On This Page – Quick Medical Summary
When Emily received her NIPT results at 11 weeks pregnant, she stared at the numbers on her patient portal for 20 minutes, heart pounding. “1 in 8,500” for Down syndrome—what did that actually mean? Was her baby okay?
Your NIPT results show your baby’s risk for chromosomal conditions through a simple blood test. Most results (99.3%) come back low-risk, meaning there’s less than a 1 in 10,000 chance of conditions like Down syndrome. High-risk results don’t mean your baby definitely has a condition—they indicate the need for confirmatory testing like amniocentesis.
Quick Takeaways:
- Timeline: Results typically arrive in 7-10 business days (some labs in 5-7 days)
- Low Risk: Less than 0.01% chance (1 in 10,000+) of chromosomal abnormalities
- High Risk: Doesn’t mean diagnosis—50-80% are false positives depending on condition
- Accuracy: 99.5% detection rate for Down syndrome, the highest of any prenatal screening
Medical Disclaimer: This article provides educational information only and is not a substitute for professional medical advice. Always consult your healthcare provider about your specific results.
The 7-Day NIPT Results Timeline: What to Expect
Understanding when your NIPT results will arrive can ease the anxiety of waiting. The timeline varies by laboratory, but 2026 averages show most results return within 7-10 business days.
When Can You Take NIPT?
NIPT requires sufficient fetal cell-free DNA in your bloodstream, which typically reaches detectable levels after 10 weeks of pregnancy. Testing before this point often results in inconclusive results due to low fetal fraction (less than 4% placental DNA).
Your healthcare provider will confirm gestational age through ultrasound before drawing blood. If you’re using a pregnancy due date calculator to track your timeline, ensure you’re at least 10 weeks from your last menstrual period before scheduling NIPT.
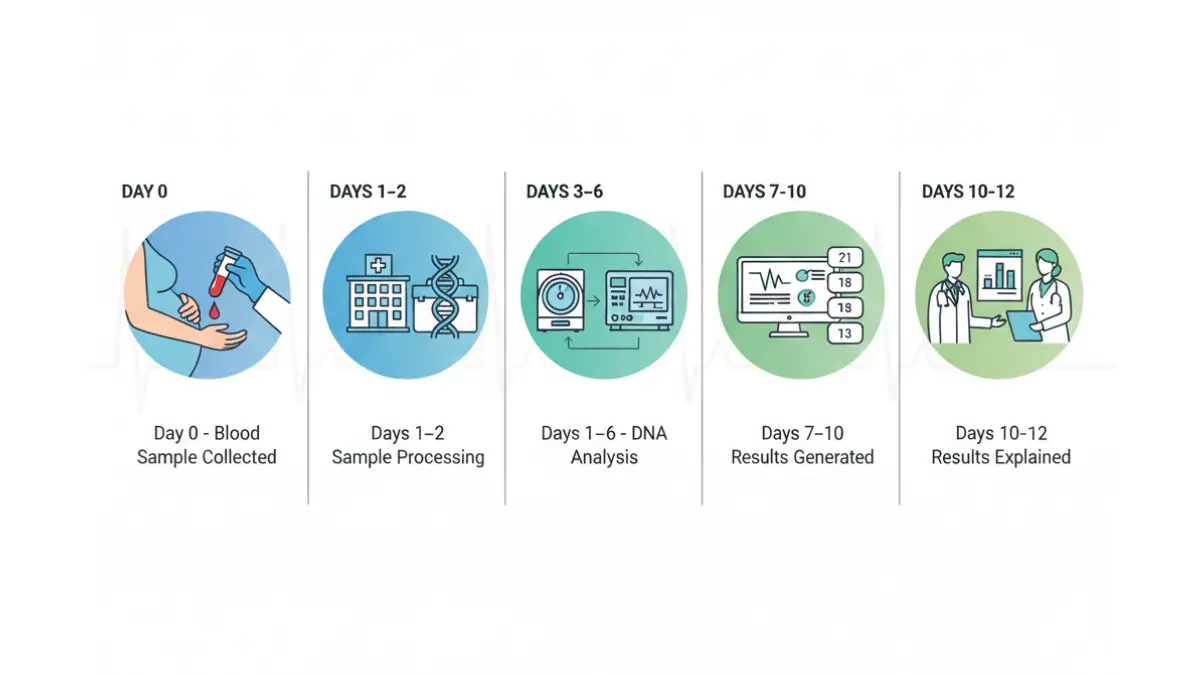
Day-by-Day Breakdown (2026 Laboratory Averages)
Day 0: Blood draw at your provider’s office (after 10 weeks gestation) Days 1-2: Sample arrives at laboratory, logged into system Days 3-6: DNA extraction, sequencing, and chromosomal analysis Days 7-10: Quality review, results sent to your healthcare provider Days 10-12: Your provider reviews results and contacts you
2026 Laboratory Comparison
| Laboratory | Average Timeline | Down Syndrome Accuracy | Twin Testing | Cost Range |
|---|---|---|---|---|
| Panorama (Natera) | 5-7 days | 99.9% | Yes (identical & fraternal) | $149-$349 |
| MaterniT 21 PLUS | 7-10 days | 99.5% | Yes (identical only) | $99-$299 |
| Harmony (Ariosa) | 7-14 days | 99.3% | Yes (both types) | $195-$495 |
| QNatal Advanced | 7-10 days | 99.1% | Limited | $250-$450 |
What Causes Delays?
