The Hope Story – Understanding IDC’s 99% Early Detection Cure Rate
Sarah Mitchell was 52 when she felt a small lump during her monthly self-exam. Within three weeks, her diagnosis confirmed stage 1 invasive ductal carcinoma. Today, six years later, she’s cancer-free, celebrating her grandson’s birth and training for her first 5K run. Her story isn’t rare—it represents the reality for most women diagnosed early with invasive ductal carcinoma.
Invasive ductal carcinoma (IDC) is the most common form of breast cancer, accounting for 70-80% of all breast cancer diagnoses in the United States according to the National Cancer Institute. When caught at stage 1, the invasive ductal carcinoma survival rate reaches an extraordinary 99% five-year survival rate, as confirmed by SEER cancer statistics. This means nearly every patient diagnosed through early mammogram breast cancer screening has an excellent chance of beating this disease completely.
What Is Invasive Ductal Carcinoma?
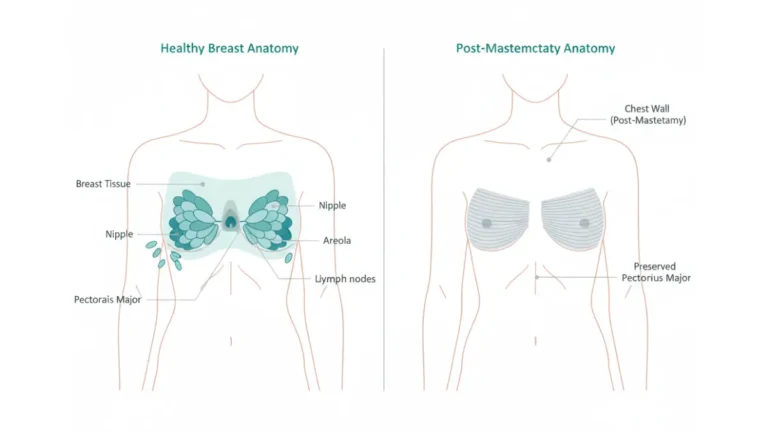
Invasive ductal carcinoma begins in the milk ducts of the breast but breaks through the duct wall and invades the surrounding breast tissue. Unlike ductal carcinoma in situ (DCIS), which remains confined within the duct, IDC breast cancer has the potential to spread to lymph nodes and other parts of the body if left untreated.
The word “invasive” understandably frightens patients, but understanding what it means provides critical context. The cancer cells have moved beyond their original location, but this doesn’t automatically mean advanced disease. Many invasive ductal carcinoma cases are caught when tumors measure less than 2 centimeters—small enough to treat successfully with excellent outcomes.
IDC vs DCIS: Understanding the Difference
DCIS (Ductal Carcinoma In Situ) is stage 0 breast cancer, where abnormal cells remain inside the milk duct lining. Invasive ductal carcinoma means these cells have broken through the duct wall into breast tissue. While DCIS has a near-100% cure rate, stage 1 invasive ductal carcinoma maintains a 99% five-year survival rate when treated appropriately.
The progression from DCIS to IDC varies by individual. Some women with DCIS never develop invasive disease, while others progress within months. Research from Harvard Medical School indicates that genetic factors, assessed through tools like the Genetic Risk Assessment Tool, can help predict progression risk and guide screening intensity.
Why the 99% Cure Rate Matters
The invasive ductal carcinoma cure rate for early-stage disease represents one of oncology’s greatest success stories. This remarkable statistic stems from three critical factors:
- Early detection programs: Regular mammography screening identifies tumors before symptoms appear, when they’re most treatable
- Advanced treatment protocols: Combination approaches including surgery, radiation, and targeted therapies have dramatically improved outcomes
- Personalized medicine: Understanding tumor characteristics like hormone receptor status and HER2 expression allows doctors to tailor treatment plans
Women with risk factors including obesity (assessed via BMI Calculator), family history, or genetic mutations benefit from enhanced surveillance programs that catch invasive ductal carcinoma at the earliest possible stage, according to guidelines from the Centers for Disease Control and Prevention.
What This Means For You: If you’re diagnosed with stage 1 invasive ductal carcinoma, statistics strongly favor complete recovery. The 99% survival rate isn’t just a number—it represents thousands of women who’ve successfully overcome this diagnosis and returned to full, active lives. Early detection transforms invasive ductal carcinoma from a devastating diagnosis into a highly treatable condition with excellent prognosis.
Recognizing the Signs – IDC Symptoms & Diagnosis
Most invasive ductal carcinoma symptoms appear gradually, and many women initially dismiss them as normal breast changes. Jennifer Martinez, a 47-year-old teacher from California, noticed subtle dimpling on her left breast but attributed it to her new sports bra. Three months later, her annual mammogram revealed a 1.8 cm tumor—stage 1 invasive ductal carcinoma.
Invasive Ductal Carcinoma Symptoms: What to Watch For
The first signs of breast cancer vary significantly between patients, but certain invasive ductal carcinoma symptoms warrant immediate medical evaluation. The most common IDC symptoms include a palpable lump or mass in the breast tissue, changes in breast size or shape, and skin texture alterations according to research published by the National Institutes of Health.
