
On This Page – Quick Medical Summary
Understanding Your BRCA Test Results Instantly
Rachel Martinez, a 38-year-old teacher from Austin, Texas, stared at the envelope for twenty minutes before opening it. Inside was her BRCA test result—a single page that would determine her cancer screening strategy for life. Like 300,000 Americans who receive genetic testing results each year, she needed to understand what those numbers and medical terms actually meant.
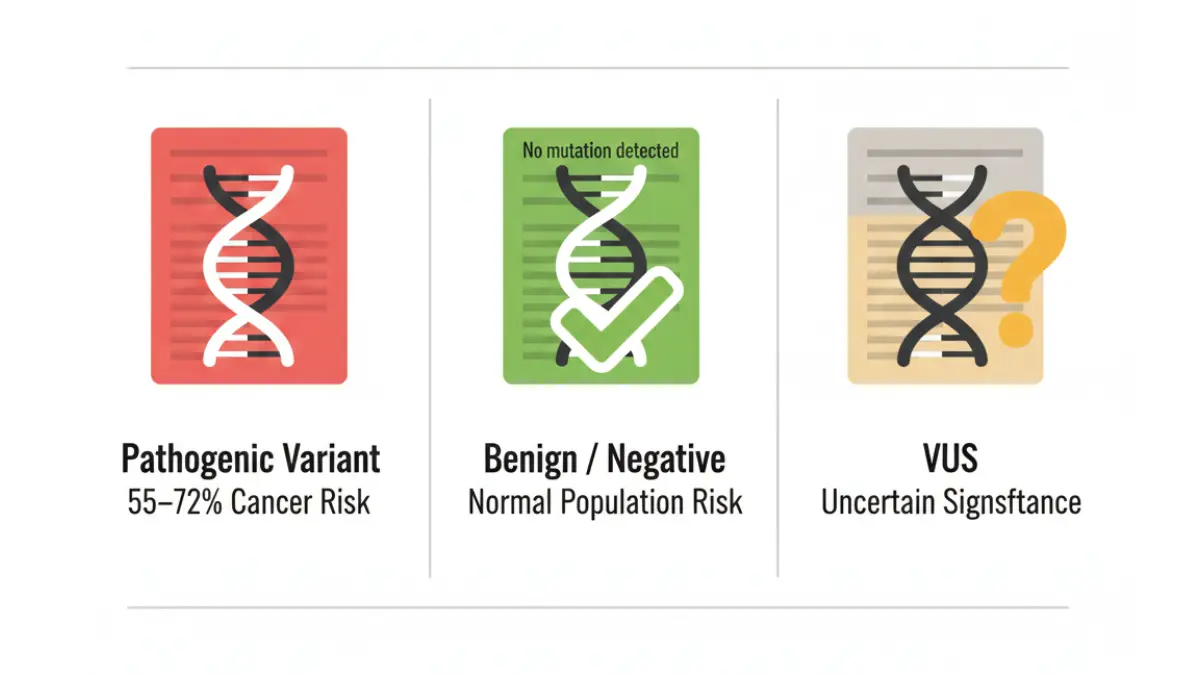
Here’s what you need to know immediately: BRCA results reveal whether you carry a harmful mutation in the BRCA1 or BRCA2 genes that significantly increases your risk of breast, ovarian, prostate, and pancreatic cancers. There are three possible outcomes—positive (pathogenic variant detected), negative (no harmful mutation found), or VUS (variant of uncertain significance). Your result doesn’t predict if you’ll develop cancer, but it does indicate your risk level and guide prevention strategies.
According to the National Cancer Institute, approximately 1 in 400 people in the general population carries a BRCA mutation, but this rises dramatically to 1 in 40 among Ashkenazi Jewish individuals. Understanding your BRCA results is the first step toward proactive health management, and our Genetic Risk Assessment Tool can help you evaluate your overall genetic risk profile.
Quick Reference: The 3 BRCA Result Types
| Result Type | What It Means | Next Steps |
|---|---|---|
| Positive | Pathogenic mutation detected | Enhanced screening, risk-reduction options |
| Negative | No harmful mutation found | Standard screening (varies by family history) |
| VUS | Uncertain significance | Treat as negative, monitor for reclassification |
What This Means For You: Reading your BRCA results correctly determines your entire cancer prevention strategy. This 2026 guide translates complex genetic terminology into actionable health decisions backed by the latest medical research and clinical guidelines.
Understanding Your BRCA Results: The 3 Outcomes
Positive Result (Pathogenic Variant Detected)
A positive BRCA result means laboratory testing identified a harmful mutation—either in BRCA1 or BRCA2—that significantly elevates your cancer risk. This is NOT a cancer diagnosis. It’s a risk indicator that helps you and your medical team create a proactive prevention plan.