Several factors can extend your waiting time beyond the standard 7-10 days:
Low Fetal Fraction: If placental DNA comprises less than 4% of your blood sample, the lab cannot generate accurate results. This affects approximately 3-8% of initial tests and is more common in early pregnancy (before 11 weeks), maternal obesity (BMI >30), or pregnancies with inadequate weight gain.
Technical Issues: Rare equipment malfunctions or sample processing errors (occurring in <1% of cases) may require retesting.
Multiple Pregnancy: Twin and triplet pregnancies require additional analysis time, potentially adding 2-3 business days.
What This Means For You: If you haven’t received results within 14 business days, contact your provider’s office. Most laboratories offer result tracking through patient portals where you can monitor processing status in real-time.
Understanding Your NIPT Results: The Numbers Explained
NIPT results come in three primary categories: low risk, high risk, or inconclusive. Each requires different interpretation and next steps.
Low Risk Results: What “<0.01%” Really Means
A low-risk NIPT result indicates your baby has less than a 1 in 10,000 chance (0.01%) of having the tested chromosomal conditions. According to the National Library of Medicine, this negative predictive value exceeds 99.99% for common trisomies.
How to Read Your Risk Score:
| Your Result | Interpretation | What It Means |
|---|---|---|
| <1 in 10,000 | Ultra-low risk | 99.99%+ chance baby is unaffected |
| 1 in 5,000-10,000 | Very low risk | 99.98% chance baby is unaffected |
| 1 in 1,000-5,000 | Low risk | 99.9% chance baby is unaffected |
| 1 in 100-1,000 | Borderline | Consider genetic counseling |
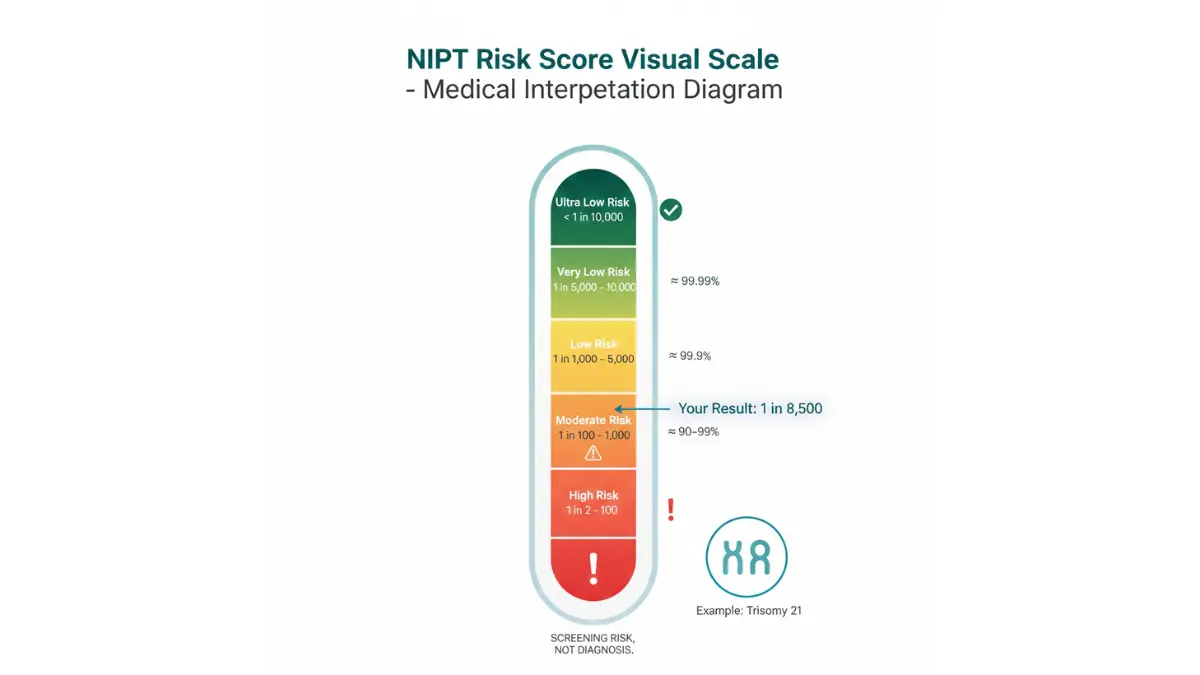
Real Example: If your trisomy 21 result shows “1 in 8,500,” this means that among 8,500 pregnancies with similar results, only 1 would actually have Down syndrome. Your baby has a 99.988% chance of not having trisomy 21.
