On This Page – Quick Medical Summary
Quick Answer: A c-section (cesarean section) is major abdominal surgery used to deliver a baby when vaginal birth is unsafe or impossible. According to the CDC National Vital Statistics Report (2025), 32.3% of all U.S. births in 2023 were cesarean deliveries — that’s 1 in 3 babies. Recovery takes 6–8 weeks physically and up to 3 months fully. This guide covers what actually happens, what the real risks are, and what most medical websites leave out.
What Is a C-Section? The Real, Complete Answer
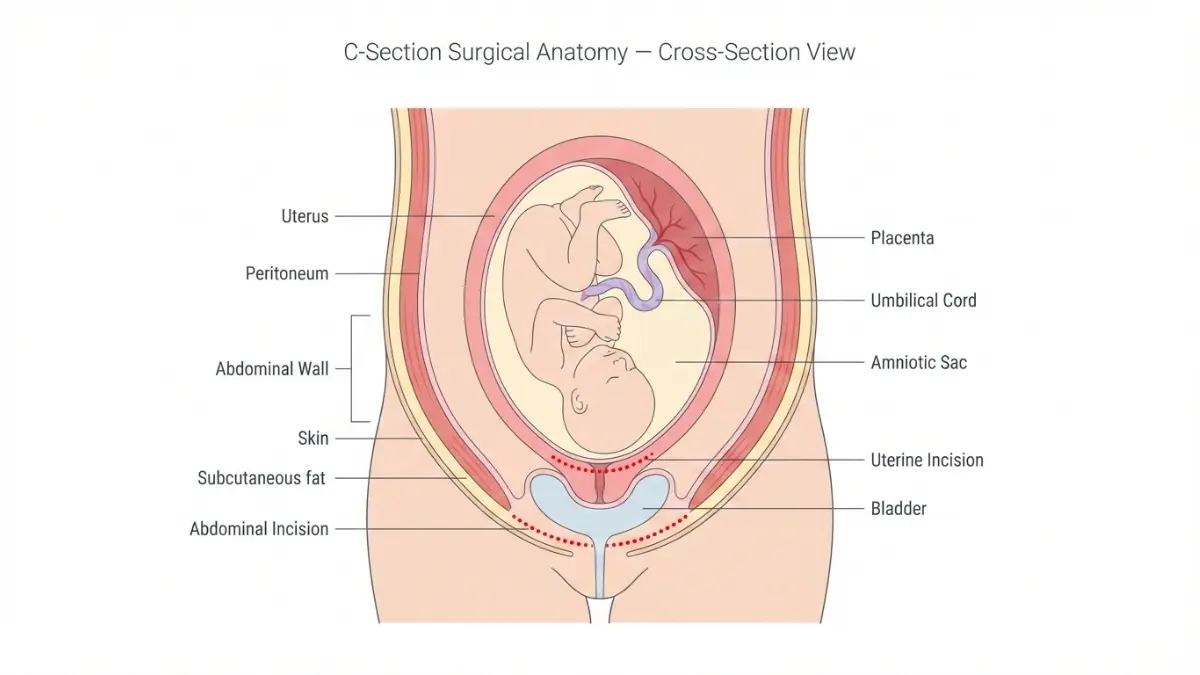
A c-section, or cesarean section, is a surgical procedure in which your baby is delivered through two incisions — one through your abdomen and one through your uterus. It is performed when vaginal delivery is unsafe for you, your baby, or both.
According to CDC birth data, the cesarean delivery rate in the United States was 32.3% in 2023, rising 1% from the prior year. Globally, the World Health Organization projects c-section rates will reach 28.5% worldwide by 2030.
This is one of the most common surgical procedures in the United States — yet most women feel underprepared for what it truly involves.
