On This Page – Quick Medical Summary
You just got a breast cancer diagnosis — here’s where to start
The breast cancer questions to ask your oncologist at your first appointment directly shape the treatment plan you leave with. Knowing what to ask — and when — is the difference between an informed patient and one who nods through a 20-minute consultation without understanding what was decided.
Preparing for a first oncology appointment? Start with Phase 1 (your pathology report) and Phase 2 (surgery and treatment sequencing). Treatment has already begun? Phase 3 covers chemotherapy, targeted therapy, and hormonal treatment. Researching for a family member? Phase 4 addresses second opinions and how to advocate for multidisciplinary care team review.
Before these questions make full sense, understanding what your stage determines is essential — our complete guide to breast cancer stages and what they mean for treatment walks through every classification your oncologist will reference. If symptoms prompted this investigation and a diagnosis is not yet confirmed, our Symptom Checker can help you organize them before the appointment.
ℹ️ Medical Disclaimer: The diagnostic criteria, treatment protocols, surgical procedures, medication options, and insurance-related information discussed in this article reflect current clinical guidelines and are provided for educational purposes only. Individual diagnostic conclusions, treatment decisions, and medication choices depend on your specific pathology findings, tumor biology, staging, comorbidities, and the assessment of the specialist who has reviewed your complete medical record. Consult a board-certified medical oncologist, surgical oncologist, or gynecologic oncologist before acting on any clinical information in this article.
The 25 questions — organized by your clinical decision moment
Organize your appointment around five clinical decision phases. These are the breast cancer questions to ask your oncologist, grouped by the decision each answer determines — not by topic. Phase 1 answers must be resolved before any other phase has clinical meaning.
Phase 1: Understanding your pathology report (Questions 1–5)
- What is my tumor’s ER, PR, and HER2 receptor status? (determines which therapies are biologically active against your specific tumor)
