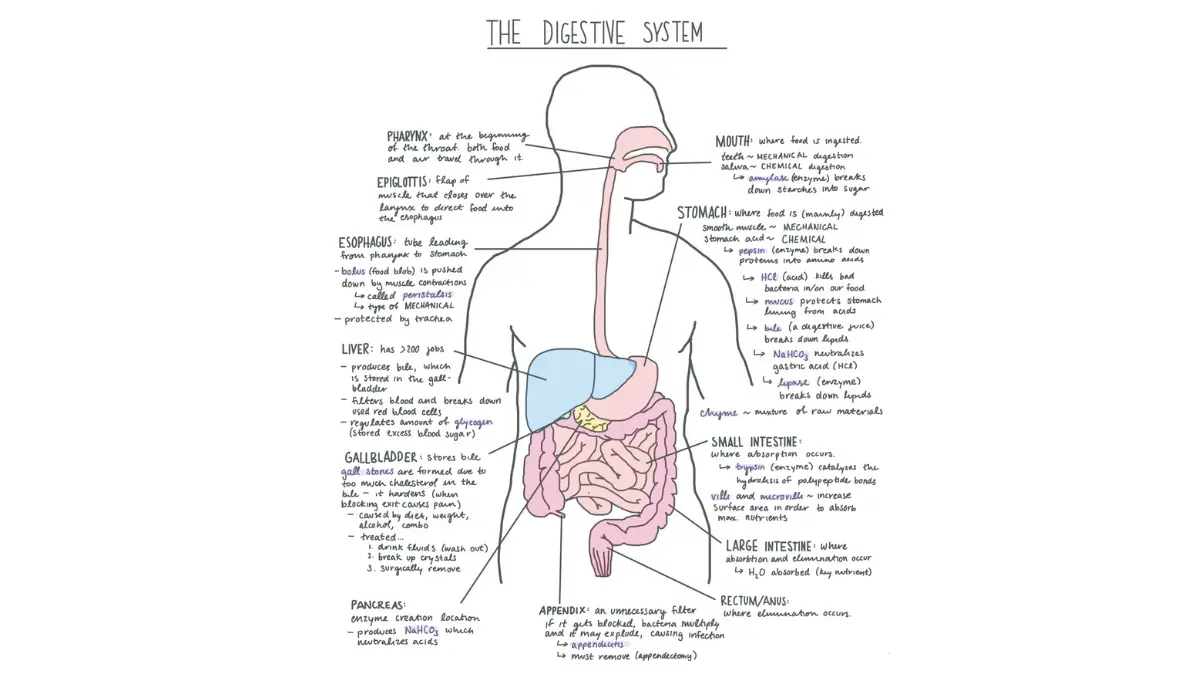
🔬 How It Works: Colorectal cancer almost always begins as a small growth called a polyp on the inner lining of the colon or rectum. Certain polyps — called adenomas — can change into cancer over the course of years. Because this happens deep inside the bowel, where an early growth neither presses on anything nor bleeds in a way you would notice, it usually produces no sensation at all.