The Two Types of C-Section
Planned (elective) c-section:
- Scheduled in advance due to a known medical condition
- Examples: breech position, placenta previa, previous classical uterine incision
- You arrive at the hospital calm, fasted, and prepared
Emergency c-section:
- Performed urgently when complications arise during labor
- Examples: fetal distress, cord prolapse, stalled labor
- Decision to delivery can happen in as little as 30 minutes
What Actually Happens in the OR — Minute by Minute
Most guides summarize this in two sentences. Here is what actually happens:
| Step | What Happens | Time |
|---|---|---|
| 1. Prep | IV line, catheter, abdominal shave, antiseptic wash | ~15 min |
| 2. Anesthesia | Spinal block or epidural administered | ~10 min |
| 3. Drape placed | Surgical screen positioned; you are awake but numb | Immediate |
| 4. Incision | Horizontal “bikini cut” made just above pubic hairline | ~2 min |
| 5. Uterine incision | Second incision into lower uterine segment | ~1 min |
| 6. Baby delivered | Baby guided out; cord clamped | ~2–5 min |
| 7. Placenta removed | Placenta manually extracted | ~3 min |
| 8. Closure | Multiple layers sutured closed | ~30–40 min |
| Total | 45–60 minutes in routine cases | — |
What you will feel: No pain. But expect significant pressure, tugging, and pulling when your baby is delivered. Your legs may shake involuntarily from the anesthesia. The operating room will be cold. These sensations are completely normal.
What competitors miss: Emergency c-sections involving complications — including adhesions from a prior surgery, excessive bleeding, or fetal positioning challenges — can extend to 2 hours or more, sometimes requiring general anesthesia.
Use our Pregnancy Due Date Calculator to map your full pregnancy timeline and understand when a scheduled c-section would typically fall in your third trimester.
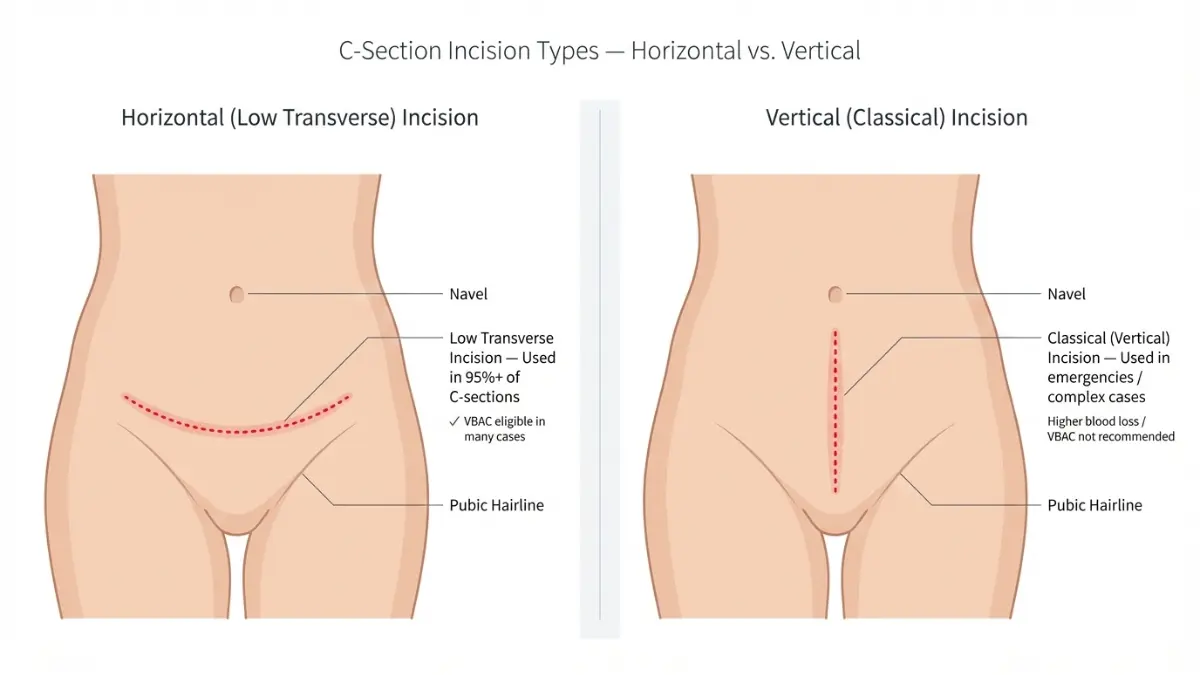