While reassuring, low-risk results don’t eliminate all possibility of chromosomal abnormalities. You’ll still receive routine prenatal care, including the anatomy ultrasound around 20 weeks to screen for structural differences NIPT cannot detect.
High Risk Results: Don’t Panic—Here’s Why
A high-risk NIPT result (typically reported as risk greater than 1 in 100) means your pregnancy has an increased probability of a chromosomal condition. This is not a diagnosis.
The crucial factor most parents don’t understand is the positive predictive value (PPV)—the likelihood that a high-risk result represents a true positive rather than a false alarm.
False Positive Rates by Condition (2026 Data):
| Condition | NIPT Detection Rate | False Positive Rate | True Positive Likelihood |
|---|---|---|---|
| Trisomy 21 (Down syndrome) | 99.5% | 5-20% | 80-95% |
| Trisomy 18 (Edwards syndrome) | 98.9% | 40-50% | 50-60% |
| Trisomy 13 (Patau syndrome) | 96.1% | 45-55% | 45-55% |
| Sex chromosome aneuploidies | 90-95% | 30-50% | 50-70% |
These statistics reveal a critical truth: If you receive a high-risk result for trisomy 18 or 13, there’s approximately a 50% chance it’s a false positive. Even for Down syndrome, where NIPT performs best, 5-20% of high-risk results don’t reflect actual fetal abnormalities.
According to research from the American College of Medical Genetics, false positives occur due to confined placental mosaicism (chromosomal differences limited to placenta), vanishing twin syndrome, or maternal chromosomal variations.
What This Means For You: A high-risk NIPT result requires confirmatory diagnostic testing through chorionic villus sampling (CVS) or amniocentesis—tests that analyze actual fetal cells rather than placental DNA. Your provider will refer you to genetic counseling, where specialists using tools like our genetic risk assessment tool can calculate your personalized probability.
Inconclusive Results: Low Fetal Fraction Explained
Approximately 1-5% of NIPT tests return “no call” or “test failure” results, most commonly due to insufficient fetal fraction.
Common Causes:
- Testing too early (before 10 weeks)
- Maternal BMI >30
- Multiple pregnancy (triplets or higher)
- Certain maternal health conditions
Next Steps: Your provider will typically recommend retesting 1-2 weeks later. Studies show 70-80% of repeat tests succeed. If a second attempt fails, diagnostic testing (CVS or amniocentesis) becomes the recommended pathway for chromosomal assessment.
What Does NIPT Test For? Complete 2026 Screening Panel
NIPT analyzes cell-free DNA fragments circulating in maternal blood to detect chromosomal imbalances. Understanding what conditions NIPT screens for—and importantly, what it doesn’t—helps set appropriate expectations.
