On This Page – Quick Medical Summary
A high PSA result is scary — but it often isn’t cancer
Seeing the word “elevated” next to your PSA result can make your stomach drop. The fear that jumps to mind — cancer — is understandable, but a single high number is a signal to look closer, not a diagnosis.
This guide is built to meet you wherever you are. If you just got an abnormal prostate-specific antigen result and want to understand what it means, the next two sections explain what PSA measures and the common non-cancer reasons it climbs. If you take a medication like finasteride, the section on medications matters most for you. If you want to know what happens next, the workup section walks through it step by step.
Here is the reassuring reality up front: most elevated results are not cancer. Among men who go on to have a biopsy because of a high PSA, only about a quarter are found to have prostate cancer.
ℹ️ Medical Disclaimer: This article is educational information about elevated PSA results, the conditions and medications that affect them, prostate cancer screening, and related testing. It is not a diagnosis, a treatment plan, or medical advice, and it does not replace your own clinician. Reading it does not create a doctor–patient relationship. Decisions about testing, medications, and follow-up must be made with a licensed clinician — ideally a urologist — who knows your history. If you have severe or sudden symptoms, seek medical care right away.
What a high PSA actually measures (and what “high” means)
PSA is a protein your prostate makes, and it shows up normally in every man’s blood. The PSA test simply measures how much is circulating — it does not, on its own, tell you why a level is high.
Where PSA comes from and why it rises
Both healthy prostate cells and cancerous ones produce PSA, so anything that irritates, enlarges, or inflames the gland can push the number up. That is the central reason an elevated result is not the same as cancer.
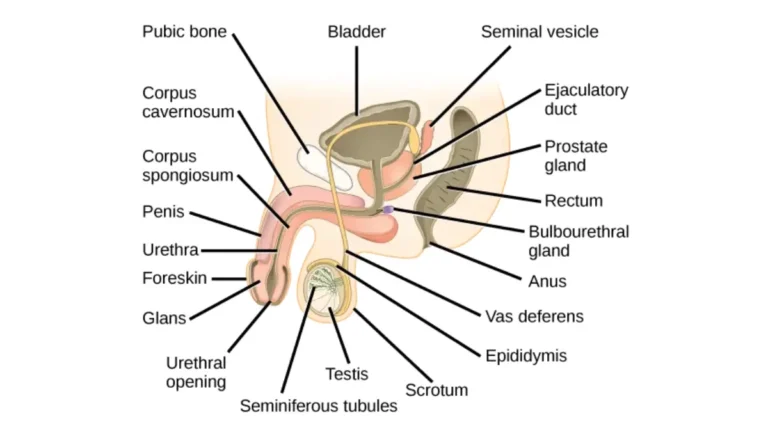
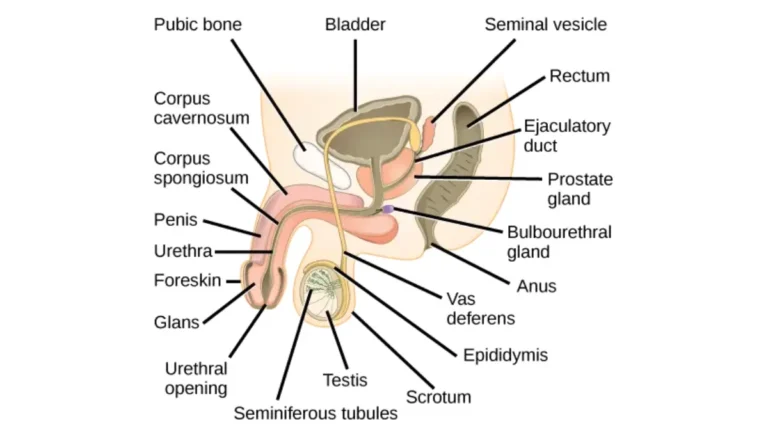
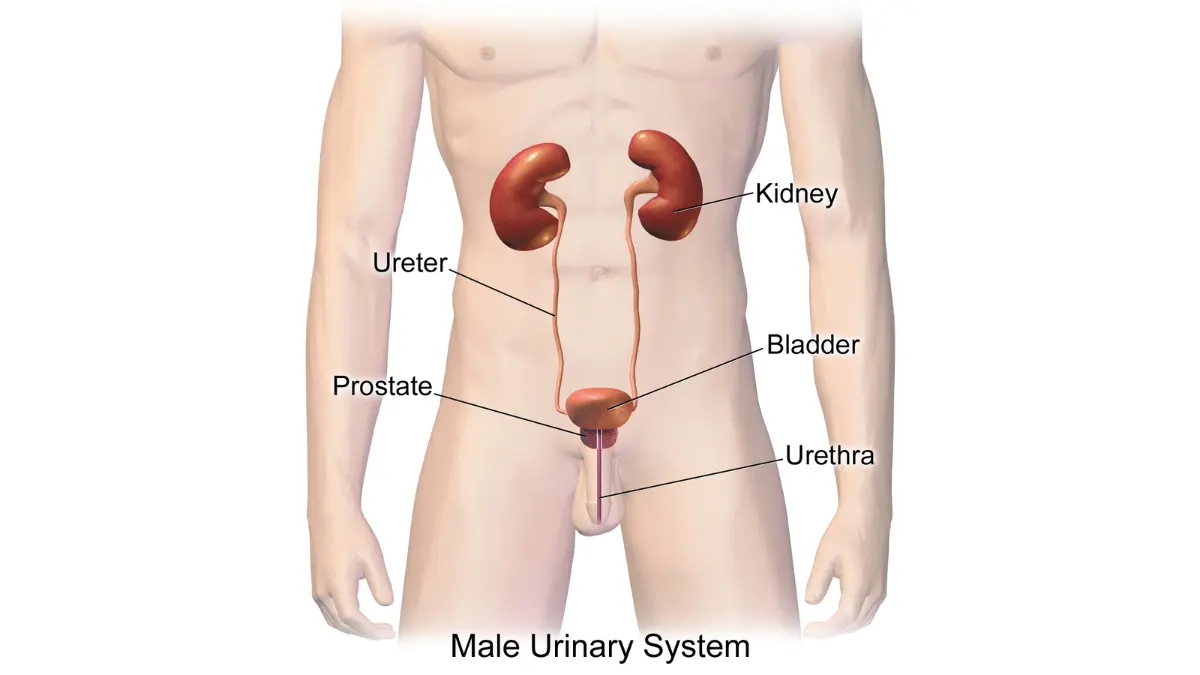
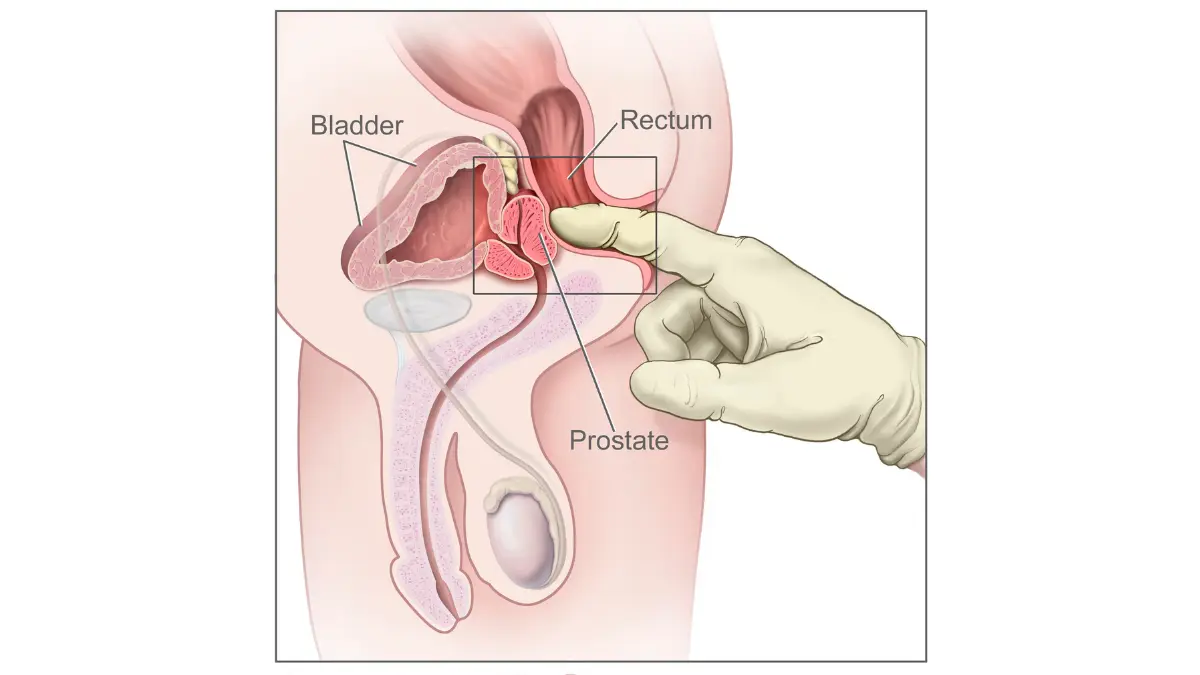
🔬 How It Works: The prostate sits just below the bladder and surrounds the urethra. When prostate tissue grows, becomes inflamed, or is disturbed, more PSA leaks into the bloodstream — which is why a raised level points to “something is going on with the prostate,” not to one specific cause.
Is there a “normal” PSA level?
There is no single universal cutoff. PSA tends to drift upward with age, and the level once treated as a rough dividing line — around 4 ng/mL — is now understood as a starting point for discussion, not a verdict.
📊 Clinical Data Point: Only about 25% of men who have a biopsy because of an elevated PSA are found to have prostate cancer — Source: National Cancer Institute, PSA Test Fact Sheet.
