On This Page – Quick Medical Summary
You have a choice in how your body looks after mastectomy
The moment your surgeon mentions mastectomy, a second conversation often starts — and it moves faster than most patients expect. Reconstruction options come up before you have had time to process the first piece of news.
This guide gives you the clinical framework to navigate that conversation on your own terms.
Breast reconstruction is planned alongside your cancer treatment — not after it. Understanding your breast cancer stage and full treatment sequence is the clinical starting point, because your radiation schedule, surgical approach, and chemotherapy plan all directly shape which reconstruction path is safest and most durable for you.
You have time to understand this decision. You deserve to.
ℹ️ Medical Disclaimer: The surgical options, reconstruction timing considerations, implant safety information, insurance coverage requirements, and complication data discussed in this article reflect current clinical guidelines and published medical evidence, and are provided for educational purposes only. Individual decisions about reconstruction type, timing, implant selection, and insurance eligibility depend on factors including your specific cancer diagnosis, staging, radiation and chemotherapy plan, body composition, comorbidities, and specialist evaluation. Consult a board-certified plastic surgeon with oncologic reconstruction experience — in coordination with your oncology team — before making any surgical or treatment decision discussed in this article. Nothing in this article constitutes a diagnosis, treatment plan, or substitute for individualized medical care.
Implants vs flap reconstruction: how the two procedures compare
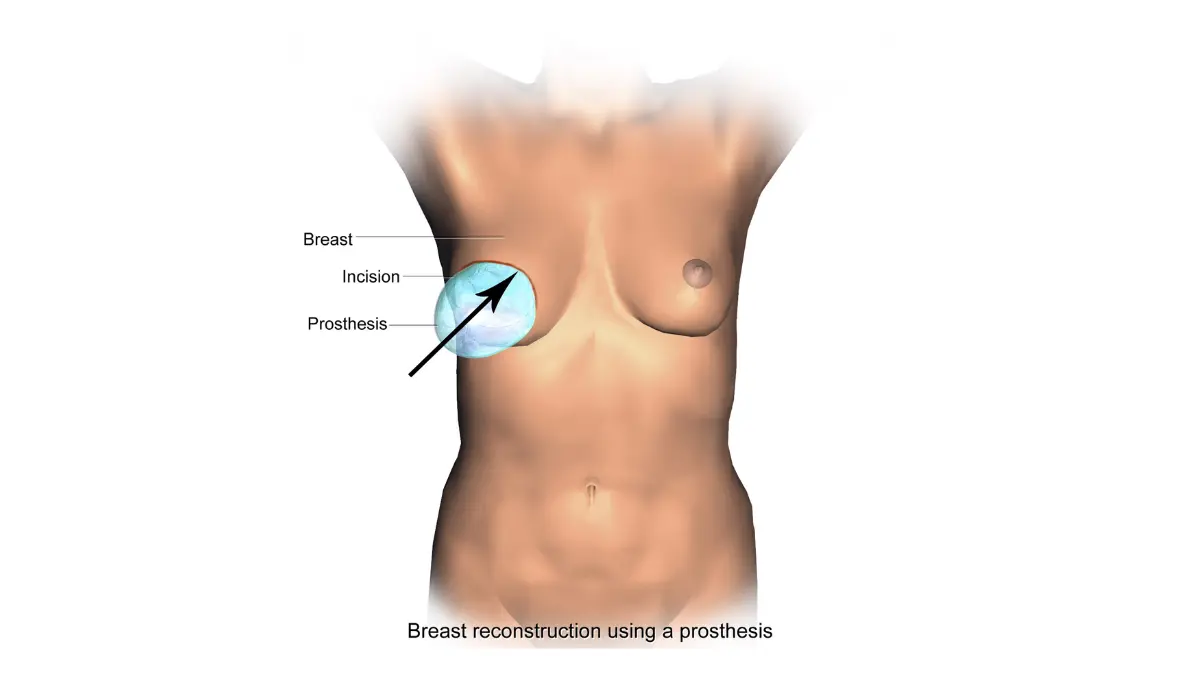
Breast reconstruction after mastectomy falls into two primary surgical categories. Implant-based reconstruction uses silicone or saline implants — typically placed using a tissue expander — to rebuild the breast mound. Autologous flap reconstruction uses the patient’s own living tissue, harvested from the abdomen, back, or thigh, to create the new breast.
Each pathway differs substantially in surgical complexity, recovery length, radiation compatibility, and long-term outcomes. The table below gives you the core clinical comparison to bring to your surgeon consultation.