Common Trisomies (Highest Accuracy)
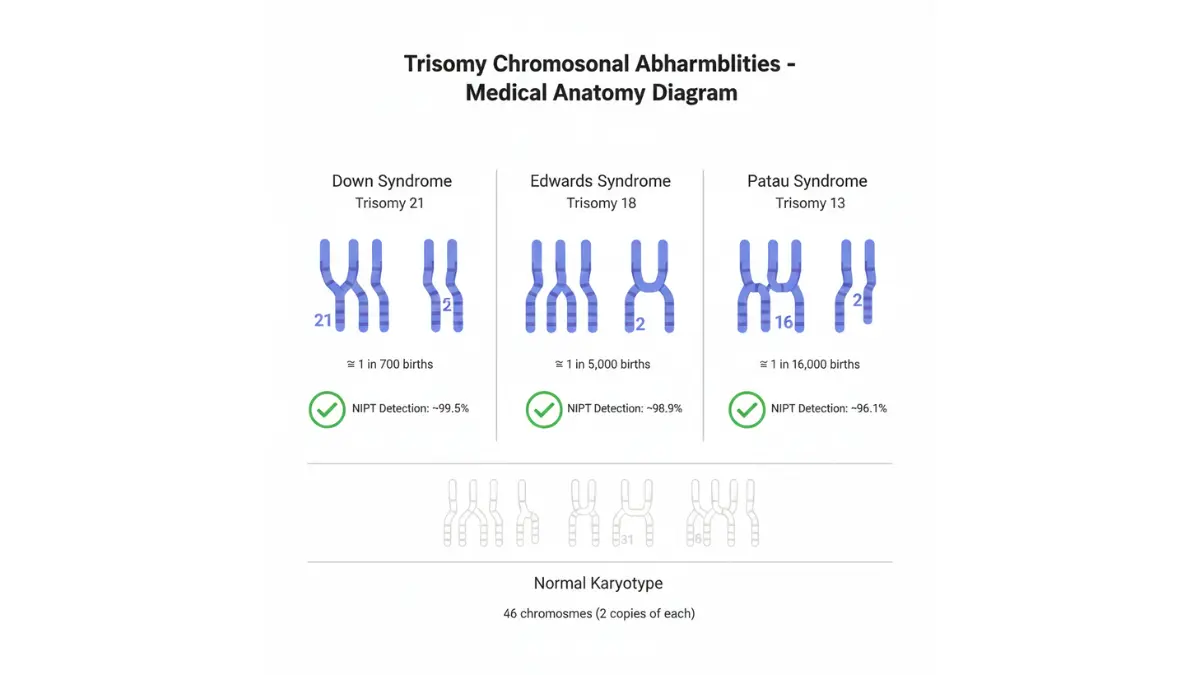
NIPT performs best when screening for conditions caused by an extra chromosome:
Trisomy 21 (Down Syndrome): The most common chromosomal condition, occurring in 1 in 700 live births. Characteristics include intellectual disability (mild to moderate), distinctive facial features, and increased risk of heart defects. NIPT detects 99.5% of Down syndrome cases with a false positive rate under 0.1%.
Trisomy 18 (Edwards Syndrome): Affects 1 in 5,000 births and causes severe developmental issues. Most babies with trisomy 18 do not survive beyond the first year. NIPT detection rate: 98.9%.
Trisomy 13 (Patau Syndrome): Occurs in 1 in 16,000 births with severe intellectual disability and physical abnormalities. NIPT detection rate: 96.1%.
Sex Chromosome Differences
NIPT can identify variations in X and Y chromosomes, though accuracy is slightly lower than for autosomal trisomies:
Turner Syndrome (Monosomy X): Affects 1 in 2,500 female births; causes short stature and infertility but often normal intelligence.
Klinefelter Syndrome (XXY): Affects 1 in 500-1,000 male births; may cause learning differences and reduced testosterone.
Triple X Syndrome (XXX): Affects 1 in 1,000 female births; usually causes mild or no symptoms.
XYY Syndrome: Affects 1 in 1,000 male births; typically no significant health issues.
Fetal Sex Determination: NIPT identifies fetal sex with 99.99% accuracy after 10 weeks, earlier than ultrasound (accurate around 18-20 weeks).
Microdeletions (Optional Extended Panels)
Some NIPT versions screen for tiny chromosomal deletions:
- 22q11.2 deletion (DiGeorge syndrome): 1 in 4,000 births
- 1p36 deletion syndrome: 1 in 5,000 births
- Cri-du-chat syndrome (5p deletion): 1 in 15,000 births
- Prader-Willi/Angelman syndromes: 1 in 12,000-20,000 births
Important Note: Microdeletion screening has significantly higher false positive rates (up to 50%) compared to trisomy screening. The American College of Obstetricians and Gynecologists recommends discussing the value and limitations of expanded panels with your provider.