- What is my Nottingham tumor grade (I, II, or III)? (Grade III typically bypasses genomic testing and moves directly toward a chemotherapy discussion)
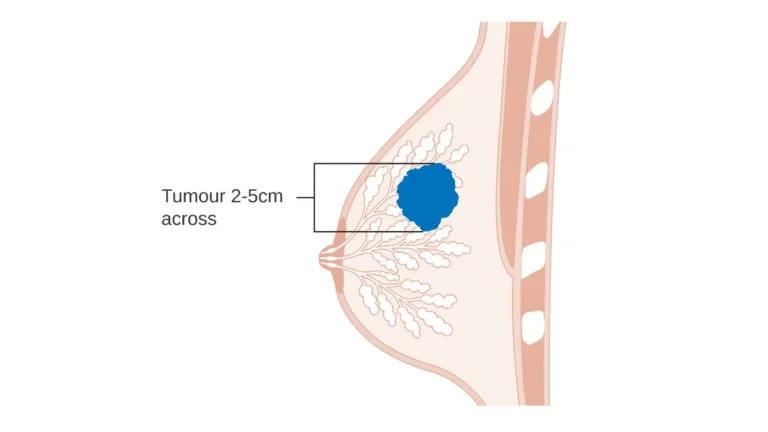
- Has my staging been confirmed by PET-CT or CT imaging? (imaging can upstage a diagnosis and alter the entire treatment sequence)
- Do I need genomic testing — Oncotype DX or MammaPrint? (a low recurrence score for eligible patients can safely eliminate chemotherapy)
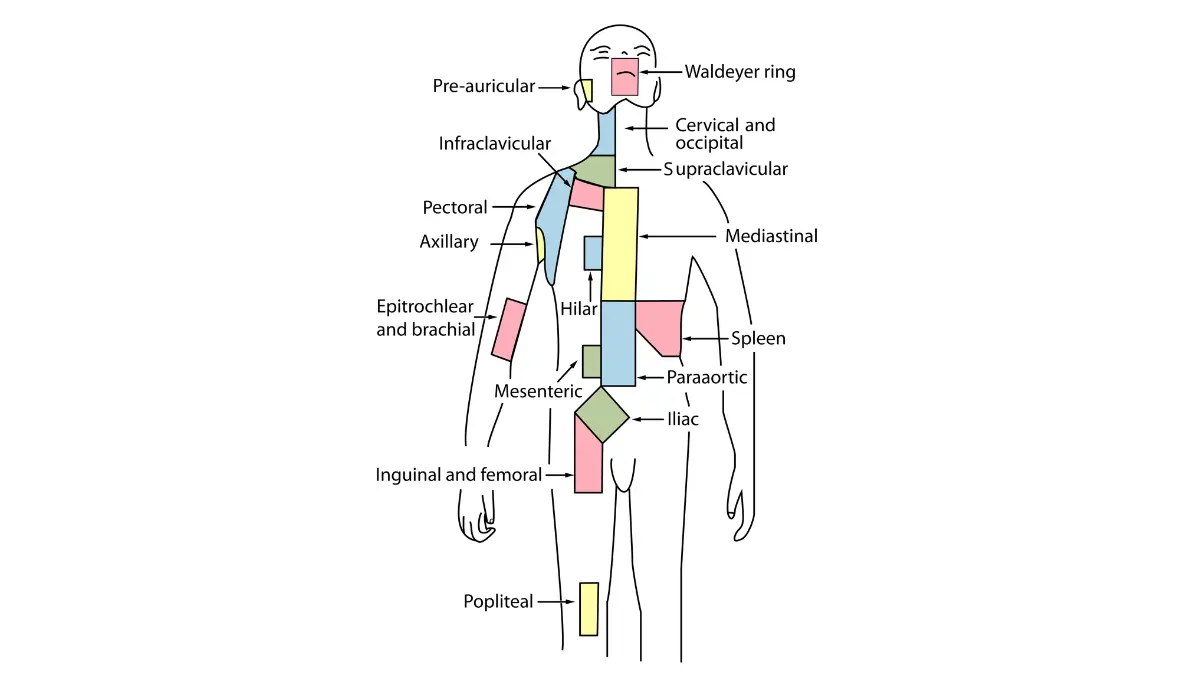
- Were my lymph nodes biopsied, and what did the results show? (nodal status is a primary staging factor that affects surgery type and adjuvant therapy decisions)
Phase 2: Surgery and treatment sequencing (Questions 6–10)
- Am I a candidate for lumpectomy, or do you recommend mastectomy?
- Should I receive chemotherapy before or after surgery?
- Will I need a sentinel lymph node biopsy or full axillary lymph node dissection?
- Should I consult a plastic surgeon before deciding on mastectomy?
- What is my risk of local recurrence with each surgical option?
Phase 3: Systemic therapy (Questions 11–15)
- Which chemotherapy regimen is recommended for my subtype, and why?
- Am I eligible for targeted therapy — trastuzumab, pertuzumab, or both?
- Will I need hormone therapy, and for how long?
- Which side effects are most likely to affect my daily life, and which require an emergency call?
- Will treatment affect my fertility, and should I see a specialist before we begin?
Phase 4: Clinical trials, second opinions, and your care team (Questions 16–20)
- Are there any open clinical trials I qualify for based on my subtype and stage?
- Will you support me in getting a second opinion at an NCI-designated cancer center?
- How many breast cancer cases does your team treat each year?
- Is a multidisciplinary tumor board reviewing my case before we finalize the plan?
- Do I need BRCA1/BRCA2 genetic counseling, and does your center offer it?
Phase 5: Practical logistics and long-term monitoring (Questions 21–25)
- What is the realistic timeline from today to the start of treatment?
- How will treatment affect my ability to work and manage daily responsibilities?
- What support services — nutrition counseling, social work, mental health — are available here?
- How will we know if treatment is working, and when will you reassess the plan?
- What signs of recurrence should I watch for, and how often will I be monitored after treatment ends?
