On This Page – Quick Medical Summary
What Is a Stool Report? (Quick 2026 Overview)
Jasper, a 42-year-old accountant from Chicago, stared at his lab results with complete confusion. Numbers, abbreviations, medical terms—his stool report might as well have been written in another language. Within hours, his anxiety spiraled into late-night internet searches filled with worst-case scenarios.
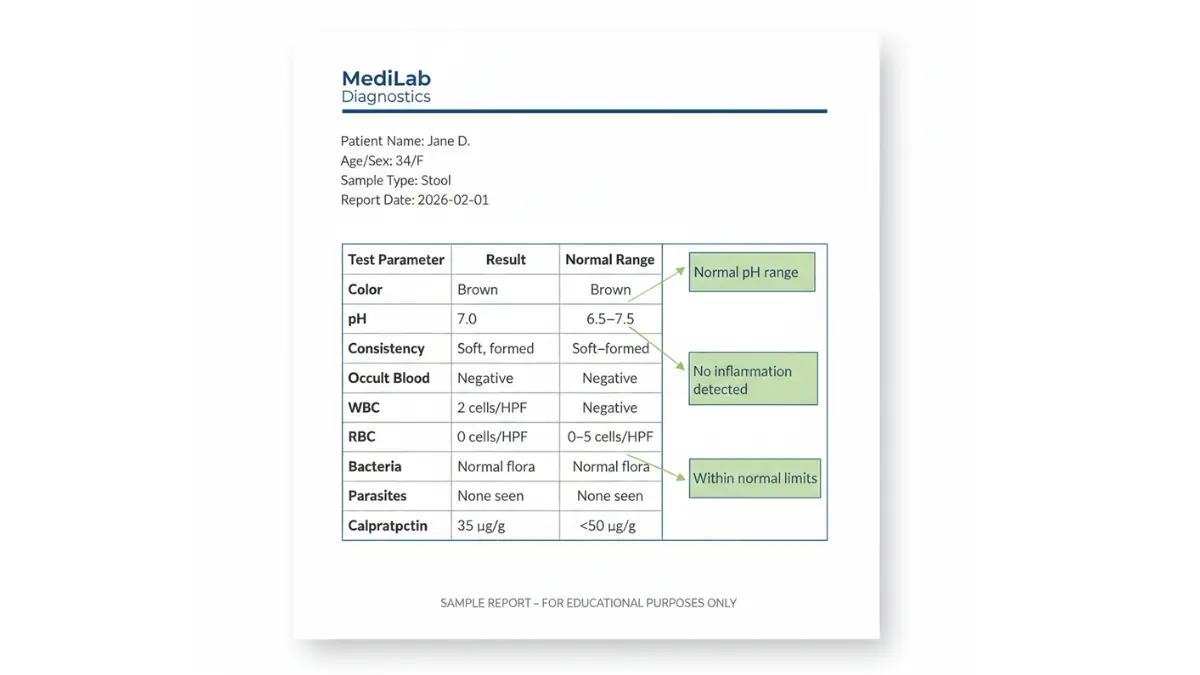
Here’s what Jasper needed to know immediately: A stool report is a laboratory analysis document that shows the physical, chemical, and microscopic characteristics of your stool sample. It reveals crucial information about digestive health, infections, inflammation, and potential bleeding in your gastrointestinal tract.
Your stool test results typically arrive 24-72 hours after specimen collection. The report contains parameters like color, consistency, pH levels, presence of blood, white blood cells (WBC), red blood cells (RBC), bacteria, parasites, and specialized markers like calprotectin or elastase. Each value tells your doctor something specific about how your digestive system functions.
Why reports look confusing: Medical laboratories use standardized formats designed for healthcare providers, not patients. Values appear as numbers, chemical abbreviations, and ranges that require medical interpretation. Most people receive results before their doctor appointment, leaving them anxious and uncertain.
What’s changed in 2026: Advanced testing now includes more sensitive detection methods for inflammatory markers, genetic risk assessment tools integration, and AI-assisted result interpretation. New reference ranges reflect diverse population data, and faster turnaround times mean you get results within 24-48 hours instead of 3-5 days.
This comprehensive guide walks you through every section of your stool report. You’ll learn what each parameter means, understand normal versus abnormal ranges, identify red flags requiring immediate attention, and know exactly what questions to ask your doctor.
Understanding Different Stool Test Types
Not all stool tests are the same. Your doctor orders specific tests based on your symptoms, medical history, and diagnostic needs.
