On This Page – Quick Medical Summary
If you or someone you love was just told the prostate cancer is stage 4, the first question is almost always the hardest one: how long. This page answers that honestly — with the most current verified survival figure, an explanation of why other websites show a different number, and a clear look at the treatments that can extend life and control the disease.
How you use this page depends on where you are right now. If you are newly diagnosed, start with what stage 4 actually means and then the survival section. If you are a caregiver trying to understand a partner’s or parent’s diagnosis, the symptoms and treatment sections will help you follow the care plan. If you are comparing treatment options, skip ahead to how stage 4 is treated and the factors that shape an individual outlook. Wherever you start, the goal is the same: an accurate picture, not false comfort and not a single frightening number without context.
ℹ️ Medical Disclaimer: This article is general health education and is not a substitute for professional medical diagnosis, treatment, or advice about any medication, procedure, or insurance decision. Survival statistics describe large groups of people, not you, and cannot predict your outcome. Decisions about staging, treatment, and prognosis should be made with a board-certified medical oncologist or urologist who knows your full medical picture.
What stage 4 prostate cancer means
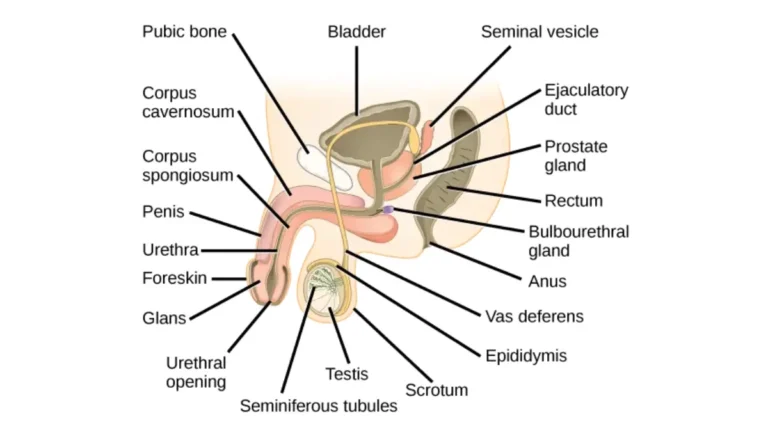
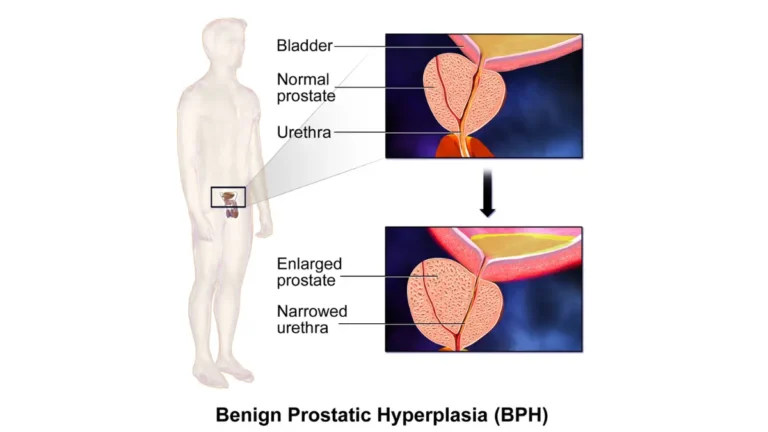
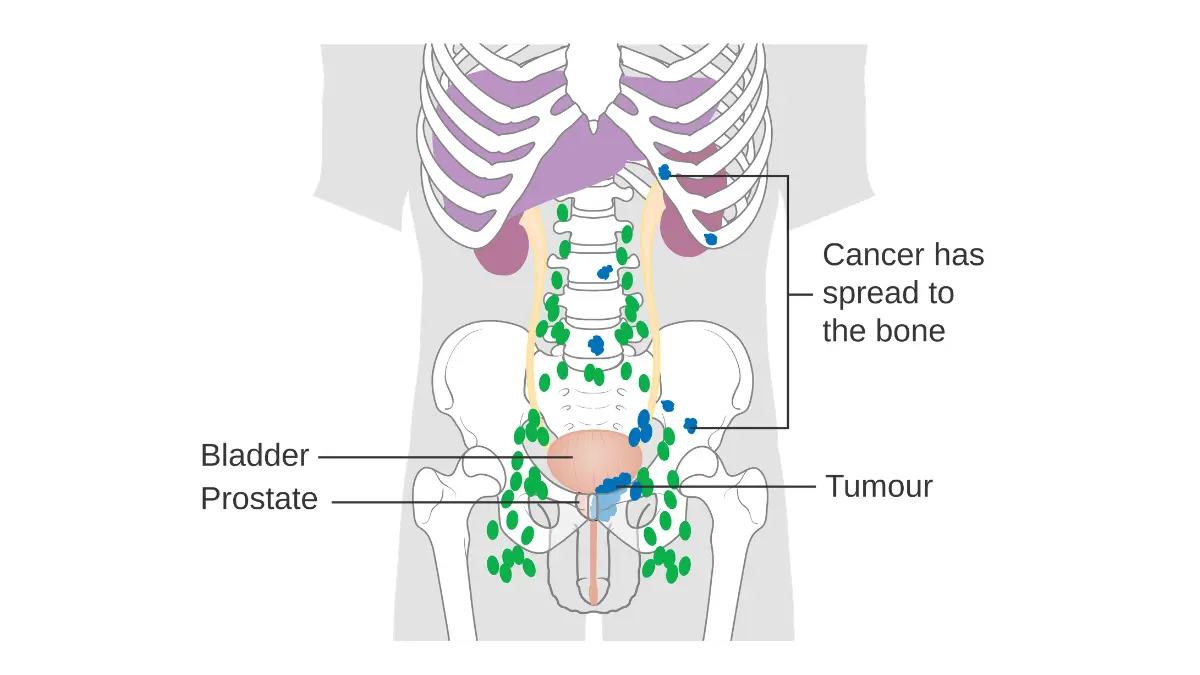
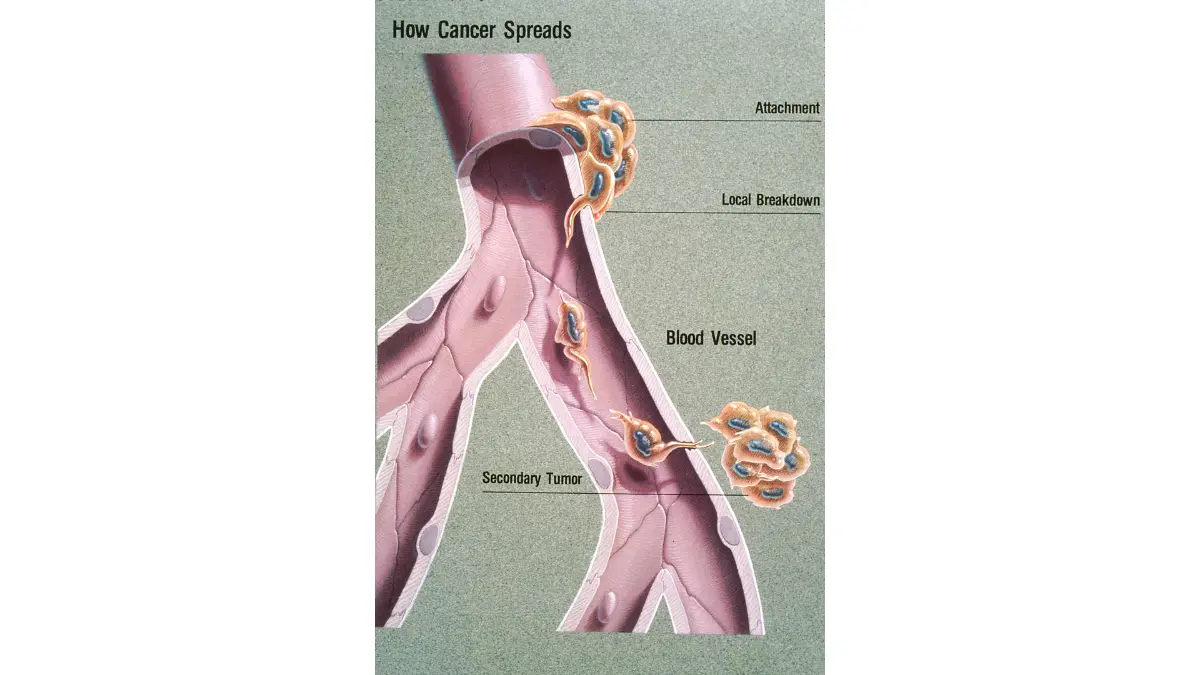
Stage 4 prostate cancer is the most advanced stage, meaning the cancer has spread beyond the prostate gland to other parts of the body. Doctors assign it using the American Joint Committee on Cancer’s TNM system, which describes the tumor (T), nearby lymph nodes (N), and distant spread, or metastasis (M). About 8% of prostate cancers in the United States are already distant — spread to far-off lymph nodes, bones, or organs — at the time of diagnosis, according to the National Cancer Institute.