For a detailed review of how your cancer stage affects treatment sequencing, see our guide to what each breast cancer stage means clinically and how it affects treatment planning.
| Implant-Based Reconstruction | Autologous Flap Reconstruction | |
|---|---|---|
| Surgical Duration | Expander placement: 1–2 hrs; implant exchange: 1–2 hrs | DIEP: 6–8 hrs; TRAM: 4–6 hrs; latissimus dorsi: 2–4 hrs |
| Hospital Stay | 1–2 days | 3–5 days |
| Initial Recovery | 4–6 weeks | 6–8 weeks |
| Full Settling Timeline | 3–6 months (after final implant exchange) | 3–6 months (tissue softening and settling) |
| Radiation Compatibility | Higher complication risk in irradiated tissue | Preferred option in previously irradiated tissue |
| Candidacy Profile | Adequate skin envelope; no planned radiation; BMI typically below 35; non-smoker | Sufficient donor tissue; no prior surgery damaging perforator vessels; non-smoker |
| Best For Patient Profile | No planned radiation; shorter surgery preferred; staged recovery manageable | Planned radiation; natural tissue result preferred; core function a priority |
Data source: Surgical duration and recovery benchmarks consistent with current reconstructive surgical standards
For an authoritative clinical overview of both procedures, the National Cancer Institute’s breast reconstruction information for patients provides NCI-reviewed summaries of implant and flap options.
What implant-based reconstruction involves
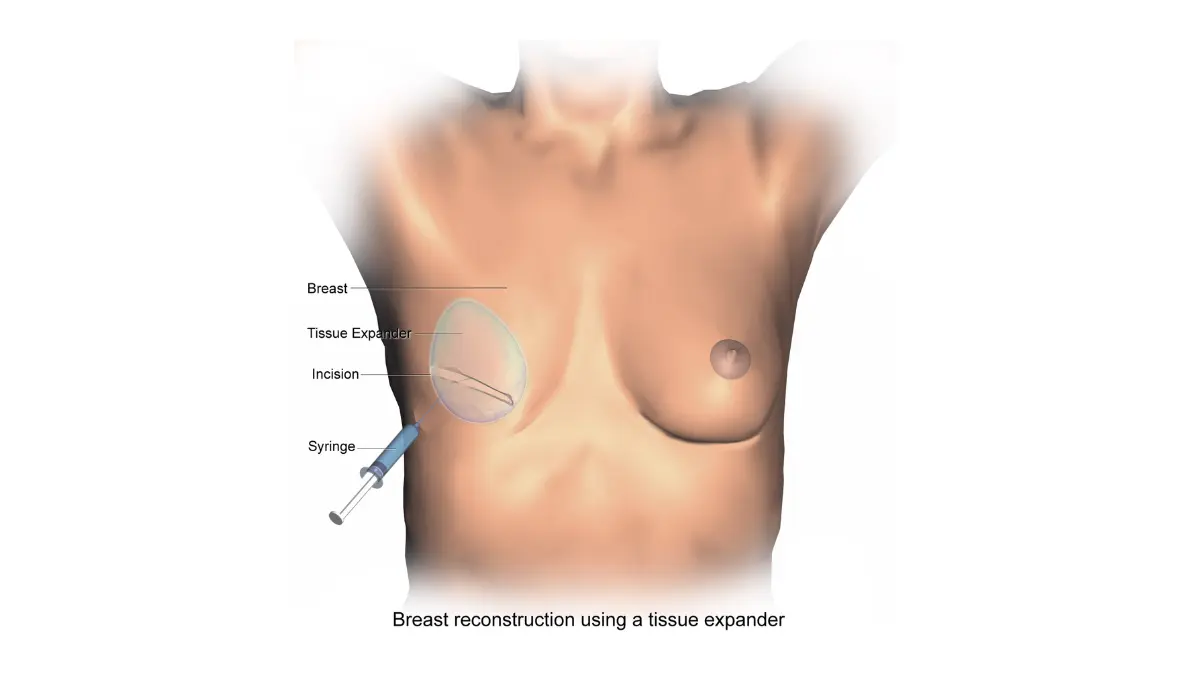
In implant-based reconstruction, a tissue expander is placed beneath the chest wall muscle at the time of mastectomy. Over the following 3–6 months, the surgeon progressively injects saline at clinic visits to gradually stretch the overlying skin and muscle. A second procedure then removes the expander and places the permanent silicone or saline implant.
