On This Page – Quick Medical Summary
When should you start prostate cancer screening?
If you’ve just turned 45, watched a brother get diagnosed, or had a doctor mention a PSA test in passing, you’re asking the right question at the right time. There is no single age when every man should begin prostate cancer screening — the answer depends on your risk.
This guide routes you by situation. If you’re at average risk with no family history, your starting point is one age; if you’re a Black man or have a father or brother who had prostate cancer, it’s earlier; if you carry a BRCA mutation or have several affected relatives, earlier still. Caregivers helping a partner decide will find the same tiers, plus the questions worth asking, and if you already have a raised PSA result, the section on reading your numbers is written for you.
You can read the complete prostate cancer guide for the full picture, or stay here for the screening decision itself.
ℹ️ Medical Disclaimer: This article explains prostate cancer screening for general education only. Decisions about whether to be screened, how to interpret a PSA result, when to have a biopsy, and how to weigh your personal risk should be made with a board-certified urologist or your primary care clinician, who can account for your individual health, age, and history. It is not a substitute for personalized medical care.
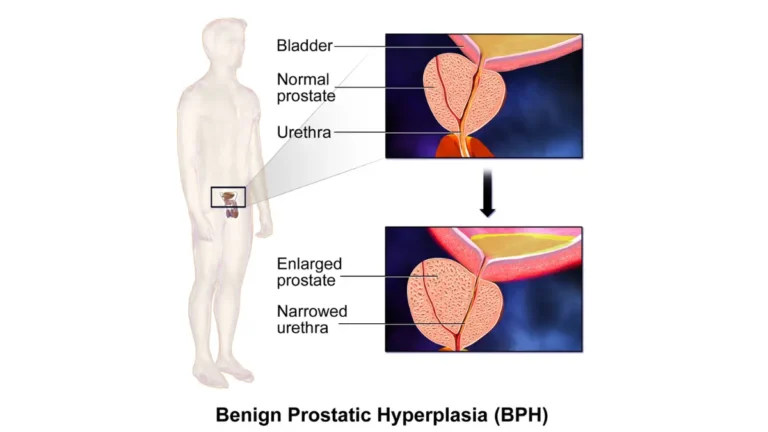
What prostate cancer screening actually involves
Screening means looking for cancer in men who feel completely well, before any symptoms appear. The main tool is the PSA test, a simple blood draw.
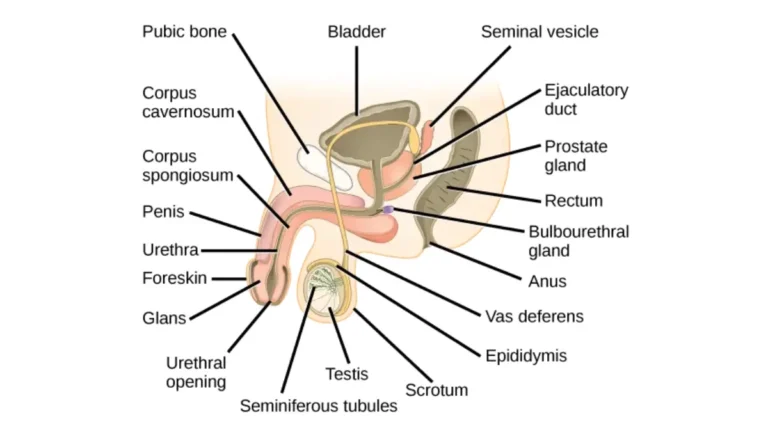
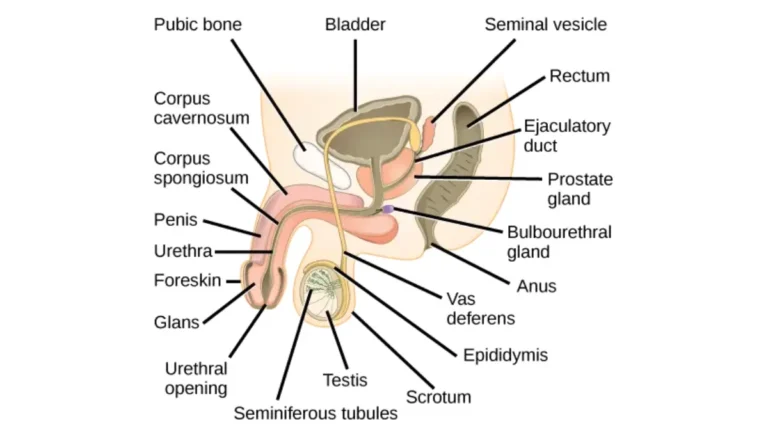
🔬 How It Works: PSA, or prostate-specific antigen, is a protein made by the prostate gland and released into the blood. The test measures how much is circulating. Higher levels can reflect cancer, but also an enlarged prostate, inflammation, infection, or recent activity, which is why one number alone never tells the whole story.
