On This Page – Quick Medical Summary
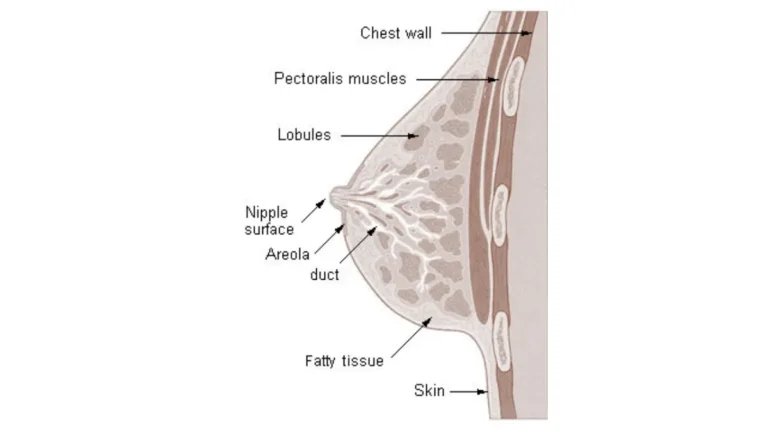
What your breast cancer stage actually means
The moment you hear a stage number, something shifts. The clinical vocabulary that seemed distant five minutes ago suddenly belongs to your life.
Breast cancer staging is a precise clinical measurement — it describes where cancer is in your body and how far it has spread. It is not a verdict. Two patients with identical stage numbers can have dramatically different prognoses depending on tumor biology, biomarker status, and the treatments now available in 2026.
In my practice, I tell every newly diagnosed patient the same thing: the stage tells us where we are starting. It does not tell us where we are going. For a comprehensive overview of how staging connects to long-term prognosis and treatment planning, start with our guide to the breast cancer stages and survival overview.
If you noticed a symptom that led to your diagnosis, our article on breast cancer symptoms and what they mean clinically may also answer questions you have about your initial presentation.
ℹ️ Medical Disclaimer: The diagnostic criteria, staging classifications, treatment options, medication information, and survival statistics discussed in this article reflect current clinical guidelines and are provided for educational purposes only. Individual diagnostic conclusions, treatment decisions, and medication choices depend on factors including patient history, comorbidities, pathology report findings, biomarker results, and specialist assessment. The information in this article does not apply uniformly to every patient and does not substitute for a consultation with a board-certified medical oncologist, surgical oncologist, or gynecologic oncologist who has reviewed your complete clinical picture. Consult a board-certified oncologist before acting on any clinical information in this article.
How the AJCC TNM system defines each breast cancer stage
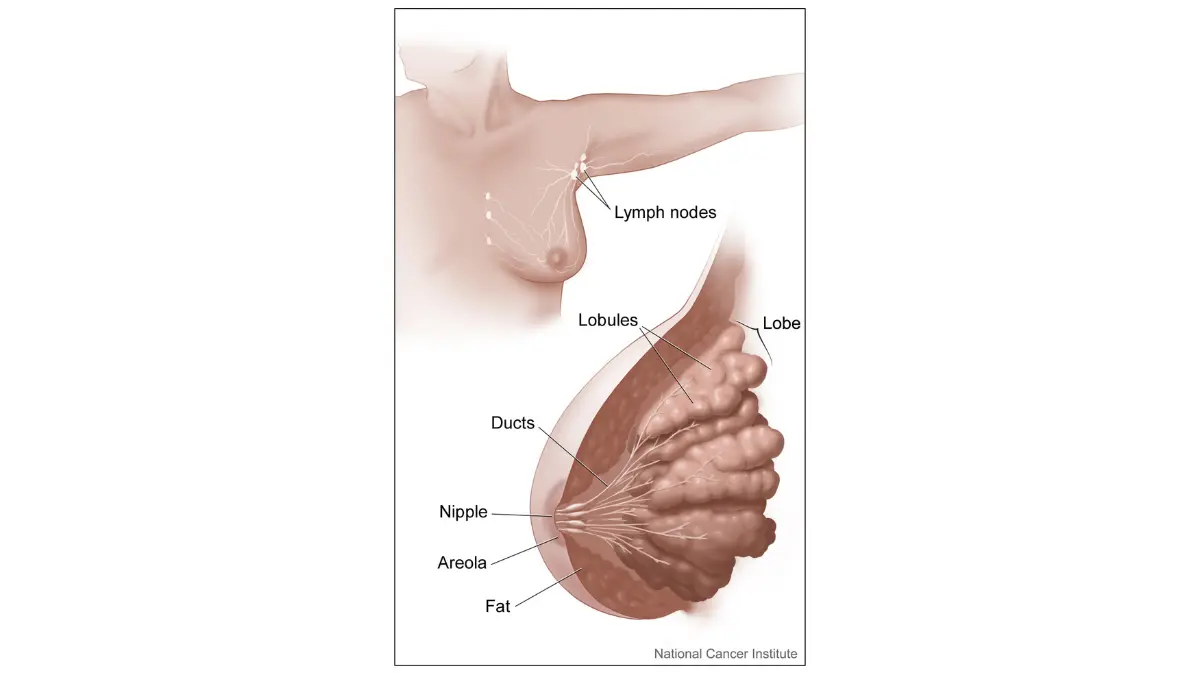
Breast cancer staging uses the American Joint Committee on Cancer (AJCC) 8th Edition TNM system — the current standard used by oncologists across the United States and worldwide. Every stage classification is built from three measurements: tumor size (T), regional lymph node involvement (N), and whether cancer has spread to distant organs — distant metastasis (M).