Stage 4A vs stage 4B
Stage 4 is divided into two groups. Stage 4A means the cancer has reached distant lymph nodes but not other organs or bone. Stage 4B means it has spread to bones or other distant sites, which is what most people mean by metastatic prostate cancer. A small subset, called oligometastatic disease, involves only a few metastatic spots and may be treated more aggressively.
Is stage 4 the same as metastatic?
In everyday use, yes — stage 4B and metastatic prostate cancer describe the same situation. One source of confusion is that the SEER cancer database does not use stage numbers at all; it groups prostate cancer as localized, regional, or distant. “Distant” is the database’s word for what your doctor calls stage 4B or metastatic, and that mismatch is exactly why survival numbers differ between websites. You can see the full staging picture in our guide to prostate cancer signs and stages.
Is stage 4 prostate cancer curable?
Once prostate cancer has spread beyond the pelvis, it is generally considered treatable but not curable, according to the NCI. That distinction matters: not curable does not mean untreatable or immediately life-ending. Modern therapy can often control metastatic prostate cancer for years while preserving quality of life.
Symptoms and how stage 4 is diagnosed
The symptoms of advanced prostate cancer come both from the prostate itself and from wherever the cancer has spread. Because prostate cancer most often spreads to bone, new or worsening bone pain — frequently in the back, hips, or ribs — is one of the most common signs of metastatic disease. Recognizing what to report to your care team is the most useful thing this section can give you.
Common symptoms of advanced prostate cancer
- Bone pain, especially in the back, hips, pelvis, or ribs
- Trouble urinating, a weak stream, or needing to urinate often, particularly at night
- Blood in the urine or semen
- Unintended weight loss and persistent fatigue
- Swelling in the legs or feet, or numbness and weakness if the spine is involved
These symptoms can all have causes other than cancer, which is why a doctor’s evaluation is essential. If you are tracking new or changing symptoms before an appointment, our symptom checker can help you organize what to describe. For more detail on earlier signals, see our overview of early warning signs of prostate cancer and the full list of prostate cancer symptoms.
⚠️ Clinical Warning: New severe back pain combined with leg weakness, numbness, or loss of bladder or bowel control can signal spinal cord compression from bone metastasis — a medical emergency in advanced prostate cancer. Do not wait for a scheduled appointment. Seek emergency care immediately, because rapid treatment can prevent permanent nerve damage.