A digital rectal exam (the DRE) may be used alongside the blood test, but PSA is the primary screen and the exam is no longer used on its own. You can read more about how the PSA test works from the National Cancer Institute.
The most important distinction in this whole topic is that screening is not diagnosis. A screening test that flags something abnormal leads to more evaluation, not a cancer diagnosis. Many men with an unexpected result turn out not to have cancer at all.
At what age should you start, based on your risk?
Most men at average risk should have their first conversation about screening at age 50. Men at higher risk should start at 45, and those at the highest risk at 40. The exact age depends on which risk group you fall into.
The American Cancer Society recommends that average-risk men with at least a 10-year life expectancy discuss screening at 50. The U.S. Preventive Services Task Force frames it differently, describing an individual decision for men aged 55 to 69 after a conversation with a clinician — a Grade C recommendation. You can review the American Cancer Society’s screening recommendations directly.
Higher-risk men should start earlier. The ACS sets age 45 for high risk — including Black men and those with a father or brother diagnosed before 65 — and age 40 for the highest risk, meaning more than one such relative or a known BRCA mutation. The American Urological Association similarly suggests a baseline PSA at 45 to 50 for most men, and 40 to 45 for those with Black ancestry, inherited mutations, or a strong family history.
These aren’t really contradictions, but different framings of the same evidence. Here is how the three major bodies line up:
| Risk group (patient profile) | American Cancer Society | USPSTF | AUA/SUO |
|---|---|---|---|
| Average risk | Discuss at 50 (≥10-yr life expectancy) | Individual decision, ages 55–69 (Grade C) | Baseline PSA at 45–50; screen every 2–4 yrs, 50–69 |
| High risk (Black men; father/brother diagnosed <65) | Discuss at 45 | Same 55–69 decision window | Begin at 40–45 |
| Highest risk (>1 relative; BRCA carrier) | Discuss at 40 | (not separately specified) | Begin at 40–45 |
| Age 70+ | Generally not screened if <10-yr life expectancy | Recommends against (Grade D) | Personalize, often discontinue |
Source: American Cancer Society early-detection recommendations; USPSTF (2018); AUA/SUO Early Detection of Prostate Cancer guideline (2023; 2026 update).
Who is at higher risk and should start earlier
Some men carry a meaningfully higher risk and should begin screening before 50.
Black and African-ancestry men face the steepest risk, covered in detail in our guide to prostate cancer in Black men.
📊 Clinical Data Point: Black men have roughly 67% higher prostate cancer incidence and about twice the mortality of White men — Source: American Cancer Society, Prostate Cancer Statistics, 2025. This is why both the ACS and AUA advise starting the screening conversation at 45 or earlier.
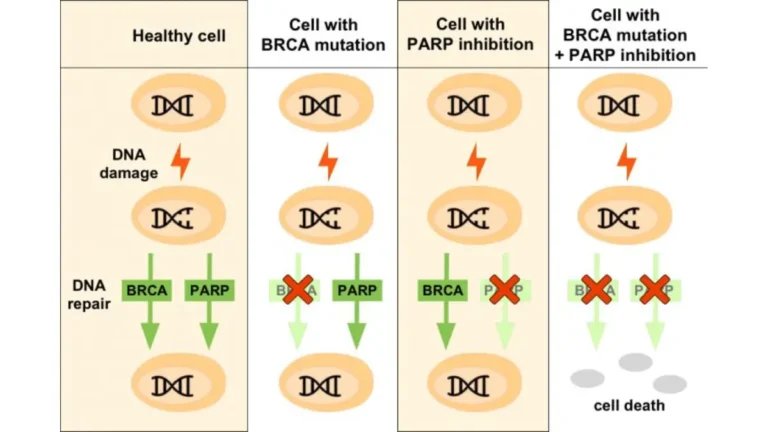
A family history matters too. A father or brother diagnosed before 65 raises your risk; more than one such relative, or an inherited BRCA1 or BRCA2 mutation, raises it further, and these are the men advised to start at 40. Our overview of what raises prostate cancer risk covers the full list, and you can assess your inherited risk with our genetic risk tool.