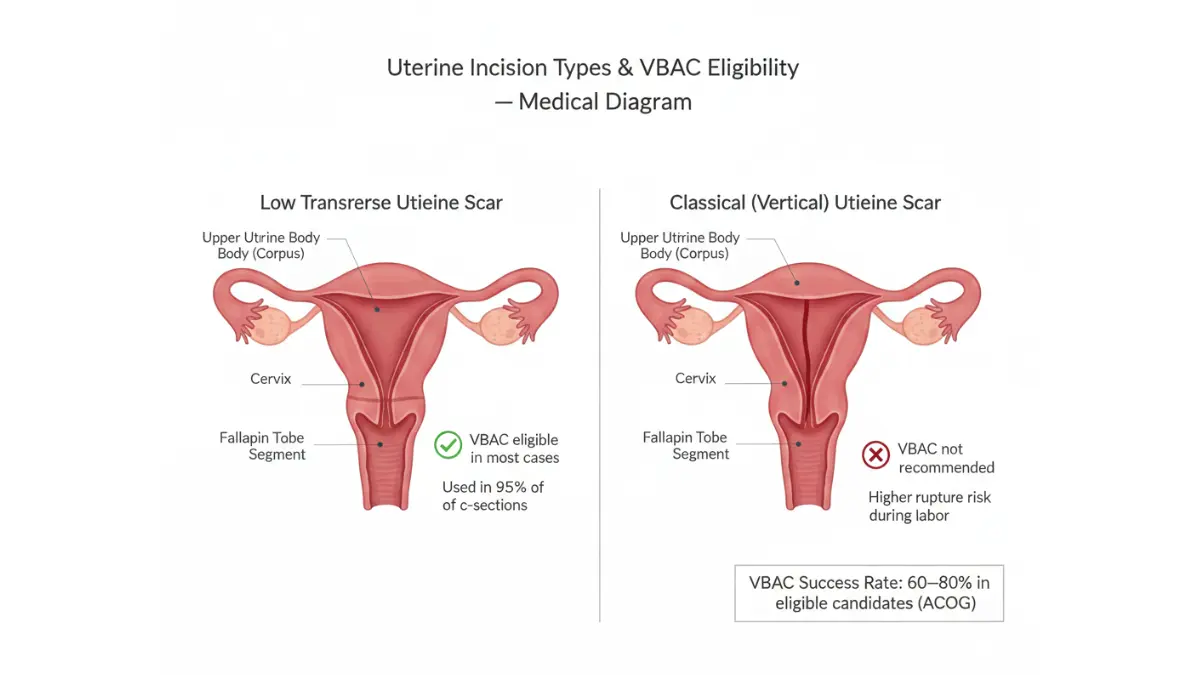
Horizontal vs. Vertical Incision
- Horizontal (low transverse): Used in 95%+ of c-sections. Heals well. Less blood loss. Enables VBAC in future pregnancies.
- Vertical (classical): Reserved for severe emergencies, very preterm babies, or transverse fetal lie. Higher blood loss. Rules out future VBAC.
Your OB-GYN will decide incision type based on your specific circumstances.
9 Medical Reasons a C-Section Is Recommended
Not all c-sections are equal. Some are lifesaving emergencies. Others are scheduled weeks in advance. Understanding why your doctor recommends one helps you ask better questions.
Emergency Indications — Non-Negotiable
These conditions require immediate cesarean delivery:
- Fetal distress — Abnormal heart rate patterns signaling oxygen deprivation
- Umbilical cord prolapse — Cord slips through cervix before baby; a true obstetric emergency
- Placental abruption — Placenta separates from uterine wall prematurely
- Uterine rupture — A tear in the uterine wall; life-threatening for mother and baby
- Maternal hemorrhage — Severe bleeding that cannot be controlled with medication
Planned Indications — Scheduled in Advance
These are medically planned before or early in labor:
- Breech or transverse position — Baby is not head-down by 36–37 weeks
- Placenta previa — Placenta covers the cervical opening
- Prior c-section with classical incision — High risk of uterine rupture in labor
- Multiple pregnancies — Twins in certain positions, triplets, or more
The Grey Zone: What Doctors Don’t Always Fully Explain
This is where most websites stop. Here is what the research actually shows:
“Failure to progress” is the most common reason given for an unplanned c-section. Yet the American College of Obstetricians and Gynecologists (ACOG) notes that this diagnosis is sometimes applied before the recommended waiting period has elapsed — particularly in first-time mothers.
