On This Page – Quick Medical Summary
If your care team has raised hormone therapy as part of your prostate cancer treatment, two questions are probably louder than the rest: what will it do to my body, and how long will I be on it? This guide answers both in plain language and points you to what to ask your own doctor.
Where you are shapes what matters most. If you were newly diagnosed and are weighing options, start with how it works and when it’s used. If treatment begins soon, the duration and side-effect sections matter most. If you’re a partner or caregiver, the management and “questions to ask” sections will help you support someone through it. If you have advanced or recurrent disease, the section on long-term treatment speaks to your situation.
Hormone therapy is also called androgen deprivation therapy (ADT) — one of the most established prostate cancer treatments, and one of the most misunderstood.
ℹ️ Medical Disclaimer: This article is general health information, not medical advice. It does not diagnose disease, recommend a specific treatment or medication, or replace your care team. Hormone therapy for prostate cancer is prescribed, dosed, and monitored by a qualified clinician, and both the type and the length of treatment are individual medical decisions. Do not start, stop, or change any treatment without speaking to a board-certified urologist or oncologist.
How hormone therapy works against prostate cancer
Prostate cancer cells usually depend on male hormones to grow — which is exactly what this treatment targets.
Why testosterone fuels prostate cancer
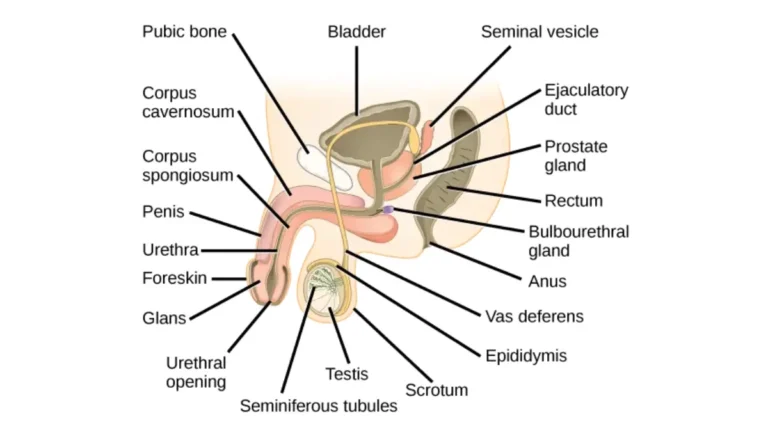
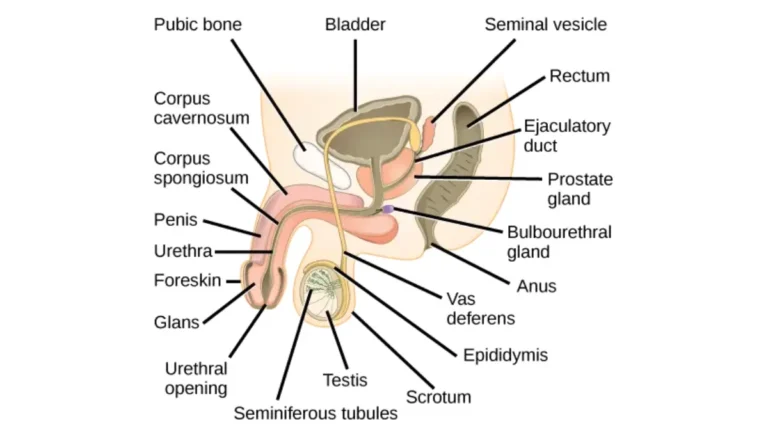
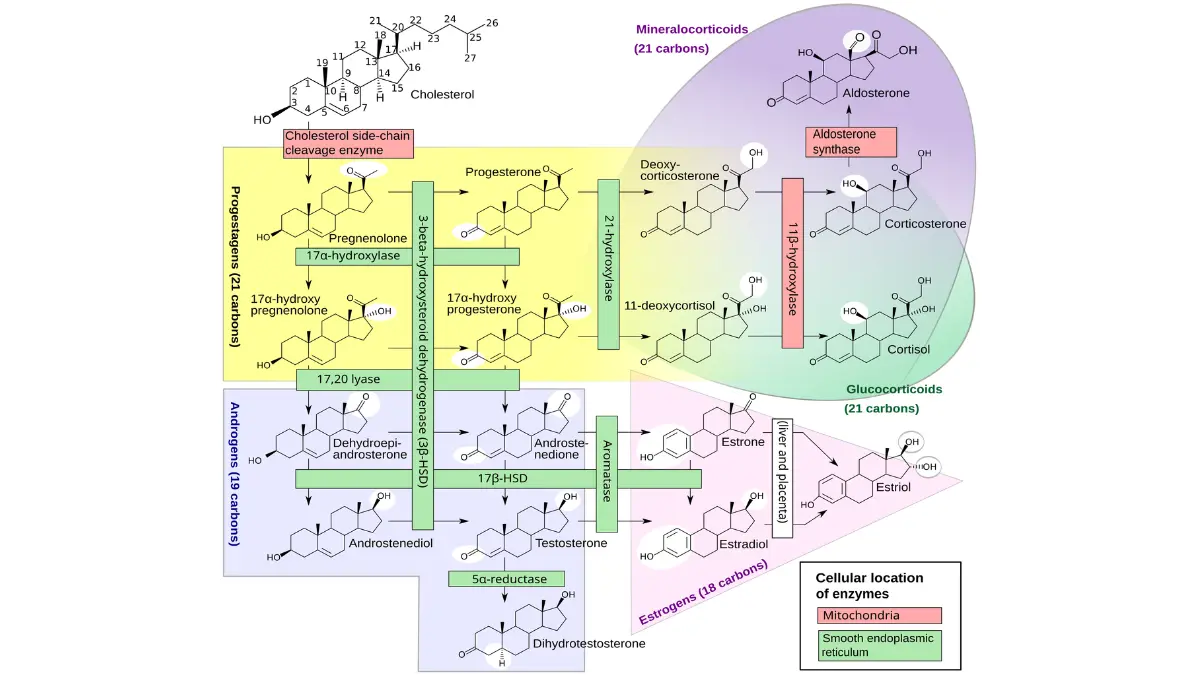
The main androgens in the body are testosterone and dihydrotestosterone (DHT), and most are made by the testicles. Prostate cancer cells use these hormones as fuel. Lowering androgen levels, or blocking them from reaching the cancer, can make many prostate cancers shrink or grow more slowly.
🔬 How It Works: Picture androgens as fuel for many prostate cancer cells. Hormone therapy either turns down the supply — less testosterone made — or blocks the cell’s fuel intake at the androgen receptor, so the cancer loses a key growth signal.