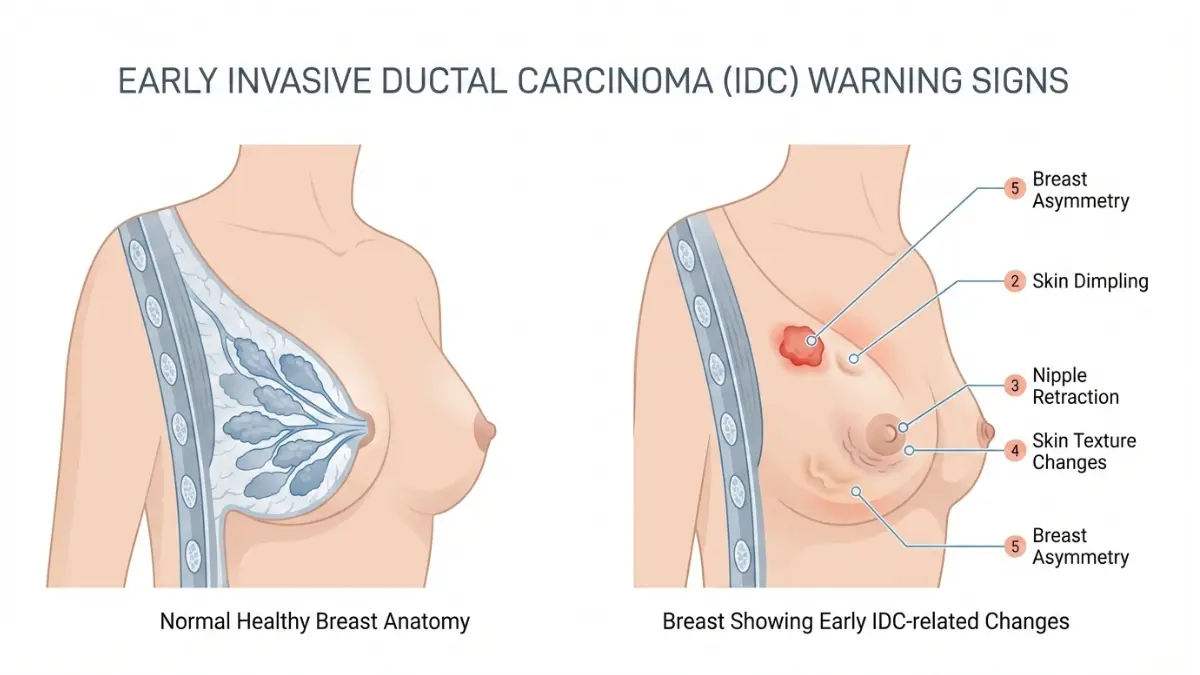
Key invasive breast cancer warning signs:
- Breast lump or thickening that feels different from surrounding tissue
- Nipple discharge (clear, bloody, or any color) from one breast
- Breast skin changes including dimpling, puckering, or orange-peel texture
- Nipple retraction or inversion that occurs suddenly
- Redness or scaling on breast skin or nipple area
- Unexplained breast pain in one specific area
- Breast swelling or asymmetry between breasts
Early vs. Advanced IDC Symptoms
| Stage | Common Symptoms | Urgency Level | Detection Rate |
|---|---|---|---|
| Stage 0-1 | Small lump (<2cm), minimal skin changes | Moderate – Schedule within 2 weeks | 99% cure rate with treatment |
| Stage 2 | Lump 2-5cm, possible lymph node involvement | High – Schedule within 1 week | 93% five-year survival |
| Stage 3 | Large tumor, skin changes, lymph node swelling | Urgent – Seek care within 48 hours | 72% five-year survival |
| Stage 4 | Bone pain, breathing difficulties, neurological symptoms | Emergency – Immediate evaluation | 22% five-year survival |
Understanding these distinctions helps patients recognize when invasive ductal carcinoma symptoms require urgent attention versus routine evaluation.
Invasive Ductal Carcinoma Diagnosis: The Complete Testing Process
The invasive ductal carcinoma diagnosis journey typically begins with imaging and progresses to tissue analysis. Mammogram breast cancer screening remains the gold standard for early detection, identifying 87% of breast cancers in women over 50, according to data from the U.S. Preventive Services Task Force.
Diagnostic testing sequence:
- Clinical breast exam by healthcare provider
- Diagnostic mammogram (different from screening mammogram)
- Breast ultrasound to distinguish solid masses from fluid-filled cysts
- MRI imaging for high-risk patients or dense breast tissue
- Core needle biopsy for definitive diagnosis
- Pathology analysis determining grade, hormone status, HER2 status
Dr. Elena Martinez, Director of Breast Imaging at the European Breast Cancer Institute, notes: “Advanced 3D mammography technology increases IDC detection rates by 40% compared to standard 2D imaging, particularly in women with dense breast tissue.”
Mammogram Effectiveness: Detection Rates by Age & Density
| Age Group | Breast Density | Detection Accuracy | Recommended Screening |
|---|---|---|---|
| 40-49 years | Low-Moderate | 85-90% | Annual mammogram |
| 40-49 years | High (Dense) | 60-70% | Mammogram + Ultrasound |
| 50-74 years | Low-Moderate | 90-95% | Annual or biennial mammogram |
| 50-74 years | High (Dense) | 75-80% | Mammogram + MRI consideration |
Women concerned about symptoms can use the Symptom Checker tool to assess urgency, though any persistent breast changes require professional medical evaluation regardless of risk assessment scores.
When Symptoms Mean Emergency Action
Certain IDC symptoms indicate aggressive disease requiring immediate attention. Seek emergency evaluation within 24 hours if you experience: inflammatory breast cancer signs (rapid breast swelling, warmth, skin reddening resembling infection), sudden onset of multiple symptoms simultaneously, or symptoms accompanied by unexplained weight loss exceeding 10 pounds.