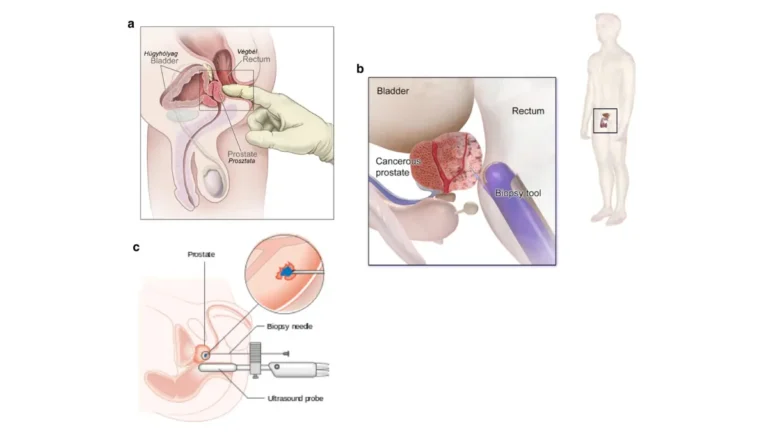
Tests used to confirm metastasis
Diagnosis and staging of advanced disease usually combine a PSA blood test, imaging, and a biopsy. Imaging may include a bone scan, CT, or MRI, and increasingly a PSMA-PET scan, which is especially sensitive for finding prostate cancer that has spread. A biopsy confirms the cancer and its grade, which together with imaging tells the care team how advanced the disease is.
Life expectancy and survival rates for stage 4 prostate cancer
The 5-year relative survival rate for distant-stage prostate cancer is 38%, according to the American Cancer Society’s 2025 report — but this is a population average and does not predict any individual’s outcome. By comparison, survival for prostate cancer caught before it spreads approaches 100%. The number below is a starting point for understanding the disease, not a forecast for one person.
📊 Clinical Data Point: 5-year relative survival for distant-stage (metastatic) prostate cancer is 38% (diagnoses 2015–2021). — Source: American Cancer Society, Prostate Cancer Statistics, 2025.
5-year relative survival for distant-stage disease
Relative survival compares people with this diagnosis to the general population over five years. The 38% figure reflects men diagnosed between 2015 and 2021, the most recent group ACS has analyzed. It is an average across people whose situations vary enormously, so an individual’s outlook can fall well above or below it.
Why survival estimates vary between sources
If you have seen 28% or 32% on other reputable websites, those figures come from earlier ACS data editions, before more recent therapies were reflected. The distant-stage figure has improved over time, which is one reason ACS now reports 38%. Different pages also sometimes mix five-year survival with other measures, so always check the data year and what is being measured. You can read the underlying statistics on the ACS prostate cancer survival rates page and the methodology in the ACS 2025 prostate cancer report.
What statistics can and can’t tell you
A survival statistic is a description of the past for a large group, not a prediction for your future. Your age and overall health, your PSA level, your cancer’s grade, how much it has spread, and how well it responds to treatment all shift the picture in ways a population average cannot capture.
✅ Patient Action: Ask your medical oncologist: “Given my PSA, my Gleason score, and where the cancer has spread, what does a realistic outlook look like for me specifically — and which treatments are most likely to extend it?”
How stage 4 prostate cancer is treated
Treatment for stage 4 prostate cancer is systemic, meaning it works throughout the body rather than targeting one spot. The categories below are general education; your oncologist decides which apply to you and in what order, based on your disease and overall health. The NCI’s prostate cancer treatment overview describes these options in patient-friendly detail.
Hormone therapy (ADT) and what it does
Androgen deprivation therapy (ADT), or hormone therapy, is the foundation of treatment for metastatic prostate cancer. It is frequently combined early with a newer hormonal medicine called an androgen receptor pathway inhibitor (such as abiraterone, enzalutamide, apalutamide, or darolutamide), and sometimes with chemotherapy, to improve survival.
🔬 How It Works: Most prostate cancer cells grow in response to male hormones called androgens, mainly testosterone. ADT lowers testosterone or blocks its signal, which slows or shrinks the cancer. Newer hormonal agents block the androgen pathway more completely, which is why combining them with ADT often works better than ADT alone.
When hormone therapy stops working
Over time, many metastatic prostate cancers stop responding to hormone therapy and become castration-resistant (mCRPC). This is expected, not a personal failure, and it is the point at which other treatments move to the front of the plan. Genetic testing of the tumor can matter here, because certain inherited or tumor mutations open the door to targeted drugs; our genetic risk assessment tool explains what genetic testing involves.