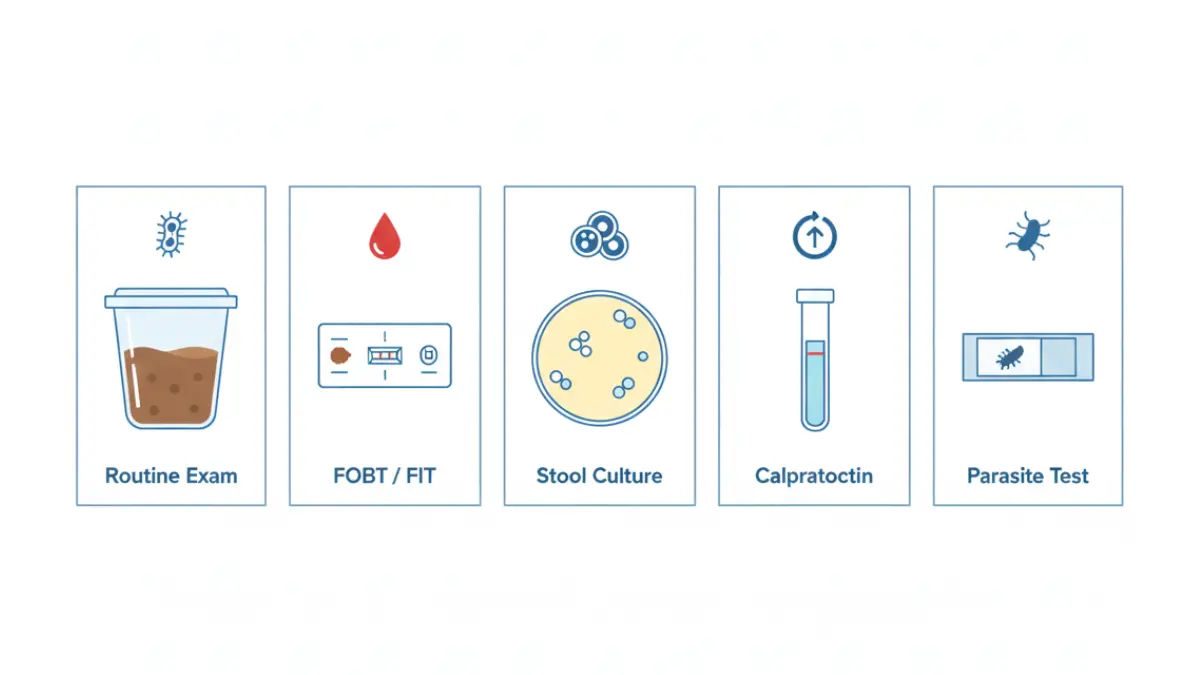
Routine Stool Examination (Most Common)
This comprehensive analysis evaluates physical appearance, chemical properties, and microscopic elements. The Centers for Disease Control and Prevention (CDC) provides detailed stool specimen collection guidelines that laboratories follow for accurate testing.
Routine examinations check color, consistency, pH, blood (visible and occult), mucus, pus cells, fat globules, undigested food particles, and muscle fibers. Doctors order this test when you experience persistent diarrhea, unexplained abdominal pain, changes in bowel habits, or suspected digestive disorders.
Fecal Occult Blood Test (FOBT/FIT)
The fecal immunochemical test (FIT) detects hidden blood in stool that’s invisible to the naked eye. This screening tool identifies early signs of colorectal cancer, polyps, ulcers, or inflammatory bowel disease (IBD).
Key difference in 2026: Modern FIT tests require only one sample instead of three, have 94% sensitivity for detecting colorectal cancer, and produce fewer false positives than older guaiac-based tests. The American Cancer Society recommends annual FIT screening for adults 45-75 years old.
Stool Culture (For Bacterial Infections)
Laboratory technicians place your sample in special growth media to identify disease-causing bacteria like Salmonella, Shigella, Campylobacter, or E. coli. Results typically take 48-72 hours as bacteria colonies multiply to detectable levels.
Your doctor orders stool cultures when you have bloody diarrhea, severe abdominal cramping, high fever above 102°F, recent international travel, or suspected food poisoning. The MedlinePlus C. diff testing guide explains how specific bacterial infections like Clostridioides difficile require specialized detection methods.