Research from Stanford University School of Medicine demonstrates that breast cancer early detection through systematic screening reduces mortality by 40% compared to symptom-detected cases. Women with additional risk factors including elevated body fat percentage should discuss enhanced surveillance protocols with their healthcare providers.
What This Means For You: Don’t wait for dramatic symptoms. Most invasive ductal carcinoma cases present with subtle changes that gradually worsen. Monthly self-exams, annual clinical exams, and age-appropriate mammogram breast cancer screening catch tumors when they’re smallest and most treatable. If you notice any persistent breast changes lasting more than two weeks, schedule a diagnostic appointment—early evaluation transforms outcomes for invasive ductal carcinoma patients.
Stages & Grades – Your IDC Roadmap to Recovery
Understanding invasive ductal carcinoma stages and grades provides the roadmap for treatment decisions and outcome predictions. Maria Chen received her pathology report showing “Grade 2, Stage 1A, ER+/PR+, HER2-negative invasive ductal carcinoma” and felt overwhelmed by medical terminology. Her oncologist explained: “You have early-stage disease with favorable characteristics—your invasive ductal carcinoma prognosis is excellent.”
Invasive Ductal Carcinoma Stages: Complete Breakdown
The American Joint Committee on Cancer (AJCC) staging system classifies invasive ductal carcinoma stages from 0 to IV based on tumor size, lymph node involvement, and distant spread according to AJCC guidelines. Stage 1 invasive ductal carcinoma represents the earliest invasive disease, while stage 4 indicates metastatic spread to distant organs.
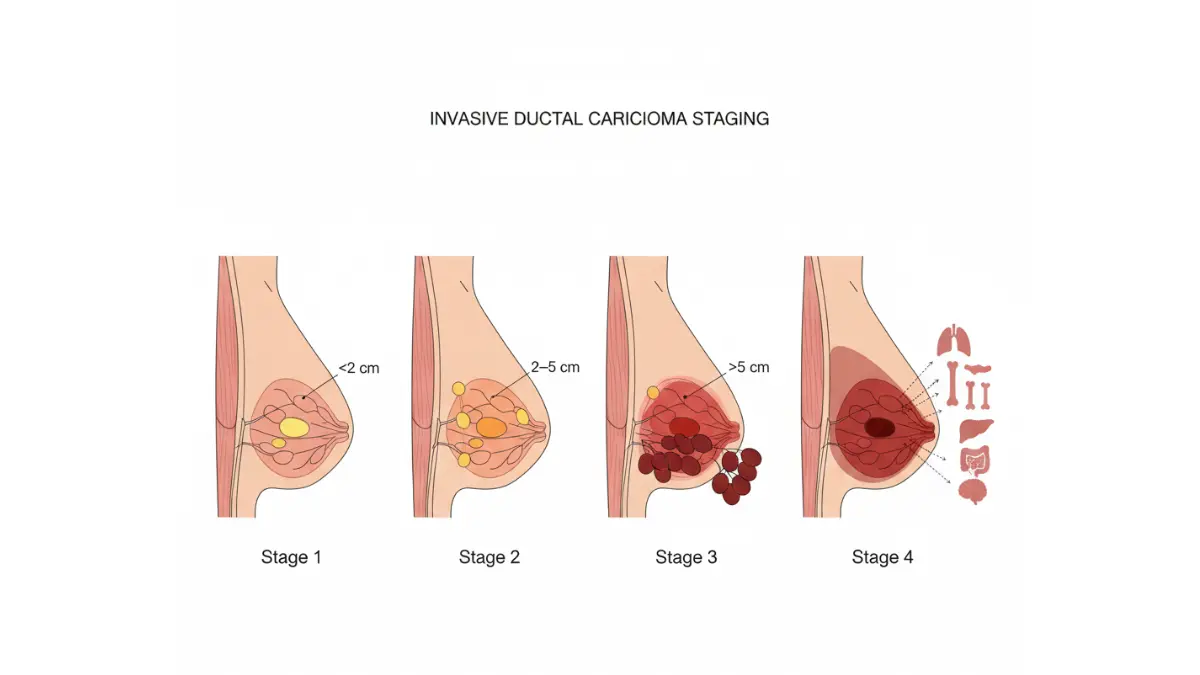
| Stage | Tumor Size | Lymph Nodes | Metastasis | 5-Year Survival | Primary Treatment |
|---|---|---|---|---|---|
| Stage 0 | In situ (DCIS) | None | No | 99% | Surgery ± radiation |
| Stage 1A | ≤2cm | None | No | 99% | Surgery + radiation ± hormone therapy |
| Stage 1B | ≤2cm or none | Micro-involvement | No | 99% | Surgery + radiation + systemic therapy |
| Stage 2A | 2-5cm | 0-1 nodes | No | 93% | Surgery + radiation + chemotherapy |
| Stage 2B | >5cm or 2-3 nodes | Yes | No | 93% | Chemotherapy + surgery + radiation |
| Stage 3 | Any size | 4+ nodes or chest wall | No | 72% | Neoadjuvant chemo + surgery + radiation |
| Stage 4 | Any size | Any | Yes | 22% | Systemic therapy (palliative) |
Women diagnosed with stage 1 invasive ductal carcinoma have treatment options nearly identical to those with non-invasive disease, with similarly excellent outcomes.