What autologous flap reconstruction involves
In autologous flap reconstruction, living tissue — skin, fat, and sometimes muscle — is transferred from a donor site on the patient’s body to the chest wall. That tissue is either tunneled while still attached to its original blood supply (pedicled flap), or disconnected and reconnected to chest wall vessels under a surgical microscope (free flap). Because the tissue is alive and growing with the patient’s body, the reconstructed breast often behaves more like natural tissue over time.
Which procedure fits which patient profile
No single procedure is universally superior. The most important clinical variable is your radiation plan. If adjuvant radiation therapy is part of your treatment — even if unconfirmed — that changes the reconstruction equation significantly. Implants placed in tissue that will subsequently be irradiated face substantially elevated rates of capsular contracture and implant failure, making autologous tissue the clinically preferred option in that scenario.
✅ Patient Action: Before your mastectomy date is confirmed, ask your breast surgeon and plastic surgeon in the same conversation: “Is radiation therapy in my current treatment plan — and does that make implant-based reconstruction higher-risk for me?” Answering this question before surgery, not after, is the single most important step in reconstruction planning.
📊 Clinical Data Point: Procedure volume and complication benchmark data — Source: ASPS 2026 Plastic Surgery Statistics Report.
Implant-based breast reconstruction: what the procedure actually involves
Implant-based reconstruction is the most commonly performed breast reconstruction approach in the United States. It is typically completed in two surgical stages over 3–6 months, with the tissue expansion phase creating the pocket for the permanent implant.
Your plastic surgeon will assess several physical and oncological factors before recommending this pathway. Two of the most clinically significant are your body composition and your adjuvant treatment plan.
How tissue expanders work before final implant placement
A tissue expander is a temporary, adjustable silicone device placed beneath the chest wall muscle — or behind a layer of acellular dermal matrix (ADM) — immediately after mastectomy.
🔬 How It Works: Over 3–6 months following mastectomy, saline is progressively injected into the expander at clinic visits — typically every 1–2 weeks. Each injection stretches the overlying skin and chest wall muscle incrementally, creating the pocket needed for the permanent implant. ADM is a specially processed biological material that provides structural support for the expander against the chest wall and helps shape the implant pocket.
Once the target volume is reached and the skin has been adequately stretched, a second procedure removes the expander and places the permanent implant — either silicone gel or saline.
Silicone vs saline implants: what the FDA requires patients to know in 2026
Both silicone gel and saline implants are FDA-approved for breast reconstruction following mastectomy. Before selecting between them, review the FDA breast implant safety updates and 2026 patient decision checklist, which includes current informed consent requirements specific to silicone gel implants.
📊 Clinical Data Point: FDA breast implant safety requirements, 2026 patient decision checklist, and updated labeling for silicone gel and saline implants — Source: U.S. Food and Drug Administration, fda.gov/medical-devices/breast-implants.
Who is the best candidate for implant-based reconstruction
The strongest candidates for implant-based reconstruction share these clinical characteristics:
- Adequate chest skin envelope after mastectomy — skin-sparing or nipple-sparing mastectomy techniques typically preserve the best envelope for implant placement
- No adjuvant radiation therapy planned or anticipated
- BMI typically below 35 — higher BMI increases infection risk and wound healing complications at the mastectomy flap
- Non-smoker status — smoking significantly impairs wound healing and raises infection rates
- No autoimmune conditions associated with elevated implant complication risk
Your BMI is one of the physical factors your plastic surgeon will evaluate during the surgical planning consultation. Use our free BMI Calculator to check your body mass index before your appointment.
⚠️ Clinical Warning: If radiation therapy is added to your treatment plan after implant placement — for example, because final surgical pathology reveals positive margins — the risk of capsular contracture, implant infection, and implant loss increases substantially. This is not a rare clinical scenario. Discuss the possibility of post-mastectomy radiation explicitly with your oncologist before committing to implant-based reconstruction, and ask what would happen to your reconstruction plan if radiation becomes necessary.
✅ Patient Action: Before choosing between silicone and saline implants, ask your plastic surgeon: “Given my body type, BMI, and adjuvant treatment plan, which implant type has the better long-term outcome profile for a patient like me — and what is your personal complication rate for each?”
Flap reconstruction: DIEP, TRAM, and latissimus dorsi options explained
Autologous flap reconstruction uses the patient’s own living tissue to rebuild the breast. Three primary flap options are performed in the United States — each differing in harvest site, surgical technique, recovery timeline, and candidacy criteria.
