On This Page – Quick Medical Summary
Marcus, a 42-year-old attorney from Boston, stared at his genetic test results for nearly an hour, his hands trembling. The medical terminology felt like decoding a foreign language, and the phrase “variant of uncertain significance” sent his anxiety spiraling.
What do genetic test results mean?
Your genetic test results reveal whether your DNA contains specific changes (mutations or variants) that may increase your risk for certain diseases, confirm a diagnosis, or indicate carrier status for hereditary conditions. In 2026, clinical genetic testing achieves 99.0-99.9% accuracy for most conditions, but understanding what those numbers actually mean for your health requires careful interpretation.
This comprehensive guide translates complex genetic testing terminology into actionable insights you can use today. Whether you received positive, negative, or uncertain results, you’ll learn exactly what your specific outcome means, what steps to take next, and how to navigate the emotional and practical challenges that come with genetic information.
By the end of this article, you’ll understand the critical differences between test types, know when to seek genetic counseling, and have a clear action plan based on your results.
Decoding Your Results – The Core Guide
Types of Genetic Test Results (And What Each Means)
Understanding genetic test results requires knowing which category your outcome falls into and what that means for your health trajectory.
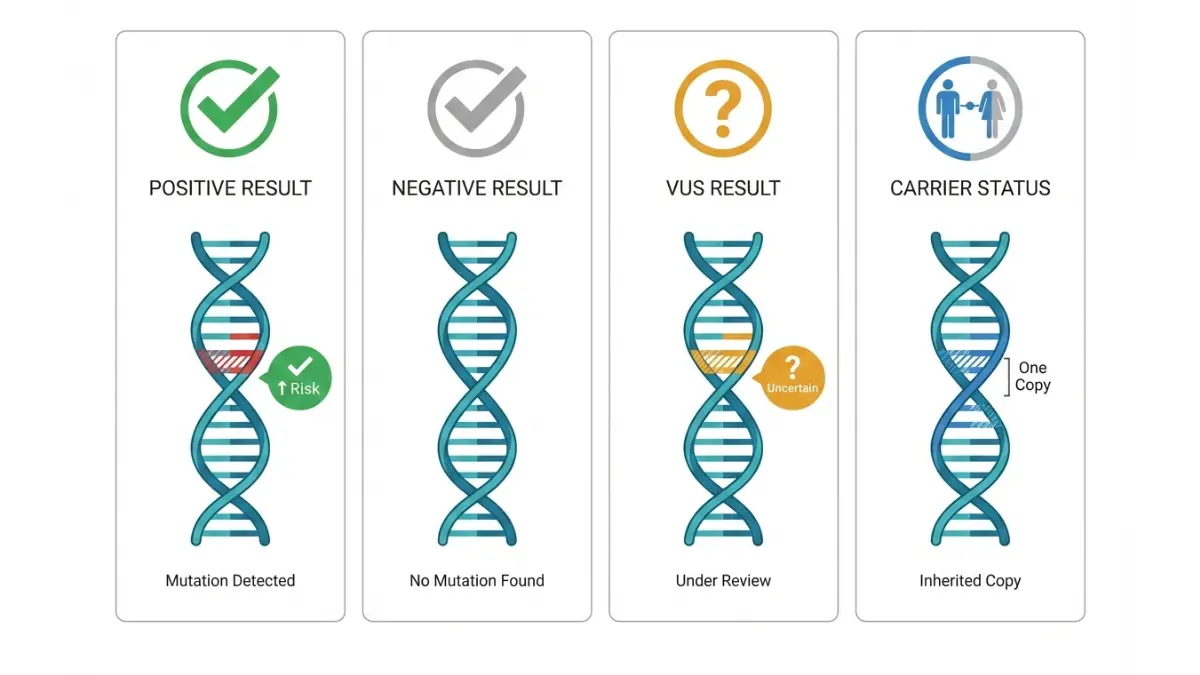
Positive Results: What They Really Tell You
A positive genetic test result means laboratory analysis detected a specific gene mutation known to increase disease risk or confirm a diagnosis. However, positive doesn’t mean you have or will definitely develop the condition—it indicates elevated probability compared to the general population.