In general, the chance of cancer rises as the level rises, but a higher number still has many possible explanations. For more on how the numbers are read at different ages, see our guide to PSA test levels by age, and for the foundational basics you can read MedlinePlus’s plain-language PSA test page.
Common reasons for a high PSA that aren’t cancer
Most of the conditions that raise PSA are benign, and several are temporary. Knowing them can turn a frightening result into a question you can actually work through with your clinician.
Common non-cancer causes of a high PSA include:
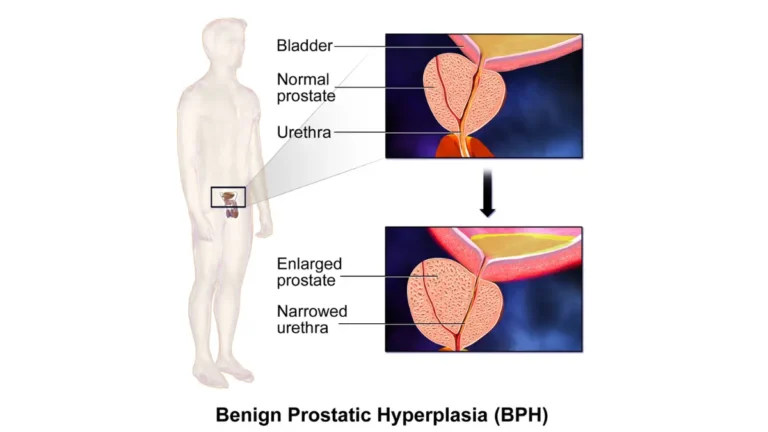
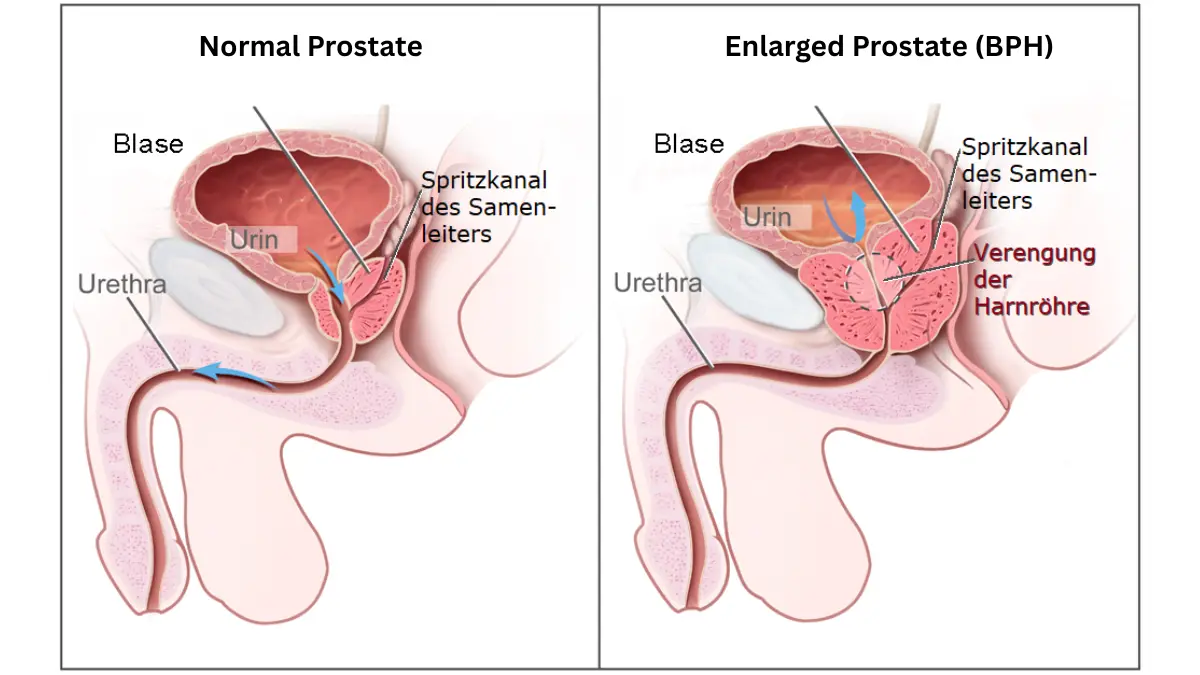
- Benign prostatic hyperplasia (BPH) — a non-cancerous enlargement of the prostate that becomes common with age
- Prostatitis — inflammation or infection of the prostate
- A urinary tract infection
- Recent ejaculation
- Vigorous exercise, especially cycling
- A recent digital rectal exam, catheter, or other prostate procedure
- Normal, age-related rises in PSA over time
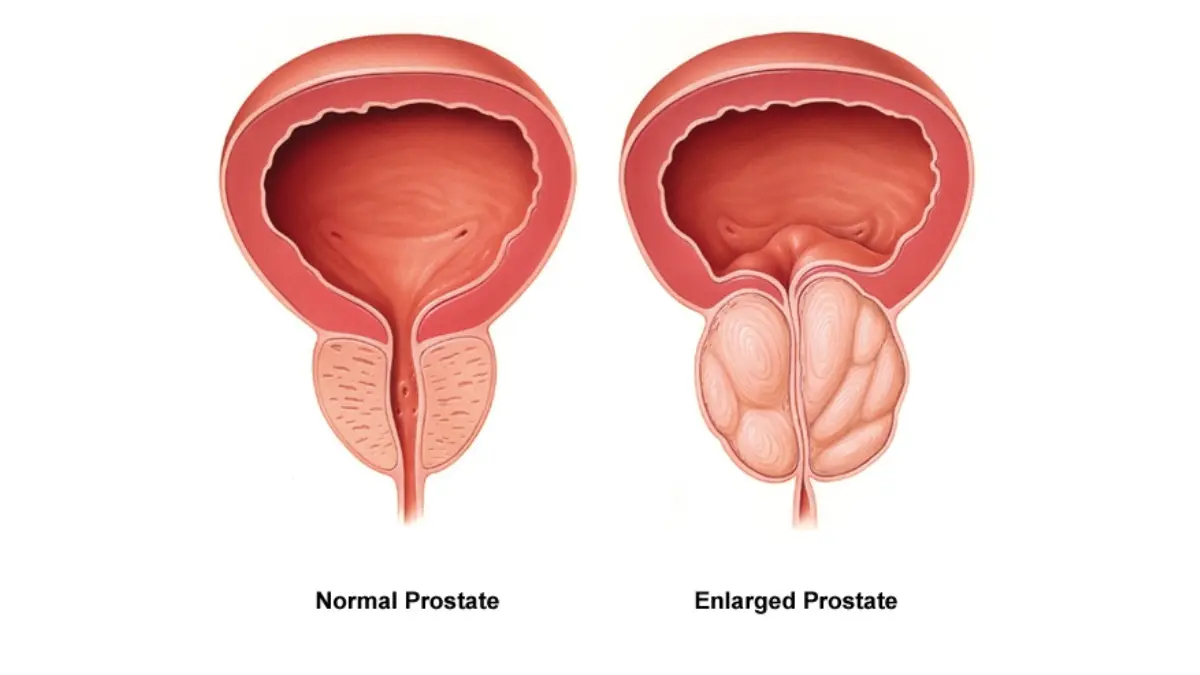
Enlarged prostate (BPH) and prostatitis
An enlarged prostate is among the most frequent benign reasons for an elevated PSA — more tissue simply makes more PSA. Prostatitis can raise the level too, and an active infection or inflammation can sometimes push it surprisingly high while still being benign.
Infections, ejaculation, cycling, exams and procedures