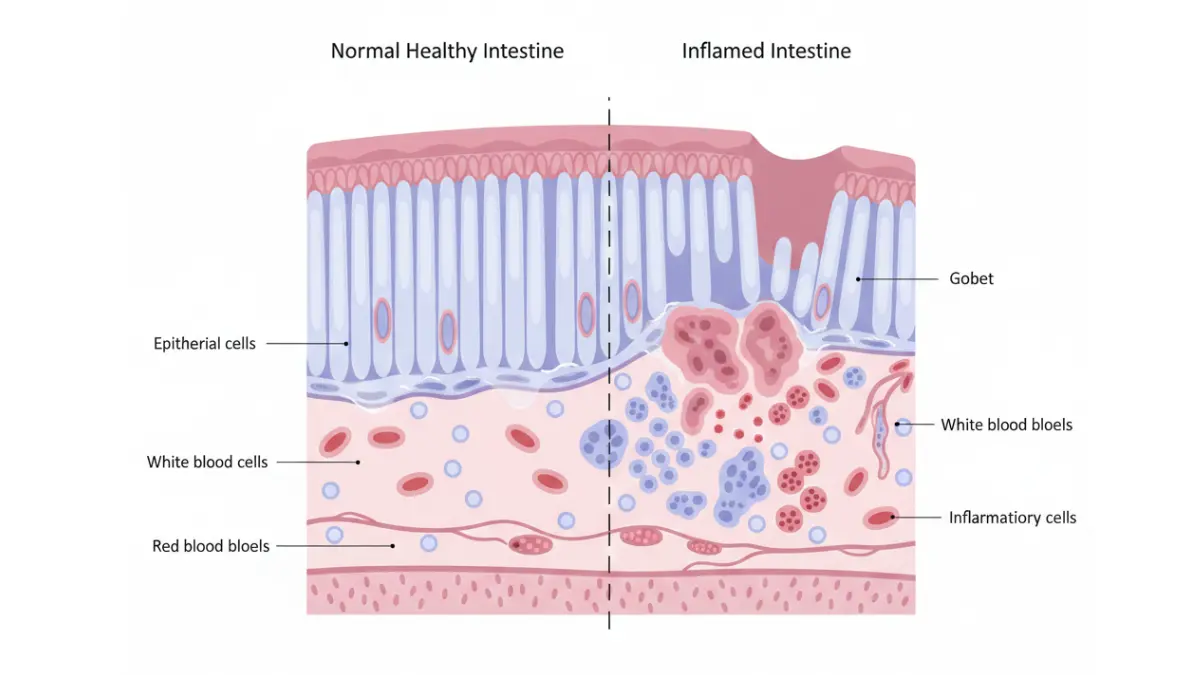
Calprotectin Test (For Inflammation)
This marker measures neutrophil activity in intestines. According to MedlinePlus calprotectin testing information, levels above 50 μg/g indicate inflammation, helping distinguish IBD from irritable bowel syndrome (IBS).
Clinical significance: Calprotectin testing has 93% sensitivity and 96% specificity for detecting inflammatory bowel disease in adults. It helps avoid unnecessary colonoscopies when levels are normal, reducing healthcare costs and patient anxiety.
Specialized Tests
- H. pylori antigen: Detects stomach bacteria causing ulcers
- Stool elastase: Measures pancreatic enzyme production (normal: >200 μg/g)
- Fat analysis: Quantifies fat malabsorption (normal: <7g per 24 hours)
- Parasite examination: Identifies protozoa, helminths, eggs, or cysts using the ova and parasite test methodology
Test Type Comparison Table:
| Test Type | Sample Needed | Turnaround Time | Primary Purpose |
|---|---|---|---|
| Routine Examination | 1 sample | 24-48 hours | General digestive health |
| FOBT/FIT | 1-3 samples | 24-72 hours | Cancer screening, bleeding detection |
| Stool Culture | 1 fresh sample | 48-96 hours | Bacterial infection diagnosis |
| Calprotectin | 1 sample | 24-48 hours | IBD vs IBS differentiation |
| Ova & Parasite | 3 samples over 3 days | 3-7 days | Parasitic infection detection |
| Elastase | 1 formed sample | 48-72 hours | Pancreatic function assessment |
Understanding which test your doctor ordered helps you interpret your specific report correctly. If you’re experiencing digestive symptoms alongside other health concerns, tools like our symptom checker can help identify patterns before your medical appointment.
Decoding Your Stool Report: Parameter-by-Parameter Guide
This section breaks down every line of your stool report exactly as it appears on laboratory documents.