For cancer risk genes like BRCA1/BRCA2, a positive result means lifetime breast cancer risk increases to 45-87% (compared to the general population’s 12-13% baseline). The National Cancer Institute provides detailed risk breakdowns by specific mutations.
Key distinctions in positive results:
- Diagnostic positive: Confirms you have a genetic condition causing current symptoms
- Predictive positive: Shows increased future disease risk before symptoms appear
- Carrier positive: You carry one copy of a recessive gene mutation (typically doesn’t affect your health but has reproductive implications)
Clinical genetic testing in 2026 achieves 99.0-99.9% accuracy for single-gene disorders, meaning false positive rates remain below 0.5% in CLIA-certified laboratories.
Negative Results: The Full Picture
A negative genetic test result indicates the laboratory found no known disease-causing mutations in the genes analyzed. This outcome has two possible interpretations depending on your family history.
True negative: In families where a specific mutation was already identified in a relative, your negative result means you didn’t inherit that mutation and have average population risk for that condition.
Uninformative negative: When multiple family members have a disease but all test negative, genetic testing hasn’t identified the cause. This occurs in 15-30% of families with strong disease history, often because current testing technology can’t detect all mutation types or the causative gene hasn’t been discovered yet.
False negative rates vary by test type but typically range from 1-3% according to CDC genomics data. Technology limitations mean some mutations may be missed, particularly in non-coding DNA regions.
VUS Results: The Gray Zone Explained
A Variant of Uncertain Significance (VUS) occurs when genetic testing detects a DNA change, but insufficient scientific evidence exists to classify it as harmful or benign. Think of VUS results as “needs more research”—not positive, not negative, but undetermined.
2026 VUS landscape:
- Approximately 30-40% of people undergoing panel testing receive at least one VUS
- Labs reclassify 18-22% of VUS results annually as more research accumulates
- Less-studied populations (non-European ancestry) have higher VUS rates due to limited research representation
| VUS Status | Clinical Action | Recheck Timeline |
|---|---|---|
| Initial VUS | Treat as negative | Annually |
| 2+ years unchanged | Likely benign | Every 2 years |
| Family members with same VUS + disease | May guide decisions | Every 6 months |
Most VUS results eventually reclassify as benign (harmless natural variations). Using our Genetic Risk Assessment Tool can help contextualize your baseline risk while awaiting VUS resolution.
Carrier Results: Family Planning Implications
Carrier screening reveals you have one copy of a gene mutation for a recessive condition like cystic fibrosis or sickle cell disease. Being a carrier typically doesn’t affect your personal health—you need two copies (one from each parent) for disease manifestation.
Reproductive considerations:
- If your partner is also a carrier for the same condition, each pregnancy has a 25% chance of an affected child
- Carrier screening costs $0-$250 with insurance, recommended before conception
- Options include prenatal testing, preimplantation genetic diagnosis (PGD), or using donor gametes
The American College of Medical Genetics recommends carrier screening for 113 conditions as of 2026, expanded from 23 conditions in 2020.