Several everyday things can nudge PSA upward for a short time, which is why preparation before a test matters. Recent ejaculation, hard cycling, a urinary tract infection, and recent prostate stimulation or instrumentation can all temporarily raise the reading.
Age and prostate size
PSA naturally tends to increase as you get older and as the prostate grows, even with no disease present. If urinary symptoms prompted your test, our guide to prostate cancer symptoms can help you sort which signs are worth raising, and you can run a quick check with the Symptom Checker.
Medications that can change your PSA reading — especially finasteride
One common reason for a misleading PSA is invisible unless someone asks about it: medication. A group of drugs called 5-alpha-reductase inhibitors can lower PSA substantially, which can make a result look more reassuring than it really is.
How finasteride and dutasteride lower PSA
Finasteride (taken for an enlarged prostate or, at a lower dose, for hair loss) and dutasteride both shrink prostate tissue, and as they do, your PSA falls.
🔬 How It Works: These medications block conversion of testosterone to a hormone that drives prostate growth. Less of that hormone means a smaller prostate and lower PSA output — so the number drops even when nothing has improved about your cancer risk.
📊 Clinical Data Point: Finasteride lowers total PSA by roughly 50% after about 6 to 12 months of use — Source: Prostate Cancer Prevention Trial analysis (National Library of Medicine / PubMed).
Why your reading may need to be interpreted differently
Because the drug roughly halves the number, clinicians often interpret a PSA on these medications as if it were about double the printed value. The exact adjustment can grow with longer use, which is why this is a conversation for your clinician rather than a calculation to do at home.
⚠️ Clinical Warning: If you take finasteride or dutasteride, an “in-range” PSA can be falsely reassuring. A level that looks normal may actually be elevated once the medication’s effect is accounted for — so the result has to be interpreted, not taken at face value.
✅ Patient Action: Before your PSA is interpreted, tell your prescribing clinician or urologist that you take finasteride or dutasteride (including the low-dose hair-loss version), and ask how your specific result should be adjusted. Details on how these are read appear on a Prostate Cancer Prevention Trial analysis of finasteride and PSA.
What to do after a high PSA result
A single elevated result rarely sends you straight to a biopsy. There is a methodical path that turns uncertainty into a plan, and the first step surprises many people.
- Repeat the PSA test before anything else, since levels fluctuate and often come back down.
- Add secondary tests that refine risk — such as free PSA, PSA density, an MRI, or a biomarker blood panel.