Physical Characteristics Section
Color
- Normal: Brown (various shades from light to dark)
- Interpretation: Brown color comes from bile pigment breakdown (stercobilin)
Abnormal color meanings:
- Black/tarry: Upper GI bleeding, iron supplements, bismuth medications
- Bright red: Lower GI bleeding, hemorrhoids, anal fissures
- White/clay: Bile duct obstruction, liver disease, certain medications
- Yellow/greasy: Fat malabsorption, pancreatitis, celiac disease
- Green: Rapid intestinal transit, high vegetable intake, antibiotics
Consistency
- Normal: Soft, formed, sausage-shaped
- Abnormal: Watery (acute infection), hard pellets (constipation), loose (malabsorption)
The Bristol Stool Chart provides standardized descriptions. Types 3-4 are ideal, Type 1-2 suggest constipation, Types 5-7 indicate diarrhea.
Amount
- Normal: 100-200 grams per day
- Increased: >200g suggests malabsorption, excessive fiber intake, or rapid transit
- Decreased: <100g indicates constipation or inadequate dietary intake
Chemical Parameters Section
pH Level
- Normal range: 6.5-7.5 (neutral to slightly alkaline)
- Acidic (<6.5): Excessive carbohydrate fermentation, lactose intolerance
- Alkaline (>8.0): Protein putrefaction, small intestine disorders, chronic constipation
According to 2026 reference standards, pH variations outside normal ranges combined with other abnormal findings suggest specific digestive disorders requiring targeted treatment.
Occult Blood
- Normal: Negative (no blood detected)
- Positive: Indicates bleeding anywhere from esophagus to rectum
The fecal occult blood test can detect as little as 0.3mg hemoglobin per gram of stool—amounts invisible to the naked eye.
Microscopic Findings Section
White Blood Cells (WBC/Leukocytes)
- Normal range: 0-4 cells per high-power field (HPF)
- Elevated (>4 cells/HPF): Bacterial infection, inflammatory bowel disease, colitis
The white blood cell in stool test helps differentiate inflammatory from non-inflammatory diarrhea causes. More than 10 WBCs per HPF strongly suggests bacterial invasion.
Red Blood Cells (RBC)
- Normal: 0-2 cells/HPF
- Elevated: Intestinal bleeding, hemorrhoids, polyps, inflammatory conditions
Epithelial Cells
- Normal: 0-2 cells/HPF
- Increased: Intestinal lining shedding from inflammation or infection
Pus Cells
- Normal: 0-4 cells/HPF
- Elevated: Active infection, severe inflammation, abscess formation
Pus presence always indicates active disease requiring immediate medical evaluation.
Microbiological Results Section
Bacteria
- Normal: Mixed colonic flora (Bacteroides, E. coli, Enterococcus)
- Abnormal: Pathogenic species like Salmonella, Shigella, Campylobacter, C. difficile
Culture results identify specific organisms and antibiotic sensitivity patterns.
Parasites
- Normal: None detected
- Common findings: Giardia lamblia, Entamoeba histolytica, roundworms, tapeworms
Parasite identification requires multiple samples collected over 2-3 days since organism shedding is intermittent.
Fungi/Yeast
- Normal: Minimal Candida species
- Abnormal: Overgrowth indicates antibiotic disruption of normal flora
Special Markers Section
Calprotectin
- Normal: <50 μg/g
- Borderline: 50-100 μg/g (repeat testing recommended)
- Elevated: >100 μg/g (suggests IBD)
- Very high: >250 μg/g (active inflammation likely)
Studies show calprotectin correlates directly with intestinal inflammation severity. Monitoring levels helps assess IBD treatment effectiveness.
Elastase
- Normal: >200 μg/g
- Moderate insufficiency: 100-200 μg/g
- Severe insufficiency: <100 μg/g
The stool elastase test evaluates pancreatic enzyme production. Low levels indicate exocrine pancreatic insufficiency requiring enzyme replacement therapy.
Fat Quantification
- Normal: <7 grams per 24 hours (on 100g fat diet)
- Steatorrhea: >7 grams indicates fat malabsorption
Excess fat causes greasy, floating, foul-smelling stools. Common causes include pancreatitis, celiac disease, and cystic fibrosis.
What This Means For You: Each parameter provides one piece of the diagnostic puzzle. Isolated minor abnormalities often require no treatment, but multiple abnormal values together point toward specific conditions. Your doctor interprets results within the context of your symptoms, medical history, and physical examination findings.