2026 Cancer Risk Statistics:
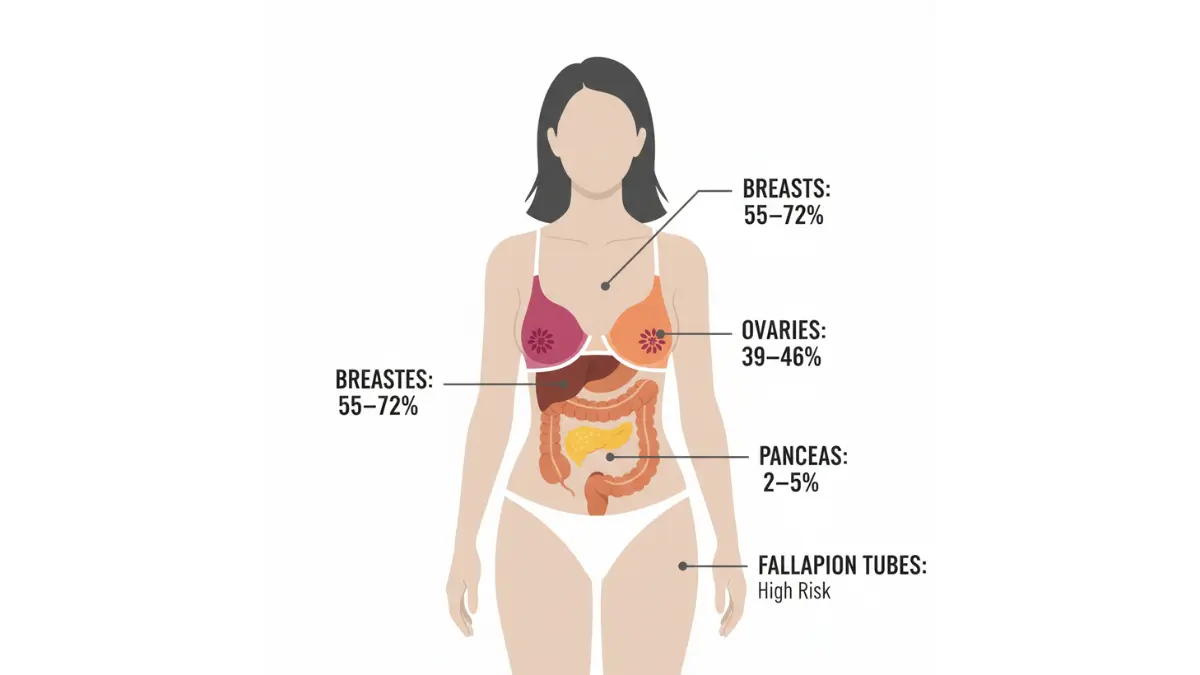
Women with BRCA1 mutations face a 55-72% lifetime risk of developing breast cancer by age 70, compared to the general population risk of 12-13%. For BRCA2 mutations, the breast cancer risk is 45-69% by age 70. The American College of Obstetricians and Gynecologists reports that ovarian cancer risk reaches 39-46% for BRCA1 carriers and 10-27% for BRCA2 carriers by age 70.
Key Points About Positive Results:
- Your children have a 50% chance of inheriting the same mutation
- Enhanced screening protocols start earlier (often age 25-30)
- Risk-reduction surgeries can decrease cancer risk by 90%
- PARP inhibitor medications are now available for prevention
- Not everyone with a mutation develops cancer—some never do
Men with BRCA2 mutations face an 8% lifetime breast cancer risk (compared to 0.1% in the general population) and a 25-50% prostate cancer risk. The National Comprehensive Cancer Network updated their 2026 guidelines to recommend annual prostate screening starting at age 40 for male BRCA carriers.
Your Risk vs. General Population:
| Cancer Type | BRCA1 Risk | BRCA2 Risk | General Population |
|---|---|---|---|
| Breast (Female) | 55-72% | 45-69% | 12-13% |
| Ovarian | 39-46% | 10-27% | 1.5% |
| Prostate (Male) | 20-25% | 25-50% | 14% |
| Pancreatic | 2-3% | 3-5% | 1% |
Similar to how you might use a BMI Calculator to assess weight-related health risks, BRCA testing quantifies your genetic cancer risk so you can take preventive action.
Negative Result (No Harmful Mutation Detected)
A negative BRCA test result can have two very different meanings depending on your family history. Understanding which type of negative result you received is crucial for determining your ongoing screening needs.
True Negative Result:
This occurs when a known family mutation has been ruled out. For example, if your mother tested positive for a specific BRCA1 mutation and you test negative for that same mutation, you have a true negative. Your cancer risk returns to general population levels, and you can follow standard screening guidelines.