Maternal request c-sections are rising globally. In the U.S., some women choose elective cesarean for personal, psychological, or scheduling reasons. The decision is complex, ethically nuanced, and should always involve full informed consent about surgical risks.
Health equity matters: According to the 2025 State of Maternal Health report, Black women are 25% more likely to deliver via c-section than white women, placing them at disproportionate risk for the surgical complications described in Section 3.
Women tracking maternal health can use our Pregnancy Weight Gain Calculator to monitor recommended ACOG weight targets throughout pregnancy — a factor that influences c-section risk.
C-Section Risks — What Most Websites Understate
This is the section that separates a genuinely useful medical article from a sanitized overview. C-sections are safe and often lifesaving — but they are major surgery. The risks deserve honest, complete coverage.
Immediate Short-Term Risks (For the Mother)
| Risk | Estimated Frequency | What to Watch For |
|---|---|---|
| Wound infection | ~6–8% | Redness, warmth, discharge at incision |
| Hemorrhage | ~1–3% | Soaking pads hourly, dizziness, pallor |
| Blood clot (DVT/PE) | ~0.5–1% | Leg swelling, chest pain, shortness of breath |
| Urinary tract infection | ~5% | Burning, fever, frequent urination |
| Bladder or bowel injury | Rare (<1%) | Blood in urine, bowel changes |
| Anesthesia reaction | Very rare | Nausea, headache (spinal headache 1–5%) |
Risks for the Baby
- Transient tachypnea (wet lung): Babies born by c-section miss the chest compression of the birth canal that squeezes fluid from their lungs. Up to 5–7% of c-section newborns experience temporary breathing difficulty.
- Accidental surgical nick: Rare, occurring in approximately 1–2 per 1,000 c-sections.
- Microbiome differences: Emerging 2025 research shows c-section babies are exposed to fewer maternal vaginal bacteria at birth, which may affect early immune development. Research is ongoing.
Long-Term Risks — What Gets Left Off Most Lists
A landmark November 2025 scoping review published in the Journal of Clinical Medicine, covering 42 studies from 2015–2025, confirmed several underreported long-term complications. This research is not cited by any of the top-ranking competitor articles.
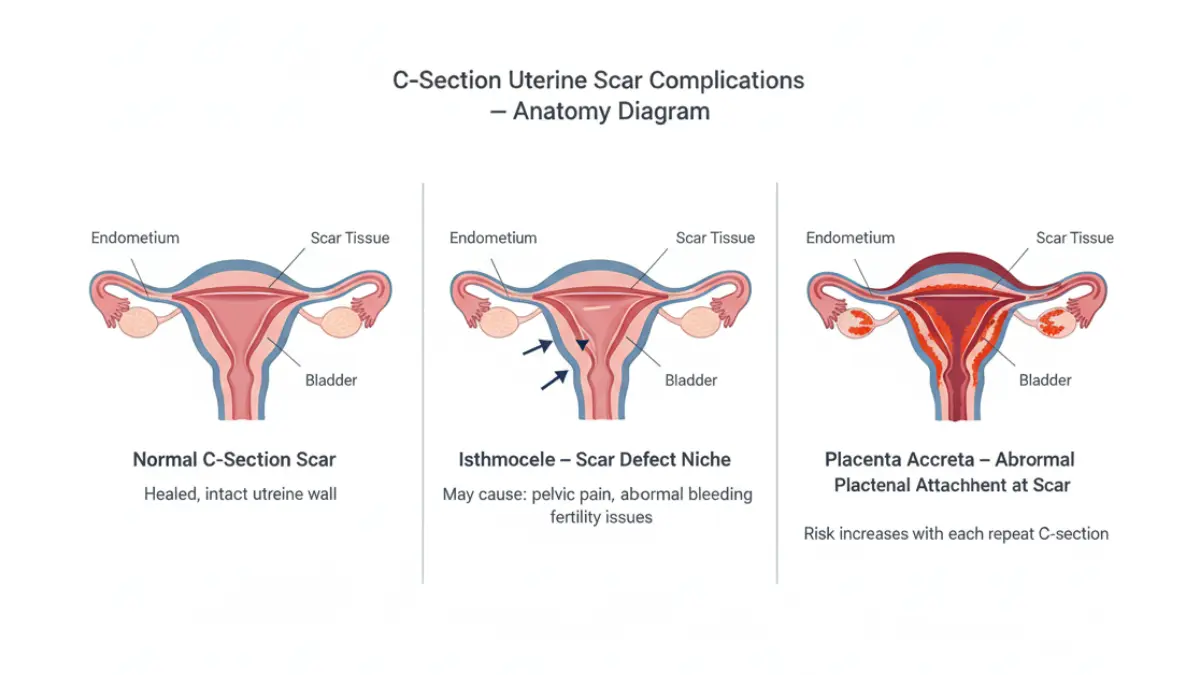
Isthmocele (Cesarean Scar Defect)
- A pouch-like niche that forms at the uterine scar site
- Can cause: abnormal uterine bleeding, chronic pelvic pain, dyspareunia, and infertility
- Risk increases significantly with each repeat cesarean
Adhesions
- Internal scar tissue bands that develop after any abdominal surgery
- After a c-section: can bind the uterus, bladder, and bowel together
- Complicate every future abdominal surgery — including repeat c-sections