Chemotherapy, targeted radiation, and other options
Beyond hormone therapy, several categories of treatment are used for advanced disease:
- Chemotherapy (such as docetaxel or, later, cabazitaxel) to slow cancer growth; our guide to chemotherapy side effects covers what to expect.
- Radioligand therapy, a targeted form of radiation for PSMA-positive disease.
- Radium-223 for cancer that has spread to bone and is causing symptoms.
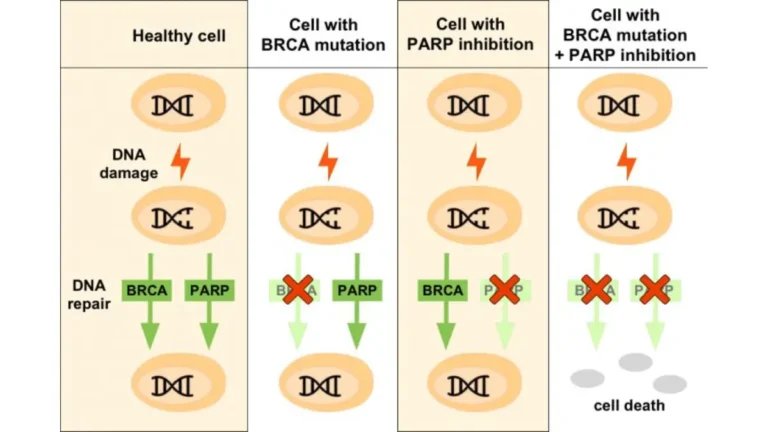
- PARP inhibitors for cancers with specific DNA-repair mutations.
- Palliative radiation to relieve bone pain; see our overview of radiation therapy.
- Clinical trials, which may offer access to newer approaches.
Immunotherapy plays a limited role in prostate cancer compared with some other cancers, though it is used in select cases; our explainer on how immunotherapy works covers the basics.
📊 Clinical Data Point: In March 2025, the FDA expanded approval of the radioligand therapy lutetium Lu-177 vipivotide tetraxetan (Pluvicto) to PSMA-positive mCRPC patients after hormonal therapy but before chemotherapy. — Source: U.S. FDA / Memorial Sloan Kettering Cancer Center.
🔬 How It Works: Radioligand therapy uses a molecule that seeks out PSMA, a protein found on most prostate cancer cells, and delivers radiation directly to those cells from the inside. Because it homes in on the cancer, it can reach metastases throughout the body while limiting damage to healthy tissue. Eligibility depends on a PSMA-PET scan and prior treatments, which your oncologist evaluates.
Factors that affect your individual outlook
The 38% five-year figure is an average across a very mixed group, and several factors move an individual above or below it. Understanding which ones apply to you turns a frightening statistic into a set of specific questions you can bring to your care team.
What makes some outlooks better than others
Generally, a better outlook is associated with younger age and good overall health, a lower PSA, a lower Gleason grade group, fewer sites of spread, and a strong, durable response to hormone therapy. A heavier burden of disease, spread to organs rather than bone alone, and early resistance to hormone therapy tend to point the other way. None of these factors acts alone, and treatment response often reshapes the picture as time goes on.
Questions that determine your prognosis
These are the variables your oncologist weighs, so they are worth asking about directly. Knowing your grade group, the exact sites of metastasis, and your treatment plan’s goals helps you understand your own situation far better than any website average.
🩺 Physician Note: Current oncology practice has shifted toward intensifying treatment earlier — combining hormone therapy with additional agents from the start in many men — rather than using hormone therapy alone. This is one reason survival figures have improved, and it is a reasonable thing to ask whether it applies to your case.
What to do next
A stage 4 diagnosis is serious, and it is also a situation with real, life-extending treatment options and an active field of research behind it. The most useful next step is to make sure you are seeing the right specialist and asking the right questions. A medical oncologist who specializes in prostate cancer, often working alongside a urologist and radiation oncologist, should lead a metastatic care plan.
Bring this short list to your appointment:
- What is my exact stage, Gleason grade group, and where has the cancer spread?
- Has my cancer been tested for PSMA and for DNA-repair mutations that affect treatment?
- Should my treatment combine hormone therapy with another agent from the start?