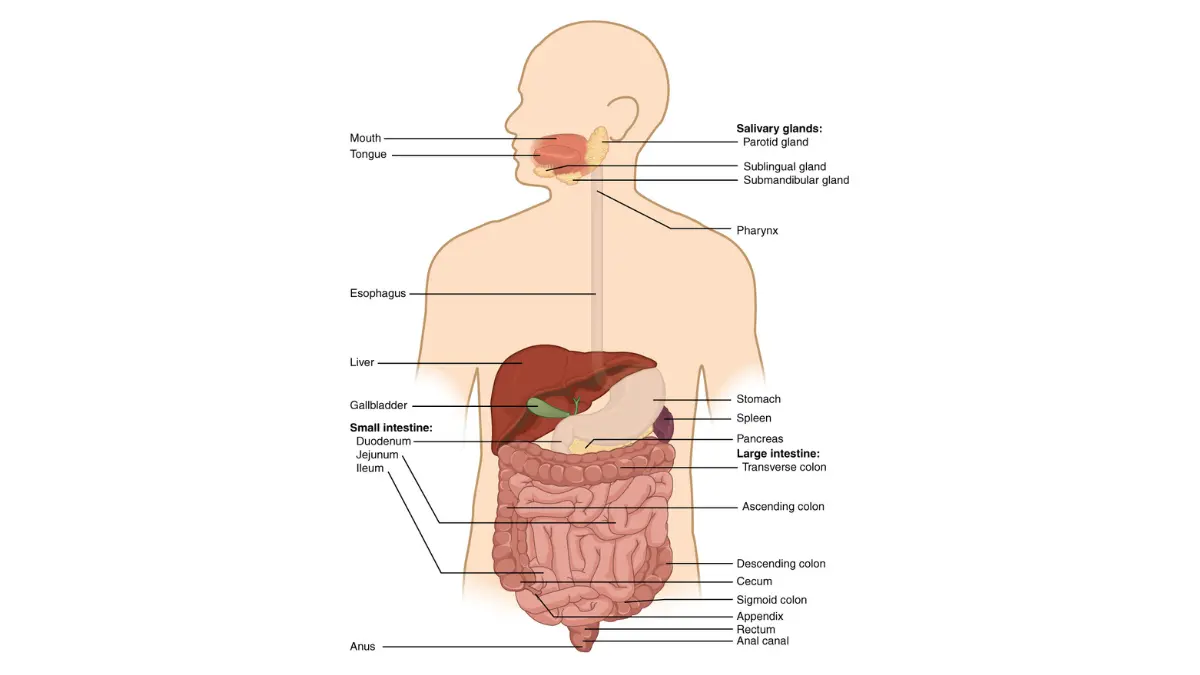
Adapted from Wikimedia Commons 2401 Components of the Digestive System, licensed under Creative Commons Attribution 3.0 Unported license.
This silent timeline is the foundation of screening. The CDC notes that screening can find and remove precancerous polyps before they ever become cancer, and can catch cancer at an early, more treatable stage — see its overview of how colorectal cancer screening works. That gives screening a power most cancer tests lack: it can prevent the disease, not just detect it. Our explainer on how colon polyps relate to cancer risk goes deeper, but the takeaway is simple — feeling fine tells you nothing about whether polyps are present.
Who should get a colonoscopy at 45 with no symptoms
For average-risk adults, both the U.S. Preventive Services Task Force and the American Cancer Society recommend starting colonoscopy screening at age 45 — even with no symptoms — and continuing through 75. The American Cancer Society reaffirmed this starting age in its updated guideline released in May 2026.
Average risk has a specific meaning: no personal history of colorectal cancer, adenomatous polyps, or inflammatory bowel disease, and no personal or family history of inherited syndromes such as Lynch syndrome or familial adenomatous polyposis. Most adults fall into this group. If that describes you and you are 45 or older, the recommendation applies — symptoms or not.
Some people should start earlier. The National Cancer Institute notes that a family history of colorectal cancer, a personal history of advanced polyps, an inherited syndrome, or inflammatory bowel disease may mean beginning before 45 and screening more often. Our genetic risk assessment tool can help you map your family pattern before your appointment.
If you are under 45 with no symptoms and no risk factors, routine screening is not yet standard — though that does not mean ignoring changes in your body. The reasoning behind the threshold is in our piece on why colorectal screening now starts at 45, and the American Cancer Society’s colorectal cancer screening guidelines lay out the average-risk and higher-risk paths side by side.
✅ Patient Action: Ask your primary care provider or a gastroenterologist a specific question: “Based on my family history and personal medical history, what age should I start screening, and which test fits my risk level?”
What the data shows about screening before symptoms
The case for screening when you feel fine is strongest in the numbers, drawn from the American Cancer Society’s Colorectal Cancer Statistics, 2026 report and the National Cancer Institute’s SEER program.