- Severity increases with each procedure
Chronic Surgical Pain
- 18.3% of women report chronic pain at the incision site at 3 months post-op
- 6.8% still report surgical pain at 12 months
- Largely underreported and undertreated
Placenta Accreta Spectrum
- In repeat c-sections, the placenta can abnormally attach to or grow through the uterine scar
- Risk after 1st c-section: ~0.3%. After 3rd c-section: up to 0.57–2.13%
- Can require emergency hysterectomy to control bleeding
What This Means For You: If this is not your first c-section, have an explicit conversation with your OB-GYN before 36 weeks about the specific risks of repeat cesarean, including placenta accreta screening. This discussion saves lives.
For related surgical recovery information, our article on laparoscopic surgery recovery covers abdominal healing principles that apply broadly to post-surgical recovery.
How Many C-Sections Is Safe?
Most OB-GYNs recommend a maximum of 3 c-sections as a general clinical guideline. The cumulative risk from adhesions, placenta accreta, bladder injury, and hemorrhage rises substantially after the third procedure.
Some women safely have 4 or more — but this requires careful specialist planning, advanced imaging, and delivery at a center equipped to handle complex obstetric surgery.
What Is a Gentle C-Section? The 2025 Revolution
If you have a planned c-section, this is the section that could transform your entire birth experience. And it is the section that none of the top-ranking competitor articles — including Mayo Clinic, Healthline, and WebMD — cover in any meaningful way.
What Makes a Gentle C-Section Different
A gentle c-section (also called a family-centered or natural cesarean) is a modified surgical protocol designed to make the birth feel less clinical and more connected — without compromising safety.
Key differences from a standard c-section:
| Feature | Standard C-Section | Gentle C-Section |
|---|---|---|
| Surgical drape | Opaque — you see nothing | Clear or lowered so you see the birth |
| Baby delivery | Rapid extraction | Slow, controlled delivery mimics vaginal birth |
| Skin-to-skin contact | Often delayed 1–2+ hours | Immediate in the OR |
| Cord clamping | Immediate | Delayed (60+ seconds) |
| Music/environment | Standard OR sounds | Parents’ choice of music, softer lighting |
| Dad/partner role | Observing at distance | Often positioned to see baby emerge |
What the 2025 Data Shows
Dr. Cindy Celnik, OB-GYN, noted in an American Medical Association report that as of 2025, enhanced recovery c-section protocols are “more common to see at hospitals outside of HCA Healthcare, but it’s still not the norm” across the U.S. healthcare system.
This means: the option exists at most major hospitals — but you may need to ask for it.