For a comprehensive guide to the mastectomy techniques that create the surgical foundation for reconstruction, see what your surgeon won’t always tell you before mastectomy.
DIEP flap: abdominal tissue reconstruction without muscle sacrifice
The DIEP flap (deep inferior epigastric perforator) is the most widely performed free flap procedure in breast reconstruction. Skin and fat are harvested from the lower abdomen without sacrificing the underlying rectus abdominis muscle.
🔬 How It Works: The surgeon identifies the perforator blood vessels running through the abdominal tissue, carefully dissects them away from the surrounding rectus abdominis muscle — preserving the muscle intact — and connects them to blood vessels in the chest wall under a surgical microscope. This microsurgical anastomosis reconnects the tissue’s blood supply at its new location on the chest. DIEP flap surgery takes 6–8 hours under general anesthesia and requires 3–5 days in hospital.
Ideal candidates have sufficient lower abdominal tissue, have not had prior abdominal surgeries that may have damaged the perforator vessels (including certain tummy tuck incisions and midline laparoscopic procedures), are non-smokers, and have no significant clotting disorders.
TRAM flap: the older standard and its long-term trade-offs
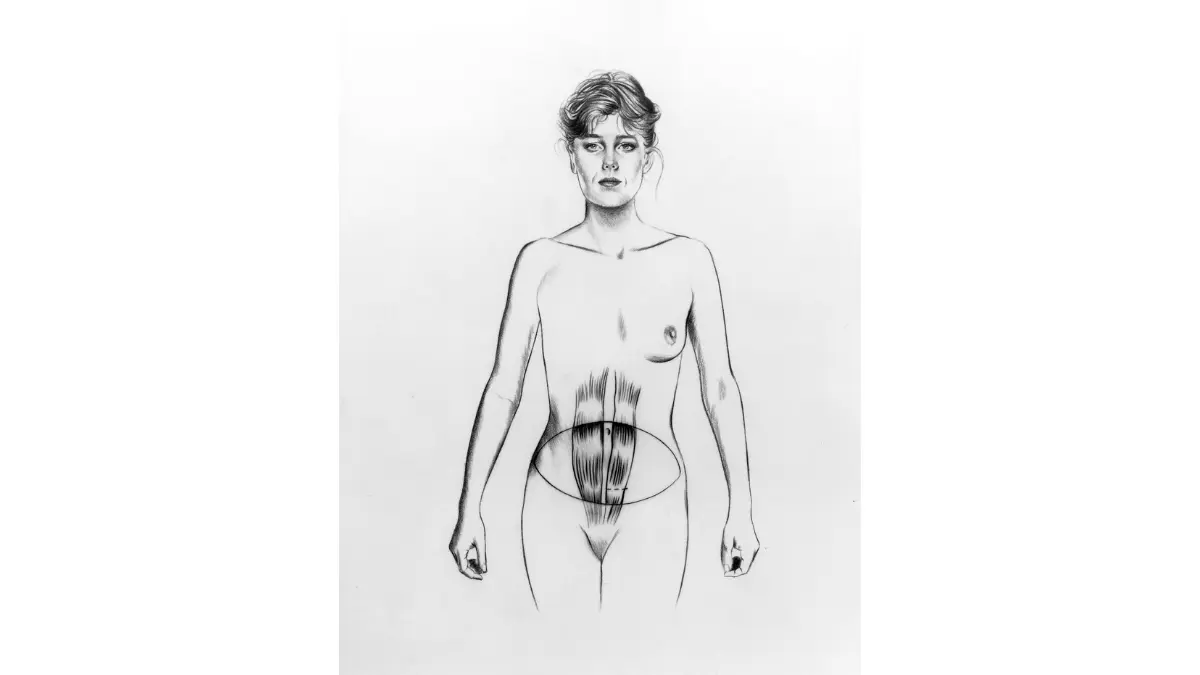
The TRAM flap (transverse rectus abdominis myocutaneous) uses skin, fat, and a portion of the rectus abdominis muscle itself to reconstruct the breast. It can be performed as a pedicled flap — tunneling the tissue to the chest while keeping it attached to its original blood supply — or as a free flap requiring microsurgical vessel connection.
The central clinical trade-off compared to DIEP is abdominal wall function. Harvesting rectus abdominis muscle increases the risk of long-term abdominal weakness, donor site hernia, and reduced core strength — a meaningful consideration for physically active patients.
