On This Page – Quick Medical Summary
If your oncologist has raised chemotherapy for prostate cancer, you are probably here for one of three reasons. Maybe you were recently told the cancer has spread and chemo is now on the table — start with when it’s used and whether it works. Maybe you are a caregiver trying to picture what treatment days involve — the sections on how it’s given and what to expect are written for you. Or maybe you are weighing chemo against other treatments and want the honest evidence — head to the survival data and decision sections.
Here is the reassurance to hold onto first. Hearing the word “chemotherapy” does not mean the situation is hopeless. Chemo is one specific tool, used at specific points in advanced prostate cancer, and for many men it adds meaningful time and eases symptoms.
This guide explains exactly when chemo is used, which drugs are involved, what treatment feels like, and what the evidence actually shows — with every fact tied to a named medical authority.
ℹ️ Medical Disclaimer: This article is general health education — not a diagnosis, treatment plan, or medication recommendation for your specific situation. Decisions about chemotherapy, hormone therapy, other prostate cancer drugs, and any procedure should be made with a board-certified medical oncologist or urologist who knows your full medical history. Do not start, stop, or change any treatment based on this page alone.
When is chemotherapy used for prostate cancer?
Chemotherapy is used for prostate cancer that has spread beyond the prostate (metastatic disease) — not for early-stage cancer still confined to the gland. It enters care in two distinct situations: alongside hormone therapy when the cancer is newly metastatic, or later, after hormone therapy stops controlling it.
Chemo with hormone therapy in newly metastatic disease
When prostate cancer has already spread but still responds to hormone treatment — called metastatic hormone-sensitive prostate cancer — doctors may add docetaxel chemotherapy to androgen deprivation therapy (ADT) from the start. This combination is offered mainly to men with a higher burden of disease. You can read more about how hormone therapy works for prostate cancer, the backbone of most advanced treatment, and review the National Cancer Institute’s prostate cancer treatment overview.
Chemo for castration-resistant prostate cancer
Over time, prostate cancer can keep growing even when hormone levels are very low — known as castration-resistant prostate cancer. At this stage chemotherapy becomes a main option to slow the cancer and relieve symptoms such as bone pain.
Why chemo isn’t used for early-stage prostate cancer
For cancer still confined to the prostate, treatments like surgery, radiation therapy, or active surveillance are standard, and chemo adds no benefit there. Where chemo fits depends on the stage of the cancer.
✅ Patient Action: Before treatment planning, ask your medical oncologist: “Is my cancer still hormone-sensitive or castration-resistant, and does that make chemotherapy the right choice now or later in the sequence?”
Which chemo drugs are used for prostate cancer?
Two chemotherapy drugs do most of the work in prostate cancer: docetaxel and cabazitaxel, each given together with a steroid such as prednisone. Both belong to a drug class called taxanes, and both have been shown to help men live longer on average than older chemo drugs.
Docetaxel (Taxotere) — the usual first chemo
Docetaxel is almost always the first chemo drug used. The U.S. Food and Drug Administration (FDA) approved it for advanced prostate cancer in 2004, and it is paired with a steroid to improve how well it works and to reduce reactions, per the American Cancer Society’s overview of chemo for prostate cancer.
Cabazitaxel (Jevtana) — when docetaxel stops working
If docetaxel stops controlling the cancer, cabazitaxel is often the next chemo drug tried, also alongside a steroid. The FDA approved cabazitaxel in June 2010, specifically for men whose cancer progressed during or after docetaxel.