Test Types & Interpretation Differences
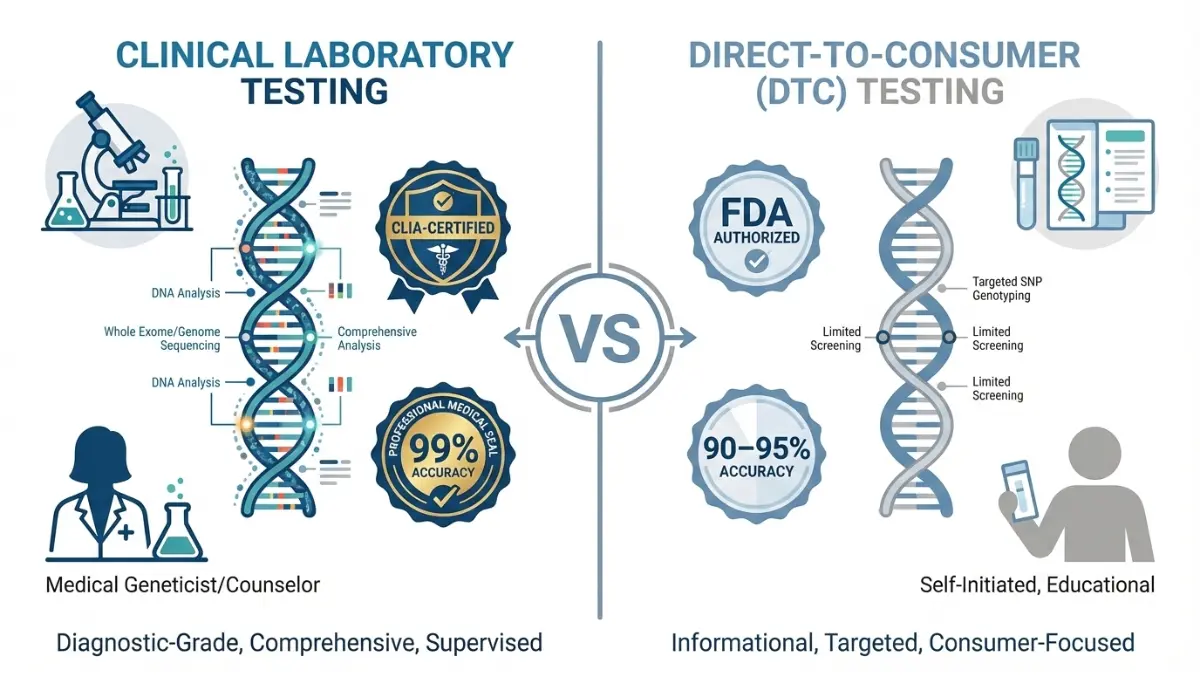
Clinical vs. At-Home Tests: Critical Differences
The genetic testing you receive—and how accurately it predicts your health risks—depends heavily on whether you used clinical laboratory testing or direct-to-consumer (DTC) at-home kits.
Clinical Laboratory Tests (CLIA-Certified)
Clinical genetic testing through healthcare providers uses CLIA-certified laboratories meeting strict federal accuracy standards. These tests analyze DNA with medical-grade precision and include genetic counselor interpretation.
Clinical test characteristics:
- Accuracy: 99.0-99.9% for single-gene and panel tests
- Cost: $0-$500 with insurance (pre-authorization required); $500-$5,000 without coverage
- Turnaround: 2-6 weeks for panels; 8-12 weeks for whole genome sequencing
- Major labs: Invitae, GeneDx, Ambry Genetics, Quest Diagnostics
Insurance typically covers clinical genetic testing when you meet medical necessity criteria—personal or family history suggesting hereditary conditions, or when results will guide treatment decisions. Similar to how diagnostic imaging results require expert interpretation, genetic test results benefit from professional genetic counseling.
Direct-to-Consumer Tests
At-home DNA tests like 23andMe Health, AncestryDNA Health, and Color Genomics provide health risk information directly to consumers without physician orders.
DTC test limitations:
- Accuracy: 90-95% for analyzed variants (they test far fewer genetic changes)
- Scope: Screen limited marker sets rather than comprehensive gene sequencing
- Regulatory status: FDA-authorized for specific reports only (BRCA variants, carrier screening)
- Clinical use: Results should NOT guide medical decisions without clinical confirmation
Critical caveat: A negative DTC test doesn’t rule out genetic conditions because these services analyze only common variants, potentially missing rare mutations. If DTC testing suggests increased risk, confirm with clinical testing before making medical decisions.
Pharmacogenomics Testing
Pharmacogenomic testing analyzes how your genetics affect medication metabolism and response—a rapidly growing field as precision medicine advances.