🩺 Physician Note: In coordinating breast cancer care between oncology and reconstructive surgical teams, I observe that the DIEP-versus-TRAM trade-off matters most to younger, physically active patients — runners, those in manual labor, and patients for whom core function is essential. If long-term abdominal strength is a priority, ask your plastic surgeon specifically about DIEP flap candidacy at your center, and inquire about their annual case volume for microsurgical procedures.
Latissimus dorsi flap: back tissue for smaller or supplemental reconstruction
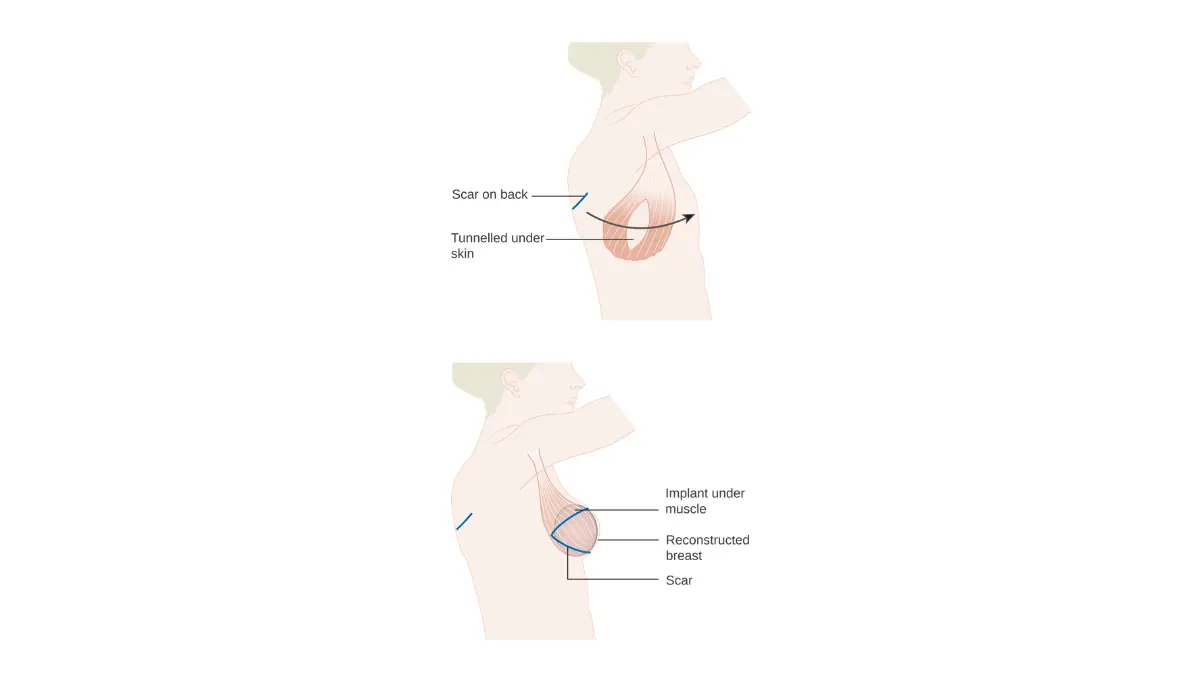
The latissimus dorsi flap uses skin, fat, and the latissimus dorsi back muscle to create the breast mound. It is typically used for smaller breast volumes, or as a supplement to an implant in patients who have received prior chest wall radiation and need well-vascularized tissue to protect the implant from radiation-damaged skin.
✅ Patient Action: Confirm your flap candidacy by asking: “Do I have sufficient abdominal tissue for DIEP flap? Have any of my prior surgeries affected those perforator vessels? Does your center perform at least 50 DIEP procedures annually?” Surgeon volume is a meaningful quality indicator for microsurgical outcomes.
Immediate vs delayed reconstruction: timing your surgery around treatment
Reconstruction timing is one of the hardest decisions in breast cancer care — because it requires making a long-term body image choice in the middle of an acute cancer crisis, often under time pressure. There is no universally correct answer. The right timing is the one that fits your specific oncology treatment plan.
Immediate breast reconstruction is performed in the same surgical session as the mastectomy. Delayed reconstruction begins only after cancer treatment — including radiation therapy and chemotherapy — is complete.
For a detailed review of how mastectomy type affects reconstruction options, see our guide to lumpectomy vs mastectomy: what surgeons recommend by cancer stage and tumor profile. For patients with radiation in their treatment plan, the article on breast cancer radiation therapy and its effects on surrounding tissue explains what adjuvant radiation involves clinically.