Age itself is the largest factor. National incidence and survival data show prostate cancer is uncommon before 50 and climbs steadily afterward.
✅ Patient Action: If a first-degree relative had prostate cancer, especially before 65, or your family carries a BRCA mutation, ask your clinician: “Given my family history, should I start PSA screening at 40 or 45 rather than 50, and do I need genetic counseling?”
Is prostate cancer screening worth it?
This is the question most men actually want answered, and an honest answer includes both sides.
📊 Clinical Data Point: Screening men aged 55 to 69 may prevent about 1.3 prostate cancer deaths and roughly 3 cases of metastatic disease for every 1,000 men screened over about 13 years — Source: U.S. Preventive Services Task Force, 2018.
Those are real benefits, concentrated in that age band. The CDC’s plain-language summary of the USPSTF guidance explains the reasoning. Screening also causes harm, and many resources gloss over it. The main downsides:
- False positives — a raised PSA that isn’t cancer, leading to anxiety and sometimes a biopsy.
- Overdiagnosis — finding a cancer that never would have caused symptoms, estimated to happen in 20% to 50% of screen-detected cases.
- Overtreatment — treating those harmless cancers anyway.
📊 Clinical Data Point: Among men who have their prostate surgically removed, about 1 in 5 develop long-lasting urinary incontinence and about 2 in 3 experience long-term erectile dysfunction — Source: the USPSTF evidence statement, 2018.
Context matters here: many low-risk cancers found today are watched with active surveillance rather than treated immediately, which avoids much of that harm.
✅ Patient Action: Before agreeing to a first PSA test, ask your clinician: “For someone my age and risk, how much benefit am I likely to get, and what are the chances of a false alarm or of finding a cancer that wouldn’t have harmed me?”
How to get screened and what your PSA result means
Getting screened starts with a conversation, not a test.
Screening is a shared decision: you and your clinician weigh your age, risk, and preferences, then decide whether to draw a PSA. The test itself is a routine blood sample. For men who choose to screen, the AUA suggests repeating the PSA every 2 to 4 years between ages 50 and 69, personalized to your risk and previous results, and men with a very low baseline reading may safely wait longer.
There is no universal “normal” PSA, because ranges drift upward with age. The figures below are general references a clinician interprets in context, not personal cut-offs:
| Age range | General PSA reference (ng/mL) |
|---|---|
| 40s | ~2.5 |
| 50s | ~3.5 |
| 60s | ~4.5 |
| 70s | ~6.5 |
Source: AUA/SUO Early Detection of Prostate Cancer guideline (2023; 2026 update). These are reference points, not diagnostic thresholds.
🩺 Physician Note: Current guidelines emphasize confirming an elevated PSA with a repeat test before moving to imaging or biopsy, because PSA can rise temporarily from infection, recent ejaculation, or even a vigorous bike ride. A trend over time is more meaningful than any single reading.
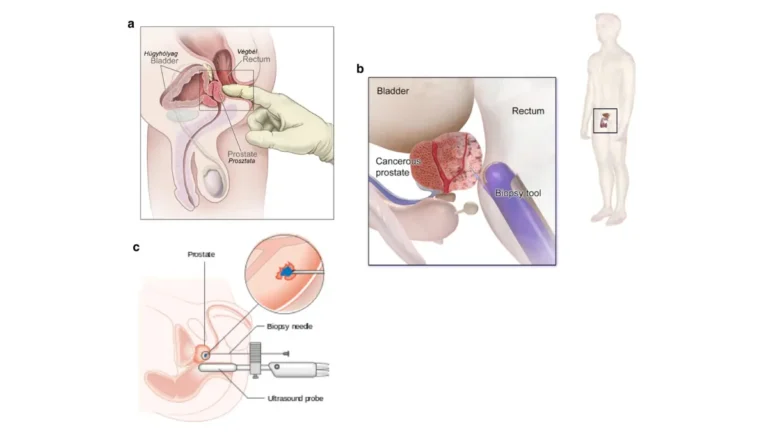
A single high number is not a diagnosis. A newly elevated PSA is usually repeated after a few months before any further step, and many raised results turn out to be benign — our guide on a high PSA that doesn’t mean cancer explains why. You can also see typical PSA levels by age in more detail.
✅ Patient Action: If your PSA comes back elevated, ask a urologist: “Should we repeat the test before any biopsy, and what besides cancer could be raising my number?”