2026 pharmacogenomics expansion:
- Medicare now covers testing for warfarin, clopidogrel, and several chemotherapy drugs
- CYP450 gene testing predicts response to 30+ medications including antidepressants, pain medications, and blood thinners
- Cost: $200-$500; increasingly covered by insurance when prescribing specific drugs
For example, CYP2D6 testing reveals whether you’re a poor metabolizer of codeine (making it ineffective for pain) or an ultra-rapid metabolizer (increasing overdose risk). This information can prevent adverse reactions and improve treatment efficacy.
Test Type Comparison:
| Test Type | Accuracy | Cost Range | Turnaround | Best For |
|---|---|---|---|---|
| Clinical panel | 99.0-99.9% | $0-$2,500 | 2-6 weeks | Medical diagnosis, cancer risk |
| Whole genome | 99.5% | $1,500-$5,000 | 8-12 weeks | Complex/undiagnosed conditions |
| DTC health | 90-95% | $99-$299 | 3-8 weeks | Ancestry + basic health screening |
| Pharmacogenomic | 98-99% | $200-$500 | 1-3 weeks | Medication optimization |
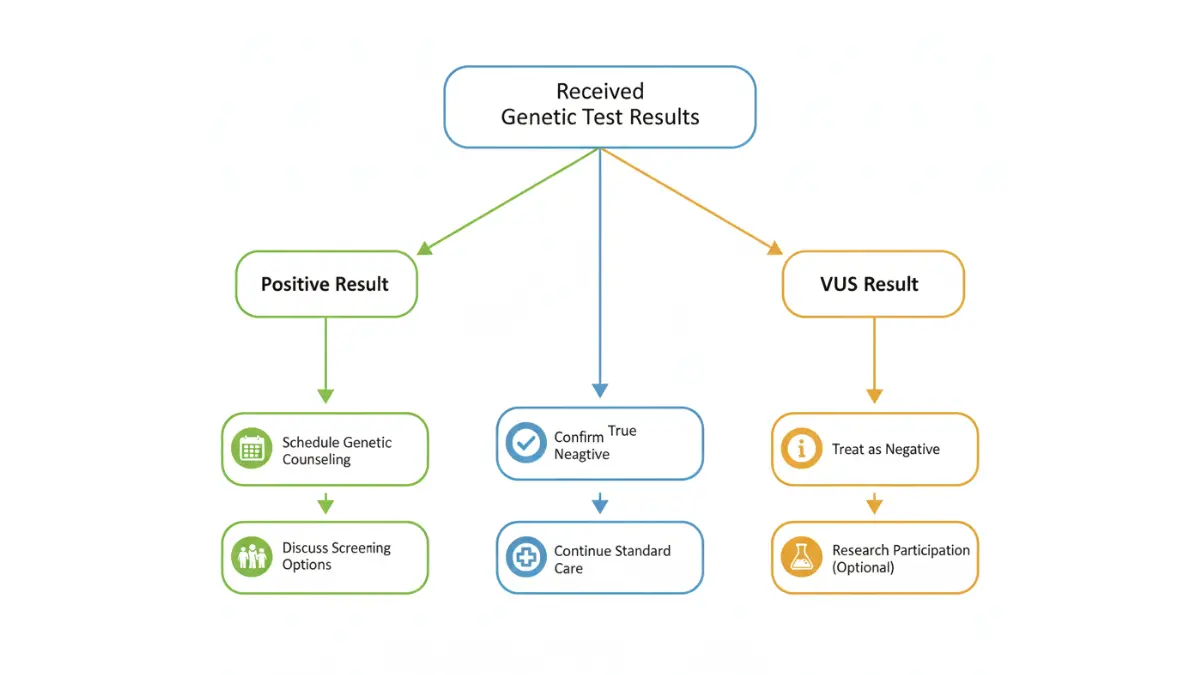
What to Do After Getting Results
Your Action Plan: Next Steps Based on Results
Receiving genetic test results—especially unexpected ones—triggers a cascade of questions: What do I do first? Who needs to know? How does this change my medical care?