Is hormone therapy a cure?
On its own, hormone therapy does not cure prostate cancer. It controls the disease, often for years, but over time some cancers adapt and keep growing even when testosterone is very low — a stage called castration-resistant prostate cancer. That is why ADT is usually paired with other treatments rather than used alone. For more background, see the National Cancer Institute’s overview of hormone therapy.
When hormone therapy is used for prostate cancer
Hormone therapy is not for every prostate cancer; it is matched to specific situations.
With radiation for intermediate- and high-risk disease
For cancer still in or around the prostate that carries a higher chance of returning, ADT is often combined with radiation therapy, and sometimes started beforehand to shrink the tumor first. Understanding where this fits in your overall prostate cancer treatment can make the recommendation clearer.
For advanced, recurrent, or metastatic cancer
If cancer comes back after surgery or radiation, or has spread beyond the prostate, hormone therapy becomes a main treatment because it works throughout the body rather than in one spot.
Why it isn’t usually used alone for early-stage cancer
For low-risk, early-stage disease, ADT by itself has not been shown to help men live longer than careful monitoring, so it is generally not advised as a standalone treatment.
✅ Patient Action: Ask your radiation oncologist or urologist: “Given my risk group and PSA, is hormone therapy recommended alongside my other treatment, and what is it adding?”
The main types of hormone therapy
“Hormone therapy” is really a family of treatments that work in different ways — by injection, implant, pill, or surgery.
Lowering testosterone: surgery and injections
An orchiectomy surgically removes the testicles and permanently lowers testosterone. Most men instead choose medicines: LHRH agonists such as leuprolide and goserelin, and faster-acting LHRH antagonists such as degarelix (an injection) and relugolix (a daily pill).
📊 Clinical Data Point: Removing the testicles lowers blood testosterone by roughly 90–95%. — Source: National Cancer Institute, Hormone Therapy for Prostate Cancer.