When immediate reconstruction is clinically appropriate
Immediate reconstruction is appropriate for most patients whose treatment plan does not include adjuvant radiation therapy. Skin-sparing and nipple-sparing mastectomy techniques preserve the best possible tissue envelope for immediate reconstruction — which is one reason mastectomy technique and reconstruction planning are coordinated together rather than sequenced separately.
Why radiation therapy may require delayed reconstruction
Radiation-induced fibrosis hardens the breast skin envelope and impairs the blood supply to irradiated tissue. Implants placed in tissue that will subsequently be irradiated face substantially elevated rates of capsular contracture — the development of a hardening collagen capsule around the implant requiring surgical revision — as well as infection and implant failure.
📊 Clinical Data Point: Reconstruction timing recommendations in the setting of planned adjuvant radiation — Source: NCCN Clinical Practice Guidelines in Oncology: Breast Cancer [2026].
Delayed reconstruction, or planning autologous flap tissue from the outset, allows radiation effects on the chest wall tissue to stabilize before reconstruction begins. In irradiated tissue, DIEP flap reconstruction is often preferred over implants because living autologous tissue has superior blood supply compared to fibrotic, radiation-damaged skin.
How to prepare for the reconstruction timing conversation with your surgical team
- Confirm whether radiation therapy is in your current treatment plan — and whether that status could change based on final surgical pathology.
- Ask your breast surgeon and plastic surgeon to discuss reconstruction timing in the same consultation before your mastectomy date is set.
- If you carry BRCA1 or BRCA2 variants and are considering prophylactic mastectomy, use our Genetic Risk Assessment Tool to document your hereditary risk profile before your genetic counseling and surgical planning appointments.
✅ Patient Action: Before your mastectomy date is finalized, ask your oncologist and breast surgeon: “Is radiation therapy currently in my treatment plan — and if my final pathology changes that, how would it change our reconstruction approach?” Getting a clear answer before the primary surgery protects you from a rushed decision in the post-operative period.
Risks, complications, and recovery: what clinical data shows by procedure type
Every breast reconstruction procedure carries surgical risk. Understanding those risks honestly — and in procedure-specific terms — is what allows you to arrive at your surgical consultation prepared to ask the right questions.
⚠️ Clinical Warning: Complication rates reported in published medical literature typically reflect high-volume academic medical centers performing 100 or more reconstruction procedures annually. At lower-volume facilities, individual complication profiles may differ significantly. Always ask your plastic surgeon for their personal complication rate data — not only published benchmarks.
Complication rates by procedure type: implant vs flap reconstruction compared
| Complication | Implant-Based | Flap-Based | Clinical Notes |
|---|---|---|---|
| Capsular contracture | Present; substantially elevated in irradiated tissue | Lower overall risk | Baker Grade III–IV typically requires surgical revision |
| Implant rupture | Present (silicone: may be silent) | Not applicable | FDA recommends regular MRI monitoring for silicone gel implants |
| Infection | Moderate risk | Moderate risk | Risk elevated in patients with diabetes, obesity, or immunosuppression |
| Flap necrosis | Not applicable | Partial or total possible | Total flap loss (rare at high-volume centers) requires return to operating room |
| Seroma | Common at mastectomy site | Common at donor site | Managed with drain; typically resolves without surgical intervention |
| Donor site complications | Not applicable | Hernia; abdominal weakness (TRAM > DIEP) | DIEP preferred for abdominal wall preservation in active patients |
Data source: All complication rate figures
Recovery timeline by procedure type: what to expect week by week
Implant-based reconstruction:
- Weeks 1–2: Drain management; restricted arm movement; no lifting above shoulder height
- Weeks 3–4: Drain removal; return to light daily activities; driving with surgeon clearance
- Weeks 4–6: Return to desk work and most sedentary daily activities
- Months 3–6: Second-stage procedure — tissue expander exchange for permanent implant
DIEP or TRAM flap reconstruction:
- Weeks 1–2: Hospital discharge; limited mobility at both chest and donor site; drain management
- Weeks 3–4: Return to light activity; walking actively encouraged to reduce blood clot risk
- Weeks 6–8: Return to most daily activities; surgeon clearance required before driving
- Months 3–6: Tissue softening and final settling; appearance stabilizes progressively
📊 Clinical Data Point: BREAST-Q patient-reported satisfaction outcomes comparing implant-based and flap-based reconstruction
Long-term outcomes and patient satisfaction data
Both implant-based and autologous flap reconstruction achieve high long-term patient satisfaction when matched to the appropriate candidate. The strongest predictor of satisfaction is not which procedure was chosen — it is whether that choice was made with full information about the radiation plan, recovery expectations, and candidacy criteria before surgery.