📊 Clinical Data Point: An estimated 158,850 new colorectal cancer cases and 55,230 deaths are projected in the United States in 2026 — Source: American Cancer Society, 2026. It is the second-leading cause of cancer death overall, and the leading cause of cancer death in adults younger than 50.
The disease is also shifting younger, which is the reason the starting age dropped. Colorectal cancer incidence is rising about 3% per year in adults aged 20–49, and the share of cases in people under 55 has roughly doubled — from about 11% in 1995 to about 1 in 5 today. Lifetime risk now sits at about 1 in 24 men and 1 in 26 women — real, though screening is designed to push it down. You can review the figures in the ACS colorectal cancer statistics.
Catching it early is the whole point, and this is where “no symptoms” lands hardest. Most adults under 50 who develop colorectal cancer are diagnosed at a later stage — in large part because they were not yet being screened, and the disease was found only once symptoms appeared (American Cancer Society, 2026).
📊 Clinical Data Point: About 9 out of 10 people whose colorectal cancers are found early and treated appropriately are alive five years later — Source: CDC. Overall five-year relative survival is now about 65% (SEER / American Cancer Society), up substantially over recent decades.
Those survival figures fall sharply when the cancer is found at a later, spread stage — the practical cost of waiting for a symptom to announce it.
Colonoscopy vs other screening tests when you have no symptoms
A colonoscopy is not the only way to screen, and for an average-risk person with no symptoms there is genuine choice. The main options, their schedules, and who they suit best are below.
| Screening test | How it works | How often | Best for patient profile | Key clinical detail |
|---|---|---|---|---|
| Colonoscopy | Direct look at the whole colon and rectum; polyps removed during the exam | Every 10 years | Anyone average-risk; the only test that both prevents and detects | Needs bowel prep and sedation; the follow-up test for any abnormal result from the others |
| FIT (fecal immunochemical test) | At-home stool test for hidden blood | Every year | Average-risk people who will test reliably each year | No prep; a positive result needs a follow-up colonoscopy |
| Multitarget stool DNA test | At-home stool test for hidden blood plus altered DNA | Every 3 years | Average-risk people who prefer at-home testing | No prep; a positive result needs a follow-up colonoscopy |
| CT colonography | Imaging scan that builds a 3-D view of the colon | Every 5 years | People who want to avoid a scope | Bowel prep still needed; abnormal findings need a colonoscopy |
| Flexible sigmoidoscopy | Scope of the rectum and lower colon only | Every 5 years (or every 10 with annual FIT) | People for whom a full colonoscopy is not suitable | Does not view the entire colon |
| Blood-based test | Office blood draw checking for tumor DNA | Per manufacturer | Only those unwilling to do a stool test or visual exam | Added by ACS in 2026 but not a preferred option; a positive result needs a colonoscopy |
Source: U.S. Preventive Services Task Force (2021); CDC; American Cancer Society (2026).