- What are the goals of treatment for me — control, symptom relief, or both?
- Am I a candidate for any clinical trials?
You do not have to absorb all of this at once, and you do not have to face it alone. Take the questions above, bring someone with you if you can, and let your oncologist build the picture that is specific to you.
Frequently asked questions about stage 4 prostate cancer
1. Is stage 4 prostate cancer a death sentence?
No. Stage 4 prostate cancer is generally treatable but not curable, and the 5-year relative survival rate for distant-stage disease is 38% according to the American Cancer Society. That is an average across a varied group, and modern treatment can control the disease for years in many men. Discuss your specific outlook with a medical oncologist.
2. What is the life expectancy for stage 4 prostate cancer?
There is no single number that fits everyone. The 5-year relative survival rate for distant-stage (metastatic) prostate cancer is 38% (2015–2021 diagnoses, ACS), but individual life expectancy depends on age, overall health, PSA, cancer grade, extent of spread, and treatment response. Your oncologist can give a more personalized estimate.
3. Can stage 4 prostate cancer be cured?
Once prostate cancer has spread beyond the pelvis, it is generally considered incurable but treatable, according to the National Cancer Institute. Treatment focuses on controlling the cancer, extending life, and maintaining quality of life rather than eliminating it entirely. A small group with very limited spread may be treated more aggressively, so ask your oncologist what applies to you.
4. What treatments are used for stage 4 prostate cancer?
Treatment is systemic and usually starts with hormone therapy (ADT), often combined early with a newer hormonal agent and sometimes chemotherapy. Later options include radioligand therapy for PSMA-positive disease, radium-223 for bone spread, PARP inhibitors for certain mutations, and clinical trials. Your medical oncologist determines the right combination and sequence for you.
5. What is the difference between stage 4A and stage 4B?
Stage 4A means prostate cancer has reached distant lymph nodes but not bones or other organs. Stage 4B means it has spread to bone or other distant sites and is what most people mean by metastatic prostate cancer. The distinction affects treatment planning, so confirm your exact stage with your care team.
6. Does hormone therapy stop working over time?
Often, yes. Many metastatic prostate cancers eventually stop responding to hormone therapy and become castration-resistant, which is an expected part of the disease course rather than a personal failure. When this happens, other treatments such as chemotherapy or radioligand therapy move forward. Your oncologist monitors for this with PSA tests and imaging.
7. What are the symptoms of stage 4 prostate cancer?
Common symptoms include bone pain (especially in the back, hips, or ribs), urinary changes, blood in the urine, unintended weight loss, and persistent fatigue. Leg swelling or weakness can occur if the spine is affected. These can have other causes, so report new or worsening symptoms to your care team rather than self-diagnosing.
8. How fast does stage 4 prostate cancer progress?
The pace varies widely and depends on the cancer’s grade, how much it has spread, and how it responds to treatment. Some metastatic prostate cancers grow slowly over years, while higher-grade or castration-resistant disease can progress faster. Your oncologist tracks progression with PSA levels and imaging and adjusts treatment accordingly.
9. What questions should I ask my oncologist?
Ask about your exact stage and Gleason grade group, where the cancer has spread, whether your tumor has been tested for PSMA and DNA-repair mutations, whether your treatment should combine hormone therapy with another agent from the start, the goals of your treatment, and whether you qualify for clinical trials. Bring the list to your appointment.
10. Why do different sources give different survival rates for prostate cancer?
Mainly because they use data from different years and sometimes measure survival differently. Older editions cited around 28–32% for distant-stage disease; the current American Cancer Society figure is 38% (2015–2021 diagnoses), reflecting newer treatments. Always check the data year and confirm with your care team, since population figures do not predict individual outcomes.
11. Where does stage 4 prostate cancer usually spread?
Prostate cancer most often spreads to bone, particularly the spine, hips, pelvis, and ribs, and to distant lymph nodes. Less commonly it reaches organs such as the liver or lungs. The location and extent of spread influence both symptoms and treatment, so your care team will map this with imaging such as a bone scan or PSMA-PET.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.