Patients managing chronic conditions often benefit from tracking related health metrics. For example, those with inflammatory bowel disease might use our calorie deficit calculator to maintain nutrition during flare-ups, or monitor hydration needs with our water intake calculator.
Stool Report Normal Range: What Your Numbers Should Be
Laboratory reference ranges vary slightly between facilities, but 2026 standardized guidelines provide consistent benchmarks for interpretation.
Complete Normal Values Table (2026 Standards)
| Parameter | Normal Range | Units | Clinical Significance |
|---|---|---|---|
| Physical Characteristics | |||
| Color | Brown | Visual | Bile metabolism |
| Consistency | Soft, formed | Visual | Transit time, hydration |
| Amount | 100-200 | grams/day | Dietary intake, absorption |
| Odor | Characteristic, not foul | Qualitative | Bacterial fermentation |
| Chemical Parameters | |||
| pH | 6.5-7.5 | pH units | Digestive enzyme activity |
| Occult Blood | Negative | Qualitative | GI tract integrity |
| Microscopic Findings | |||
| WBC (Leukocytes) | 0-4 | cells/HPF | Inflammation marker |
| RBC (Erythrocytes) | 0-2 | cells/HPF | Bleeding indicator |
| Epithelial Cells | 0-2 | cells/HPF | Mucosal shedding |
| Pus Cells | 0-4 | cells/HPF | Infection marker |
| Specialized Markers | |||
| Calprotectin | <50 | μg/g | IBD screening |
| Elastase | >200 | μg/g | Pancreatic function |
| Fat (72-hour collection) | <7 | grams/day | Absorption efficiency |
| Reducing Substances | Negative | Qualitative | Carbohydrate malabsorption |
| Microbiological | |||
| Pathogenic Bacteria | None detected | Qualitative | Infection status |
| Parasites/Ova | None detected | Qualitative | Parasitic infection |
| Fungi/Yeast | Minimal | Qualitative | Flora balance |
Age-Specific Variations:
Infants (0-12 months):
- pH: 5.0-7.0 (more acidic due to milk-based diet)
- Bilirubin: May be present (immature gut flora)
- Fat: Higher baseline (breast milk/formula fat content)
- Consistency: Pasty to soft (varies with feeding method)
Children (1-12 years):
- Similar to adult ranges with slightly more variation
- pH: 6.0-7.5
- Consistency depends on diet and developmental stage
Adults (18+ years):
- Standard reference ranges apply
- Values stable unless affected by medications, diet, or disease
Elderly (65+ years):
- May have slower transit (firmer consistency)
- Medication effects more common
- Decreased pancreatic enzyme production possible
When “Slightly Abnormal” Isn’t Concerning
Laboratory variation: Different testing methods produce slightly different results. A calprotectin of 55 μg/g (just above 50 cutoff) from one lab might read 48 μg/g at another facility.
Dietary influences:
- Beets cause red-tinged stool
- Iron supplements create black color
- High-fat meals temporarily elevate fat levels
- Vitamin C affects occult blood testing
Medication effects:
- Antibiotics alter bacterial flora
- Bismuth compounds (Pepto-Bismol) darken stool
- NSAIDs may cause microscopic bleeding
- Laxatives change consistency and pH
Timing factors:
- Recent barium studies interfere with analysis
- Menstrual contamination affects occult blood results
- Hemorrhoid bleeding mimics GI tract bleeding
If only one minor parameter falls slightly outside range with no symptoms, your doctor typically recommends repeat testing in 2-4 weeks rather than immediate intervention.
Red Flag Values Requiring Immediate Action
Emergency situations (call doctor same day):
- Gross blood visible in stool (bright red or black/tarry)
- Pus cells >10/HPF with fever, severe pain, or dehydration
- Positive for C. difficile toxin (especially post-antibiotic)
- Multiple pathogenic bacteria detected
- Severe dehydration markers with persistent diarrhea (>7 days)
Urgent follow-up needed (within 48-72 hours):
- Occult blood positive on screening test
- Calprotectin >250 μg/g (high IBD probability)
- Elastase <100 μg/g (severe pancreatic insufficiency)
- WBC 5-10/HPF with chronic diarrhea
- Parasites detected (treatment needed)
Routine follow-up (1-2 weeks):
- Calprotectin 50-100 μg/g (borderline, needs monitoring)
- pH slightly abnormal without symptoms
- Minor fat elevation on single test
- 1-4 WBC/HPF without other abnormalities
Understanding these distinctions prevents unnecessary anxiety while ensuring serious findings receive appropriate attention. Similar to how our CBC test results guide helps patients understand blood work, stool report interpretation requires context and clinical correlation.