What NIPT Cannot Detect
NIPT is a powerful screening tool but has important limitations:
Cannot Detect:
- Neural tube defects (spina bifida, anencephaly)
- Congenital heart defects
- Cleft lip/palate
- Clubfoot and limb abnormalities
- Most single-gene disorders (cystic fibrosis, sickle cell disease)
- Autism spectrum disorders
- Intellectual disabilities without chromosomal basis
These conditions require other screening methods, including the quad screen (for neural tube defects) and detailed anatomy ultrasound at 20 weeks. If you have concerns about specific genetic conditions in your family history, genetic counseling before pregnancy can identify appropriate testing strategies, similar to how preconception BRCA testing helps assess hereditary cancer risks.
NIPT Accuracy: The Complete Picture
| Test Type | Down Syndrome Detection | False Positive Rate | Timing |
|---|---|---|---|
| NIPT | 99.5% | 0.1% | 10+ weeks |
| First Trimester Combined Screen | 85-90% | 5% | 11-13 weeks |
| Quad Screen | 81% | 5% | 15-20 weeks |
| Sequential Screen | 90-95% | 5% | Both trimesters |
The superiority of NIPT over conventional screening has led the Centers for Disease Control and Prevention to recommend offering it to all pregnant individuals, regardless of age or risk factors—a significant change from earlier guidelines that limited NIPT to high-risk pregnancies.
What to Do After Getting Your NIPT Results
Your NIPT results dictate different care pathways depending on whether they indicate low risk, high risk, or require additional testing.
If Your Results Are Low Risk
Congratulations—this is the outcome for 99.3% of NIPT tests. Your next steps focus on routine prenatal care:
Immediate Actions:
- Continue prenatal vitamins with folic acid
- Schedule anatomy ultrasound for 18-22 weeks
- Maintain regular prenatal appointments
- Monitor fetal growth percentiles at each visit
What Low Risk Means Long-Term: While your baby has less than 0.01% chance of tested chromosomal conditions, remember that all pregnancies carry a 3-5% baseline risk of birth defects from other causes. The 20-week anatomy scan remains crucial for detecting structural abnormalities NIPT cannot identify.
You may still choose additional testing if you have specific concerns, a family history of genetic conditions, or if ultrasound findings later suggest potential issues. These are personal decisions best made with your healthcare provider’s guidance.
If Your Results Are High Risk: Your Action Plan
Receiving high-risk NIPT results triggers understandable anxiety, but remember: this is not a diagnosis. Here’s your step-by-step pathway:
Within 48 Hours:
- Schedule genetic counseling (often provided free by your insurance or NIPT laboratory)
- Request detailed result interpretation including your specific risk score and PPV
- Avoid making major decisions until you understand the false positive rates for your specific result
Week 1-2: 4. Attend genetic counseling session where specialists will:
- Explain your exact probability (accounting for age, test type, and condition)
- Discuss confirmatory testing options
- Provide unbiased information about the condition if confirmed
- Offer emotional support and resources
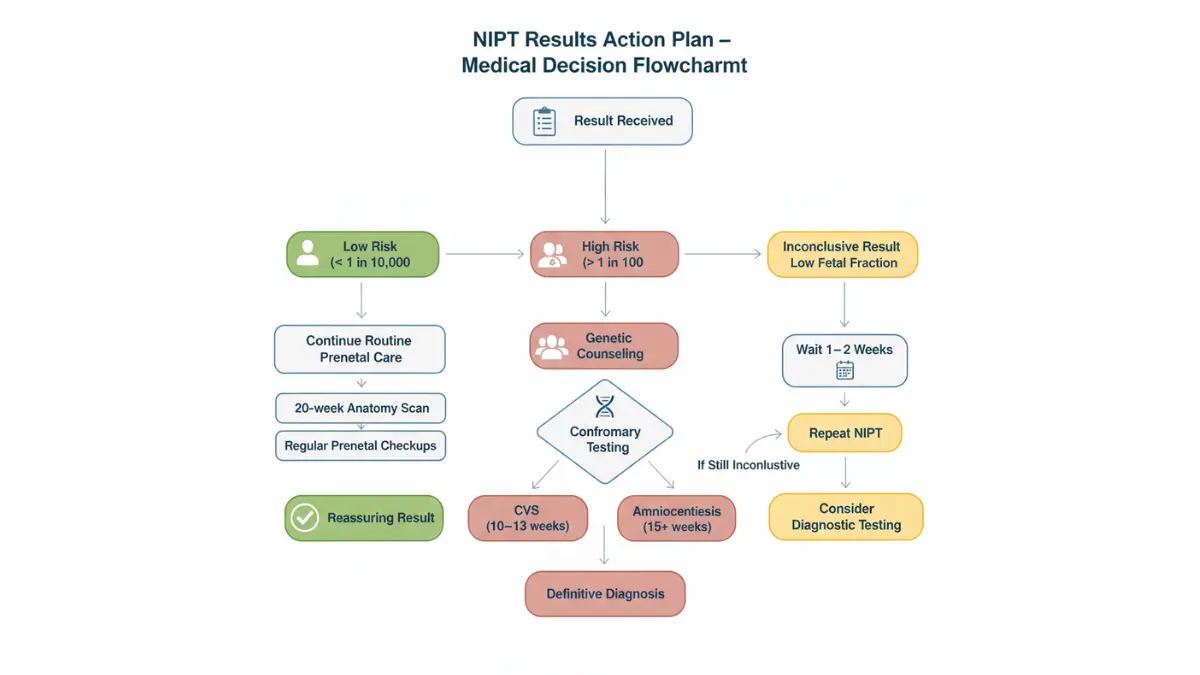
Week 2-4: 5. Decide on confirmatory testing:
| Test | Best Timing | Accuracy | Miscarriage Risk | Results Timeline | Cost |
|---|---|---|---|---|---|
| CVS | 10-13 weeks | 99%+ | 0.22-0.33% | 7-14 days | $1,500-$3,000 |
| Amniocentesis | 15+ weeks | 99%+ | 0.11-0.25% | 7-14 days | $1,500-$3,000 |