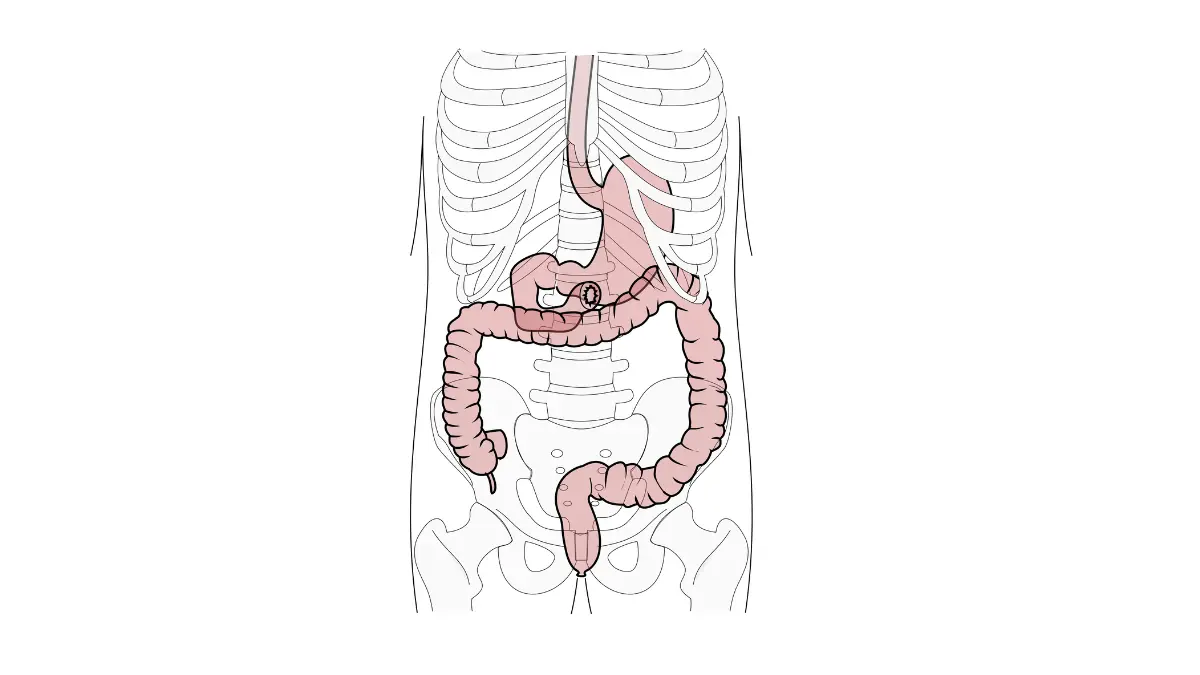
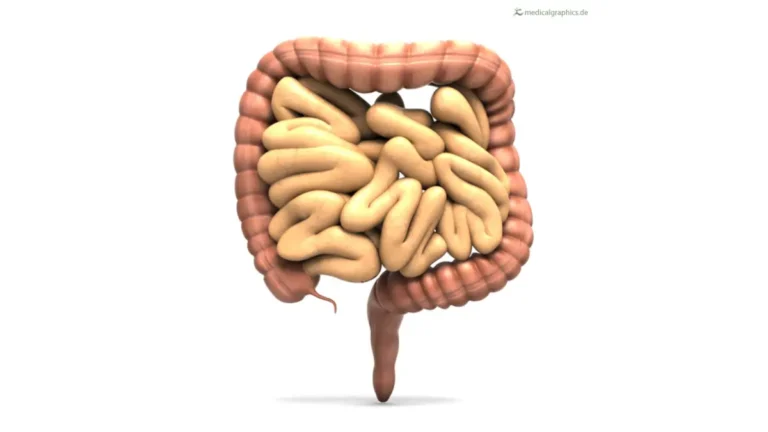
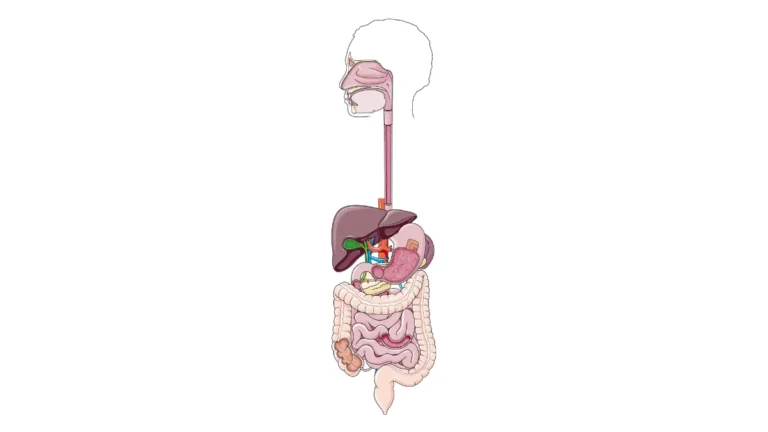
Adapted from Wikimedia Commons Tractus intestinalis cum ossibus, licensed under Creative Commons Attribution-Share Alike 2.5 Generic, 2.0 Generic and 1.0 Generic license.