How taxanes work and why a steroid is added
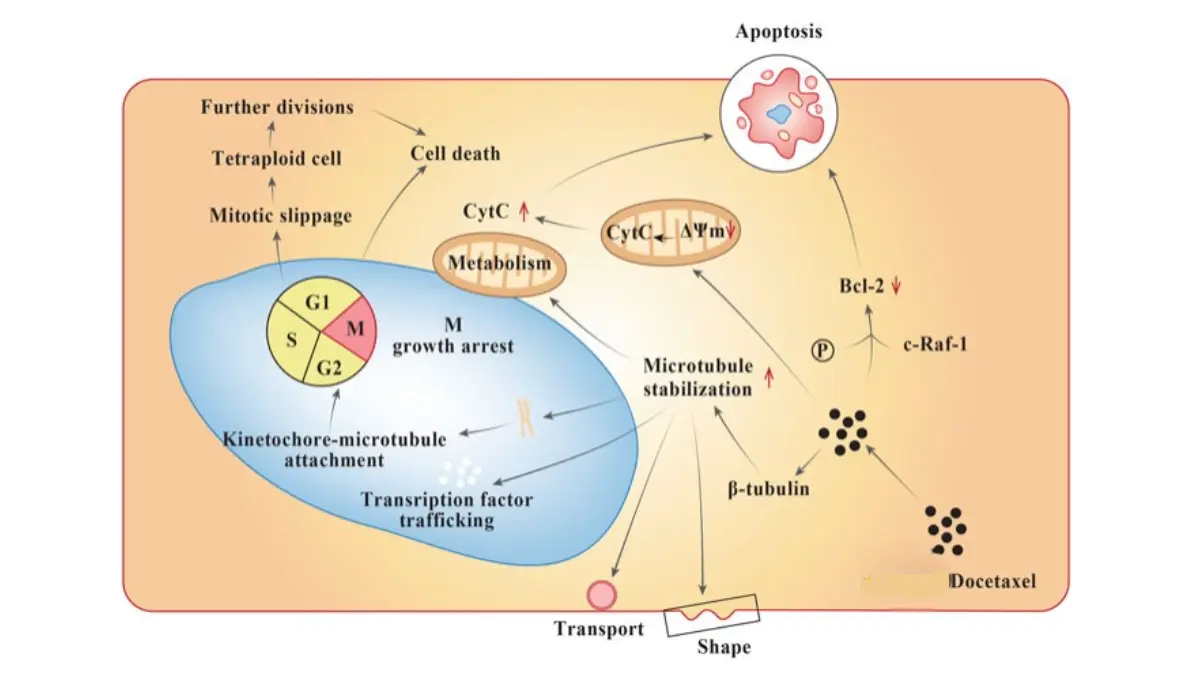
🔬 How It Works: Cancer cells must copy themselves and divide in order to spread. Taxanes like docetaxel jam the internal “scaffolding” (called microtubules) that a cell needs to split in two, which stops cancer cells from multiplying. Cabazitaxel was designed to keep working even when cancer cells have learned to pump docetaxel back out — which is why it can still help after docetaxel fails.
The steroid is given with chemo to lower the risk of allergic reactions and to add a modest anti-cancer effect of its own.
How is chemotherapy for prostate cancer given?
Chemotherapy for prostate cancer is given as an intravenous (IV) infusion — the drug drips into a vein — usually once every three weeks in repeating cycles. Treatment takes place in a doctor’s office, an infusion clinic, or a hospital.
What an infusion day looks like
On treatment day you typically receive premedication first, then the chemo infusion over roughly an hour, with monitoring throughout. Most men go home the same day.
How many cycles and how long it takes
The number of cycles depends on the situation. When docetaxel is added to hormone therapy for newly metastatic disease, it is commonly given for about six cycles. In castration-resistant disease, treatment continues as long as it keeps helping and side effects stay manageable. Your oncologist sets your exact schedule.
Premedication and monitoring
Before each infusion you are given medicines — often including a steroid — to reduce the chance of an infusion reaction. Your blood counts are checked regularly, because chemo can temporarily lower them.
What are the side effects of chemotherapy for prostate cancer?
Chemotherapy affects fast-growing healthy cells along with cancer cells, which is what causes most side effects. Many are manageable, but a few need urgent attention.
Common side effects
According to the American Cancer Society, common effects of docetaxel and cabazitaxel include fatigue, hair loss, nausea, mouth sores, and temporarily low blood counts. These often ease in the days between cycles.