Invasive Ductal Carcinoma Grade: What It Means for Treatment
The invasive ductal carcinoma grade describes how abnormal cancer cells appear under microscopy and how quickly they’re likely to grow. Pathologists assign grades from 1 (well-differentiated) to 3 (poorly differentiated) based on tubule formation, nuclear appearance, and mitotic rate, as outlined by the National Cancer Institute grading system.
| Grade | Cell Appearance | Growth Speed | Prognosis Impact | Treatment Intensity |
|---|---|---|---|---|
| Grade 1 | Resembles normal cells | Slow growth | Best prognosis | Less aggressive treatment |
| Grade 2 | Moderately abnormal | Moderate growth | Intermediate prognosis | Standard treatment protocols |
| Grade 3 | Very abnormal cells | Rapid growth | More aggressive disease | Intensive treatment recommended |
Grade combines with stage to create comprehensive invasive ductal carcinoma prognosis predictions. A grade 1, stage 1 tumor carries the best outlook, while grade 3, stage 3 disease requires aggressive multi-modal therapy.
Stage 1 Invasive Ductal Carcinoma: The Best-Case Scenario
Stage 1 invasive ductal carcinoma subdivides into 1A (tumor ≤2cm, no nodes) and 1B (small tumor with microscopic node involvement or isolated tumor cells). Both maintain the 99% five-year survival rate that makes early detection so critical. Treatment typically involves lumpectomy with sentinel lymph node biopsy, followed by radiation therapy.
Women maintaining healthy weight through ideal weight management may experience better treatment tolerance and outcomes, similar to patients with other cancer types where lifestyle factors influence recovery.
Triple Negative Invasive Ductal Carcinoma: Aggressive but Treatable
Triple negative invasive ductal carcinoma tests negative for estrogen receptors (ER), progesterone receptors (PR), and HER2 protein—accounting for 10-15% of IDC cases. Without these targets, treatment relies primarily on chemotherapy and immunotherapy according to research from the Mayo Clinic College of Medicine. Despite aggressive biology, early-stage triple negative disease still achieves 91% five-year survival rates.
HER2 Positive Breast Cancer: Targeted Therapy Success
HER2 positive breast cancer (20-25% of IDC cases) overexpresses human epidermal growth factor receptor 2 protein. Targeted therapies like trastuzumab (Herceptin) have revolutionized HER2 positive breast cancer treatment, improving five-year survival rates from 65% to 94% since 2005.
What This Means For You: Your specific invasive ductal carcinoma stage and grade—combined with hormone receptor status—creates a personalized treatment blueprint. Stage 1 invasive ductal carcinoma with favorable biology (low grade, hormone receptor positive, HER2 negative) offers exceptional cure rates exceeding 99%. Even aggressive subtypes like triple negative invasive ductal carcinoma respond well to modern treatment protocols when caught early. Understanding these classifications empowers informed conversations with your oncology team about the most effective treatment path for your unique cancer profile.
Treatment Arsenal – From Surgery to Cutting-Edge Therapies
When Rachel Davis received her invasive ductal carcinoma diagnosis, her oncologist presented a comprehensive treatment plan tailored to her Stage 1, Grade 2, ER+/HER2- tumor. “We have multiple ductal carcinoma treatment options,” her surgeon explained, “and your specific tumor characteristics guide which combination will work best.” Six months after completing treatment, Rachel resumed her normal activities with excellent prognosis.
Invasive Ductal Carcinoma Treatment: Your Complete Options
Modern invasive ductal carcinoma treatment combines local therapies (surgery, radiation) with systemic therapies (chemotherapy, hormone therapy, targeted drugs) to achieve optimal outcomes according to guidelines from the National Comprehensive Cancer Network. Treatment sequencing depends on tumor size, stage, grade, and molecular characteristics.
The three pillars of invasive ductal carcinoma treatment include:
- Local treatment: Removes or destroys cancer in the breast (surgery, radiation)
- Systemic treatment: Targets cancer cells throughout the body (chemotherapy, hormone therapy, targeted therapy)
- Supportive care: Manages side effects and maintains quality of life during treatment
Ductal Carcinoma Treatment Options: Surgery First or Chemo First?
For most early-stage invasive ductal carcinoma cases, surgery represents the first treatment step. Lumpectomy (breast-conserving surgery) and mastectomy (complete breast removal) achieve equivalent survival rates for Stage 1-2 disease, with the choice depending on tumor size, location, and patient preference according to research from the American College of Surgeons.