For comprehensive health tracking, patients managing digestive issues often monitor related metrics. The BMI calculator helps track weight changes from malabsorption, while the sleep calculator addresses the fatigue common with chronic digestive conditions.
Most Common Stool Test Findings: From Blood to Bacteria
Positive Occult Blood: Causes & Action Steps
What positive means: Microscopic blood detected in stool sample, invisible to naked eye.
Possible causes:
- Hemorrhoids (most common, 60% of positive tests)
- Colorectal polyps (15-20%)
- Colorectal cancer (2-5%)
- Ulcers (stomach or duodenal)
- Inflammatory bowel disease
- Diverticulosis
- Anal fissures
Immediate actions:
- Schedule colonoscopy within 30-60 days (your doctor’s primary recommendation)
- Document all current medications, especially blood thinners or NSAIDs
- Note any dietary changes (some foods cause false positives)
- Avoid repeat home testing—one positive result requires investigation
Long-term outlook: Most positive FOBT results don’t indicate cancer. A 2025 multicenter study found 96% of positive screenings revealed benign causes. However, early detection through screening saves lives—when found early, colorectal cancer has a 90% five-year survival rate.
Elevated WBC Count: Infection or Inflammation?
Normal range: 0-4 cells/HPF
Elevated range: 5-20+ cells/HPF
High WBC with acute symptoms (fever, severe diarrhea):
Likely bacterial infection requiring stool culture to identify pathogen.
Common culprits:
- Salmonella (food poisoning, typically resolves 4-7 days)
- Shigella (severe dysentery, needs antibiotics)
- Campylobacter (undercooked poultry, supportive care usually sufficient)
- E. coli O157:H7 (hemorrhagic colitis, avoid antibiotics)
High WBC with chronic symptoms (>2 weeks):
Suggests inflammatory bowel disease—ulcerative colitis or Crohn’s disease.
What This Means For You: WBC elevation points toward inflammation but doesn’t specify cause. Your doctor considers symptom duration, severity, associated findings, and medical history. Acute onset favors infection, gradual development suggests IBD.
Treatment varies dramatically:
- Bacterial infections: Antibiotics or supportive care with hydration
- IBD: Anti-inflammatory medications, immunosuppressants, biologics
- Parasites: Specific antiparasitic drugs
Detected Parasites: Treatment Protocols
Common parasites in United States:
- Giardia lamblia (33% of parasitic infections)
- Cryptosporidium (waterborne, particularly in immunocompromised)
- Entamoeba histolytica (rare but serious, can cause liver abscess)
- Pinworms (most common in children)
Symptoms prompting parasite testing:
- Chronic diarrhea after travel
- Weight loss despite normal appetite
- Bloating, gas, abdominal cramps
- Floating, greasy stools
- Fatigue, weakness
Treatment approach:
- Giardiasis: Metronidazole or tinidazole (single-dose treatment)
- Cryptosporidiosis: Nitazoxanide (self-limiting in immunocompetent)
- Amebiasis: Metronidazole followed by paromomycin
- Pinworms: Mebendazole or albendazole (treat household contacts)
Prevention: Proper handwashing, water filtration during travel, thorough cooking of meat, washing produce. Travelers to endemic areas should use bottled water and avoid ice, raw vegetables, and street food.
High Calprotectin: IBD vs IBS Differentiation
This test revolutionized gastroenterology by distinguishing inflammatory from non-inflammatory bowel conditions without invasive procedures.
Result interpretation:
- <50 μg/g: IBD unlikely (96% negative predictive value)
- 50-100 μg/g: Gray zone, consider repeat testing, clinical context
- 100-250 μg/g: Moderate inflammation, possible mild IBD
- >250 μg/g: High probability active IBD
IBS characteristics (calprotectin normal):
- Functional disorder without structural damage
- Triggered by stress, diet, hormones
- Symptoms include bloating, cramping, alternating diarrhea/constipation
- Managed with dietary modifications, stress reduction, medications
IBD characteristics (calprotectin elevated):
- Autoimmune destruction of intestinal lining
- Progressive disease requiring lifelong management
- Risk of complications (strictures, fistulas, cancer)
- Treated with immunosuppressants, biologics, sometimes surgery
What This Means For You: Elevated calprotectin doesn’t diagnose specific IBD type (Crohn’s vs ulcerative colitis) but confirms inflammation warrants colonoscopy with biopsies for definitive diagnosis.