Both procedures involve inserting a thin needle through your abdomen (guided by ultrasound) to collect fetal cells for chromosomal analysis. While they carry small miscarriage risks, they provide definitive yes/no answers about chromosomal conditions.
Alternative Option: Some families choose to wait for additional ultrasound findings rather than pursue invasive testing immediately. Certain chromosomal conditions cause detectable physical markers on ultrasound that become visible later in pregnancy.
Questions to Ask Your Doctor:
- What is my baby’s exact risk score for each condition?
- What’s the positive predictive value for my age and result?
- Do you recommend CVS or amniocentesis in my situation?
- What are my insurance coverage options for confirmatory testing?
- What support resources are available regardless of my decision?
- If the condition is confirmed, what does this mean for my baby’s quality of life?
- What is the timeline for making decisions about continuing the pregnancy?
Emotional Support: High-risk results cause significant stress regardless of outcome. Consider:
- Professional genetic counseling (covered by most insurance)
- Support groups through organizations like the National Down Syndrome Society
- Talking with families who have children with the condition in question
- Mental health support through your healthcare system
- Maintaining healthy sleep patterns and stress management during this period
Research shows that 30-40% of people who receive high-risk NIPT results for rare trisomies ultimately have unaffected babies after confirmatory testing—emphasizing why diagnostic tests are essential before making major pregnancy decisions.
If Results Are Inconclusive
An inconclusive NIPT result typically stems from insufficient fetal DNA (low fetal fraction) and occurs in 1-5% of tests.
Immediate Steps:
- Wait 1-2 weeks for fetal DNA levels to increase
- Repeat NIPT (usually free from the same laboratory)
- If repeat fails, consider diagnostic testing (CVS or amniocentesis)
Success Rates: Approximately 70-80% of repeat NIPT tests after low fetal fraction succeed in generating results.
Important Consideration: While most inconclusive results simply reflect timing or technical factors, research indicates slightly higher rates of chromosomal abnormalities in pregnancies with persistent low fetal fraction. Your provider may recommend proceeding directly to diagnostic testing if a second NIPT attempt fails.
Common Questions About NIPT Results (2026)
1. How accurate is NIPT for Down syndrome?
NIPT detects 99.5% of Down syndrome cases with a false positive rate under 0.1%, making it significantly more accurate than conventional prenatal screening methods like the quad screen (81% detection rate) or first-trimester combined screen (85-90% detection rate).
However, “99.5% accurate” requires context. This refers to sensitivity—the test’s ability to identify affected pregnancies. The positive predictive value (likelihood a high-risk result represents true Down syndrome) varies by maternal age: approximately 95% for women over 40, but closer to 80% for women under 30. This difference stems from Down syndrome’s increased baseline prevalence with advanced maternal age.
2. Can NIPT results be wrong?
Yes. NIPT is a screening test, not diagnostic testing. False positives occur when results indicate high risk but confirmatory testing reveals the baby doesn’t have the condition. False positive rates range from 0.1% for Down syndrome to 45-55% for trisomy 13.