First 24 Hours: Immediate Actions
Don’t panic checklist:
- Read results carefully: Note whether you received positive, negative, VUS, or carrier results
- Document details: Screenshot or photograph result pages showing specific genes tested and mutations found
- Schedule genetic counseling: Book within 1-2 weeks for result interpretation (don’t wait months)
- Avoid Dr. Google spiraling: Online statistics often reflect outdated data or worst-case scenarios
Finding genetic counselors:
The National Society of Genetic Counselors directory helps locate board-certified counselors by specialty and location. Consultation costs range from $150-$500 per session, with most insurance plans covering genetic counseling when medically indicated.
Virtual genetic counseling expanded significantly post-2020, making access easier regardless of geographic location. Many academic medical centers now offer telemedicine genetic counseling covered by insurance.
Understanding Risk Percentages
Genetic test results often report risk as percentages that can be deeply confusing and anxiety-provoking without proper context.
Relative vs. absolute risk clarity:
- “10% increased risk”: Your risk is 10% higher than baseline (if population risk is 10%, yours is 11%)
- “10x risk” or “10-fold risk”: Your risk is ten times higher than baseline (if population risk is 10%, yours is 100% or near-certain)
- Lifetime risk: Probability of developing condition by age 80
- 10-year risk: Probability of developing condition in next decade

For BRCA1-positive women, lifetime breast cancer risk is 45-87% (compared to general population’s 12-13%), representing a 3.5-7x increased relative risk. However, this also means 13-55% of BRCA1-positive women never develop breast cancer despite the mutation.
Understanding these distinctions reduces anxiety and helps make informed screening and prevention decisions. Just as blood test result interpretation requires understanding reference ranges, genetic risk interpretation requires understanding how probability translates to personal health decisions.
Family Communication Protocol
Who needs to know about your results:
Positive results or VUS findings have implications for biological relatives who share your DNA—specifically first-degree relatives (parents, siblings, children) who have a 50% chance of inheriting the same variant.
Communication approach:
- Share results with first-degree relatives within 2-4 weeks
- Provide them your genetic counselor’s contact information
- Offer to share your written test report (redact personal medical details if preferred)
- Discuss cascade testing—where relatives get targeted testing for your specific mutation
Family letter template: Most genetic testing labs provide family communication letters explaining your results and recommending relatives consider testing. These letters use medically accurate but accessible language appropriate for sharing.
Second-degree relatives (grandparents, aunts/uncles, nieces/nephews, half-siblings) may also benefit from knowing, depending on the specific condition and inheritance pattern.
Insurance & Privacy Protections
GINA Law 2026 protections:
The Genetic Information Nondiscrimination Act (GINA) prohibits health insurance companies and employers from discriminating based on genetic information.
GINA covers:
- Health insurance coverage and premiums (cannot be denied or increased)
- Employment decisions (hiring, firing, promotions, job assignments)
GINA does NOT cover:
- Life insurance, disability insurance, or long-term care insurance
- Military members
- Companies with fewer than 15 employees
Practical implications: Consider purchasing life and disability insurance BEFORE genetic testing if you have family history suggesting high-risk mutations. While ethically questionable, insurers can legally request genetic testing results when underwriting these policies.
Some individuals choose to pay out-of-pocket for genetic testing (rather than using insurance) to avoid potential documentation in medical records, though GINA protections have been robust since enactment.
Accuracy, Limitations & When to Retest
Test Accuracy & Limitations You Should Know
How Accurate Are Genetic Tests in 2026?
Genetic testing accuracy varies significantly by test type, laboratory quality, and specific genes analyzed.
Current accuracy benchmarks:
- CLIA-certified clinical labs: 99.0-99.9% for single-gene and panel tests
- Whole exome sequencing: 97-99% (lower due to complexity of analyzing 20,000+ genes)
- Direct-to-consumer tests: 90-95% for variants they analyze (but test fewer variants)
- Pharmacogenomic testing: 98-99% for drug metabolism genes
False positive rates remain below 0.5% in clinical testing, while false negative rates range from 1-3% depending on mutation type. Complex rearrangements and large deletions/duplications are harder to detect than single-letter DNA changes.
Accuracy by ancestry:
Testing accuracy is highest for individuals of European descent because most genetic research historically focused on this population. People of African, Asian, Hispanic, or Indigenous ancestry may have higher VUS rates—not due to actual higher mutation frequencies, but because scientific databases contain fewer reference samples from these populations.