Monitoring calprotectin during treatment helps assess medication effectiveness. Values decreasing toward normal indicate disease control; persistent elevation suggests treatment adjustment needed.
Abnormal pH Levels: What They Indicate
Low pH (<6.5) – Acidic stool:
- Causes: Lactose intolerance, excessive carbohydrate fermentation, small intestinal bacterial overgrowth (SIBO)
- Associated symptoms: Gas, bloating, watery diarrhea, abdominal distension
- Testing: Hydrogen breath test confirms lactose intolerance or SIBO
High pH (>8.0) – Alkaline stool:
- Causes: Protein maldigestion, small intestine disease, chronic constipation
- Associated symptoms: Foul odor, putty-like consistency, mucus
- Underlying conditions: Pancreatic insufficiency, celiac disease, chronic pancreatitis
Clinical approach:
Abnormal pH alone rarely changes management but provides supportive evidence for suspected diagnoses. Combined with other findings, it helps pinpoint specific digestive dysfunction.
Fat in Stool: Malabsorption Concerns
Steatorrhea definition: >7 grams fat per 24 hours (on diet containing 100g fat daily)
Visible signs:
- Greasy, shiny appearance
- Floats in toilet water
- Difficult to flush
- Offensive odor
- Pale yellow/gray color
Major causes:
- Pancreatic insufficiency (most common)
- Chronic pancreatitis
- Cystic fibrosis
- Pancreatic cancer
- Requires pancreatic enzyme replacement (Creon, Pancrelipase)
- Small intestine disease
- Celiac disease
- Crohn’s disease
- Small intestinal bacterial overgrowth
- Treated by addressing underlying condition
- Bile acid deficiency
- Liver disease
- Bile duct obstruction
- Gallbladder removal (some patients)
Diagnostic workup:
Fat malabsorption triggers cascade testing—elastase for pancreatic function, celiac antibodies, imaging studies, possibly endoscopy with biopsies.
Nutritional implications: Fat malabsorption prevents absorption of vitamins A, D, E, K. Patients require supplementation and monitoring for deficiency complications (osteoporosis, bleeding disorders, night blindness).
Understanding your results empowers informed discussions with healthcare providers. Similar to our liver function test results guide, stool report interpretation requires integrating multiple data points for accurate diagnosis.
Patients with malabsorption often need nutritional support tools. The macro calculator helps plan balanced intake, while the protein intake calculator ensures adequate protein despite digestive challenges.
Red Flags: When Stool Reports Signal Serious Conditions
Certain findings demand urgent evaluation regardless of symptom severity.
Cancer screening indicators:
- Positive FOBT/FIT after age 45
- Iron-deficiency anemia with positive occult blood
- Unexplained weight loss (>10 pounds in 3 months) with abnormal stool tests
- Persistent change in bowel habits (>6 weeks) with blood
Colorectal cancer risk increases with:
- Age >50 years (45 in African Americans)
- Family history of colon cancer/polyps
- Personal history of IBD >8 years
- Previous adenomatous polyps
- Hereditary syndromes (Lynch syndrome, familial adenomatous polyposis)
Colonoscopy urgency:
Positive screening tests require colonoscopy within 30-60 days. Delays beyond 90 days reduce cancer detection rates and worsen outcomes.
Infectious disease emergencies:
- C. difficile toxin positive (severe colitis risk)
- E. coli O157:H7 (hemolytic uremic syndrome possible)
- Shigella with high WBC (invasive dysentery)
- Parasites in immunocompromised patients
Inflammatory bowel disease warning signs:
- Calprotectin >250 μg/g with bloody diarrhea
- WBC >10/HPF with chronic symptoms
- Weight loss, anemia, malnutrition
- Extraintestinal manifestations (joint pain, skin lesions, eye inflammation)
Pancreatic insufficiency red flags:
- Elastase <100 μg/g with steatorrhea
- Progressive weight loss despite eating
- Fat-soluble vitamin deficiencies
- Diabetes development (suggests pancreatic destruction)
When second opinions matter:
- Ambiguous results requiring repeated testing
- Recommended invasive procedures (colonoscopy, endoscopy)
- Diagnosis of serious conditions (IBD, cancer)
- Treatment failures despite compliance
Emergency symptoms requiring immediate ER visit:
- Massive rectal bleeding (soaking through clothing)
- Severe dehydration (decreased urination, dizziness, confusion)
- High fever (>103°F) with bloody diarrhea
- Severe abdominal pain with rigidity
- Inability to keep down fluids for >24 hours
Early recognition and prompt action dramatically improve outcomes for serious gastrointestinal conditions.