For additional patient resources to review before your appointment, the American Cancer Society’s breast cancer patient appointment guide provides a complementary framework. For clinical context on what symptoms may have preceded your diagnosis, our article on the earliest warning signs of breast cancer and what they indicate clinically is worth reading before you walk in.
Phase 1: reading your pathology report before the appointment
Your pathology report contains three receptor results — ER, PR, and HER2 — that determine which therapies are biologically active against your specific tumor. These numbers define every treatment conversation that follows. Getting them clearly explained at your first appointment is not a courtesy — it is the clinical foundation for everything else.
ER, PR, and HER2: the numbers that open or close treatment options
Estrogen receptor (ER) and progesterone receptor (PR) positivity means endocrine agents — tamoxifen or aromatase inhibitors — are effective first-line therapy. HER2-positive status means targeted therapies trastuzumab and pertuzumab are available. Your Nottingham grade (I through III) determines whether a genomic assay is clinically appropriate or whether a chemotherapy conversation takes precedence.
📊 Clinical Data Point: Approximately 70–80% of breast cancers are hormone receptor-positive (ER-positive, PR-positive, or both), making endocrine therapy the cornerstone of adjuvant treatment for the majority of newly diagnosed patients. — Source: National Cancer Institute, 2026
If a family history of breast or ovarian cancer is part of your picture, our guide to BRCA1 and BRCA2 gene test results and what a positive finding means for surgery is worth reviewing before your surgical consultation. Our Genetic Risk Assessment Tool can help you organize hereditary risk factors before the appointment. The NCI’s breast cancer treatment overview provides the full 2026 clinical evidence base your oncologist is drawing from.
Oncotype DX: the question that may remove chemotherapy from your plan
Oncotype DX is a 21-gene assay that produces a recurrence score from 0 to 100 for ER-positive, HER2-negative, node-negative or limited-node-positive tumors. Per NCCN 2026, a score below 18 indicates low recurrence risk — for most eligible patients, chemotherapy can be safely omitted. A score above 30 indicates high risk and a clear chemotherapy benefit. Nottingham Grade III typically bypasses the assay entirely.
✅ Patient Action: Before accepting or declining chemotherapy for an ER-positive tumor, ask your medical oncologist: “Does my tumor qualify for Oncotype DX testing, and does my Nottingham grade make genomic testing appropriate for my case?” Consult a board-certified medical oncologist before signing any systemic treatment consent.
Phase 2: surgery and treatment sequencing — the decision most patients make too fast
For HER2-positive and triple-negative breast cancer at Stage II–III, chemotherapy before surgery — neoadjuvant therapy — is the preferred sequence per NCCN 2026 guidelines. For ER-positive, HER2-negative Stage I–II disease, surgery typically comes first. The sequence depends entirely on subtype and stage, not on which option the patient prefers or which is offered first.
Lumpectomy vs. mastectomy: what the clinical evidence shows
For Stage I–II tumors meeting size and margin criteria, long-term survival between lumpectomy plus radiation and mastectomy is comparable per 2026 clinical evidence. The question is not which is “safer” — it is which is appropriate given your tumor size, location, BRCA status, and personal preference. If mastectomy is recommended, our guide to breast reconstruction options after mastectomy should be reviewed before your surgical consultation — reconstruction planning often requires a plastic surgery consultation before the primary operation, not after.
Neoadjuvant therapy, pathologic complete response, and the tumor board question
For HER2-positive Stage II–III disease, the NCCN 2026 preferred neoadjuvant regimen is TCHP — docetaxel, carboplatin, trastuzumab, and pertuzumab — given before surgery. For triple-negative Stage II–III, an AC-T or carboplatin-containing regimen is standard. Achieving a pathologic complete response (pCR) — no residual invasive cancer at surgery — is the primary treatment efficacy marker for neoadjuvant cases. Residual disease triggers consideration of adjuvant therapy escalation.
✅ Patient Action: Ask your medical oncologist and surgical oncologist together: “Based on my subtype and stage, should chemotherapy come before or after surgery — and is my case being reviewed by a multidisciplinary tumor board?” Per ASCO 2026 patient guidelines, complex cases should be reviewed by a team that includes a medical oncologist, surgical oncologist, radiation oncologist, and pathologist before treatment begins. Consult both specialists together — not separately — before finalizing the treatment sequence.