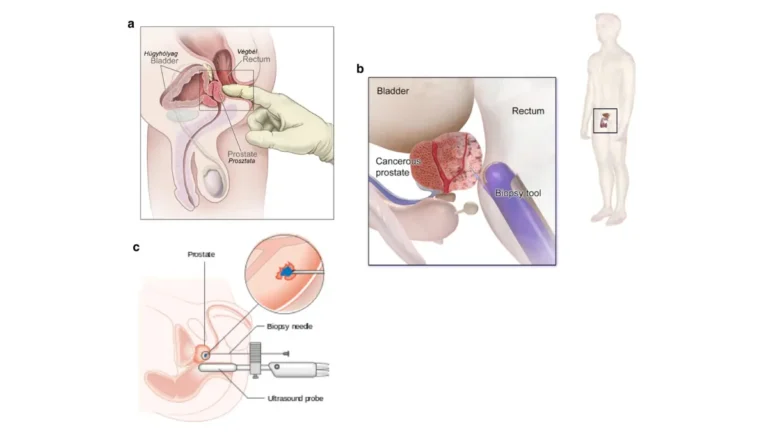
- Consider a prostate biopsy only if those results still point to meaningful risk.
Repeat the PSA before anything else
Guidelines advise rechecking a newly elevated PSA before ordering more tests, because a meaningful share of results normalize on a second draw. It also helps to avoid retesting right after ejaculation, hard exercise, or an infection, any of which can distort the value.
🩺 Physician Note: Current urology guidance emphasizes confirming a high PSA with a repeat test before moving to imaging or a biopsy. A common point of confusion is treating one elevated reading as final — in practice, the trend over repeated tests carries far more weight than any single number.
Secondary tests that refine the picture
If the level stays up, several tools can sharpen the picture before any biopsy. These include the percentage of “free” PSA, PSA density, multiparametric MRI, and biomarker panels — each adding information about how likely a meaningful cancer is.
When a prostate biopsy is considered
A biopsy becomes a considered decision, not an automatic next step, once the repeat test and any secondary tests are in. You can read more about these steps on the American Cancer Society’s guide to prostate-cancer tests.
✅ Patient Action: Ask your urologist, “Should we repeat my PSA first, and which test would you use next before considering a biopsy?” Bringing that exact question turns a vague worry into a clear plan.
How often does a high PSA actually turn out to be cancer?
Numbers help put the fear in proportion. The data consistently show that most elevated results are not cancer — while still being worth evaluating.
The numbers: false positives and biopsy results
📊 Clinical Data Point: About 6%–7% of men have a false-positive PSA on any given screening round, and only about 25% of those biopsied for an elevated PSA are found to have cancer — Source: National Cancer Institute, PSA Test Fact Sheet.
That second figure cuts both ways: most biopsies prompted by a high PSA do not find cancer, but a meaningful minority do, which is why a persistent elevation still deserves a workup rather than dismissal.
Screening guidelines and shared decision-making
Whether to screen at all is a personal, informed decision rather than an automatic one. Major U.S. guidance frames it by age and risk:
| Group | What major US guidance suggests | Key clinical detail |
|---|---|---|
| Men aged 55–69 | Make an individual decision after discussing the benefits and harms with a clinician | The USPSTF grades this a “C” — a shared, informed choice, not a routine test |
| Men 70 and older | Routine PSA screening is not recommended | The USPSTF grades this a “D”; expected harms generally outweigh benefits at this age |
| Higher-risk men (Black men, a strong family history, or a known inherited mutation) | A baseline conversation earlier, often around age 40–45 | The AUA/SUO guideline notes meaningfully higher risk in these groups |
Source: U.S. Preventive Services Task Force (2018); AUA/SUO Early Detection of Prostate Cancer guideline.
If a family history is part of your picture, the Genetic Risk Assessment Tool can help you frame the conversation, and the CDC’s overview of who should consider PSA screening lays out the trade-offs. If your workup does lead to a cancer diagnosis, our guide to prostate cancer stages explains what comes next.
When a high PSA or new symptoms need prompt medical attention
Most men reading this are not facing an emergency. Still, a few situations call for timely care, and a steadily climbing PSA should never simply be ignored.
Symptoms that warrant prompt evaluation
Some symptoms point to a problem that needs attention sooner rather than later, separate from cancer risk.