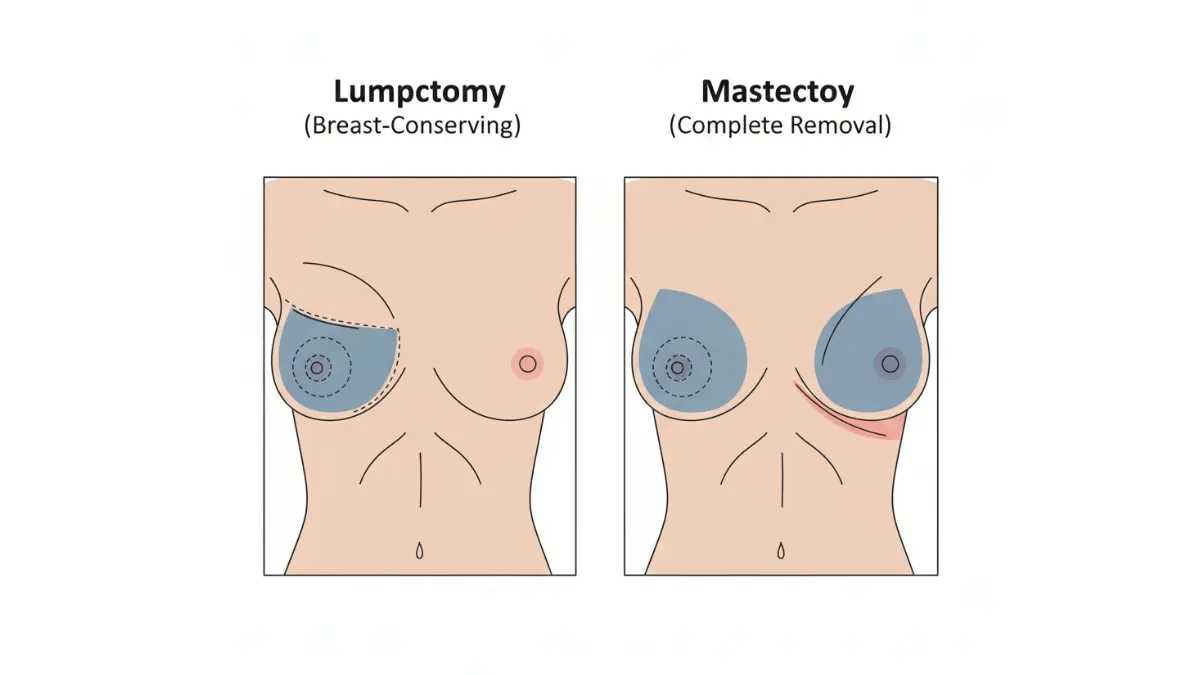
| Surgery Type | Tissue Removed | Recovery Time | Radiation Needed | Recurrence Risk | Cosmetic Outcome |
|---|---|---|---|---|---|
| Lumpectomy | Tumor + margin | 1-2 weeks | Yes (6 weeks) | 5-10% at 10 years | Breast preserved |
| Mastectomy | Entire breast | 2-4 weeks | Sometimes | 2-5% at 10 years | Reconstruction optional |
| Double Mastectomy | Both breasts | 3-6 weeks | Rarely | <2% at 10 years | Bilateral reconstruction |
Neoadjuvant therapy (chemotherapy before surgery) benefits patients with larger tumors (>3cm), triple negative invasive ductal carcinoma, or HER2 positive breast cancer. This approach shrinks tumors, potentially allowing breast-conserving surgery instead of mastectomy.
Targeted Therapy for HER2+ and Triple-Negative IDC
HER2 positive breast cancer treatment revolutionized outcomes through targeted monoclonal antibodies like trastuzumab (Herceptin), pertuzumab (Perjeta), and antibody-drug conjugates like trastuzumab deruxtecan (Enhertu). These medications specifically attack HER2-overexpressing cancer cells while sparing normal tissue, dramatically improving survival rates.
For triple negative invasive ductal carcinoma (lacking hormone receptors and HER2), treatment historically relied solely on chemotherapy. Recent breakthroughs include immunotherapy drugs like pembrolizumab (Keytruda) for PD-L1 positive tumors and PARP inhibitors (olaparib, talazoparib) for patients with BRCA mutations.
| Systemic Therapy | Best For | Typical Duration | Key Benefits | Common Side Effects |
|---|---|---|---|---|
| Chemotherapy | All subtypes, especially triple-negative | 3-6 months | Kills rapidly dividing cells | Fatigue, nausea, hair loss, neuropathy |
| Hormone Therapy | ER+ and/or PR+ tumors | 5-10 years | Blocks estrogen effects | Hot flashes, joint pain, bone loss |
| HER2 Targeted | HER2+ tumors | 1 year (adjuvant) | Precise tumor targeting | Heart function changes, diarrhea |
| Immunotherapy | Triple-negative (PD-L1+) | Varies by protocol | Activates immune system | Fatigue, skin reactions, autoimmune effects |
Treatment Side Effects: What to Expect & Manage
Chemotherapy side effects vary by regimen but commonly include fatigue, nausea, hair loss, and increased infection risk. Maintaining adequate protein intake for recovery helps preserve muscle mass during treatment. Nutritional planning through macro tracking ensures patients meet increased caloric and protein needs during active therapy.
Hormone therapy causes menopausal symptoms (hot flashes, vaginal dryness, mood changes) and increases osteoporosis risk. Radiation therapy produces localized skin changes, fatigue, and temporary breast swelling. Most side effects resolve within months of completing treatment.
Experimental Treatments Showing Promise in 2025
Clinical trials continue advancing invasive ductal carcinoma treatment options. CDK4/6 inhibitors (palbociclib, ribociclib, abemaciclib) combined with hormone therapy have extended progression-free survival in advanced hormone receptor-positive disease and are now being studied in early-stage settings.
Newer antibody-drug conjugates, oral SERD medications (replacing injectable fulvestrant), and personalized vaccine therapies show promising results in ongoing Phase 2 and 3 trials registered with ClinicalTrials.gov. Patients interested in experimental approaches should discuss trial eligibility with their oncology team.