Phase 3: chemotherapy, targeted therapy, and hormonal treatment
Two patients with Stage II breast cancer can receive entirely different systemic therapy plans. Tumor subtype — not stage — determines the regimen. Understanding which agents apply to your case before you consent is the clinical purpose of Phase 3 questions.
Chemotherapy and targeted therapy: what changes by subtype
For HER2-positive disease, targeted therapies trastuzumab and pertuzumab are added to chemotherapy — they are not a substitute for it. Trastuzumab continues for 12 months after surgery regardless of when it was started. For triple-negative Stage II–III, the AC-T regimen (doxorubicin, cyclophosphamide, then paclitaxel) or a carboplatin-containing protocol is standard per NCCN 2026. For ER-positive, HER2-negative Stage I–II with a low Oncotype DX score, systemic therapy may be endocrine therapy only.
Hormonal therapy, CDK4/6 inhibitors, and the fertility question
Long-term endocrine therapy — tamoxifen for premenopausal patients, aromatase inhibitors for postmenopausal patients — typically runs 5–10 years for ER-positive disease. Our clinical comparison of tamoxifen vs. aromatase inhibitors — differences, side effects, and switching criteria explains which agent applies by menopausal status.
⚠️ Clinical Warning: CDK4/6 inhibitors — palbociclib, ribociclib, abemaciclib — are FDA-approved for hormone receptor-positive, HER2-negative metastatic breast cancer and select high-risk early-stage settings per NCCN 2026 (abemaciclib for qualifying adjuvant cases). They are not standard therapy for all ER-positive early-stage tumors. Ask your oncologist specifically whether your stage and recurrence risk profile qualify before expecting this drug class to be part of your plan.
Per ASCO 2026 guidelines, fertility preservation should be discussed with all patients of reproductive age before any cytotoxic or hormonal therapy begins. Our complete guide to fertility preservation options before breast cancer treatment covers embryo freezing, oocyte cryopreservation, and ovarian suppression with GnRH agonists — including the critical timing window before chemotherapy must start.
✅ Patient Action: Before signing chemotherapy consent, ask your medical oncologist: “Which agents are in my specific regimen, what is the dosing schedule, and which side effects — cardiotoxicity, peripheral neuropathy, premature menopause — apply to my drugs specifically?” Consult a board-certified medical oncologist for a toxicity profile matched to your regimen and medical history.
Phase 4: clinical trials, second opinions, and knowing if treatment is working
Yes — and a well-trained oncologist will support this without hesitation. NCCN 2026 guidelines explicitly endorse second opinion consultations at NCI-designated cancer centers before any treatment is finalized, particularly for Stage II–IV disease, rare subtypes such as inflammatory breast cancer, and any case where multidisciplinary tumor board review has not been offered.
How to ask about clinical trials and second opinions
Use this direct language for clinical trials: “Are there any open trials I qualify for based on my subtype, stage, and receptor status — can we search ClinicalTrials.gov together?” Our guide to what breast cancer clinical trials involve and how patients qualify explains Phase I, II, and III trial structure and what eligibility criteria typically look like by subtype. You can also search the federal registry for active breast cancer trials by subtype and stage before your appointment to bring specific trial IDs into the conversation.
For a second opinion, the language that works: “I’d like a second opinion at an NCI-designated cancer center before we finalize the plan — can you help transfer my records?” How an oncologist responds to this request tells you a great deal about the quality of care you are receiving.
How will you know if treatment is working?
For neoadjuvant cases, pathologic complete response at surgery is the primary efficacy marker. For hormone therapy, imaging and tumor marker trends are assessed over time. Ask for a written monitoring and reassessment schedule at the start of treatment.