T, N, and M: the three clinical factors that determine your stage
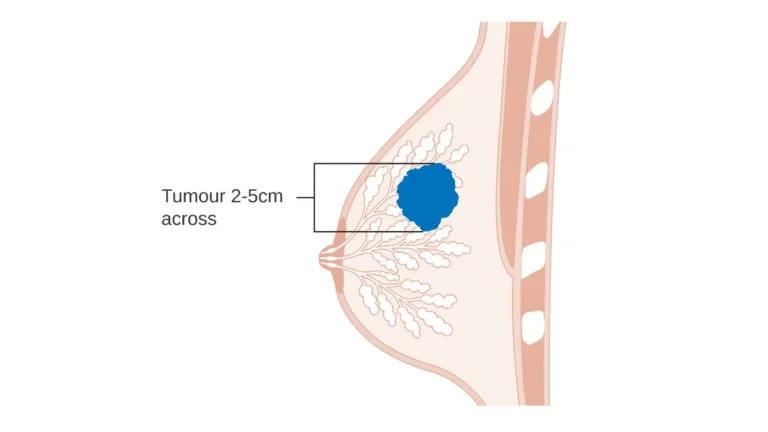
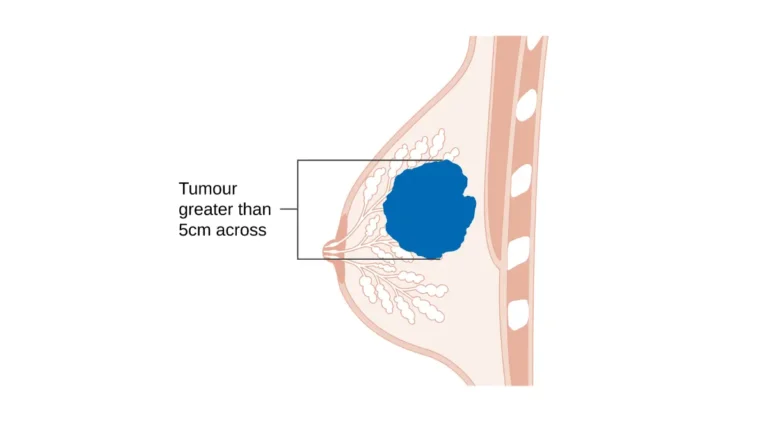
The T classification describes tumor size: T1a means the tumor is 5mm or smaller; T1b ranges from 5 to 10mm; T1c from 10 to 20mm; T2 covers tumors 20 to 50mm; T3 means larger than 50mm; and T4 indicates extension into the chest wall or skin.
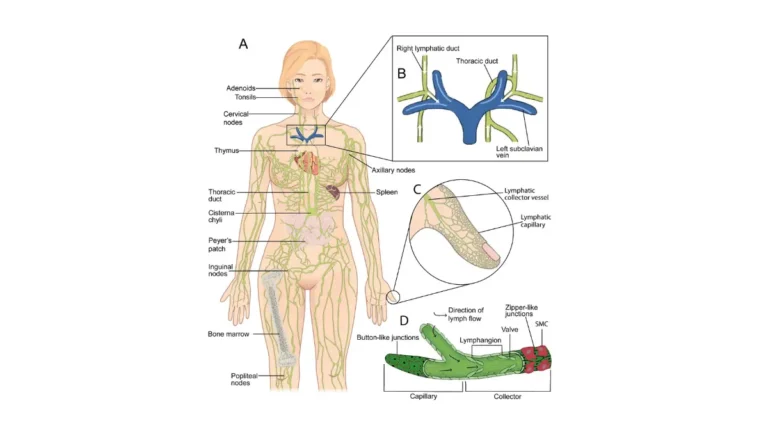
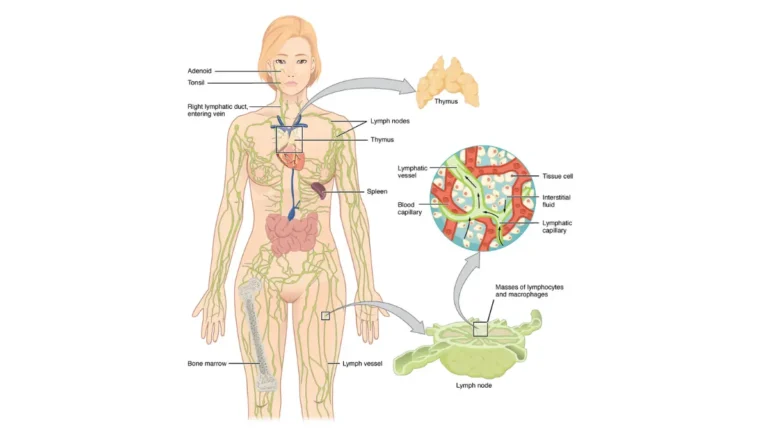
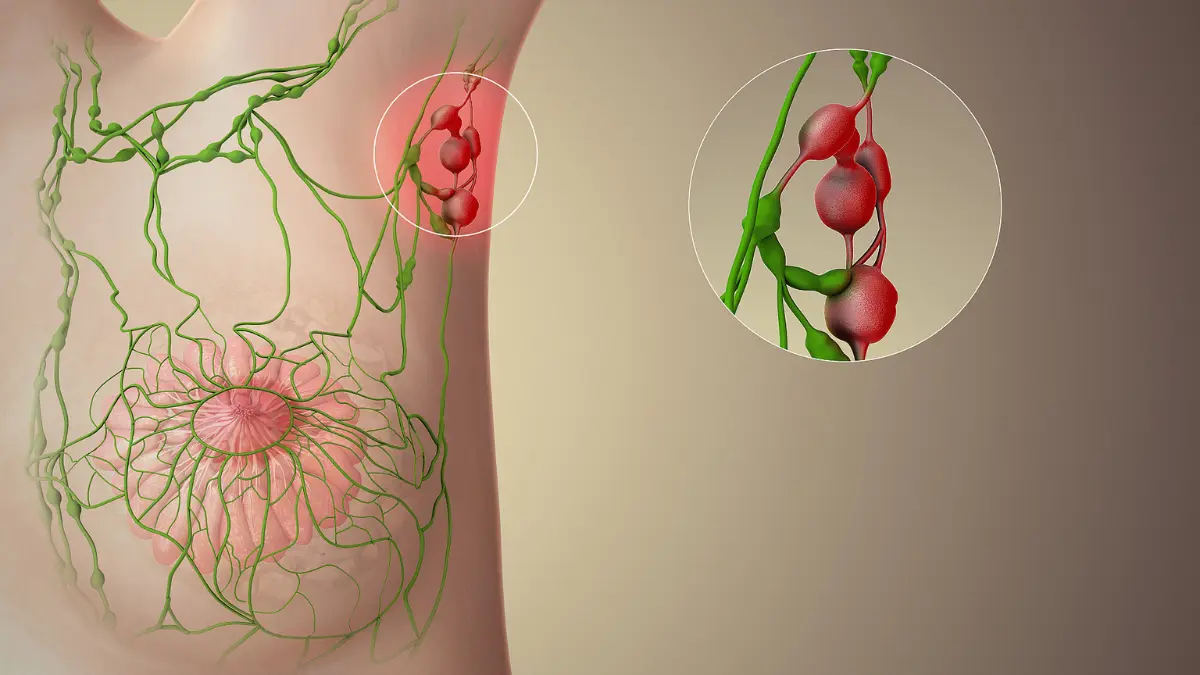
The N classification describes lymph node status: N0 means no nodal involvement; N1mi indicates micrometastasis — cancer deposits larger than 0.2mm but no more than 2mm, or no more than 200 cells; N1 through N3 describe increasingly extensive regional lymph node spread.
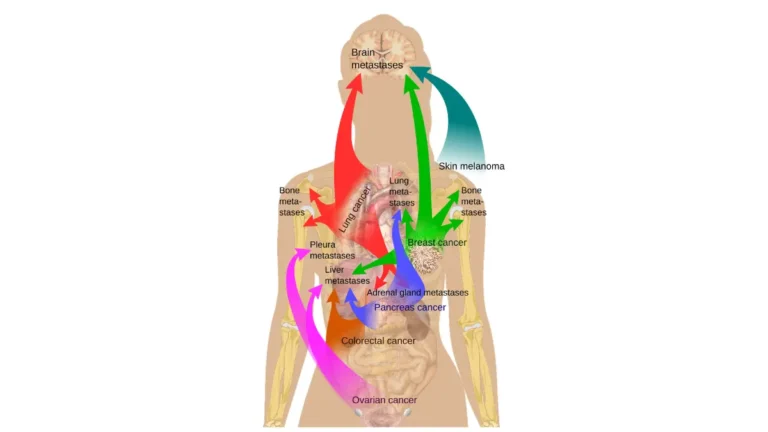
M0 means no distant spread. M1 means cancer has been confirmed in a distant organ — the bones, liver, lungs, or brain — by histologic or cytologic evaluation.
Stage 0 through Stage IV: what each level means
| Stage | Tumor (T) | Nodes (N) | Metastasis (M) | What this means |
|---|---|---|---|---|
| 0 (DCIS) | Tis | N0 | M0 | Abnormal cells confined to milk ducts — not yet invasive |
| IA | T1 (≤20mm) | N0 | M0 | Small tumor, no node involvement, no spread |
| IB | T0 or T1 | N1mi | M0 | Small or no primary tumor; micrometastasis in nodes only |
| IIA | T0–T1, N1 or T2, N0 | — | M0 | Larger tumor or limited node involvement |
| IIB | T2, N1 or T3, N0 | — | M0 | Larger tumor with nodes, or tumor >50mm without nodes |
| IIIA | T0–T2, N2 or T3, N1–2 | — | M0 | Multiple involved lymph nodes — locally advanced |
| IIIB | T4, N0–2 | — | M0 | Tumor involves chest wall or skin |
| IIIC | Any T | N3 | M0 | Extensive nodal spread: ≥10 nodes, or supraclavicular/infraclavicular nodes |
| IV | Any T | Any N | M1 | Confirmed spread to a distant organ |
Source: AJCC 8th Edition Staging System — current standard as of 2026.