False negatives (test shows low risk but baby has the condition) are rare but possible, occurring in approximately 0.5-1.5% of affected pregnancies. This is why NIPT results should be confirmed with amniocentesis or CVS before making major medical decisions.
The American College of Medical Genetics emphasizes that NIPT analyzes placental DNA, not fetal DNA directly. Chromosomal differences confined to the placenta (confined placental mosaicism) can produce results that don’t reflect the baby’s actual chromosomes.
3. What does “low fetal fraction” mean?
Low fetal fraction indicates that less than 4% of cell-free DNA in your blood sample comes from the placenta. Without sufficient placental DNA, laboratories cannot reliably distinguish fetal chromosomal patterns from maternal patterns.
Common Causes:
- Testing before 10 weeks of pregnancy (most common)
- Maternal obesity (BMI >30)
- Certain medications like heparin or low-molecular-weight heparin
- Multiple pregnancy with three or more fetuses
- Suboptimal blood sample handling
Solution: Most cases resolve by retesting 1-2 weeks later. As pregnancy progresses and the placenta grows, fetal fraction increases. Studies show 70-80% success rates for repeat NIPT after initial low fetal fraction.
When to Worry: Persistently low fetal fraction (failing two NIPT attempts) occurs in <1% of pregnancies but may signal placental issues or, rarely, chromosomal abnormalities. Your provider may recommend proceeding to diagnostic testing.
4. How long do NIPT results take?
Average turnaround time in 2026 is 7-10 business days from the date the laboratory receives your blood sample. Some laboratories offer faster results:
- Panorama by Natera: 5-7 business days (fastest option)
- MaterniT 21 PLUS: 7-10 business days (most widely used)
- Harmony: 7-14 business days (reliable for twins)
Your healthcare provider receives results first, then contacts you to discuss findings. Many medical systems now provide patient portal access where you can view results as soon as they’re released, though we recommend discussing them with your provider for proper interpretation.
5. What’s the difference between high risk and positive?
This distinction is crucial: “High risk” comes from screening tests like NIPT, indicating increased probability. “Positive” comes from diagnostic tests like amniocentesis, confirming the condition exists.
NIPT High Risk: Your baby has a higher-than-average chance of a chromosomal condition, but this is not confirmation. Depending on the condition, 5-55% of high-risk NIPT results are false positives.
Diagnostic Positive: Amniocentesis or CVS analyzes actual fetal chromosomes and provides yes/no answers with >99% accuracy. A positive diagnostic result confirms your baby has the chromosomal condition.
Think of NIPT as a smoke detector—it alerts you to potential problems requiring investigation. Diagnostic testing is the fire inspection that confirms whether there’s actually a fire.
6. Does insurance cover NIPT?
Coverage varies significantly based on your insurance plan and medical indications:
Typically Covered:
- Women 35 or older at delivery
- Previous pregnancy with chromosomal abnormality
- Ultrasound findings suggesting increased risk
- Abnormal conventional screening results
- Family history of chromosomal conditions
Variable Coverage:
- Average-risk pregnancies under age 35 (some insurers cover, others don’t)
- Extended panels testing for microdeletions
- Repeat testing after inconclusive results
Out-of-Pocket Costs (2026):
- With insurance: $0-$500 (depending on plan)
- Without insurance: $300-$800 (most labs offer self-pay discounts)
- Financial assistance available from most laboratories for qualified patients
Always verify coverage with your insurance before testing. Most NIPT companies provide pre-authorization services and will inform you of expected costs before processing your sample.
7. Can NIPT detect all birth defects?
No. NIPT specifically screens for chromosomal conditions—situations where there are extra or missing chromosomes, or pieces of chromosomes. It cannot detect:
Structural Birth Defects:
- Heart defects (affecting 1 in 100 babies)
- Neural tube defects like spina bifida
- Cleft lip and palate
- Clubfoot or limb abnormalities
- Kidney or urinary tract issues
- Gastrointestinal malformations
Single-Gene Disorders:
- Cystic fibrosis
- Sickle cell disease
- Thalassemia
- Muscular dystrophy
- Most metabolic disorders
These conditions require other screening methods: quad screen for neural tube defects, carrier screening for single-gene disorders, and detailed anatomy ultrasound around 20 weeks for structural abnormalities. Comprehensive prenatal screening involves multiple tests at different stages, similar to how multiple blood tests assess different aspects of health.