✅ Patient Action: Ask directly: “Is a multidisciplinary tumor board reviewing my case?” Per NCCN 2026, your case should be reviewed by a team that includes a medical oncologist, surgical oncologist, radiation oncologist, and pathologist. If tumor board review is not offered, ask for a referral to a center where it is standard. Consult a board-certified medical oncologist to confirm that this review has occurred before you consent to any treatment sequence.
A gynecologic oncologist’s note: the three questions that matter most
Twenty-five questions is too many for a 20-minute appointment. After years of clinical consultations, I prioritize three.
“What is my tumor’s biology — and what does that mean specifically for my options?”
This question does more work than any other. It requires the oncologist to explain receptor status, grade, and subtype in a single answer. Every decision that follows — surgery, chemotherapy, targeted therapy, hormonal therapy — depends on what they say.
“Who else is reviewing my case before we make a decision?”
A confident oncologist will name the multidisciplinary team. The absence of a clear answer is itself clinically meaningful information.
“What happens if this treatment doesn’t work?”
This is the question most patients are afraid to ask. It is not pessimism — it is informed consent. A prepared oncologist has a Plan B. An answer of “let’s not think about that yet” is a signal, not a reassurance.
🩺 Physician Note — Dr. Carolyn D. Fairweather, MD, Gynecologic Oncology: “In my consultations, the patients who ask these three questions in the first ten minutes leave with a fundamentally different understanding of their situation. They are not being difficult. They are doing exactly what I would do if I were sitting in that chair. Every question you ask in that room is an act of advocacy for your own life.”
When active treatment ends, the questions shift — our guide to what life after breast cancer looks like from a survivorship care perspective addresses the clinical landscape beyond the final treatment cycle.
Frequently asked questions about breast cancer questions to ask your oncologist
1. What should I ask my oncologist at my first appointment?
At the first appointment, prioritize your tumor’s receptor status (ER, PR, HER2), Nottingham grade, staging confirmation by imaging, lymph node biopsy results, and genomic testing eligibility. These five answers determine every treatment decision that follows. The breast cancer questions to ask your oncologist in later appointments — about surgery, chemotherapy, and clinical trials — depend on what these foundational results reveal. Consult a board-certified medical oncologist to review your complete pathology report before any treatment is discussed.