Uninformative Negative Result:
This happens when you test negative but no family member with cancer has been tested first, or your family doesn’t have a known mutation. According to research published in the Journal of Medical Genetics, an uninformative negative doesn’t rule out hereditary cancer risk. Your family may carry a mutation in a different gene (PALB2, CDH1, TP53) or have a BRCA variant that current testing didn’t detect.
What Negative Results Mean for Screening:
- True negative: Follow age-appropriate screening for general population
- Uninformative negative with strong family history: Enhanced screening may still be recommended
- Consider expanded panel testing: Test for 50+ other cancer-related genes
- Family members with cancer should test first: Provides most informative results
The distinction between these two types of negative results confuses approximately 35% of patients, according to 2025 data from genetic counseling sessions. If you’re uncertain which type of negative result you received, schedule a consultation with a board-certified genetic counselor through the National Society of Genetic Counselors.
VUS – Variant of Uncertain Significance (The Confusing Result)
Here’s what competitors don’t tell you: 40-45% of people undergoing comprehensive genetic panel testing receive a VUS result. A variant of uncertain significance means the laboratory detected a genetic change in BRCA1 or BRCA2, but current scientific evidence can’t determine whether this specific variant increases cancer risk.
Why VUS Results Happen:
Genetic testing laboratories compare your DNA sequence to massive databases containing thousands of previously classified variants. When your result shows a genetic change that hasn’t been studied enough, it gets classified as VUS. Think of it as medical science saying “we found something different, but we don’t yet know if it matters.”
Critical Facts About VUS:
- Most VUS results (approximately 90%) eventually get reclassified as benign (harmless)
- Only 5-10% get upgraded to pathogenic (disease-causing)
- Reclassification typically occurs within 2-5 years as research advances
- You should request lab updates every 2-3 years
- For medical management purposes, treat VUS as a negative result
Dr. Sarah Chen, genetic counselor at MD Anderson Cancer Center, explains: “A VUS doesn’t change your medical management. We base screening recommendations on your personal and family cancer history, not on the uncertain variant.”
How VUS Reclassification Works:
The laboratory continues monitoring scientific literature and variant databases. When enough evidence accumulates—either from population studies, functional testing, or family segregation analysis—they reclassify the variant. Your healthcare provider should receive automatic updates when reclassification occurs.
2026 Update: Advanced computational tools and international data-sharing initiatives have reduced VUS rates by 18% since 2023. The ClinGen Evidence Repository now contains over 3.2 million variant classifications, accelerating the reclassification process.
Family cascade testing—when multiple blood relatives get tested—can help resolve VUS results faster. If three relatives with breast cancer all carry the same variant, it suggests pathogenicity. Conversely, if healthy elderly relatives also carry it, the variant is likely benign.
How to Interpret Your BRCA Laboratory Report
Your BRCA test results arrive as a multi-page laboratory report filled with technical terminology that can overwhelm even medically-trained individuals. Understanding the key sections helps you have informed conversations with your healthcare team.
Key Sections of Your Report
Patient Identifiers and Test Information:
The first page verifies your demographic information and lists which specific test was performed. Confirm your name, date of birth, and medical record number match exactly. The test methodology section indicates whether you received comprehensive BRCA1/BRCA2 sequencing, a targeted familial variant test, or an expanded multi-gene panel.
Variant Classification Section:
This is the most critical part of your report. The laboratory lists any genetic variants detected and assigns them a classification level using the American College of Medical Genetics (ACMG) five-tier system:
- Class 5 – Pathogenic: Confirmed disease-causing mutation
- Class 4 – Likely Pathogenic: Probably disease-causing (>90% certainty)
- Class 3 – VUS: Uncertain significance
- Class 2 – Likely Benign: Probably harmless
- Class 1 – Benign: Confirmed harmless variation
Clinical Significance Statement:
This section translates the variant classification into plain language. You’ll see phrases like “This result is consistent with hereditary breast and ovarian cancer syndrome” (positive result) or “No pathogenic or likely pathogenic variants detected” (negative result).
Recommendations Section:
The laboratory typically includes clinical management suggestions, such as “Genetic counseling is recommended” or “Enhanced surveillance may be appropriate.” These recommendations follow National Comprehensive Cancer Network guidelines.