Can You Request a Gentle C-Section?
Yes — if:
- Your c-section is planned (not an emergency)
- Your hospital has the protocol in place
- You are medically stable
Questions to ask your OB-GYN:
- “Does this hospital offer family-centered cesarean protocols?”
- “Can we discuss delayed cord clamping for my c-section?”
- “Is immediate skin-to-skin contact possible during my procedure?”
- “Can my partner be positioned to see the birth?”
Not suitable for: Emergency c-sections, cases requiring general anesthesia, or complex surgical presentations.
What This Means For You: If you are scheduled for a planned c-section, raise the gentle c-section option at your 36-week appointment. Most hospitals can accommodate it with 1–2 weeks of advance notice.
To plan your pregnancy timeline and prepare your birth plan calendar, use our Pregnancy Due Date Calculator and Fetal Growth Percentile Calculator.
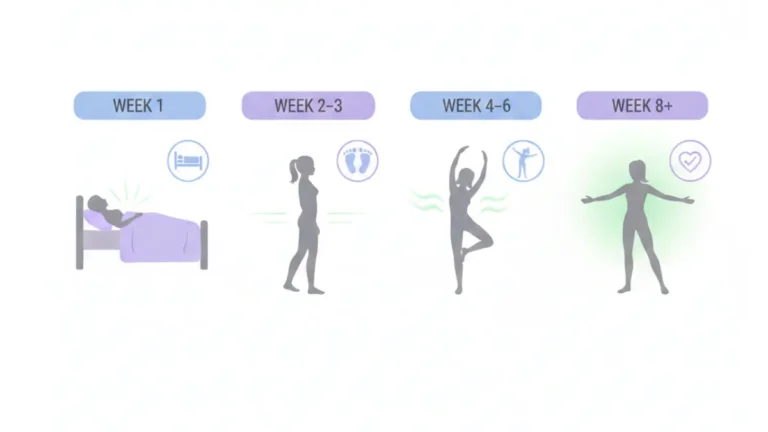
C-Section Recovery — A Week-by-Week Truth
Most sources say “6 weeks.” That is accurate but incomplete. Many women feel like something is wrong at week 4 or 5 because they expected to feel normal. You will not feel normal at 6 weeks. Here is the honest recovery timeline.
In Hospital: Days 1–3
Day 1:
- Anesthesia wears off 4–6 hours post-surgery
- You will be encouraged to walk (assisted) within 24 hours — this is critical for preventing blood clots and restarting bowel function
- Catheter typically removed after 12–24 hours
- Pain is managed with scheduled ibuprofen + acetaminophen, with stronger options for breakthrough pain
Day 2–3:
- First bowel movement may not occur until Day 2–4 — completely normal
- Stool softeners are frequently recommended; ask your nurse if not offered
- Vaginal bleeding (lochia) begins — expected to last 4–6 weeks
- Breastfeeding: Use the football hold or side-lying position to avoid pressure on the incision
- Most women are discharged after 2–4 days
Week 1 at Home — The Hardest Week
Physical reality:
- Incision is raised, slightly puffy, and darker than your skin tone — all normal
- Avoid lifting anything heavier than your baby
- Driving is prohibited — minimum 4–6 weeks (U.S.) / until emergency stop is pain-free (NHS/UK guidance)
- Gas pain can be significant; short walks help more than lying still
- Shower (not bathe) daily; keep incision dry and clean
Emotional reality:
- “Baby blues” peak in Week 1, driven by rapid hormone shifts
- Feeling overwhelmed, tearful, or anxious is normal for up to 2 weeks
- If intense sadness persists beyond 2 weeks, discuss postpartum depression with your provider — 1 in 8 U.S. women develop PPD (CDC)
Weeks 2–3: Gradual Improvement
- 2-week postpartum check: Your OB inspects the incision and monitors recovery. Bring your full list of questions.