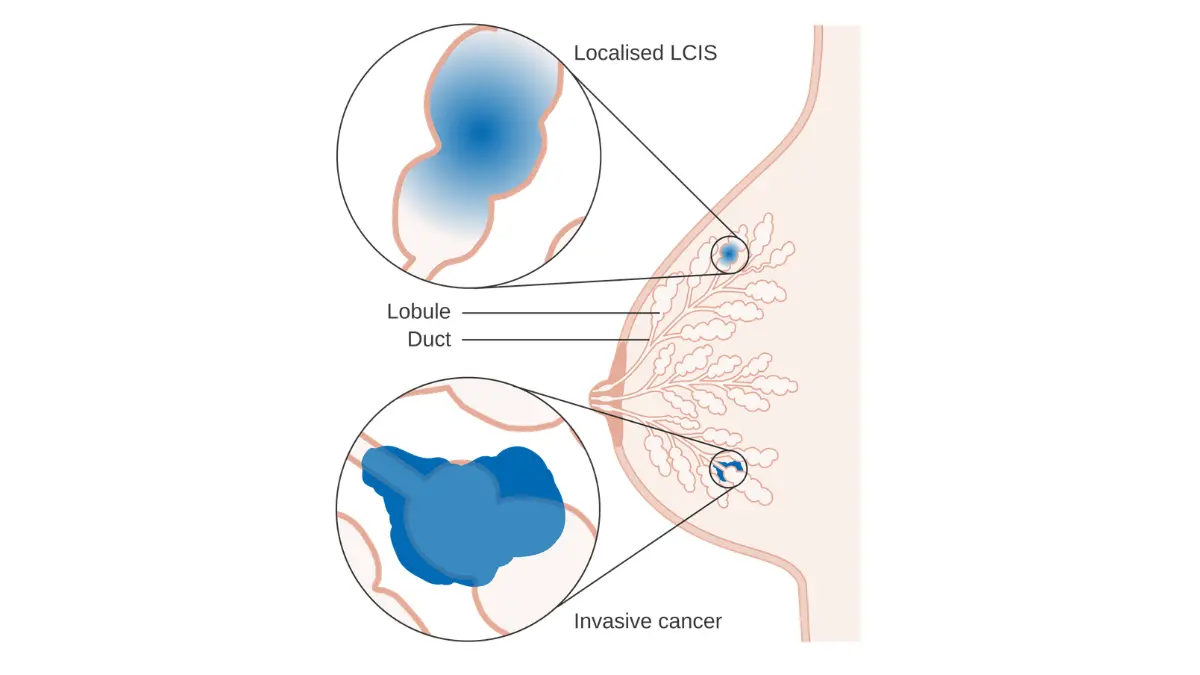
2. How do I understand my breast cancer pathology report?
Your report includes three receptor results — ER, PR, and HER2 — plus a Nottingham grade from I (slow-growing) to III (fast-growing). ER and PR status determines endocrine therapy eligibility; HER2 status determines targeted therapy eligibility. Grade III in an ER-positive tumor typically bypasses genomic testing and advances directly to a chemotherapy discussion. Ask a board-certified medical oncologist to walk through each result with you line by line before any treatment consent is signed.
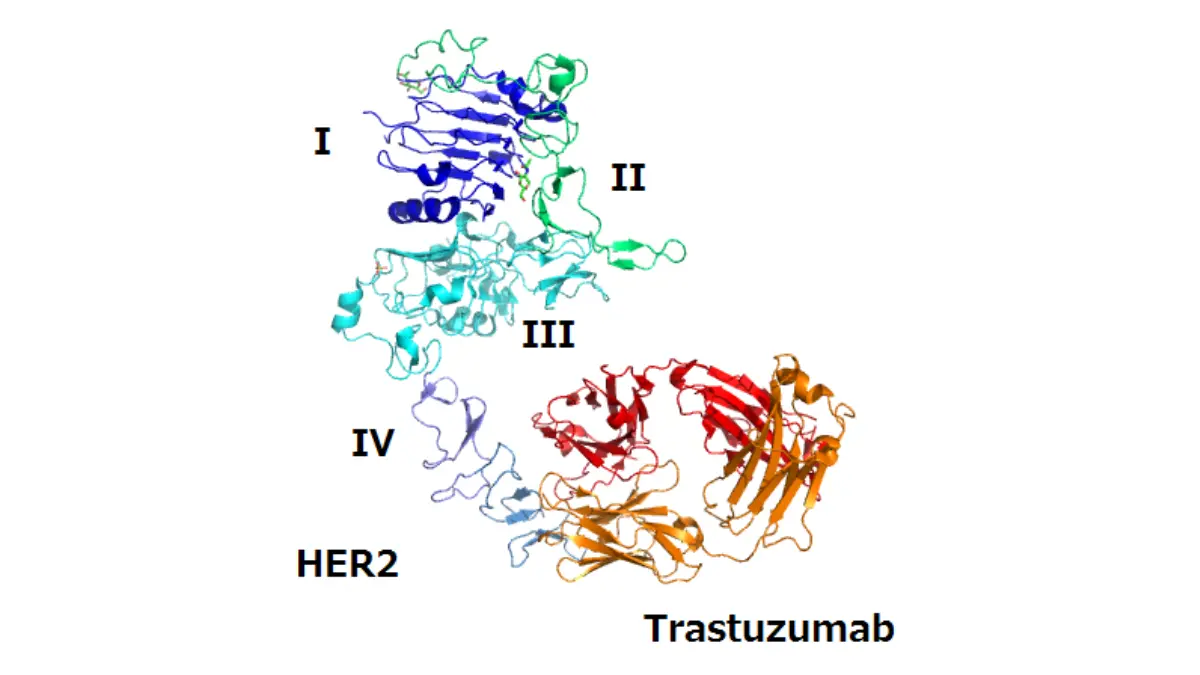
3. What does it mean if my breast cancer is HER2-positive?
HER2-positive breast cancer means the tumor overexpresses the HER2 protein, making it eligible for FDA-approved targeted therapies trastuzumab and pertuzumab. Dual HER2 blockade is the standard for Stage II–III disease per NCCN 2026, typically administered before surgery. Among the breast cancer questions to ask your oncologist, confirm which targeted agents are included in your specific regimen and how long post-surgical trastuzumab continues. Consult a board-certified medical oncologist to verify your HER2 status and treatment eligibility.