Confusing Terms Translated
Medical reports use precise terminology that can confuse patients. Here’s what key terms actually mean:
Pathogenic / Likely Pathogenic = Positive Result
- Your test detected a harmful mutation
- Increased cancer risk confirmed
- Risk-reduction strategies recommended
Benign / Likely Benign = Negative Result
- No harmful mutation detected
- Return to general population risk (if true negative)
- Standard screening applies
Variant of Uncertain Significance (VUS) = Uncertain Result
- Genetic change detected but significance unknown
- Treat as negative for medical management
- Request updates as research evolves
Germline vs. Somatic Mutation:
- Germline: Inherited mutation present in all cells (what BRCA testing detects)
- Somatic: Acquired mutation only in tumor cells (not inherited, not passed to children)
Penetrance Percentage:
- Likelihood that someone with the mutation will develop cancer
- BRCA1/BRCA2 have “high penetrance” (60-80% develop cancer)
- Not a guarantee—just a probability estimate
Red Flags to Discuss with Your Doctor
Certain situations warrant additional consultation with your genetic counselor or ordering physician:
Laboratory Accreditation Issues: Ensure your test was performed at a CLIA-certified and CAP-accredited laboratory. Unaccredited labs may provide unreliable results. Check laboratory credentials through the College of American Pathologists database.
Missing Family History Consideration: If your report doesn’t reference your family cancer history, the interpretation may be incomplete. Genetic counselors integrate family pedigree analysis with test results for comprehensive risk assessment.
Conflicting Recommendations: If your report’s recommendations contradict what your physician advised, seek clarification. Sometimes laboratories provide generic guidance that needs personalization based on your complete medical picture.
Detailed interpretation of laboratory reports parallels understanding other medical test results, similar to decoding CBC test results where specific values require clinical context.
What To Do After Getting BRCA Results
If You’re BRCA Positive: Your 30/60/90-Day Action Plan
Receiving a positive BRCA result requires immediate action but not panic. Following a structured timeline helps you make informed decisions without feeling overwhelmed.
First 30 Days – Information Gathering:
Schedule a comprehensive genetic counseling session within 2-3 weeks of receiving results. A board-certified genetic counselor will review your specific mutation, explain cancer risks by organ system, and outline prevention options. Average cost: $250-$350, typically covered by insurance when medically indicated.
Inform first-degree relatives (parents, siblings, children) about your positive result. Each has a 50% chance of carrying the same mutation. Provide them with your specific genetic variant information so their testing can be targeted and cost-effective ($250-$400 for single-site familial testing versus $1,500-$3,500 for comprehensive testing).
Document your complete family cancer history going back three generations. Include cancer types, ages at diagnosis, and whether relatives are still living. This pedigree analysis helps risk stratification and influences surveillance intensity.
Review your current health insurance policy’s genetic testing and prevention coverage. The Genetic Information Nondiscrimination Act protects against health insurance discrimination but doesn’t cover life, disability, or long-term care insurance.
Days 31-60 – Enhanced Screening Protocol:
Establish a high-risk surveillance program with specialists experienced in hereditary cancer management. The 2026 NCCN guidelines recommend:
For BRCA-Positive Women:
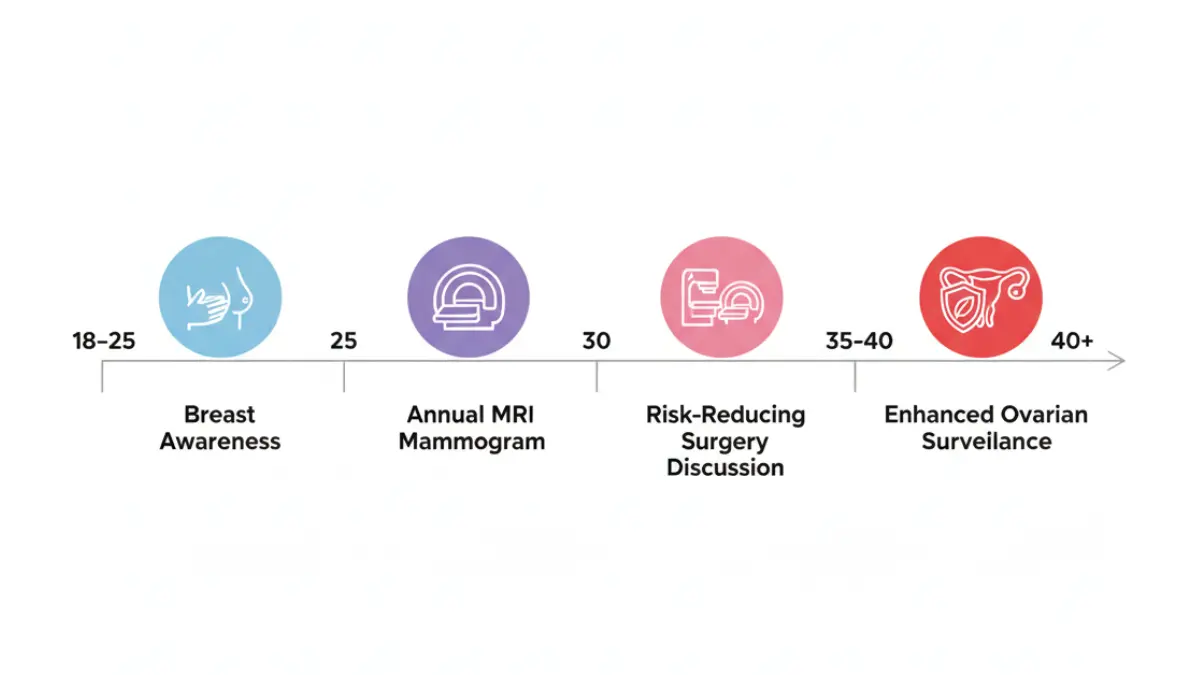
- Breast awareness and self-examination training starting age 18
- Clinical breast exams every 6-12 months starting age 25
- Annual breast MRI screening starting age 25-30
- Annual mammogram starting age 30 (alternating with MRI every 6 months)
- Consider transvaginal ultrasound plus CA-125 blood test for ovarian surveillance
- Discussion of risk-reducing salpingo-oophorectomy timing (typically age 35-40 for BRCA1, 40-45 for BRCA2)