11 Frequently Asked Questions About Stool Reports
1. How long does it take to get stool test results back?
Most routine stool tests return results within 24-48 hours. Stool cultures require 48-96 hours as bacteria colonies must grow to detectable levels. Specialized tests like ova and parasite exams may take 3-7 days since multiple samples analyzed over consecutive days improve detection rates.
2. Can I eat before a stool test?
Generally yes, normal eating is allowed. However, if testing for occult blood using guaiac method (gFOBT), avoid red meat, vitamin C supplements, and certain raw vegetables 48-72 hours before collection. Modern FIT tests have no dietary restrictions. Always follow your doctor’s specific instructions.
3. What does it mean if my stool culture is positive?
Positive culture confirms pathogenic bacteria are present causing infection. Results identify specific organism (Salmonella, Shigella, Campylobacter, C. difficile) and antibiotic sensitivities. Treatment depends on bacteria type—some require antibiotics, others resolve with supportive care and hydration alone.
4. Are home stool tests accurate?
Modern at-home FIT kits have 79-88% sensitivity for detecting colorectal cancer when used correctly. Accuracy depends on following instructions precisely, collecting adequate sample, returning promptly. Home tests work well for screening; positive results always require professional follow-up colonoscopy for diagnosis.
5. How often should I get stool tests done?
Screening (no symptoms): Annual FIT testing for colorectal cancer screening ages 45-75 years. Symptomatic: As directed by physician based on complaints. IBD monitoring: Every 3-6 months using calprotectin to assess disease activity. Post-infection: Repeat testing unnecessary if symptoms resolved unless working in food service or healthcare.
6. Can medications affect my stool test results?
Yes. Antibiotics alter bacterial flora, NSAIDs may cause microscopic bleeding, bismuth compounds darken stool, iron supplements create black color, laxatives change consistency. Inform your doctor about all medications including supplements before testing. Some tests require stopping certain drugs 1-2 weeks prior.
7. What’s the difference between FOBT and FIT tests?
Both detect hidden blood. FOBT (guaiac): Uses chemical reaction, requires dietary restrictions, detects animal and human blood, needs multiple samples, older technology. FIT: Uses antibodies specific to human hemoglobin, no dietary restrictions, more sensitive, requires 1-3 samples, fewer false positives. FIT is preferred in 2026 screening guidelines.
8. Do I need to repeat the test if results are borderline?
Usually yes. Borderline calprotectin (50-100 μg/g) warrants repeat testing in 2-4 weeks. Single borderline results may reflect temporary inflammation from medications, mild infection, or dietary factors. Persistently borderline or rising values prompt further investigation including possible colonoscopy.
9. Can stress affect stool test results?
Stress doesn’t directly alter test parameters but affects bowel function. Stress triggers IBS symptoms (diarrhea, constipation) which may prompt testing. However, stress doesn’t cause positive occult blood, elevated WBC, or pathogenic bacteria. If tests show organic disease, psychological factors aren’t the primary cause.
10. What foods should I avoid before a stool test?
For guaiac FOBT: Avoid red meat, turnips, horseradish, vitamin C supplements 48-72 hours before testing. For FIT, routine exams, cultures: No restrictions necessary. For fat analysis: Maintain diet with 100 grams fat daily for 72 hours before collection to ensure accurate baseline.
11. How do I collect a stool sample properly?
Use clean, dry container provided by laboratory. Urinate first to prevent contamination. Place plastic wrap over toilet or use collection tray. After bowel movement, scoop small amount (walnut-size) into container using collection spoon. Close lid tightly, label with name/date/time. Refrigerate if unable to deliver within 2 hours. Never collect from toilet water or allow urine mixing.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment. Always consult qualified healthcare providers for medical decisions. Stool test interpretation requires clinical correlation with symptoms, physical examination, and medical history. Do not attempt self-diagnosis or treatment based solely on test results.
About the Author: This comprehensive guide was developed with input from board-certified gastroenterologists and reviewed according to current clinical practice guidelines. Updated February 2026 with latest diagnostic criteria and reference ranges. For more health information, visit our health section.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.