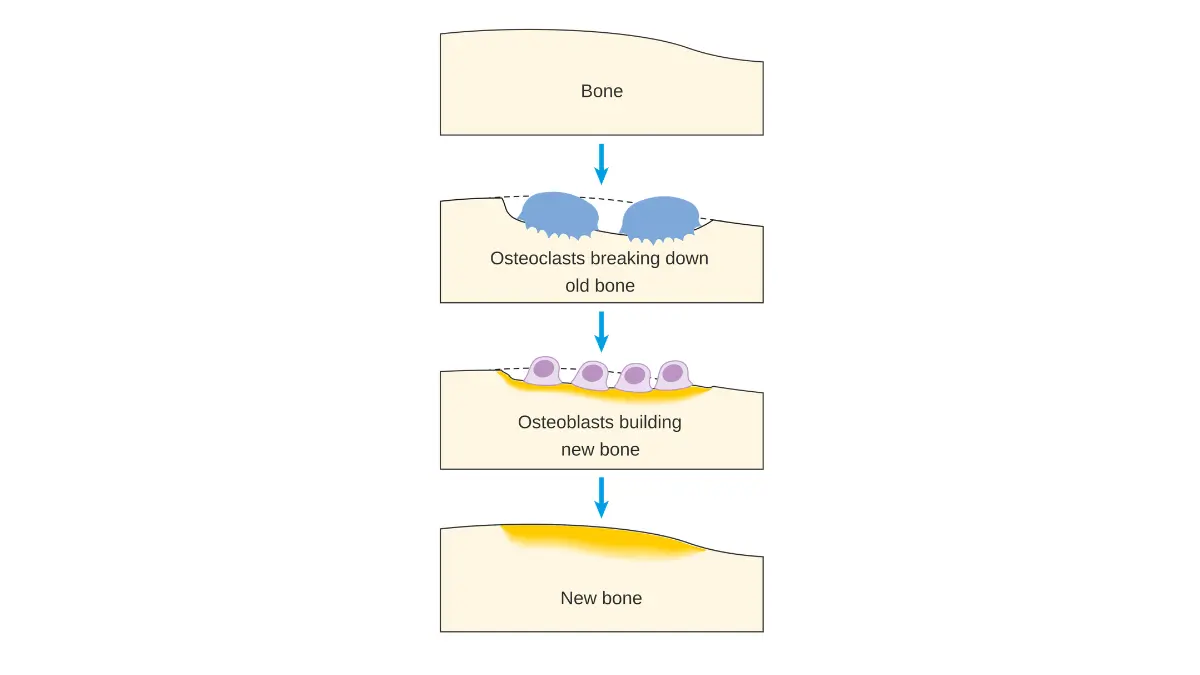
Diagram showing the position of the adrenal glands CRUK 343.svg
, licensed under CC BY-SA 4.0.
Blocking testosterone: anti-androgens and synthesis blockers
Anti-androgens — older drugs like bicalutamide and newer ones like enzalutamide, apalutamide, and darolutamide — block androgens from reaching cancer cells. Abiraterone works differently, shutting down androgen production, and is taken with a low dose of prednisone. The American Cancer Society’s guide to hormone therapy drugs lists each option in detail.
⚠️ Clinical Warning: When an LHRH agonist is first started, testosterone briefly rises — a “tumor flare” — which can temporarily worsen symptoms. In men whose cancer has reached the spine, this can rarely press on the spinal cord; new severe back pain, leg weakness, or numbness needs emergency care. A short course of an anti-androgen is often given to prevent flare.
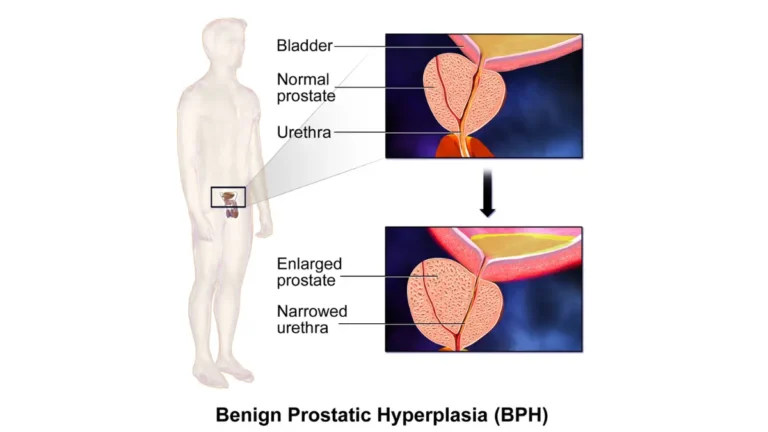
How long do you stay on hormone therapy?