The National Institutes of Health All of Us Research Program aims to address these disparities by enrolling 1 million diverse participants, improving interpretation accuracy across all ancestries.
What Tests Can’t Tell You
Even the most accurate genetic testing has inherent limitations that everyone should understand before testing.
Genetic tests cannot:
- Predict exactly when symptoms will start (age of onset remains uncertain)
- Determine how severe symptoms will be (disease penetrance and expressivity vary)
- Account for environmental factors (diet, exercise, smoking, exposures significantly modify genetic risk)
- Detect all possible mutations (some mutation types evade current technology)
- Provide 100% certainty (even high-penetrance mutations don’t guarantee disease)
Polygenic risk scores (2026 emerging tool): Rather than testing single high-risk genes, polygenic scores analyze hundreds to thousands of common genetic variants to estimate disease risk. While growing in research settings, these scores aren’t yet standard clinical practice for most conditions.
When to Consider Retesting
Genetic testing technology advances rapidly—what couldn’t be detected in 2020 may be identifiable in 2026.
Retest triggers:
- VUS reclassification: Check annually if you received VUS results; 18-22% reclassify each year
- Technology improvements: If you tested before 2020, newer sequencing methods may detect mutations missed by older techniques
- New symptoms: If you develop symptoms consistent with hereditary conditions despite previous negative results
- Family member diagnosis: If a relative receives a genetic diagnosis, you may benefit from targeted testing for their specific mutation
- Expanding gene panels: Panels now test 30-100+ genes compared to 5-20 genes in older panels
Retesting costs: $200-$1,500 depending on test scope and whether insurance covers repeat testing. Medicare generally covers retesting every 5 years or when clinically indicated.
Similar to how you might review other diagnostic test results periodically when managing chronic conditions, genetic test results warrant periodic reassessment as science advances.
11 Most-Asked Questions About Genetic Test Results
1. How long do genetic test results take?
Clinical laboratory tests typically return results in 2-6 weeks for panel tests and 8-12 weeks for whole genome sequencing. Direct-to-consumer tests usually take 3-8 weeks from sample receipt.
Turnaround time depends on test complexity—single-gene tests are fastest, while comprehensive genomic analysis takes longer. Rush processing may be available for urgent medical decisions but increases costs by $500-$1,000.
2. Can genetic test results be wrong?
Yes, though rare in CLIA-certified clinical laboratories. False positives occur in <0.5% of clinical tests, while false negatives occur in 1-3% according to 2026 accuracy data from the Centers for Disease Control.
Errors typically result from technical limitations (some mutation types are harder to detect) rather than laboratory mistakes. Confirming unexpected results through repeat testing or alternative methods is standard practice.
3. Should I tell my family about my results?
First-degree relatives (parents, siblings, children) should definitely know if you test positive for a hereditary condition or have a VUS result in a disease-associated gene. They have a 50% chance of inheriting the same variant.
Share information within 2-4 weeks of receiving results. Provide your genetic counselor’s contact information so relatives can discuss their own testing options.
Most genetic testing laboratories provide family communication letters to facilitate these conversations.
4. How much does genetic counseling cost?
Genetic counseling sessions cost $150-$500 per appointment, with initial consultations typically lasting 60-90 minutes. Most insurance plans cover genetic counseling when medically indicated (personal or family history of genetic conditions).
Medicare covers counseling when ordered by a physician for specific indications. Payment assistance programs exist through the National Society of Genetic Counselors for those without coverage.
5. What does a VUS result mean for me?
A Variant of Uncertain Significance (VUS) means genetic testing found a DNA change but insufficient evidence exists to classify it as harmful or benign. Treat VUS results as negative until reclassified.
Approximately 18-22% of VUS results get reclassified annually as research progresses. Check for updates yearly through your testing laboratory or genetic counselor. Most VUS results eventually classify as benign.