When to stop screening, and when symptoms can’t wait
Screening isn’t meant to continue indefinitely.
The USPSTF recommends against routine PSA screening for men 70 and older — a Grade D recommendation — because at that age the harms outweigh the small benefit. The ACS adds that overall health matters more than age alone: men without symptoms who have less than a 10-year life expectancy generally aren’t offered screening.
One vital caveat: screening is for men with no symptoms. If you already have urinary changes, blood in your urine or semen, or new bone pain, that calls for evaluation, not a screening schedule.
⚠️ Clinical Warning: Symptoms such as blood in the urine, difficulty urinating, or persistent bone or back pain should be checked promptly by a clinician regardless of your age or screening history. Our guide to the early signs of prostate cancer explains which symptoms warrant prompt attention.
Frequently asked questions
1. At what age should I get my first PSA test?
For prostate cancer screening, most average-risk men have their first PSA conversation at 50. Black men and those with a father or brother diagnosed before 65 should start at 45, and men with several affected relatives or a BRCA mutation at 40. The right age depends on your risk, so confirm it with your clinician.
2. When should Black men start prostate cancer screening?
Black and African-ancestry men carry roughly 67% higher incidence and about twice the mortality of White men, so the ACS and AUA recommend starting the prostate cancer screening conversation at age 45 — or earlier if there is also a family history. Discuss your personal timing with a urologist or primary care clinician.
3. Does family history change when I should start?
Yes. A father or brother diagnosed with prostate cancer before 65 raises your risk and moves your screening start to 45. More than one such relative, or an inherited BRCA1 or BRCA2 mutation, moves it to 40. Genetic counseling may help if your family carries a known mutation, so ask your clinician.
4. Is prostate cancer screening worth it?
It is a genuine trade-off. For men 55 to 69, screening may prevent about 1.3 deaths and 3 metastatic cases per 1,000 men over roughly 13 years, but it also causes false alarms and overdiagnosis. Whether the benefit outweighs the harms depends on your age and risk, so weigh it with your clinician.
5. What are the harms of PSA screening?
The main harms are false positives, overdiagnosis, and overtreatment. A raised PSA may trigger a biopsy when no cancer exists, and screening can detect cancers that never would have caused harm, in an estimated 20% to 50% of screen-detected cases. Treatment of those cancers can cause incontinence and erectile dysfunction.
6. How often should I repeat a PSA test?
For men who choose screening, the AUA suggests a PSA every 2 to 4 years between ages 50 and 69, tailored to your risk and prior results. Men with a very low baseline reading may safely extend the interval. Your clinician sets the right frequency for your situation.
7. What is a normal PSA level for my age?
There is no single normal value, because PSA reference ranges rise with age — roughly 2.5 ng/mL in your 40s, 3.5 in your 50s, 4.5 in your 60s, and 6.5 in your 70s. These are general references, not diagnostic cut-offs, and only a clinician can interpret your result in context.
8. Does a high PSA mean I have cancer?
No. A high PSA is not a cancer diagnosis. Levels can rise from an enlarged prostate, infection, inflammation, or recent activity, and a newly elevated result is usually repeated before any further step. Many raised PSA results turn out to be benign, so discuss next steps with a urologist.
9. At what age should I stop screening?
The USPSTF recommends against routine PSA screening at 70 and older, and the ACS advises against screening men without symptoms who have less than a 10-year life expectancy. Overall health, not age alone, drives the decision. If you are weighing whether to continue, discuss it with your clinician.
10. Is the digital rectal exam still part of screening?
The PSA blood test is the primary prostate cancer screening tool. A digital rectal exam may be used alongside it to add information, but it is no longer recommended as a stand-alone screen. Whether a DRE adds value in your case is a decision to make with your clinician.
11. Should I get screened if I have no symptoms?
Yes — screening is specifically for men without symptoms, which is the whole point of early detection. If you already have urinary changes, blood in your urine, or bone pain, that is a reason for evaluation rather than routine screening. Bring any symptoms to a clinician promptly.
Your next step
Your starting age comes down to one thing: your risk. Average risk points to a conversation at 50, higher risk at 45, and the highest risk at 40 — and the decision is always shared with a clinician who knows your history.
The most useful move now is to book that conversation and bring your questions to it. If you’d like the wider context of symptoms, staging, and treatment, our full prostate cancer overview walks through it.
Screening is a choice, not an obligation. Understanding the trade-offs, and where you personally fall, is how you make that choice on your own terms.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.