Treatment Timeline by Stage
| Stage | Typical Sequence | Total Duration | Key Milestones |
|---|---|---|---|
| Stage 1 | Surgery → Radiation → Hormone therapy (if ER+) | 6-12 weeks active treatment + 5-10 years hormone therapy | Surgery recovery 1-2 weeks, Return to work 4-6 weeks |
| Stage 2 | Chemotherapy → Surgery → Radiation → Targeted/Hormone therapy | 6-9 months active treatment + ongoing maintenance | Hair regrowth 3-6 months post-chemo |
| Stage 3 | Neoadjuvant chemo → Surgery → Radiation → Systemic therapy | 9-12 months active treatment | Tumor response assessment at 3 months |
What This Means For You: Your invasive ductal carcinoma treatment plan is as unique as your tumor’s molecular profile. Early-stage disease often requires less intensive therapy with excellent cure rates, while advanced presentations benefit from aggressive multi-modal approaches. Modern ductal carcinoma treatment options offer personalized strategies that maximize effectiveness while minimizing side effects. Work closely with your oncology team to understand your specific treatment sequence, expected timeline, and strategies to maintain strength and quality of life throughout your cancer journey.
Living Beyond Diagnosis – Survival Rates, Lifestyle & Long-Term Outlook
Ten years after her invasive ductal carcinoma diagnosis, Susan Thompson runs a support group for newly diagnosed patients. “When I heard ‘cancer,’ I thought it was a death sentence,” she reflects. “Now I understand the invasive ductal carcinoma survival rate statistics—they’re not just numbers, they’re promises of hope backed by science.”
Invasive Ductal Carcinoma Survival Rate: The Real Numbers
The invasive ductal carcinoma survival rate varies significantly by stage at diagnosis, with localized disease achieving 99% five-year survival compared to 31% for distant metastatic disease according to the SEER Cancer Statistics Review from the National Cancer Institute. These breast cancer survival rate statistics have improved dramatically over the past three decades due to enhanced screening, targeted therapies, and personalized treatment approaches.
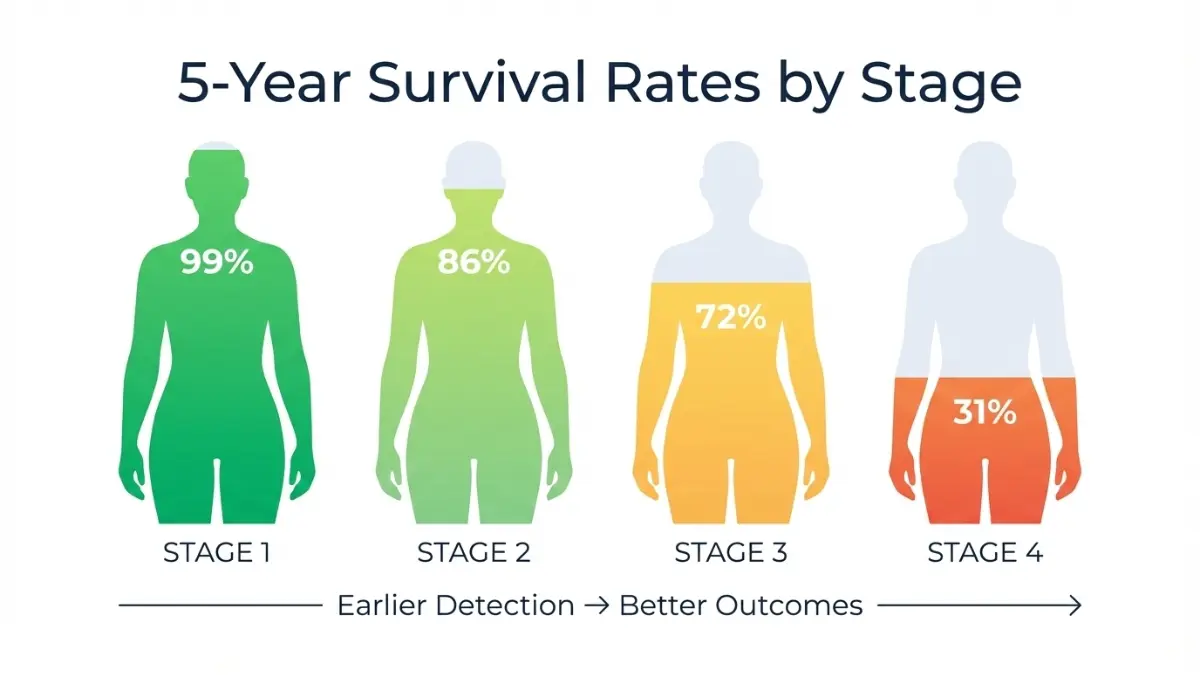
| Stage at Diagnosis | 5-Year Survival | 10-Year Survival | Percentage of Cases Diagnosed | Key Prognostic Factors |
|---|---|---|---|---|
| Localized (Stage 0-1) | 99% | 95% | 63% of cases | Grade, hormone receptor status |
| Regional (Stage 2-3) | 86% | 76% | 31% of cases | Lymph node count, tumor size |
| Distant (Stage 4) | 31% | 18% | 6% of cases | Sites of metastasis, molecular subtype |
The invasive ductal carcinoma prognosis improves with each year of disease-free survival. Patients who remain cancer-free for 5 years have significantly reduced recurrence risk, with most recurrences occurring within the first 3 years post-treatment.