For BRCA-Positive Men:
- Annual clinical breast exam starting age 35
- Prostate cancer screening (PSA + digital rectal exam) starting age 40
- Consider annual pancreatic cancer surveillance if family history warrants
- Genetic counseling about reproductive implications
Meet with a specialized breast surgeon to discuss risk-reduction mastectomy. While this is a highly personal decision, prophylactic bilateral mastectomy reduces breast cancer risk by approximately 90%. Many women choose reconstruction performed simultaneously.
Days 61-90 – Long-Term Strategy Development:
Evaluate chemoprevention (medication-based risk reduction) options:
Tamoxifen or Raloxifene: Selective estrogen receptor modulators can reduce breast cancer risk by 30-50% in high-risk women. However, benefits appear stronger for BRCA2 carriers than BRCA1 carriers. Discuss potential side effects (blood clots, endometrial changes) with your oncologist.
Oral Contraceptives: Birth control pills reduce ovarian cancer risk by 42% in BRCA carriers according to meta-analysis data. The effect on breast cancer risk remains controversial, with some studies showing slight elevation. Risk-benefit analysis depends on your individual mutation type and family history.
2026 Update: New PARP inhibitor trials are investigating prophylactic use in high-risk BRCA carriers. Clinical trials are available through ClinicalTrials.gov.
Consider joining BRCA support communities like FORCE (Facing Our Risk of Cancer Empowered). Connecting with others navigating similar decisions provides emotional support and practical insights that complement medical advice.
If You’re BRCA Negative: Ongoing Monitoring
A negative BRCA result requires different follow-up depending on whether you received a true negative or uninformative negative result.
True Negative Pathway:
- Follow standard screening recommendations for the general population
- Annual mammograms starting age 40 (or earlier based on other risk factors)
- No need for breast MRI unless other high-risk features exist
- Family members may still benefit from testing if multiple relatives have cancer
Uninformative Negative Pathway:
- Enhanced screening may still apply if strong family history persists
- Consider expanded panel testing (50+ genes including PALB2, CDH1, TP53, CHEK2, ATM)
- Encourage affected family members to test first for more informative results
- Discuss whether clinical features warrant MRI screening despite negative BRCA
Dr. Michael Roberts, oncologist at Mayo Clinic, emphasizes: “A negative BRCA test doesn’t mean zero cancer risk. We still base screening recommendations on your complete risk profile, which includes family history, personal history, breast density, and other genetic factors.”
Approximately 25% of hereditary breast cancer cases involve genes other than BRCA1/BRCA2. Expanded panel testing captures mutations in PALB2 (14% of hereditary cases), CHEK2 (9%), and ATM (7%). Testing costs have decreased to $250-$500 for comprehensive panels in 2026.
If You Have VUS: The Waiting Strategy
Managing a VUS result requires patience and periodic reassessment. Current clinical guidelines recommend treating VUS as a negative result for medical decision-making purposes.
Immediate Actions:
- Request a copy of your laboratory report including the specific variant detected
- Ask your genetic counselor how to check for reclassification updates
- Document the testing laboratory’s contact information for future inquiries
- Base screening decisions on personal and family cancer history, NOT on the VUS
Ongoing Monitoring:
- Contact the laboratory every 2-3 years requesting variant reclassification status
- Many labs provide automatic updates when variants get reclassified
- Consider cascade testing for relatives—their results may help resolve your VUS
- New family cancer diagnoses warrant genetic counselor re-consultation
The ClinVar database maintained by the National Institutes of Health tracks variant classifications. You can search your specific variant (using the nomenclature from your report) to see current classification status and supporting evidence.