Stage 2A vs. 2B: why the substage letter matters
The letter after a stage number is not a minor technical detail. A Stage IIA patient with no lymph node involvement and a 30mm tumor has a meaningfully different treatment conversation than a Stage IIB patient with the same tumor size and three positive nodes. Substages reflect specific TNM combinations — and they affect which treatment sequence your oncologist recommends before you even discuss surgery.
✅ Patient Action: Ask your surgical oncologist or medical oncologist to walk through your specific T, N, and M classifications from your pathology report. You are entitled to understand exactly which criteria placed you in your substage — and how that affects what comes next.
The staging criteria are referenced in the NCI’s breast cancer staging and treatment overview.
🔬 How It Works: The AJCC TNM system works by combining three independent measurements into a single stage. Two patients can share a Stage II classification but arrive at it through completely different TNM combinations — and those combinations determine whether surgery comes first or chemotherapy does.
How doctors determine your breast cancer stage step by step
Breast cancer stage is determined through a sequential diagnostic workup that combines imaging, biopsy pathology, and surgical findings — all classified using the AJCC TNM criteria. Understanding this process helps explain why your stage might look different before and after surgery.
From biopsy to imaging: the pre-surgical workup
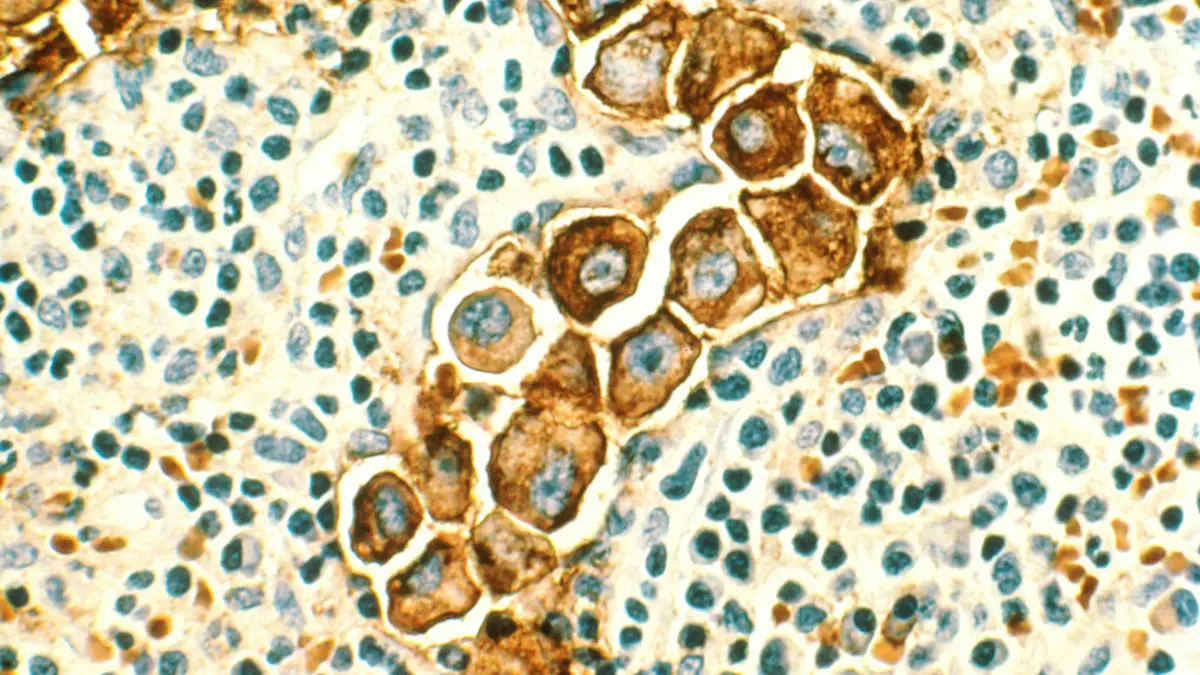
- Core needle biopsy confirms the cancer diagnosis and provides tissue for hormone receptor and HER2 biomarker testing — the results that drive treatment decisions more than the stage number alone.
- Imaging workup — mammogram, breast ultrasound, and MRI if indicated — assesses tumor size, multifocality, and whether the opposite breast is involved.
- Systemic staging imaging — bone scan, CT of the chest and abdomen, or PET-CT if clinically indicated — evaluates whether cancer has spread beyond the breast and regional nodes.
- Sentinel lymph node biopsy evaluates the first one or two lymph nodes that drain the tumor to determine whether cancer cells have entered the lymphatic system.
If you are still in the process of being evaluated, our symptom checker can help you organize your symptoms and medical timeline before your first specialist appointment.
Our guide to sentinel lymph node biopsy — what the procedure involves and what results mean explains this evaluation in detail.