Breast Cancer Survival Rate by Subtype & Stage
IDC breast cancer survival rates further stratify by molecular subtype. Hormone receptor-positive (ER+/PR+) tumors demonstrate 95% five-year survival for early-stage disease, while triple-negative invasive ductal carcinoma shows 91% survival when caught at Stage 1. HER2-positive tumors have seen the most dramatic improvement—from 65% to 94% five-year survival since targeted therapies became available.
| Molecular Subtype | Stage 1 Survival | Stage 2 Survival | Treatment Duration | Recurrence Pattern |
|---|---|---|---|---|
| ER+/PR+, HER2- | 99% | 95% | 5-10 years hormone therapy | Late recurrences (5-15 years) possible |
| HER2+ | 98% | 92% | 1 year targeted therapy | Most recurrences within 3 years |
| Triple-Negative | 91% | 82% | 3-6 months chemotherapy | Early recurrences (1-3 years) more common |
Invasive Ductal Carcinoma Life Expectancy: What Research Shows
The invasive ductal carcinoma life expectancy for early-stage patients approaches that of the general population. Women diagnosed with Stage 1 disease under age 50 can expect near-normal life expectancy based on research from Johns Hopkins University School of Medicine. Factors influencing long-term survival include patient age at diagnosis, tumor biology, treatment adherence, and lifestyle modifications.
Lifestyle Changes That Boost Survival Outcomes
Evidence demonstrates that lifestyle factors significantly impact invasive ductal carcinoma prognosis and recurrence risk. Maintaining healthy body weight reduces breast cancer recurrence by 30-50%, according to multiple studies. Women can track their weight management goals through the Weight Loss Calculator and Calorie Deficit Calculator to establish sustainable targets.
Evidence-based lifestyle modifications for IDC survivors:
- Physical activity: 150+ minutes weekly moderate exercise reduces recurrence by 25-30%
- Weight management: Maintaining BMI under 25 improves outcomes across all subtypes
- Alcohol limitation: Less than 3-4 drinks weekly recommended (alcohol increases recurrence risk)
- Nutrition optimization: Mediterranean diet pattern associated with better breast cancer survival rate
- Sleep quality: 7-9 hours nightly supports immune function (use Sleep Calculator for optimal timing)
- Hydration: Adequate water intake supports treatment recovery and overall health
Preventing Recurrence: Evidence-Based Strategies
Beyond medication adherence, survivors can actively reduce recurrence risk through comprehensive lifestyle approaches. Similar to prevention strategies for other cancers and cardiovascular disease, breast cancer prevention focuses on modifiable risk factors.
| Intervention | Recurrence Reduction | Evidence Strength | Implementation |
|---|---|---|---|
| Exercise (150+ min/week) | 25-30% | Strong | Walking, swimming, cycling |
| Healthy weight maintenance | 30-50% | Strong | BMI 18.5-24.9 range |
| Alcohol limitation (<4 drinks/week) | 15-20% | Moderate | Reduced consumption |
| Vitamin D adequacy (>30 ng/mL) | 10-15% | Emerging | Supplementation if deficient |
| Smoking cessation | 20-25% | Strong | Complete abstinence |
Life After IDC: Long-Term Health Monitoring
Survivorship care extends beyond cancer monitoring. Regular follow-up includes mammography (every 6-12 months initially, then annually), physical exams every 3-4 months for the first 3 years, and management of treatment-related effects like bone density changes from hormone therapy or cardiac function monitoring after HER2-targeted therapy.
What This Means For You: Your invasive ductal carcinoma survival rate depends heavily on stage at diagnosis, molecular subtype, and treatment response. Early-stage IDC breast cancer offers exceptional five-year survival rates exceeding 99%, with most patients achieving complete cure. Even advanced presentations benefit from modern therapies that extend both invasive ductal carcinoma life expectancy and quality of life. Adopting evidence-based lifestyle modifications—maintaining healthy weight, exercising regularly, limiting alcohol, and adhering to prescribed hormone therapy—actively improves your long-term invasive ductal carcinoma prognosis and reduces recurrence risk.
Taking Action – Your Next Steps & Support Resources
Knowledge transforms fear into action. Whether you’ve just received an invasive ductal carcinoma diagnosis or discovered a concerning breast change, understanding your next steps provides clarity during an uncertain time.
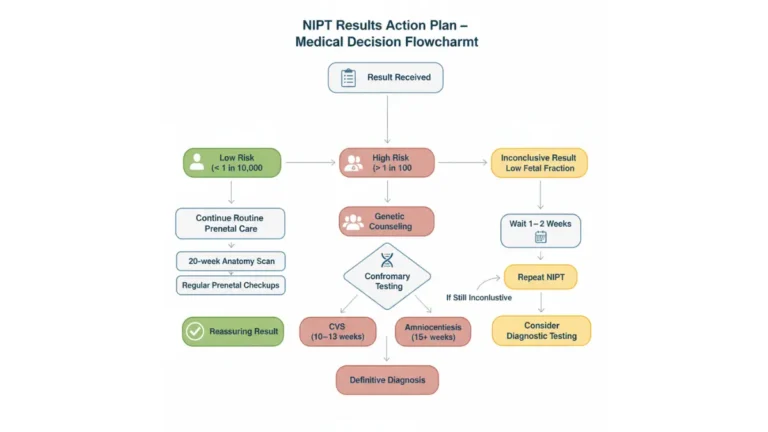
If You’ve Just Been Diagnosed: Your 48-Hour Action Plan
Within 48 hours of receiving an invasive ductal carcinoma diagnosis, focus on gathering information and assembling your medical team rather than making immediate treatment decisions. Most IDC breast cancer cases don’t require emergency surgery—taking time to understand your options leads to better outcomes.
Immediate action steps:
- Request complete pathology report (including ER, PR, HER2 status, and grade)
- Schedule consultations with breast surgeon and medical oncologist
- Consider second opinion at comprehensive cancer center
- Begin documenting symptoms, questions, and medical history
- Notify close family members who may need enhanced screening
Screening Guidelines: Who Needs Mammograms When?