Important: Don’t make surgical decisions based on VUS results. Multiple case studies document patients who underwent preventive mastectomies for VUS results that were later reclassified as benign. Wait for definitive reclassification to pathogenic before considering aggressive interventions.
Just as interpreting mammogram BIRADS results requires understanding different risk categories, BRCA results demand personalized medical management based on your complete clinical picture.
Family Impact and Financial Considerations
Who Needs to Know Your Results?
Genetic information creates unique ethical dilemmas because your BRCA status directly impacts your blood relatives’ health risks. The “50% inheritance rule” means each first-degree relative has a coin-flip chance of carrying your mutation.
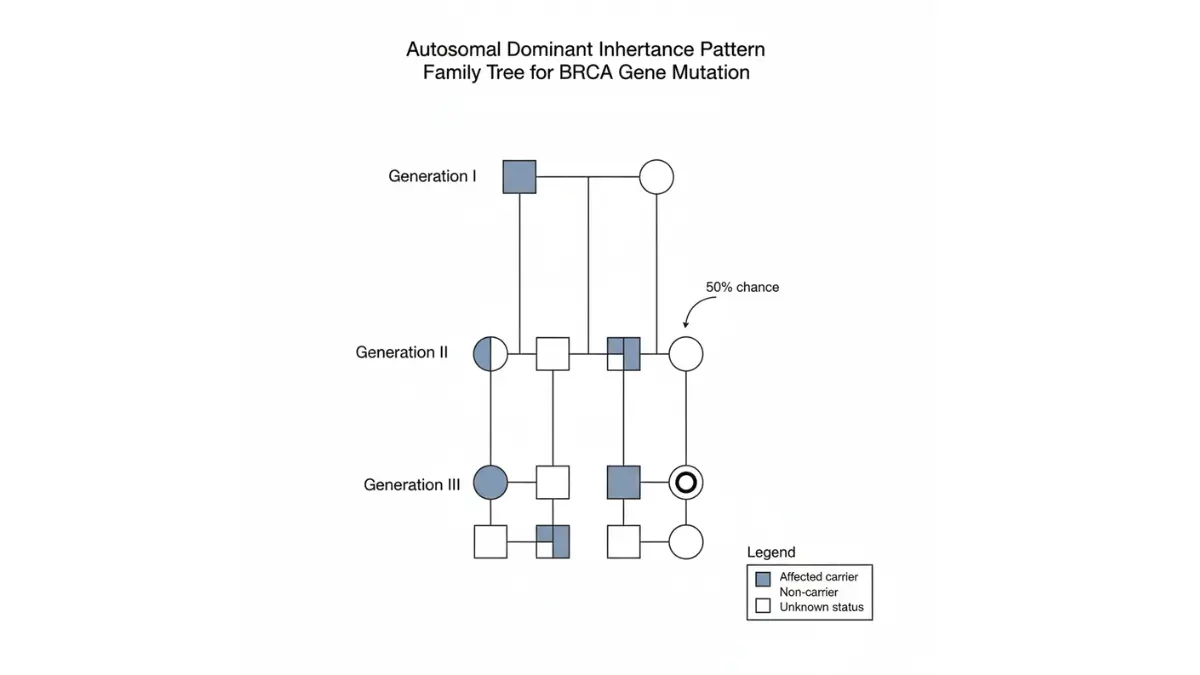
First-Degree Relatives (Share 50% of genes):
- Parents (identifies which side of family carries mutation)
- Full siblings (both brothers and sisters—BRCA affects men too)
- Children (can wait until adulthood unless cancer diagnosis requires earlier testing)
Second-Degree Relatives (Share 25% of genes):
- Grandparents (may be elderly but information helps identify risk lineage)
- Aunts and uncles (especially important if they have children)
- Half-siblings and grandchildren
Third-Degree Relatives (Share 12.5% of genes):
- First cousins (particularly relevant if multiple affected family members)
- Great-grandparents (usually for pedigree analysis)
How to Have “The Conversation”:
Script for positive results: “I recently had genetic testing for hereditary cancer risk and learned I carry a BRCA mutation. This means there’s a 50% chance you might carry it too. I wanted to share this information so you can discuss genetic testing with your doctor. I can provide my test report and genetic counselor’s contact information if you’d like.”
You have no legal obligation to disclose genetic information to relatives, but ethical guidelines from the American Society of Human Genetics encourage disclosure when: (1) the risk to relatives is significant, (2) the disease is preventable or treatable, and (3) the information could meaningfully alter medical management.
Privacy Protections and Limitations:
The Genetic Information Nondiscrimination Act (GINA) prohibits health insurance companies and employers from discriminating based on genetic information. However, GINA does NOT protect against discrimination by:
- Life insurance companies (can deny coverage or charge higher premiums)
- Disability insurance providers
- Long-term care insurance companies
- Military personnel (different regulations apply)
Fourteen states have enacted additional protections beyond GINA. California, Florida, and Massachusetts specifically prohibit genetic discrimination in life insurance. The National Human Genome Research Institute maintains updated state-by-state protection summaries.