If you received a BI-RADS callback from your mammogram and are trying to understand what it means for your staging workup, see our breakdown of mammogram BI-RADS results from 0 to 6.
Clinical staging vs. pathologic staging: why your stage can change after surgery
In my practice, I explain to every patient before surgery that the stage assigned from imaging — the clinical stage, or cTNM — is our best estimate before we have the full specimen.
After surgery, the pathologist examines the removed tumor and any lymph nodes directly. That produces the pathologic stage, or pTNM — the definitive classification your oncology team uses for all subsequent treatment decisions. Pathologic stage may be higher or lower than clinical stage. This is expected, not alarming. It means the surgical pathology gave your team more precise information than imaging alone could provide.
✅ Patient Action: Before your surgery, ask your surgical oncologist: “What is my clinical stage right now, and how might my pathologic stage differ once you have the full specimen? What would change in my treatment plan if the stage is revised?”
What treatment typically looks like at each breast cancer stage
Breast cancer treatment is not one-size-fits-all — it is stage-specific, biomarker-directed, and increasingly personalized. The following frameworks reflect current NCCN 2026 guidelines; your oncology team will tailor these to your exact tumor profile.
Stage 0 and Stage I: surgery-first with targeted adjuvant therapy
Stage 0 (DCIS) and Stage I invasive breast cancer are generally managed with a surgery-first approach. Lumpectomy with radiation or mastectomy removes the primary tumor. If the tumor is ER-positive or PR-positive, adjuvant hormone therapy — tamoxifen for premenopausal women, an aromatase inhibitor for postmenopausal women — reduces recurrence risk over five to ten years.
For HER2-positive Stage I tumors 10mm or larger (T1b+), trastuzumab-based adjuvant therapy is added per NCCN 2026 guidelines.
Our detailed guide to what a mastectomy involves and what your surgeon may not tell you upfront covers the surgical decision in depth.
Stage II and Stage III: multimodal treatment and the case for neoadjuvant chemotherapy
Neoadjuvant chemotherapy — chemotherapy given before surgery — is standard for most Stage III patients and increasingly used for Stage II patients with high-risk features. The clinical rationale is twofold: shrinking the tumor before surgery may allow breast-conserving surgery instead of mastectomy, and measuring the tumor’s response to chemotherapy in real time provides critical prognostic information.
For HER2-negative patients, standard neoadjuvant regimens typically include an anthracycline-taxane sequence (AC→T). For HER2-positive patients, TCH (docetaxel, carboplatin, trastuzumab) or AC→TH±pertuzumab is the current standard per NCCN 2026 guidelines. For HER2-positive Stage III patients with residual disease after neoadjuvant therapy, T-DM1 (trastuzumab emtansine) as adjuvant therapy has significantly improved outcomes.
See our guide to how chemotherapy works and what to expect from side effects in 2026 for a patient-focused breakdown of the treatment process.
Stage IV: systemic therapy and the goal of long-term disease control
Stage IV breast cancer is treated with systemic therapy selected by biomarker profile — hormone therapy plus CDK4/6 inhibitors for ER-positive/HER2-negative disease; anti-HER2 regimens for HER2-positive disease; immunotherapy with pembrolizumab plus chemotherapy for PD-L1-positive triple-negative disease.
The clinical goal at Stage IV is long-term disease control, not surgical removal. Sustained responses lasting years are well-documented in current practice — particularly in HER2-positive disease.
⚠️ Clinical Warning: No treatment plan for Stage II, III, or IV breast cancer should be finalized before your tumor has been fully tested for ER, PR, HER2, and — where appropriate — PD-L1 expression. The biomarker profile changes which therapy has the strongest evidence base for your specific case.
✅ Patient Action: Before agreeing to a treatment plan, ask your medical oncologist: “Am I a candidate for neoadjuvant chemotherapy before surgery, and how does my full biomarker profile — ER, PR, HER2, Ki-67, and PD-L1 — determine which drugs we use and in which order, per current NCCN 2026 guidelines?”
Breast cancer survival rates by stage: what the numbers actually mean
Breast cancer survival rates by stage come from the NCI SEER database — the most comprehensive population-level cancer outcomes registry in the United States. Before reading the table below, read what follows it. These numbers are real and they matter. They also require context to be clinically useful rather than frightening.
5-year relative survival rates by stage: the 2026 NCI SEER data
| Stage | 5-Year Relative Survival Rate | What this reflects |
|---|---|---|
| 0 (DCIS) | >99% | Non-invasive disease; highly treatable |
| I | >99% | Localized tumor, no nodal involvement |
| II | ~86–90% | Localized-regional disease; curative intent |
| III | ~73–86% | Locally advanced; curative intent with multimodal therapy |
| IV | ~28% | Distant metastasis; population-level average from prior treatment eras |
📊 Clinical Data Point: 5-year relative survival rates for breast cancer by AJCC stage — Source: NCI SEER database, 2026
Why the survival rate is not your personal prognosis
Three facts every patient must understand before internalizing these numbers.
First, these rates reflect patients diagnosed years ago under older treatment protocols. Patients receiving current HER2-targeted regimens, CDK4/6 inhibitors, and immunotherapy are not captured in five-year-old diagnosis cohorts. The baseline figures — particularly for Stage IV — understate what current therapy achieves.