8. Is NIPT safe for twins?
Yes, NIPT is completely safe for twin pregnancies. The blood draw poses no risk to either baby. Accuracy depends on twin type:
Identical Twins: NIPT accuracy matches singleton pregnancy accuracy (99%+) because identical twins share DNA. If one twin has a chromosomal condition, both typically do.
Fraternal Twins: Slightly lower accuracy because each twin has distinct DNA from separate placentas. If one twin is affected and the other isn’t, NIPT may return high-risk results without indicating which twin is affected or if both are unaffected. Some newer NIPT versions can analyze each twin separately.
Not Suitable For: NIPT is not validated for triplet or higher-order multiple pregnancies. These situations require alternative screening approaches.
9. When should I take NIPT?
NIPT requires at least 10 weeks of pregnancy, measured from the first day of your last menstrual period. Before 10 weeks, placental DNA levels are typically too low for accurate analysis.
Optimal Timing: 10-13 weeks provides the best balance of:
- Sufficient fetal fraction for accurate results
- Early enough for results before second-trimester diagnostic testing windows
- Time to consider all options if results are high risk
You can take NIPT later in pregnancy (some women do so after abnormal conventional screening results), but earlier testing provides more decision-making time. Confirm your dating through ultrasound before NIPT—incorrect gestational age calculation is a common cause of low fetal fraction results. Use our pregnancy due date calculator as a starting point, but ultrasound provides the most accurate dating.
10. What happens if I get a high-risk result?
A high-risk NIPT result initiates a specific care pathway designed to provide support and definitive answers:
Immediate: Your healthcare provider will contact you (usually within 24-48 hours of receiving results) to discuss findings and schedule genetic counseling.
Week 1: Attend genetic counseling where specialists explain your specific risk score, discuss the condition in question, review confirmatory testing options, and provide emotional support resources.
Week 2-4: Decide whether to pursue diagnostic testing (CVS at 10-13 weeks or amniocentesis at 15+ weeks). These tests provide yes/no answers with >99% accuracy but carry small miscarriage risks (0.1-0.3%).
Ongoing: Regardless of your decisions about further testing, you’ll receive additional ultrasound monitoring and access to support resources. Many hospitals offer perinatal support teams including maternal-fetal medicine specialists, genetic counselors, social workers, and mental health professionals.
Important: Don’t make major pregnancy decisions based solely on NIPT results. Confirmatory testing is essential because false positive rates for some conditions exceed 50%.
11. Can NIPT tell me my baby’s sex?
Yes, with 99.99% accuracy after 10 weeks of pregnancy. NIPT identifies fetal sex by detecting Y chromosome DNA in maternal blood. Y chromosome presence indicates male fetus; absence (with sufficient fetal fraction) indicates female fetus.
This is significantly earlier and more accurate than ultrasound sex determination, which isn’t reliable until 18-20 weeks and has 95-99% accuracy depending on baby’s position and image quality.
Options: You can choose to:
- Learn your baby’s sex from NIPT results
- Request results without sex information (marked on requisition form)
- Have sex results sent to a third party for gender reveal planning
- Wait for ultrasound confirmation
Some families use early sex determination for medical reasons (X-linked genetic conditions affect males and females differently) rather than simple curiosity.
Final Thoughts
NIPT results provide valuable information about your baby’s chromosomal health, but they’re one piece of comprehensive prenatal care. Low-risk results offer reassurance while high-risk results require confirmatory testing before any major decisions. Remember that 99.3% of NIPT tests return low-risk results, and even among high-risk results, many are false positives.
Work closely with your healthcare provider to understand your specific results, access genetic counseling when needed, and make informed decisions that align with your values and circumstances. Whether your results are low risk or high risk, you deserve clear information, compassionate support, and time to process this important aspect of your pregnancy journey.
References:
- American College of Obstetricians and Gynecologists (ACOG). Screening for Fetal Chromosomal Abnormalities. Practice Bulletin 226. 2020 (Reaffirmed 2025).
- American College of Medical Genetics and Genomics. Noninvasive Prenatal Screening for Fetal Aneuploidy. 2023 Update.
- National Library of Medicine, MedlinePlus. Noninvasive Prenatal Testing (NIPT). Updated January 2026.
- Centers for Disease Control and Prevention. Birth Defects: Data & Statistics. 2026.
For personalized medical advice about your NIPT results, schedule a consultation with your healthcare provider or genetic counselor.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.