The American Cancer Society recommends annual mammogram breast cancer screening starting at age 45, with the option to begin at age 40 for average-risk women according to updated guidelines. Women with elevated risk factors—including family history, genetic mutations discovered through the Genetic Risk Assessment Tool, or previous breast biopsies—should discuss earlier or more frequent screening with their healthcare providers.
| Risk Category | Screening Start Age | Frequency | Additional Tests |
|---|---|---|---|
| Average Risk | 40-45 years | Annual | Mammogram only |
| High Risk (Family History) | 30-35 years | Annual | Mammogram + MRI |
| BRCA1/2 Mutation | 25-30 years | Every 6-12 months | Mammogram + MRI alternating |
Breast cancer early detection through systematic screening remains the most powerful tool for achieving that 99% cure rate for invasive ductal carcinoma.
Building Your Care Team: Essential Specialists
Invasive ductal carcinoma treatment requires coordination among multiple specialists. Your core team typically includes a breast surgeon, medical oncologist, radiation oncologist, and pathologist. Additional support from nutritionists, physical therapists, and mental health professionals optimizes treatment tolerance and recovery.
Support Resources for IDC Patients & Families
Emotional support proves as essential as medical treatment. Organizations provide free resources, including the American Cancer Society’s 24/7 helpline, online support communities, and local support groups connecting newly diagnosed patients with survivors.
Questions to Ask at Every Oncology Appointment
Essential questions for your oncology team:
- What is my specific invasive ductal carcinoma stage and grade?
- What are my hormone receptor and HER2 status results?
- What invasive ductal carcinoma treatment options do you recommend and why?
- What are the expected outcomes and potential side effects?
- Are there clinical trials appropriate for my situation?
- How will treatment affect my daily activities and work?
- What lifestyle modifications can improve my prognosis?
Explore additional health tips and resources to support your overall wellness journey beyond cancer treatment.
What This Means For You: An invasive ductal carcinoma diagnosis marks the beginning of your treatment journey, not the end of your story. With 99% five-year survival rates for early-stage disease, modern medicine offers extraordinary hope. Take time to understand your diagnosis, assemble a trusted medical team, and remember that millions of women have successfully overcome IDC breast cancer and returned to full, vibrant lives. Your proactive engagement in screening, treatment decisions, and lifestyle modifications directly influences your outcomes. You are not alone in this journey.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult with qualified healthcare professionals regarding any medical condition, diagnosis, or treatment decisions. Individual results may vary based on specific medical circumstances.
Frequently Asked Questions about Invasive Ductal Carcinoma
1. What is invasive ductal carcinoma?
Invasive ductal carcinoma (IDC) is the most common type of breast cancer, accounting for 70-80% of all cases. It starts in the milk ducts and breaks through the duct wall to invade surrounding breast tissue.
2. What is the survival rate for invasive ductal carcinoma?
The invasive ductal carcinoma survival rate is 99% for Stage 1 disease when caught early. Overall five-year survival rates are 99% for localized disease, 86% for regional spread, and 31% for distant metastasis.
3. Can invasive ductal carcinoma be cured?
Yes, invasive ductal carcinoma can be cured, especially when detected early. Stage 1 IDC has a 99% cure rate with appropriate treatment combining surgery, radiation, and systemic therapies.
4. What are the early warning signs of invasive ductal carcinoma?
Early IDC symptoms include a palpable breast lump, changes in breast size or shape, nipple discharge, skin dimpling or puckering, nipple retraction, and unexplained breast pain in one area.
5. How is invasive ductal carcinoma treated?
Invasive ductal carcinoma treatment typically includes surgery (lumpectomy or mastectomy), radiation therapy, and systemic treatments like chemotherapy, hormone therapy, or targeted drugs depending on tumor characteristics.
6. What is the difference between Stage 1 and Stage 2 invasive ductal carcinoma?
Stage 1 invasive ductal carcinoma involves tumors ≤2cm with no or minimal lymph node involvement (99% survival). Stage 2 includes tumors 2-5cm or greater lymph node involvement (93% survival).
7. Is triple-negative invasive ductal carcinoma more aggressive?
Yes, triple-negative invasive ductal carcinoma grows faster and has higher recurrence risk. However, when caught at Stage 1, it still achieves 91% five-year survival with chemotherapy and immunotherapy.
8. How long does invasive ductal carcinoma treatment take?
Treatment duration varies by stage: Stage 1 typically requires 6-12 weeks of active treatment plus 5-10 years of hormone therapy if ER-positive. Stage 2-3 may require 6-12 months of active treatment.
9. What lifestyle changes reduce invasive ductal carcinoma recurrence?
Exercise 150+ minutes weekly (reduces recurrence 25-30%), maintain healthy BMI under 25 (reduces recurrence 30-50%), limit alcohol to under 4 drinks weekly, and ensure adequate sleep of 7-9 hours nightly.
10. Should I get a second opinion for invasive ductal carcinoma?
Yes, seeking a second opinion is recommended for any cancer diagnosis, especially for treatment planning. Most insurance covers second opinions, and comprehensive cancer centers offer specialized expertise in IDC treatment options.
11. How often should I get mammograms to detect invasive ductal carcinoma early?
Average-risk women should begin annual mammograms at age 40-45. High-risk women (family history, BRCA mutations) should start at age 25-30 with mammograms plus MRI every 6-12 months for optimal breast cancer early detection.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.