Serious side effects to report right away
Taxanes can cause peripheral neuropathy — numbness, tingling, or burning in the hands or feet — and occasionally severe allergic or infusion reactions, which is why premedication is given. A drop in infection-fighting white blood cells, called neutropenia, is the most dangerous risk.
⚠️ Clinical Warning: A fever during chemotherapy can signal febrile neutropenia — a low white-cell count combined with infection — and it is a medical emergency. If your temperature reaches the threshold your care team gave you (often 100.4°F / 38°C or higher), contact them or seek emergency care immediately. Do not wait, and do not try to manage it at home.
How side effects are managed
Your oncology team monitors your blood counts and can adjust the plan to keep you safe. Reporting any new symptom early gives them the best chance to treat it before it worsens.
✅ Patient Action: Ask your oncology care team: “Exactly what temperature or symptoms should make me call you right away, and what is my plan if I develop a fever after an infusion?”
Does chemotherapy work for prostate cancer?
Chemotherapy does not cure prostate cancer, but for many men it extends life and eases symptoms. In clinical trials the benefit is measured as overall survival — how long groups of men lived, on average.
Chemo doesn’t cure prostate cancer — but it can extend life
The honest framing matters. Chemo is not a cure, and roughly half of men respond to docetaxel at first, with resistance often developing within several months. What it reliably offers is time and symptom relief, which for many men is meaningful.
How much it helps, by setting
Trial results below are reported as medians — the midpoint of a group, not a prediction for any one person.
| Treatment setting | Chemo compared with | Median overall survival | Key clinical detail |
|---|---|---|---|
| High-volume metastatic, hormone-sensitive | Docetaxel + hormone therapy vs. hormone therapy alone | ~57.6 vs. 44.0 months | Benefit concentrated in higher-burden disease (CHAARTED) |
| Castration-resistant, first chemo | Docetaxel + steroid vs. older chemo (mitoxantrone) | ~18.9 vs. 16.5 months | Established docetaxel as the standard first chemo (TAX 327) |
| After docetaxel | Cabazitaxel + steroid vs. older chemo | ~15.1 vs. 12.7 months | Works after docetaxel resistance develops (TROPIC) |
Source note: Figures are from the named phase III trials (CHAARTED, Sweeney et al.; TAX 327, Tannock/Berthold et al.; TROPIC, de Bono et al.). Medians are group midpoints, not individual predictions, and your own outlook depends on factors your oncologist can explain.
🩺 Physician Note: A common point of confusion is that giving chemo earlier — alongside hormone therapy in newly metastatic disease — is not a sign the cancer is more dangerous. It is a strategy supported by trial evidence to extend survival in men with a higher burden of disease.
Why it isn’t a permanent fix
Cancer cells can adapt and resume growing, which is why chemo is given in courses and why doctors plan the next steps in advance. For a fuller picture of outcomes in advanced disease, see our guide to life expectancy with stage 4 prostate cancer.
What to know before starting chemo — and what happens if it stops working
Chemotherapy is a deliberate choice with real alternatives, and it is rarely the end of the road. Knowing the other options and the likely next steps helps you stay in control of your care.
Questions to ask your oncologist
Bring specific questions: what benefit is realistic for your situation, what the side-effect plan is, and whether a clinical trial is a fit.
Chemo isn’t the only option
Other treatments for advanced prostate cancer include hormone-pathway drugs such as abiraterone and enzalutamide, the bone-targeted drug radium-223, newer radioligand (PSMA-targeted) therapy, the immunotherapy sipuleucel-T, and clinical trials. The right sequence is individualized to each man.
What happens if chemo stops working
If one chemo drug stops helping, others may still work, and treatment can move between chemo and hormone-pathway drugs depending on what you have already had. For example, after docetaxel and a hormone-pathway drug, cabazitaxel has been shown to extend survival as a later-line option in the CARD trial.
✅ Patient Action: Ask your medical oncologist: “If this chemotherapy stops working, what are my next treatment options, and am I eligible for any clinical trials?”