🔬 How It Works: Stool-based tests like FIT detect tiny amounts of blood — too small to see — that polyps and cancers can shed into the stool. The multitarget stool DNA test adds detection of altered DNA shed by abnormal cells, which is why it runs less often.
One rule ties the menu together: any abnormal result from a stool test, CT colonography, or sigmoidoscopy must be followed by a colonoscopy to complete screening. That is also why colonoscopy is called the gold standard — it can find and remove polyps in a single visit. The National Cancer Institute’s overview of colorectal screening tests compares accuracy, and our guides on how often you need a colonoscopy and how to prepare for one cover the practical side.
Disclosure: Some at-home screening kits are available through retail partners we may earn a commission from. They are an option to discuss with your clinician — not a substitute for a colonoscopy if you are at higher risk, and any positive result still requires a follow-up colonoscopy.
Symptoms that mean you shouldn’t wait for routine screening
Screening is, by definition, for people without symptoms. If you do have certain warning signs, you have moved out of “screening” and into “evaluation” — and that should not wait for a birthday or a scheduled interval.
Warning signs worth a prompt call to your doctor include:
- Rectal bleeding or blood in or on the stool, whether bright red or dark
- A lasting change in bowel habits — new diarrhea, constipation, or stools that look narrower than usual
- Unexplained weight loss you did not intend
- Ongoing abdominal pain, cramping, or bloating that does not resolve
- Iron-deficiency anemia or unusual, persistent fatigue
⚠️ Clinical Warning: Each of these can have a harmless cause, such as hemorrhoids or a dietary change — but the same symptoms can also signal colorectal cancer. The danger is assuming the benign explanation and waiting. These signs warrant evaluation, not a wait-and-see approach.
The distinction matters for what happens next. A diagnostic colonoscopy is done to find the cause of symptoms you already have, while a screening colonoscopy is done precisely because you have none. Younger adults are especially prone to dismissing these signs, part of why early-onset cases are so often caught late — our guide to colon cancer symptoms in younger adults covers what not to ignore, and a quick symptom check can help you organize what to report.
✅ Patient Action: If you have any of these symptoms, tell your doctor directly: “I’m having [symptom] — could this need a diagnostic colonoscopy rather than waiting for routine screening?”
What happens if you wait until you have symptoms
Waiting until symptoms appear often means colorectal cancer is found at a later stage, when it is harder to treat and the options narrow. Because the disease is silent early on, the symptoms that finally prompt a visit tend to show up after it has grown or spread — which is why so many younger patients are diagnosed at an advanced stage rather than a curable one.
Screening earlier flips that math. When a colonoscopy finds a polyp, it can often be removed on the spot, before it ever becomes cancer; when it finds an early cancer, treatment is usually less extensive than for advanced disease.
It is fair to ask about the risks of the colonoscopy itself, and an honest answer matters here.
📊 Clinical Data Point: Across large studies of screening colonoscopy, serious complications are uncommon — perforation of the colon wall occurs in well under 1 in 1,000 exams, and bleeding requiring care in roughly 1 to 2 in 1,000, with risk higher when polyps are removed or in older adults — Source: pooled colonoscopy safety reviews (ASGE). For eligible average-risk adults, the benefit of screening outweighs these small risks.
A fuller breakdown is in our guide to colonoscopy risks and complications, and if a first procedure feels daunting, what to expect at your first colonoscopy walks through the day.
✅ Patient Action: If you have a bleeding disorder or take blood thinners, ask your gastroenterologist how that affects your screening plan and whether any medication needs adjusting before the procedure.