How long you stay on hormone therapy depends on your situation: roughly 4–6 months when it is paired with radiation for intermediate-risk disease, about 18–36 months for high-risk disease, and ongoing treatment for advanced or metastatic cancer.
Short-term with radiation (intermediate risk)
For unfavorable intermediate-risk cancer treated with radiation, a short course of ADT — often around 4 to 6 months — is typical.
Long-term with radiation (high risk)
For high-risk localized disease, current AUA/ASTRO guidance (2022) recommends 18 to 36 months of hormone therapy alongside radiation, supported by a systematic review of how long hormone therapy is given with radiation. Knowing your risk group is what determines where in that range you fall.
Ongoing treatment for advanced cancer
When cancer has spread, hormone therapy is generally continued long-term — for as long as it keeps the disease in check — and is combined with other drugs.
Continuous vs. intermittent: can you take a break?
Some men use intermittent therapy, stopping when PSA drops low and restarting when it rises, to get a break from side effects; this is guided by how your PSA level is tracked. Whether intermittent treatment matches continuous treatment for survival is still debated.
🩺 Physician Note: Guidelines stress that duration is individualized — set by your risk group and how your PSA responds — not a fixed number. The ranges above are starting points for a conversation, not a personal prescription.
✅ Patient Action: Ask your oncologist: “For my risk group, how many months are you recommending, and is intermittent treatment an option for me?”
Side effects of hormone therapy — and how they’re managed
Lowering testosterone has predictable effects, and many can be eased or prevented.
Common effects
The most common are hot flashes, reduced sex drive, erectile dysfunction, fatigue, and breast tenderness or growth. Many of these ease over time or after treatment ends.
Longer-term effects
Over months, ADT can thin the bones and raise fracture risk, cause weight gain and muscle loss, raise cholesterol, and affect mood, memory, or concentration. A simple way to monitor one of these at home is to track changes in your weight.
Heart health and other risks
Some research suggests a higher risk of high blood pressure, diabetes, stroke, and heart attack with hormone therapy, though not all studies agree — which is why your heart health should be monitored during treatment.
What helps
Bone-protecting medicines, certain drugs for hot flashes, and regular exercise all reduce the burden; exercise in particular helps fatigue, weight, and bone and muscle loss. If you’re cleared to start, it helps to build a safe exercise routine around the right intensity.
✅ Patient Action: Ask your care team: “Which side effects am I most at risk for, and do you recommend a baseline bone-density scan and an exercise plan?”
Talking with your care team about hormone therapy
The most useful thing you can do is turn this information into specific questions.
Questions about your type and duration
Bring these to your appointment: which type of hormone therapy you’ll have and why, how many months are planned, whether intermittent treatment is an option, and how your PSA will be tracked. The full prostate cancer staging and treatment guide can help you see where this step fits.
Questions about managing effects
Ask which side effects are most likely for you, what can be done to prevent bone loss, and when to call about symptoms like new back pain. Write the answers down — treatment spans months, and details are easy to forget.