2026 Testing Costs Breakdown
BRCA Testing Prices:
Comprehensive BRCA1/BRCA2 sequencing: $300-$3,500 depending on laboratory and insurance coverage. Major commercial laboratories (Myriad Genetics, Invitae, GeneDx) charge $1,500-$2,500 for out-of-pocket costs.
Expanded hereditary cancer panel (30-80 genes including BRCA1/BRCA2, PALB2, CDH1, TP53, PTEN, STK11): $1,500-$5,000. Most comprehensive option but increases VUS likelihood.
Single-site familial variant testing: $250-$475. When a family mutation is already identified, testing relatives costs significantly less because laboratories only check for that specific variant.
Insurance Coverage Criteria:
Approximately 90% of genetic tests are covered when patients meet National Comprehensive Cancer Network testing criteria. Insurance typically covers testing if you have:
- Personal history of breast cancer diagnosed age ≤50
- Triple-negative breast cancer diagnosed age ≤60
- Two breast cancer primaries (at any age)
- Male breast cancer
- Ovarian, fallopian tube, or primary peritoneal cancer
- Pancreatic cancer with Ashkenazi Jewish ancestry
- Metastatic prostate cancer
- Known BRCA mutation in a family member
- Three or more close relatives with breast, ovarian, pancreatic, or prostate cancer
Pre-Authorization and Appeal Tips:
Submit genetic counseling notes with testing authorization requests—documentation of medical necessity increases approval rates by 40%. If initially denied, file a formal appeal citing NCCN guidelines and family history specifics. Patient advocacy organizations like FORCE offer free appeal letter templates.
Financial Assistance Programs:
Myriad Genetics MyRisk Financial Assistance Program caps out-of-pocket costs at $250 for patients with annual household income below $125,000. Invitae offers payment plans at $50-$100 monthly for uninsured patients.
Cancer support organizations including the American Cancer Society and Susan G. Komen Foundation provide grants covering genetic testing costs for financially qualified individuals.
Managing healthcare costs and cancer risk parallels other preventive health strategies, similar to using a Weight Loss Calculator to plan sustainable health improvements.
Real Stories and Expert Insights
Patient Story 1: BRCA1 Positive – The Preventive Mastectomy Decision
Jennifer Thompson, 42, financial analyst from Seattle, discovered her BRCA1 mutation after her sister’s ovarian cancer diagnosis at age 38. “The statistics terrified me—72% breast cancer risk felt like a ticking time bomb,” she recalls. After nine months of consultations, Thompson chose bilateral prophylactic mastectomy with immediate DIEP flap reconstruction.
“The surgery was challenging, but I reduced my breast cancer risk to less than 5%. I still do annual MRI screening because you can’t remove every single breast cell, but my anxiety decreased dramatically. My 19-year-old daughter tested negative for my specific mutation, which gave our family enormous relief.”
Thompson emphasizes the importance of connecting with other BRCA carriers: “Online support groups showed me photos, shared recovery timelines, and honestly discussed the emotional complexity. Medical journals can’t prepare you for how it feels to lose your breasts preventively.”
Patient Story 2: VUS Result – Living with Uncertainty
Marcus Johnson, 51, high school teacher from Atlanta, received VUS results when his mother’s aggressive breast cancer prompted family testing. “The genetic counselor explained VUS means ‘we don’t know yet,’ which was frustrating after paying $2,800 for comprehensive testing,” he shares.
Johnson’s VUS involved a BRCA2 variant with conflicting evidence in scientific literature. His two sisters also tested, and both carried the same variant. “When all three siblings had the same change, but Mom’s cancer tissue showed a completely different mutation, geneticists suspected our variant was benign.”
After four years, the laboratory reclassified Johnson’s variant to “likely benign” based on accumulated population data. “Those four years of uncertainty taught me that genetic testing isn’t always black and white. I followed standard screening protocols and stayed connected to my genetic counselor for updates.”
Patient Story 3: True Negative – Relief and Continued Vigilance
Angela Rodriguez, 35, nurse practitioner from Miami, tested negative for her father’s known BRCA2 mutation. “Learning I didn’t inherit Dad’s mutation felt like winning the lottery,” she describes. Rodriguez’s father was diagnosed with aggressive prostate cancer at 54 and carries a BRCA2 mutation linked to 40% lifetime prostate cancer risk.