Frequently asked questions about chemotherapy for prostate cancer
1. When is chemotherapy used for prostate cancer?
Chemotherapy for prostate cancer is used when the cancer has spread beyond the prostate. It is given in two situations: alongside hormone therapy in newly metastatic, hormone-sensitive disease, and later in castration-resistant disease after hormone treatment stops working. It is not used for early-stage cancer confined to the gland.
2. Is chemo used for early-stage prostate cancer?
No. For prostate cancer still confined to the gland, standard options are surgery, radiation therapy, or active surveillance, and chemotherapy offers no added benefit. Chemo is reserved for cancer that has spread. Your treatment plan should be set with a urologist or medical oncologist based on your stage.
3. Can you have chemo and hormone therapy at the same time for prostate cancer?
Yes. In metastatic hormone-sensitive prostate cancer, docetaxel chemotherapy is often combined with androgen deprivation therapy (hormone therapy) from the start, mainly for men with a higher burden of disease. Trial evidence supports this combination. Ask your medical oncologist whether it applies to your specific situation.
4. How many cycles of chemo do you get for prostate cancer?
It depends on the setting. When docetaxel is added to hormone therapy for newly metastatic disease, it is commonly given for about six cycles. In castration-resistant disease, chemotherapy continues as long as it keeps helping and side effects stay manageable. Your oncologist sets your exact schedule.
5. What are the most serious side effects of chemo for prostate cancer?
The most dangerous risk is neutropenia — a drop in infection-fighting white blood cells. A fever during chemo can signal febrile neutropenia, a medical emergency. Severe allergic reactions and peripheral neuropathy (numbness or tingling in the hands or feet) can also occur. Contact your care team immediately about any fever.
6. Does chemo cure prostate cancer?
No, chemotherapy does not cure prostate cancer. For many men it extends life and relieves symptoms such as bone pain, but the cancer is not eliminated, and resistance often develops over time. The goal is to control the cancer and improve quality of life. Discuss realistic expectations with your medical oncologist.
7. How much does chemo extend life in prostate cancer?
It varies by setting. In high-volume metastatic hormone-sensitive disease, adding docetaxel to hormone therapy raised median overall survival to about 57.6 versus 44.0 months in the CHAARTED trial. These are group midpoints, not personal predictions. Your own outlook depends on factors your oncologist can explain.
8. What chemo drugs are used for prostate cancer?
The two main chemotherapy drugs are docetaxel (Taxotere) and cabazitaxel (Jevtana), both taxanes given with a steroid such as prednisone. Docetaxel is usually first; cabazitaxel is typically used if docetaxel stops working. Both have been shown to help men live longer than older chemo drugs.
9. What happens if chemo stops working for prostate cancer?
If one chemo drug stops helping, other treatments may still work. Care can shift between chemotherapy and hormone-pathway drugs such as abiraterone or enzalutamide, depending on what you have already received. For example, cabazitaxel can extend survival after docetaxel and a hormone-pathway drug. Ask your oncologist about your next options and trials.
10. Is chemotherapy a last resort for prostate cancer?
Not necessarily. Chemo is now sometimes given earlier — alongside hormone therapy in newly metastatic disease — rather than only after other treatments fail. It is one tool used at specific points, and several treatment lines often follow it. The best sequence is individualized to each man’s disease.
11. How is chemo for prostate cancer given?
Chemotherapy for prostate cancer is given as an intravenous (IV) infusion, usually once every three weeks in repeating cycles, at a doctor’s office, infusion clinic, or hospital. You receive premedication first, then the infusion over about an hour, and most men go home the same day. Blood counts are checked regularly.
The bottom line on chemotherapy for prostate cancer
Chemotherapy for prostate cancer is used only when the cancer has spread — either alongside hormone therapy in newly metastatic disease, or in castration-resistant disease after hormone treatment stops working. It is not a cure, but for many men it adds meaningful time and eases symptoms, and it is rarely the last step, with several other treatment lines often available.
If chemo is on the table for you, the most useful next move is a focused conversation with your medical oncologist about realistic benefit, the side-effect plan, and what comes next. For the full picture of how every stage and treatment fits together, see our pillar guide to prostate cancer signs, stages, and how treatment works.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.