If you experience unexpected new pain, swelling, skin warmth, or changes at your reconstruction site after discharge, use our Symptom Checker to help assess whether your symptoms need urgent attention from your surgical team.
✅ Patient Action: Before any reconstruction procedure, ask your plastic surgeon: “What is your personal complication rate for this specific procedure — and how does it compare to published benchmarks from high-volume academic centers?” A board-certified reconstructive surgeon performing adequate case volume should be able to answer that question directly.
A physician’s framework for the reconstruction decision: clinical and legal
In my experience coordinating breast cancer care between oncology and reconstructive surgical teams, the most common source of patient regret is not choosing the wrong procedure. It is choosing without knowing whether radiation was part of the treatment plan. That one confirmed fact — before the mastectomy date is set — changes the entire reconstruction equation.
The clinical factors your reconstructive team will weigh
The four most important clinical variables in the reconstruction decision are: (1) your adjuvant radiation plan; (2) your available donor tissue for autologous reconstruction; (3) the microsurgical expertise and case volume of your surgical center; and (4) your own recovery priorities and long-term functional goals. These factors cannot be assessed in a single appointment. They require a coordinated conversation between your breast surgeon, medical oncologist, and plastic surgeon — ideally in a multidisciplinary tumor board setting.
The American Cancer Society’s breast reconstruction patient resource offers practical guidance for finding board-certified reconstructive surgeons and navigating insurance prior authorization.
Your legal right to reconstruction coverage: the Women’s Health and Cancer Rights Act explained
Under the Women’s Health and Cancer Rights Act (WHCRA), all group health plans covering mastectomy are federally required to cover breast reconstruction — including reconstruction of both breasts for symmetry, external prostheses, and treatment of physical complications including lymphedema — without annual or lifetime benefit limits. This is established federal law. It is not a benefit that requires negotiation — it is your right.
Contact your insurer in writing before your surgery date to confirm WHCRA-mandated coverage and request prior authorization. Ask specifically: “Which reconstruction procedures are covered under WHCRA, and what prior authorization steps are required before my procedure date?”
✅ Patient Action: Before scheduling any reconstruction procedure, contact your insurance provider in writing to confirm WHCRA coverage and obtain prior authorization. Then schedule a consultation with a board-certified plastic surgeon who participates in a multidisciplinary tumor board at your cancer center and performs at least 50 reconstruction procedures annually.
Your next step: a specialist consultation built around your full treatment plan
Breast reconstruction is one of the most personal decisions in cancer care. It deserves a conversation as individual as your diagnosis — not a decision made in the window between appointments, without the right clinical framework.
Three concrete steps before your next surgical consultation:
- Request a plastic surgeon referral from your oncologist before your mastectomy date is set. Reconstruction planning is most effective when it happens before the primary surgery — not after.
- Confirm whether radiation therapy is in your treatment plan — and ask explicitly how that changes your implant vs flap decision.
- Contact your insurer in writing before scheduling any procedure to confirm WHCRA-mandated reconstruction coverage and obtain prior authorization.
Return to the complete breast cancer stages and survival guide for the full clinical foundation connecting your cancer diagnosis, treatment sequencing, and reconstruction decision.
You do not have to navigate this alone.
Breast reconstruction surgery: your questions answered
1. What are the different types of breast reconstruction after mastectomy?
Breast reconstruction after mastectomy falls into two primary categories: implant-based reconstruction, using silicone or saline implants with a tissue expander placed first, and autologous flap reconstruction, using the patient’s own tissue from the abdomen, back, or thigh. The right type depends on your cancer treatment plan, available donor tissue, body composition, and whether radiation therapy is part of your care. Consult a board-certified plastic surgeon with oncologic reconstruction experience before choosing.
2. Is implant reconstruction or flap reconstruction better?
Neither breast reconstruction option is universally superior. The right choice depends on three primary clinical factors: whether radiation therapy is planned (which substantially elevates implant complication rates), your available donor tissue for autologous reconstruction, and your recovery tolerance. BREAST-Q patient-reported outcome data consistently shows high long-term satisfaction with both procedures when matched to the appropriate clinical candidate. Consult a board-certified plastic surgeon before making any reconstruction decision.