Second, 5-year relative survival is a population average. It describes what happened to a large group of people with similar staging. It does not describe what will happen to you specifically, and it cannot account for your biomarker profile, your treatment response, or your overall health status.
Third, survival rates are not ceiling values. They are central estimates. Many patients live well beyond them.
🩺 Physician Note: In my clinical experience, the Stage IV figure is the one that causes the most harm when read without context. I have patients with HER2-positive Stage IV breast cancer who are five years into sustained disease control on targeted therapy — well beyond what that 28% figure implies. The number is not wrong. It is incomplete without the biology of your specific tumor. — Dr. Carolyn D. Fairweather, MD, Gynecologic Oncology
How biomarker status changes the survival picture
Invasive ductal carcinoma — the most common type — has meaningfully different survival trajectories depending on whether it is ER-positive, HER2-positive, or triple-negative. Our article on invasive ductal carcinoma cure rates and treatment outcomes by subtype breaks this down in detail.
The survival rates in the table above are sourced from the NCI SEER breast cancer outcomes data.
✅ Patient Action: Ask your medical oncologist: “Given my specific stage, my complete biomarker profile, and my overall health, how do these population-level survival figures apply — or not apply — to my individual prognosis? What does my response to initial treatment tell you about my likely trajectory?”
How ER, PR, and HER2 status change your prognosis at every stage
Breast cancer staging tells you where the cancer is. Hormone receptor and HER2 status tell you how the cancer behaves — and they are equally important in determining your prognosis and your treatment options.
ER-positive and PR-positive tumors: the most common and most treatable subtype
ER-positive and PR-positive tumors — the most frequently diagnosed molecular subtype — respond to hormone-blocking therapy. At every stage from I through IV, hormone receptor-positive disease can be controlled with agents including tamoxifen, aromatase inhibitors, and CDK4/6 inhibitors. These therapies have extended progression-free survival substantially in Stage IV ER-positive disease over the past decade.
Within the ER-positive subtype, the Ki-67 proliferation index matters. Tumors with a high Ki-67 score — generally defined as ≥20% by immunohistochemistry — divide more rapidly than low Ki-67 counterparts. High Ki-67 ER-positive tumors often require a more aggressive upfront chemotherapy approach. This is a nuance your oncologist should discuss with you before any treatment plan is finalized.
HER2-positive breast cancer: how targeted therapy reshapes prognosis at every stage
HER2-positive tumors, accounting for approximately 15–20% of all diagnoses, are treated with HER2-targeted agents — trastuzumab, pertuzumab, T-DM1, and others — at every stage above 0. Per NCCN 2026 guidelines, targeted therapy is added to chemotherapy for HER2-positive disease at Stage I through Stage IV. The impact on Stage IV outcomes has been substantial: HER2-positive metastatic breast cancer managed with current anti-HER2 regimens achieves survival well above the population-level baseline figure.
Triple-negative breast cancer: why stage is especially critical for this subtype
Triple-negative breast cancer lacks ER, PR, and HER2 targets, making chemotherapy the backbone of treatment at every stage. Immunotherapy with pembrolizumab is now approved for early-stage and metastatic triple-negative disease meeting PD-L1 criteria. Because triple-negative tumors tend to be more aggressive, stage at diagnosis is particularly important for this subtype — early detection changes outcomes significantly.
For patients whose oncologist has mentioned hereditary breast cancer risk or BRCA testing, use our genetic risk assessment tool to understand whether genetic counseling is appropriate for your personal and family history.
If you have already received BRCA results and need help interpreting them, our guide to reading your BRCA test results in plain language explains every possible result clearly.
📊 Clinical Data Point: HER2-positive breast cancer accounts for approximately 15–20% of invasive breast cancer diagnoses. Triple-negative breast cancer accounts for approximately 10–15%. Both figures require verification against 2026 ACS or NCI data at publish. Source: American Cancer Society 2026 breast cancer statistics — ACS 2026 breast cancer statistics report.
✅ Patient Action: Ask your oncologist: “What is my complete biomarker profile — ER status, PR status, HER2 status, and Ki-67 score — and how does each change my treatment options and my prognosis at my specific stage? Should I also be evaluated for BRCA1 or BRCA2 mutations given my personal and family history?”
Dr. Fairweather’s clinical perspective: what I tell every newly diagnosed patient
The most common misconception I encounter after a staging conversation is this: patients hear a number and stop listening. Stage III becomes a verdict. Stage IV becomes a timeline. Neither is accurate, and both prevent patients from asking the questions that actually matter.
The most common staging misconception I see in clinical practice
In my clinical practice, I have watched a Stage IV HER2-positive patient receive a prognosis that the raw statistics would suggest was dire — and then go on to achieve four years of stable disease on pertuzumab and trastuzumab before her most recent scan showed a complete response. I have also watched a Stage III patient with an ER-positive, low Ki-67 tumor complete neoadjuvant therapy, achieve pathologic complete response, and return to full work activity within eight months of diagnosis. Neither outcome was predictable from the stage number alone.