6. Can I trust at-home DNA test results?
For ancestry information: yes. For medical decisions: no—always confirm health findings with clinical testing. Direct-to-consumer tests like 23andMe analyze limited genetic variants (hundreds) compared to clinical tests (analyzing entire genes or genomes).
DTC test accuracy runs 90-95% for variants they analyze, but they miss rare mutations that clinical testing would detect. The FDA authorizes specific DTC health reports but recommends clinical confirmation before medical actions.
7. Do positive results guarantee I’ll get the disease?
No—positive results indicate increased risk, not certainty. Even high-penetrance mutations like BRCA1 (conferring 45-87% lifetime breast cancer risk) mean 13-55% of carriers never develop breast cancer.
Penetrance varies by gene and mutation. Many factors beyond genetics—including lifestyle, environment, and random chance—influence whether genetic predisposition manifests as disease. Using tools like our Symptom Checker can help monitor for early signs if you have increased genetic risk.
8. How often should I retest?
For VUS results: check annually for reclassification updates. For technology improvements: every 5 years if your initial test was older or used limited panels.
Retest if you develop new symptoms despite previous negative results, or if a family member receives a genetic diagnosis suggesting you may carry mutations not detected by your previous test. Insurance coverage for retesting varies—Medicare typically covers it every 5 years or when clinically indicated.
9. Will insurance cover genetic testing?
Often yes for high-risk patients meeting medical necessity criteria—personal or family history suggesting hereditary conditions, or when results guide treatment decisions. Insurance requires pre-authorization and documentation from your healthcare provider.
Out-of-pocket costs range from $0-$500 with insurance coverage, $500-$5,000 without coverage. Payment plans and financial assistance programs exist through most testing laboratories for those facing cost barriers.
10. What’s the difference between diagnostic and predictive testing?
Diagnostic testing confirms the genetic cause of symptoms you’re currently experiencing—identifying which mutation caused your diagnosed condition.
Predictive testing estimates future disease risk before symptoms appear—determining whether you inherited family mutations that may cause disease later. Predictive testing requires careful genetic counseling because results have profound psychological and medical implications.
Both test types use identical laboratory methods; the difference lies in clinical context and timing relative to symptom onset.
11. Can genetic results affect my life insurance?
Yes—while the Genetic Information Nondiscrimination Act (GINA) protects health insurance and employment, it does NOT cover life insurance, disability insurance, or long-term care insurance.
Insurers can legally request genetic testing results during underwriting for these policies and may deny coverage or charge higher premiums based on positive results. Consider purchasing these insurance types BEFORE genetic testing if you have family history suggesting high-risk mutations.
Some states have additional protections beyond GINA—check your state’s insurance regulations or consult an insurance attorney for specific guidance.
Final Thoughts
Genetic test results provide powerful information about your health risks and can guide medical decisions, but they represent just one piece of your overall health picture. Whether you received positive, negative, or uncertain results, the most important next step is connecting with a qualified genetic counselor who can interpret findings in the context of your personal and family medical history.
Remember that genetic risk is not genetic destiny—lifestyle factors, screening, and preventive interventions significantly modify outcomes even for high-risk individuals. Stay informed about evolving research, check periodically for VUS reclassifications, and maintain open communication with healthcare providers who can help you translate genetic information into actionable health strategies.
For additional support understanding your results, explore our Health Tips section featuring evidence-based guidance on managing genetic health risks and optimizing wellness across all life stages.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Molecular Biology Research Certification (2012) Experience: 14 years | Location: Singapore Education: BSc Biochemistry, National University of Singapore (2008); PhD Molecular Biology, Duke-NUS Medical School (2013);…

Board Certifications: Medical Oncology (1999); Hematology (2000) Experience: 26 years | Location: Milan, Italy Education: MD, University of Milan (1996); Oncology Residency, European Institute of Oncology (1999); Fellowship…

Board Certifications: European Registered Toxicologist (2008); Clinical Pharmacology Certification (2010) Experience: 18 years | Location: Madrid, Spain Education: BSc Pharmacy, Complutense University of Madrid (2004); PhD Pharmacology, University…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.