4. Should I get a second opinion after a breast cancer diagnosis?
Yes — and a well-trained oncologist will support this without hesitation. NCCN 2026 guidelines endorse second opinions at NCI-designated cancer centers before any treatment begins, particularly for Stage II–IV disease or rare subtypes. A second opinion rarely causes clinically meaningful delays. Among the breast cancer questions to ask your oncologist, how they respond to this request is itself informative about the quality of care you are receiving.
5. What is the difference between a medical oncologist and a surgical oncologist?
A medical oncologist designs and manages systemic treatment — chemotherapy, targeted therapy, and hormone therapy. A surgical oncologist performs tumor removal and lymph node evaluation. For breast cancer, you will typically work with both simultaneously. A radiation oncologist joins the team if radiation is part of your plan. Knowing which specialist to direct each question to helps you use every appointment efficiently — pathology questions go to your medical oncologist; surgical and reconstruction questions go to your surgical oncologist.
6. How do I ask my oncologist about clinical trials?
Use direct language: “Are there any open trials I qualify for based on my subtype, stage, and receptor status?” HER2-positive, triple-negative, and hormone receptor-positive tumors each have distinct trial landscapes — eligibility is not universal. Searching ClinicalTrials.gov before your appointment lets you bring specific trial IDs to the conversation. This is one of the breast cancer questions to ask your oncologist that most newly diagnosed patients never raise — but should. Consult a board-certified medical oncologist to review both institutional and network trial options.