Frequently asked questions
1. Do I need a colonoscopy if I feel completely fine?
Yes. For average-risk adults aged 45 to 75, colonoscopy screening is recommended with no symptoms, because colorectal cancer and its precancerous polyps usually cause nothing you can feel until they are advanced. Feeling fine is the state screening is built for. Confirm your start age and risk level with your doctor.
2. Can you have colon cancer with no symptoms?
Yes, and early on that is typical. Colorectal cancer starts as a slow-growing polyp deep in the colon or rectum, where it does not press on anything or bleed noticeably at first. That is exactly why a colonoscopy with no symptoms is worthwhile — it catches disease before any sign appears.
3. Why is screening recommended before symptoms appear?
Because screening can prevent colorectal cancer, not just detect it. A colonoscopy can remove precancerous polyps before they turn into cancer and catch cancer at an early stage. About 9 in 10 colorectal cancers found early and treated are alive at five years, per the CDC.
4. What age should I get a colonoscopy if I have no symptoms?
Average-risk adults should start at 45 and continue through 75, according to both the USPSTF and the American Cancer Society. People at higher risk may start earlier. Ask your doctor which starting age fits your personal history.
5. Who needs to start colonoscopy screening before 45?
People with a family history of colorectal cancer, a personal history of advanced polyps, an inherited syndrome such as Lynch syndrome or familial adenomatous polyposis, or inflammatory bowel disease may need to begin earlier and screen more often. Set your timing with a gastroenterologist.
6. Is a colonoscopy worth it if I have no family history?
Yes. Most colorectal cancers occur in people with no family history, and average risk still carries a real lifetime risk — about 1 in 24 men and 1 in 26 women. A colonoscopy with no symptoms is still standard screening from age 45. Discuss your individual risk factors with your doctor.
7. What are the alternatives to a colonoscopy?
Average-risk people can also use an annual FIT, a multitarget stool DNA test every 3 years, CT colonography every 5 years, or flexible sigmoidoscopy. A newer blood-based test exists but is not a preferred option. Any abnormal result still requires a follow-up colonoscopy. Your doctor can match the test to your risk.
8. What symptoms mean I shouldn’t wait for routine screening?
Rectal bleeding, a lasting change in bowel habits, unexplained weight loss, ongoing abdominal pain, or iron-deficiency anemia mean you should contact your doctor promptly rather than wait. These can have benign causes but can also signal colorectal cancer, so you likely need a diagnostic evaluation.
9. What’s the difference between a screening and a diagnostic colonoscopy?
A screening colonoscopy is done when you have no symptoms, to look for hidden polyps or early cancer. A diagnostic colonoscopy is done to find the cause of symptoms you already have. The procedure is similar, but the reason — and sometimes the insurance coding — differs. Your doctor can clarify which applies.
10. What happens if I wait until I have symptoms?
Waiting often means colorectal cancer is found at a later, harder-to-treat stage, because it is silent while it is most curable. That is why many people diagnosed after symptoms appear have advanced disease. A colonoscopy with no symptoms aims to catch it — or prevent it — well before that point.
11. How often do I need a colonoscopy if my results are normal?
For average-risk adults with a normal colonoscopy, screening is generally repeated every 10 years. Other tests differ — FIT yearly, stool DNA every 3 years, CT colonography every 5 years. Higher-risk people screen more often. Your gastroenterologist sets your interval based on your findings and risk.
The bottom line on colonoscopy with no symptoms
If you are an average-risk adult 45 or older, a colonoscopy with no symptoms is not optional caution — it is the standard of care, because colorectal cancer is most preventable and most curable exactly when you cannot feel it. The disease is moving younger, the data shows screening catches it early, and the procedure’s serious risks are small for eligible adults.
The single most useful next step is a conversation: ask your provider or a gastroenterologist what age and which test fit your personal risk, and book it rather than waiting for a sign. For prep, cost, sedation, and results, start with our complete guide to colonoscopy.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.