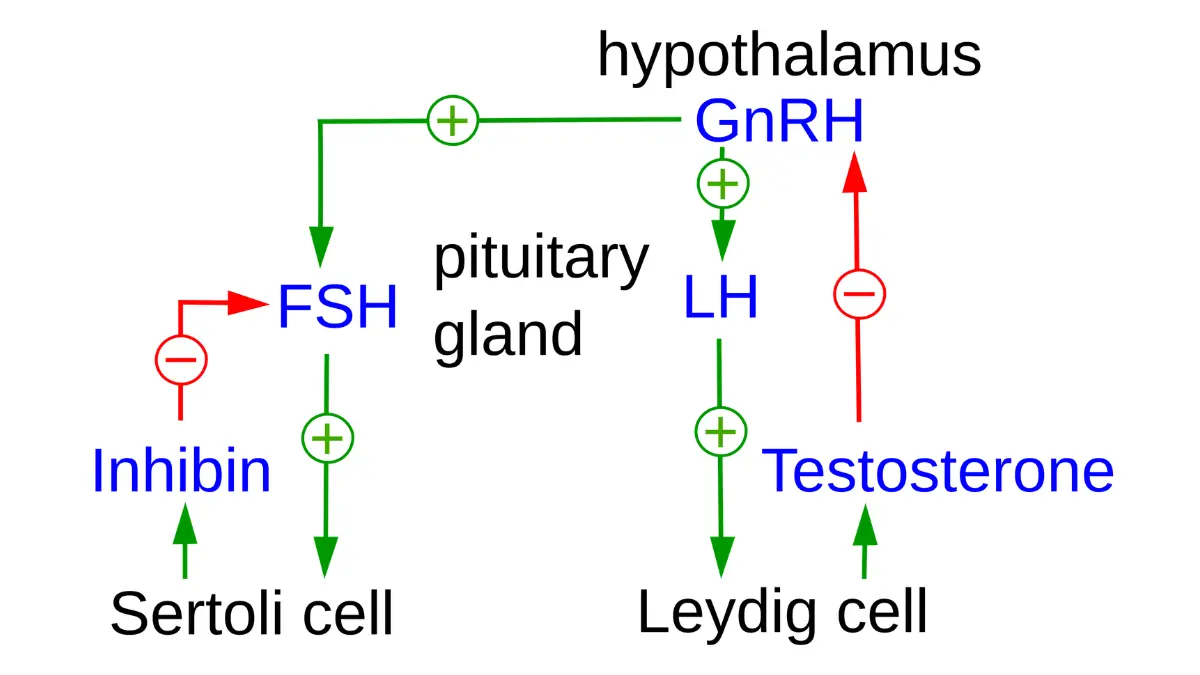
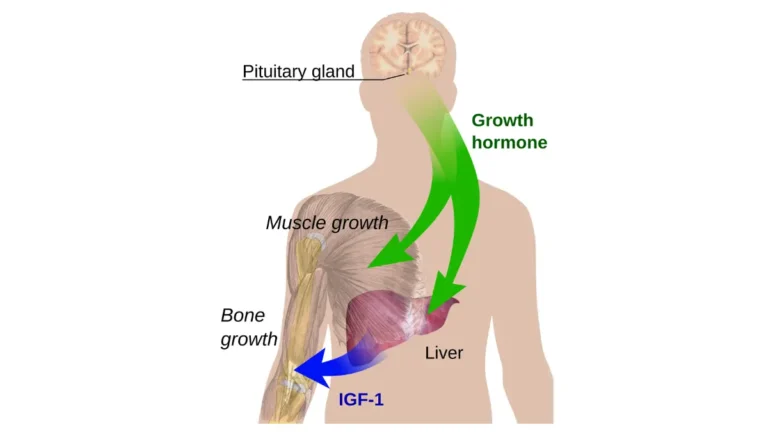
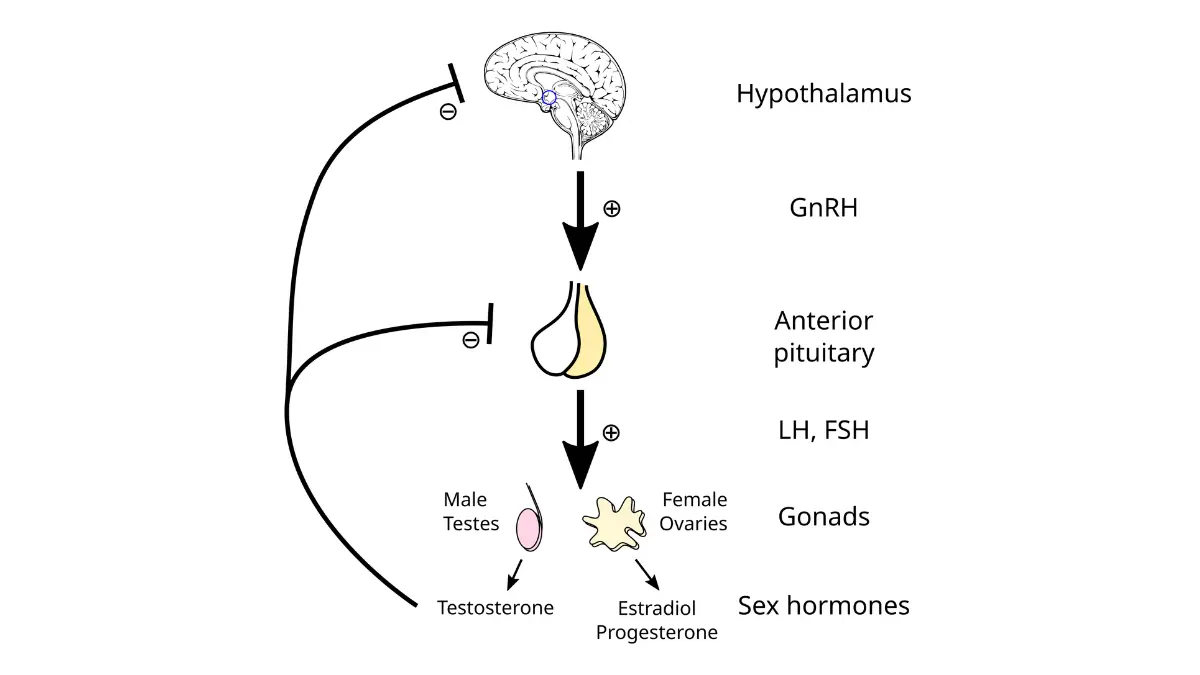
Hypothalamus-Hypophysis-Testicle-Hormone-Axis (engl.).svg
, licensed under CC BY-SA 3.0.