3. What is a DIEP flap and who is a candidate?
A DIEP flap breast reconstruction uses skin and fat harvested from the lower abdomen — preserving the rectus abdominis muscle entirely — to rebuild the breast mound through microsurgical vessel connection at the chest wall. Ideal candidates have sufficient lower abdominal tissue, no prior abdominal surgeries that damaged the perforator vessels, and are non-smokers. Surgery takes 6–8 hours under general anesthesia with a 3–5-day hospital stay. Consult a board-certified microsurgical plastic surgeon to confirm candidacy.
4. How long does breast reconstruction surgery take?
Breast reconstruction surgery duration varies significantly by procedure. Tissue expander placement at mastectomy: 1–2 hours. Final implant exchange: 1–2 hours. DIEP flap reconstruction: 6–8 hours due to microsurgical vessel connection. TRAM flap: 4–6 hours. Latissimus dorsi flap: 2–4 hours. All procedures require general anesthesia and planned hospital admission. Consult your plastic surgeon and anesthesiologist for a personalized operative timeline that accounts for your specific anatomy and planned technique.
5. Can breast reconstruction be done at the same time as mastectomy?
Yes — immediate breast reconstruction is performed in the same surgical session as the mastectomy, most commonly using tissue expanders or a one-stage implant. Immediate reconstruction is appropriate for most patients not scheduled for adjuvant radiation therapy. Patients requiring radiation therapy may be advised to delay reconstruction to avoid radiation-induced implant complications and elevated capsular contracture risk. Consult your breast surgeon and plastic surgeon together before your mastectomy date is confirmed to determine the safest timing.
6. What are the risks of breast reconstruction surgery?
Breast reconstruction risks differ by procedure. Implant-based: capsular contracture, implant rupture, infection, and asymmetry. Flap-based: partial or total flap necrosis, seroma at the donor site, donor site hernia (particularly with TRAM flap), and prolonged recovery. All reconstruction procedures carry standard surgical risks including blood clots, anesthesia reactions, and wound healing complications. Consult a board-certified plastic surgeon to review your individual risk profile and ask specifically for their personal complication rate data.
7. Does insurance cover breast reconstruction after mastectomy?
Yes — federal law requires it. Under the Women’s Health and Cancer Rights Act, all group health plans covering mastectomy must cover breast reconstruction for both breasts, external prostheses, and treatment of physical complications — without annual or lifetime benefit limits. Coverage must be provided consistently with other surgical and medical benefits under your plan. Contact your insurer in writing before surgery to confirm WHCRA-mandated coverage and obtain prior authorization before scheduling your procedure.
8. How long is recovery from breast reconstruction?
Breast reconstruction recovery varies by procedure. Implant-based: drains removed at 1–2 weeks; return to light activity by weeks 4–6; final implant exchange procedure at 3–6 months. DIEP or TRAM flap: limited mobility in weeks 1–2; most daily activities by weeks 6–8; full tissue settling over 3–6 months. Strenuous exercise and heavy lifting require surgeon clearance before resumption. Consult your plastic surgeon for a personalized recovery timeline based on your specific procedure and overall health status.
9. What is a tissue expander in breast reconstruction?
A tissue expander is a temporary, adjustable silicone device placed beneath the chest wall muscle — or behind acellular dermal matrix — at the time of mastectomy during breast reconstruction. Over 3–6 months, saline is progressively injected at clinic visits to gradually stretch the overlying skin and muscle pocket in preparation for the permanent implant. The expander is then surgically removed and replaced with the permanent silicone or saline implant in a second procedure. Consult your plastic surgeon about your specific expansion schedule and timeline.
10. Can you have breast reconstruction after radiation therapy?
Yes, but radiation therapy significantly affects breast reconstruction options and outcomes. Implant-based reconstruction in previously irradiated tissue carries substantially higher rates of capsular contracture, infection, and implant failure compared to non-irradiated tissue. Autologous flap reconstruction — particularly DIEP flap — is often preferred in irradiated tissue because living tissue provides superior blood supply compared to fibrotic, radiation-damaged skin. Consult a board-certified plastic surgeon experienced specifically in post-radiation breast reconstruction before selecting any surgical approach.
11. When is the best time to decide about breast reconstruction?
The best time to begin planning breast reconstruction is before mastectomy — during the pre-surgical consultation period when the breast surgeon and plastic surgeon can coordinate timing together. Early planning enables immediate reconstruction when appropriate and ensures the mastectomy technique preserves the best possible skin and nipple envelope. Waiting until after surgery is medically safe but limits some procedural options. Consult a board-certified plastic surgeon as early in your breast cancer treatment planning process as your oncology team allows.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.