“My true negative result meant my cancer risk returned to general population levels—about 12% lifetime breast cancer risk instead of 60-70%. I still do annual mammograms starting at 40 because Mom’s side has sporadic breast cancers, but I don’t need the intensive screening my aunt with the BRCA2 mutation requires.”
Rodriguez emphasizes the importance of testing affected family members first: “If Dad hadn’t been tested initially, my negative result would have been uninformative. Knowing his specific mutation made my negative result definitive.”
International Expert Perspectives
Dr. Sarah Mitchell, Genetic Counselor, MD Anderson Cancer Center (Houston, USA): “The most important message for BRCA-positive patients is that a mutation doesn’t equal a cancer sentence. We have powerful prevention tools—enhanced screening detects cancers early when they’re most treatable, and risk-reduction surgeries can decrease cancer probability by 90%. Every patient’s decision is personal, and we support whatever choice aligns with their values.”
Dr. James Chen, Clinical Oncologist, Royal Marsden Hospital (London, UK): “BRCA testing has revolutionized cancer prevention, but it’s created new challenges around VUS interpretation. Our international consortium works to share variant data across borders, accelerating reclassification. Patients should understand that VUS rates vary by ethnicity—individuals of non-European ancestry have higher VUS rates because variant databases contain fewer reference samples from diverse populations.”
Dr. Emily Watson, Cancer Geneticist, Peter MacCallum Cancer Centre (Melbourne, Australia): “Risk-reducing medications represent an underutilized prevention strategy. Many BRCA carriers focus exclusively on surgery, but tamoxifen reduces breast cancer risk by 30-50% in BRCA2 carriers with minimal side effects in most women. We’re also excited about emerging PARP inhibitor trials investigating prophylactic use.”
2026 Research Updates
New PARP Inhibitor Approvals: The FDA expanded olaparib (Lynparza) approval in February 2026 for preventive use in BRCA1/BRCA2 carriers with prior cancer history. Clinical trials are investigating whether PARP inhibitors can prevent first cancers in high-risk mutation carriers.
Improved VUS Reclassification Algorithms: Artificial intelligence platforms analyzing over 8 million genetic variants have reduced VUS reclassification timelines from 5 years to 18-24 months on average. The ENIGMA Consortium coordinates international BRCA variant classification using standardized evidence frameworks.
Expanded Testing Guidelines: The US Preventive Services Task Force updated 2026 recommendations to include BRCA testing for all women with breast cancer diagnosed under age 55 (previously age 50), capturing an additional 40,000 women annually who qualify for genetic testing.
Understanding genetic testing parallels interpreting other diagnostic results like thyroid levels where test values require clinical context and expert interpretation.
Frequently Asked Questions About BRCA Results
1. How long do BRCA test results take?
Most laboratories return results within 2-4 weeks; expedited processing available for active cancer patients within 5-7 days.
2. Can BRCA results change over time?
Your genetic sequence doesn’t change, but VUS classifications can get updated as scientific evidence accumulates over years.
3. Should men get BRCA testing?
Yes—men with BRCA2 mutations have 8% breast cancer risk and 25-50% prostate cancer risk, warranting early screening.
4. What cancers besides breast does BRCA affect?
Ovarian, pancreatic, prostate, melanoma (BRCA2 only), and gastric cancers all show increased incidence in BRCA carriers.
5. Can I have children if I’m BRCA positive?
Yes—BRCA doesn’t affect fertility; preimplantation genetic diagnosis can prevent transmission to offspring if desired through IVF.
6. Do I need surgery if I test positive?
No—surgery is optional; enhanced screening plus chemoprevention are alternatives though less effective than prophylactic surgery for risk reduction.
7. Will my insurance cover BRCA-related screening?
Yes—most insurers cover annual MRIs and alternating mammograms for proven mutation carriers per NCCN guidelines.
8. Can lifestyle changes reduce BRCA cancer risk?
Modest impact—maintaining healthy weight, limiting alcohol, breastfeeding (for women), and regular exercise reduce risk by 15-25%.
9. Should I tell my employer about BRCA results?
No legal requirement; GINA protects against employment discrimination based on genetic information in most workplace contexts.
10. How accurate are BRCA tests?
Highly accurate—99%+ sensitivity and specificity when performed at accredited laboratories; false positives/negatives are extremely rare.
11. Where can I find BRCA support groups?
FORCE, Bright Pink, and hospital-based programs offer in-person and virtual support for mutation carriers nationwide.
Final Thoughts: Understanding your BRCA results empowers you to make informed decisions about cancer screening, prevention, and treatment. Whether you received a positive, negative, or VUS result, working closely with experienced genetic counselors and specialized physicians ensures you receive personalized care based on your unique genetic profile and family history. For additional health resources and risk assessment tools, visit our Health Tips section or explore our comprehensive Symptom Checker for related health concerns.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