Stage tells us the terrain. Biomarker status, treatment response, and the expertise of your oncology team tell us what is possible within that terrain.
Three questions I wish every patient would bring to their next oncology appointment
I recommend every newly diagnosed patient bring these three specific questions to their next appointment with a board-certified medical oncologist or surgical oncologist:
- “What is my complete TNM classification from my pathology report, and what does my specific substage mean for the sequence of my treatment?”
- “Am I a candidate for clinical trial enrollment at my current stage and subtype — and if so, what trials are currently active near me?” For patients with Stage IV disease, active clinical trials for Stage IV breast cancer at ClinicalTrials.gov may offer access to emerging treatments not yet available as standard of care.
- “If my pathologic stage after surgery differs from my clinical stage now, how would that change my adjuvant treatment plan?”
✅ Patient Action: If you have not yet had a dedicated consultation with a board-certified medical oncologist or surgical oncologist to discuss your stage and your treatment options, that appointment is your most important immediate next step. Bring your full pathology report. Ask for your complete TNM substage, your biomarker panel results, and your treatment options before any plan is finalized.
Breast cancer stages: frequently asked questions
1. What are the 4 stages of breast cancer?
Breast cancer staging uses the AJCC TNM system to classify disease across five levels based on tumor size, lymph node involvement, and whether cancer has spread to distant organs. Stage 0 means abnormal cells are confined to ducts. Stages I through III describe increasingly advanced local and regional disease, from small localized tumors to extensive lymph node involvement. Stage IV indicates confirmed spread to a distant organ such as the bones, liver, lungs, or brain.
2. What is Stage 1 breast cancer survival rate?
According to NCI SEER data, Stage I breast cancer carries a 5-year relative survival rate exceeding 99%. This means more than 99 of every 100 patients diagnosed at Stage I are alive five years later — making it the most favorable stage for long-term outcomes. This figure reflects population averages and does not account for individual differences in biomarker profile or treatment response. Consult a board-certified oncologist to interpret your specific prognosis.
3. What is Stage 4 breast cancer life expectancy?
The 5-year relative survival rate for Stage IV metastatic breast cancer is approximately 28% based on NCI SEER population data — but this figure reflects historical averages from prior treatment eras. HER2-positive patients on current targeted regimens and hormone receptor-positive patients on CDK4/6 inhibitor combinations frequently achieve outcomes substantially above this baseline. Discuss your individual prognosis with your medical oncologist before drawing any conclusions from population-level statistics.
4. Is Stage 3 breast cancer curable?
Stage III breast cancer is treated with curative intent. Neoadjuvant chemotherapy, surgery, radiation, and biomarker-directed adjuvant therapy together achieve long-term disease control in many patients. The 5-year relative survival rate for Stage III disease ranges approximately 73–86% depending on substage and biomarker profile. Pathologic complete response after neoadjuvant therapy — no detectable residual cancer in the surgical specimen — is associated with particularly favorable long-term outcomes. Ask your oncologist what response milestones define successful treatment at your specific substage.
5. How is breast cancer stage determined?
Breast cancer stage is determined through a sequential diagnostic workup: core needle biopsy confirms the diagnosis and provides tissue for biomarker testing; imaging studies assess tumor size and extent of disease; sentinel lymph node biopsy evaluates nodal involvement; and surgical pathology provides the definitive pathologic stage after tumor removal. Clinical stage before surgery may differ from final pathologic stage — the pathologic stage is always the definitive classification used for treatment planning.
6. What does Stage 2 breast cancer mean?
Stage II breast cancer means the tumor is 20mm or larger and/or 1–3 regional lymph nodes are involved, with no evidence of distant spread. Stage IIA describes a smaller tumor with limited nodal involvement. Stage IIB describes a larger tumor or greater lymph node spread within the same regional tier. Both substages are treated with curative intent. Ask your oncologist which substage applies to your pathology report and how it affects the sequence of your recommended treatment.
7. Can Stage 4 breast cancer go into remission?
Yes — Stage IV breast cancer can respond to systemic therapy to the point of complete or partial remission. This occurs in a meaningful proportion of patients, particularly those with HER2-positive tumors on targeted agents. Remission in Stage IV does not mean the cancer is permanently eradicated, but sustained disease control lasting years is well-documented in current oncology practice. Ask your oncologist what response markers apply to your specific treatment regimen.
8. What is Stage 0 breast cancer (DCIS)?
Stage 0 breast cancer, formally called ductal carcinoma in situ (DCIS), means abnormal cells have developed inside the milk ducts but have not invaded surrounding breast tissue. It is non-invasive and carries a 5-year relative survival rate exceeding 99%. Treatment typically involves lumpectomy with radiation or mastectomy, sometimes followed by hormone therapy for ER-positive DCIS. Ask your surgeon whether adjuvant hormone therapy is recommended based on your specific DCIS grade and receptor characteristics.
9. What is the difference between Stage 2A and 2B breast cancer?
Stage IIA and IIB share the same overall stage label but reflect different tumor-node combinations. Stage IIA includes tumors up to 20mm with 1–3 positive lymph nodes, or tumors 20–50mm with no nodal involvement. Stage IIB includes tumors 20–50mm with 1–3 positive nodes, or tumors larger than 50mm with no nodal involvement. Both are treated with curative intent, though the specific treatment sequence and neoadjuvant chemotherapy decision varies by substage and biomarker status.