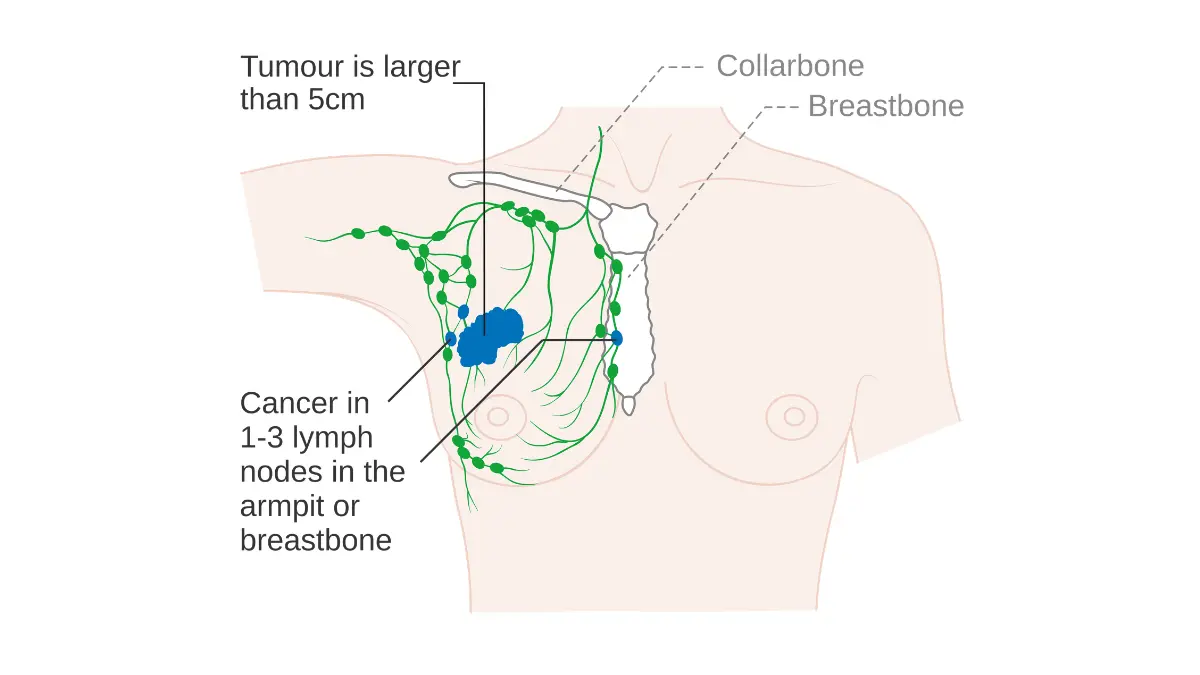
7. What does my breast cancer stage mean for treatment?
Stage describes disease extent but does not determine treatment alone — tumor biology (receptor status, HER2, grade) is equally decisive. Per NCI SEER 2026 data, 5-year survival ranges from above 99% at Stage I to approximately 28% at Stage IV across all subtypes combined. Among the breast cancer questions to ask your oncologist: “How does my tumor’s biology interact with my stage to determine which treatment is recommended for me specifically?” Consult a board-certified medical oncologist to interpret these figures in the context of your individual pathology.
8. Can I ask my oncologist about fertility preservation?
Per ASCO 2026 guidelines, oncologists are recommended to discuss fertility preservation with all patients of reproductive age before initiating any cytotoxic therapy. If your oncologist does not raise the topic, ask directly: “Will treatment affect my fertility, and what preservation options should I pursue first?” Embryo freezing, oocyte cryopreservation, and GnRH agonist ovarian suppression during chemotherapy are the standard options. This is one of the breast cancer questions to ask your oncologist with a hard biological deadline — consult a reproductive endocrinologist before your first infusion.
9. How long does breast cancer treatment typically take?
Timeline depends on subtype and stage. Hormone receptor-positive, HER2-negative early-stage disease: active treatment in 3–6 months, followed by 5–10 years of endocrine therapy. HER2-positive Stage II–III: neoadjuvant chemotherapy plus 12 months of trastuzumab spans 12–18 months total. Triple-negative Stage II–III: active treatment runs approximately 6–9 months. Request a written timeline from your oncologist — this is one of the breast cancer questions to ask your oncologist that prevents avoidable anxiety. Consult a board-certified medical oncologist to map your individual sequence.
10. What is an Oncotype DX test, and should I ask about it?
Oncotype DX is a genomic assay producing a recurrence score from 0–100 for hormone receptor-positive, HER2-negative tumors. Per NCCN 2026, a score below 18 means chemotherapy can typically be safely omitted; a score above 30 indicates a clear chemotherapy benefit. Asking “Does my tumor qualify for Oncotype DX?” is one of the breast cancer questions to ask your oncologist that could remove chemotherapy from your plan entirely if your score is low. Consult a board-certified medical oncologist to confirm whether your tumor profile qualifies.
11. What should I ask about breast cancer chemotherapy side effects?
Ask specifically which agents are in your regimen and what risks each carries. For AC-T regimens, the key risks include anthracycline cardiotoxicity, taxane-related peripheral neuropathy, premature menopause, and neutropenia requiring growth factor support. Ask your oncologist: “Which side effects require an emergency call versus a scheduled check-in?” This is one of the breast cancer questions to ask your oncologist before signing consent — side effects are regimen-specific, not interchangeable across patients. Consult a board-certified medical oncologist for a toxicity profile matched to your specific drugs and health history.
Your appointment is the beginning, not the verdict
Three actions before you walk in: print the Phase 1 and Phase 2 questions, circle those that match your specific pathology findings, and bring a trusted person whose sole job is taking notes. The questions you ask are not an imposition — they are what informed consent requires. For the clinical roadmap beyond active treatment, our guide to what life after breast cancer looks like from a survivorship standpoint addresses what patients and caregivers need to know in the months and years that follow.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.