⚠️ Clinical Warning: Seek prompt medical care if a high PSA comes alongside a fever with chills and pelvic or urinary pain (possible acute prostate infection), a sudden inability to urinate, or visible blood in your urine. These warrant timely evaluation rather than waiting for a routine appointment.
Why a persistently rising PSA shouldn’t be ignored
A single high reading often settles on retesting, but a PSA that keeps climbing across repeated tests is a different signal. The pattern over time matters more than any one value, and a steady rise is worth following up even if each individual number seems modest.
✅ Patient Action: If your PSA has risen over two or more tests, book a follow-up with a urologist and ask, “Is this trend significant for my age, and what’s the next step to evaluate it?” Don’t let a rising pattern go unaddressed.
High PSA but no cancer: frequently asked questions
1. Can you have a high PSA and not have cancer?
Yes. A high PSA is a flag, not a diagnosis. Many elevations come from benign causes, and only about a quarter of men biopsied for an elevated PSA are found to have cancer. Your number should be interpreted in context, so discuss your specific result with your clinician.
2. What is the most common cause of a high PSA besides cancer?
An enlarged prostate, known as benign prostatic hyperplasia or BPH, is among the most common non-cancer causes, along with prostatitis. Both raise PSA without being cancer. A clinician can help work out which applies to you.
3. How high can PSA go without cancer?
Benign conditions like BPH, infections, and prostatitis can meaningfully raise PSA, and occasionally even a fairly high level turns out to be benign. That said, higher numbers more often prompt a cancer evaluation, so an elevated PSA still needs review by your clinician.
4. Should I repeat a high PSA test before a biopsy?
Usually, yes. Guidelines advise repeating a newly elevated PSA before any secondary test, imaging, or biopsy, because levels fluctuate and often normalize on a recheck. Your urologist will decide the timing based on your situation.
5. Can ejaculation or cycling raise PSA?
Yes. Recent ejaculation, vigorous exercise (especially cycling), a digital rectal exam, and recent prostate procedures can all temporarily raise PSA. These effects are short-lived and avoidable before a test, so ask your clinician how to prepare for an accurate PSA test.
6. How long should I wait after ejaculation before a PSA test?
Because recent ejaculation can temporarily raise PSA, many clinicians suggest abstaining for a short period beforehand. The exact interval varies, so ask your provider how long they want you to wait before your specific PSA test.
7. What PSA level is considered high?
There is no single universal “normal” PSA — it varies with age, and the chance of cancer rises as the level rises. A number once flagged as high still has many possible explanations. Your clinician interprets it for your age and history.
8. Does finasteride affect PSA results?
Yes. Finasteride and dutasteride lower PSA by roughly half, so an in-range reading can be misleading. Clinicians often interpret your value as if it were about doubled. Always tell your doctor you take these medications so your PSA is read correctly.
9. What tests come after a high PSA?
After confirming an elevation with a repeat test, options that refine risk before any biopsy include free PSA, PSA density, multiparametric MRI, and biomarker panels. Which ones fit depends on your situation, so discuss the choices with your urologist.
10. How often does a high PSA turn out to be cancer?
About 6% to 7% of men have a false-positive PSA on a given screening round, and only about 25% of those biopsied for an elevated PSA are found to have cancer. Most elevations are not cancer, but evaluation still matters.
11. When should I worry about a high PSA?
A PSA that keeps rising across repeated tests shouldn’t be ignored. Seek prompt care for symptoms like a fever with pelvic or urinary pain, an inability to urinate, or visible blood in the urine. When in doubt, contact your clinician.
The bottom line on a high PSA with no cancer
A high PSA is unsettling, but for most men it reflects something other than cancer — an enlarged prostate, inflammation, a recent activity, or a medication effect — and only a minority of biopsies prompted by an elevated level find cancer. The number is a starting point, not a sentence.
The path forward is calmer than the fear suggests: repeat the test, account for any medications, and work through the next steps with a clinician.
✅ Patient Action: Keep your follow-up appointment, bring a complete list of your medications (especially finasteride or dutasteride), and ask your urologist whether to repeat the PSA before any further testing. That single conversation puts you back in control of the result.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.