Frequently asked questions about hormone therapy for prostate cancer
1. What is hormone therapy for prostate cancer?
Hormone therapy, or androgen deprivation therapy (ADT), lowers male hormones or blocks them from reaching prostate cancer cells, which slows the cancer’s growth. It is one of the main prostate cancer treatments, but it does not cure the disease on its own.
2. How does hormone therapy work?
Prostate cancer cells use androgens like testosterone as fuel. Hormone therapy either reduces how much testosterone the body makes or blocks the androgen receptors on cancer cells, removing a key growth signal so many cancers shrink or grow more slowly.
3. How long do you stay on hormone therapy for prostate cancer?
It depends on your situation: about 4–6 months with radiation for intermediate-risk disease, roughly 18–36 months for high-risk disease, and ongoing treatment for advanced cancer. Your care team sets the exact length based on your risk and PSA response.
4. Is hormone therapy a cure for prostate cancer?
No. Hormone therapy controls prostate cancer, often for years, but does not cure it alone, and some cancers eventually grow despite low testosterone. It is usually combined with other treatments, so discuss your specific plan with your oncologist.
5. What are the main side effects of hormone therapy?
Common effects include hot flashes, lower sex drive, erectile dysfunction, fatigue, and breast tenderness. Over time it can also thin bones, cause weight gain and muscle loss, raise cholesterol, and affect mood or memory. Many of these can be managed.
6. Do hormone therapy side effects go away after you stop?
Many effects, such as hot flashes and low sex drive, often ease or reverse after treatment ends, though recovery can take time. Some, like bone thinning, need active prevention during treatment. Ask your doctor which of your effects are likely to be temporary.
7. What’s the difference between LHRH agonists and antagonists?
Both lower testosterone. Antagonists like degarelix and relugolix work faster and avoid the early “tumor flare” that agonists like leuprolide and goserelin can cause. Your clinician chooses based on your situation, including how quickly testosterone needs to drop.
8. Can hormone therapy be taken as a pill?
Yes — some forms are pills, including relugolix, anti-androgens such as bicalutamide and enzalutamide, and abiraterone. Others are injections or implants, and orchiectomy is surgery. Which form is right depends on your cancer and plan, so ask your care team.
9. What’s the difference between continuous and intermittent hormone therapy?
Continuous therapy keeps testosterone low without breaks. Intermittent therapy pauses when PSA drops and restarts when it rises, giving a break from side effects. Whether the two are equal for survival is still debated, so discuss the trade-offs with your oncologist.
10. What is castration-resistant prostate cancer?
It means prostate cancer is still growing even though testosterone is at very low (castration) levels. Some of these cancers still respond to other hormone-based drugs, such as abiraterone or newer anti-androgens. A specialist can explain which options fit your case.
11. Can you take a break from hormone therapy?
Sometimes. Intermittent hormone therapy is built around planned breaks, usually guided by your PSA level, to reduce side effects. Whether breaks are right for you depends on your disease and response, so never stop treatment without talking to your oncologist first.
The bottom line on hormone therapy
Hormone therapy is a powerful, well-established way to control prostate cancer by lowering or blocking the hormones that feed it. Its effects are real but largely manageable, and many ease after treatment ends. How long you stay on it is not one-size-fits-all — from a few months with radiation to ongoing treatment for advanced disease — and your care team sets the plan around your risk and response. Use this guide to ask sharper questions at your next appointment, where your individual plan takes shape.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.