10. Does breast cancer stage change over time?
The stage number assigned at initial diagnosis does not change retroactively — Stage II at diagnosis remains Stage II in medical records even if disease later progresses. If cancer spreads to a new site after initial treatment, it is described as recurrent or metastatic disease, not as a higher original stage. Your oncologist will use the new clinical picture to guide retreatment decisions rather than revising the original staging classification.
11. What is the most common stage at breast cancer diagnosis in the US?
According to NCI SEER data, approximately 63% of US breast cancer diagnoses are made at a localized stage before lymph node involvement — largely because of mammography screening programs. Early detection at Stage I or early Stage II is why breast cancer survival rates have improved substantially in recent decades. Ask your oncologist when screening is appropriate for your specific age and risk profile, particularly if you have a family history of breast or ovarian cancer.
12. How does HER2 status affect breast cancer prognosis?
HER2-positive breast cancer, accounting for approximately 15–20% of diagnoses, responds to targeted therapy at every stage above 0. Trastuzumab and pertuzumab added to chemotherapy have substantially improved outcomes across all HER2-positive stages, including Stage IV. HER2-positive patients on current anti-HER2 regimens frequently achieve survival outcomes well above what population-level statistics suggest. Ask your oncologist whether your tumor has been tested for HER2 amplification by immunohistochemistry or FISH, and what a positive result means for your treatment plan.
13. What treatment is typically used for Stage 3 breast cancer?
Stage III breast cancer is typically treated with a four-step sequence: neoadjuvant chemotherapy — commonly an anthracycline-taxane regimen such as AC-T, or TCH for HER2-positive tumors — to shrink the tumor before surgery; surgical removal by mastectomy or lumpectomy depending on treatment response; radiation therapy to the chest wall and regional nodes; and adjuvant hormone or HER2-targeted therapy based on biomarker status per current NCCN guidelines.
Ask your oncologist which neoadjuvant regimen is appropriate for your biomarker profile before treatment begins.
14. Is Stage 2 breast cancer serious?
Stage II breast cancer is a serious diagnosis requiring prompt multimodal treatment, but it carries a 5-year relative survival rate of approximately 86–90% based on NCI SEER data. Most Stage II patients are treated with curative intent and achieve long-term disease control. Biomarker status — particularly ER, PR, and HER2 — significantly influences both prognosis and treatment selection even within the same substage. Ask your oncologist what your specific substage and biomarker profile mean for your individual treatment plan and prognosis.
15. What is triple-negative breast cancer staging?
Triple-negative breast cancer (ER-negative, PR-negative, and HER2-negative) is staged using the same AJCC TNM system as all breast cancer subtypes. Because it lacks hormone receptor and HER2 targets, chemotherapy is the primary systemic treatment at every stage. Immunotherapy with pembrolizumab is now approved for early-stage and metastatic triple-negative disease meeting specific PD-L1 criteria. Ask your oncologist whether immunotherapy is appropriate for your stage and whether PD-L1 testing has been performed on your tumor.
16. Can breast cancer be cured at Stage 1?
Stage I breast cancer is associated with a 5-year relative survival rate exceeding 99%, and most patients treated with standard therapy — lumpectomy or mastectomy with appropriate adjuvant treatment based on biomarker status — have no evidence of disease at five years. Long-term disease-free survival is the expected outcome for most Stage I patients. Ask your oncologist what surveillance schedule is recommended after treatment to monitor for recurrence at your specific substage and molecular subtype.
17. What is the difference between clinical and pathologic staging?
Clinical staging — also called pre-surgical or cTNM staging — is assigned before surgery based on imaging studies, biopsy pathology, and physical examination. Pathologic staging — pTNM — is assigned after surgery when the pathologist examines the removed tumor and lymph nodes directly. Pathologic staging is always the definitive classification and may be higher or lower than the initial clinical stage. If your stage changed after surgery, that is an expected and normal part of the staging process — not a sign that something went wrong.
Your next steps after learning your breast cancer stage
Your stage is the beginning of the clinical conversation — not the end of it.
The TNM classification tells your oncology team where the cancer is. Your biomarker profile tells them how it behaves. Your treatment response will tell them how effectively your specific tumor can be controlled. None of these variables operates independently — and no one number defines what is possible for you.
If you have not yet had a dedicated appointment with a board-certified medical oncologist or surgical oncologist to discuss your staging, your biomarker results, and your treatment options, schedule that appointment as your first concrete step. Bring your full pathology report. Ask for your complete TNM substage. Ask about your ER, PR, HER2, and Ki-67 results before any treatment plan is finalized.
If you have not yet discussed genetic testing with your care team, our genetic risk assessment tool can help you assess whether BRCA evaluation is appropriate based on your personal and family history.
And if you are still in the early stages of understanding what led to your diagnosis, our article on the first signs of breast cancer symptoms and what they mean provides context for the symptoms and findings that initiated your workup.
Your stage describes where you are starting. Your care team — and the treatments available in 2026 — determine where you go from here.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.