- Energy begins to return — but overexertion is the #1 setback cause in this phase
- Scar care begins: gentle patting dry, avoiding friction from waistbands
- Light walking encouraged; no vigorous exercise
- Many women can begin gentle pelvic floor exercises (Kegels) by Week 2–3
Weeks 4–6: Nearing Normal
- Most daily activities become manageable
- Postpartum bleeding typically stops or becomes very light
- Driving: most doctors clear patients around Week 4–6 if pain-free
- Breastfeeding positions become more comfortable as incision sensitivity decreases
The 6-Week Check — And What It Doesn’t Mean
Your 6-week appointment does not mean full recovery. It means clearance for most daily activities. Here is what the data shows about actual healing timelines:
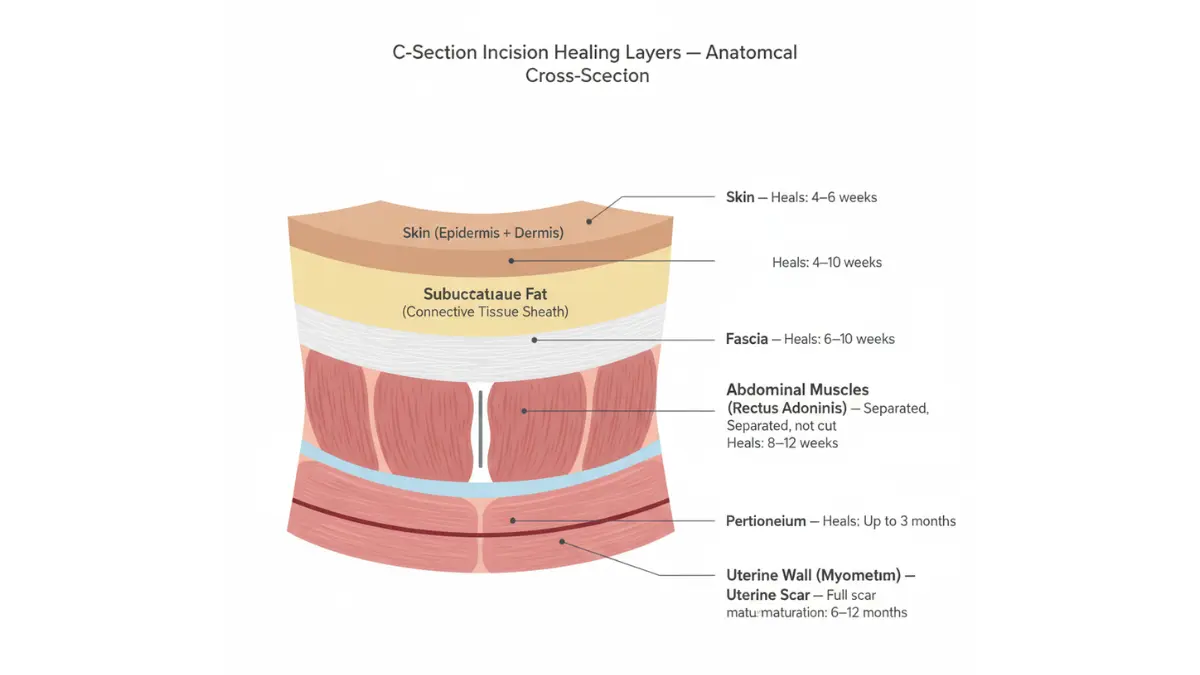
| Area Healing | Timeline |
|---|---|
| Skin/surface incision | 4–6 weeks |
| Abdominal muscle layers | 8–12 weeks |
| Uterine incision | Up to 3 months |
| Full internal scar maturation | 6–12 months |
| High-impact exercise safety | 12 weeks minimum (most guidelines) |
What This Means For You: If you still feel soreness, pulling, or fatigue at 8 or 10 weeks — you are not failing. You are healing from major surgery. Return to high-impact workouts only after 12 weeks and with your OB’s explicit clearance.
Postpartum nutrition tip: Protein supports tissue repair after surgery. Our Protein Intake Calculator and Water Intake Calculator can help you build a recovery nutrition plan, especially if breastfeeding.
For sleep optimization during recovery, our Sleep Calculator can help you structure rest around your newborn’s feeding schedule.
When to Call Your Doctor Immediately
Contact your provider the same day if you experience:
- Fever above 100.4°F (38°C)
- Soaking a pad in under 1 hour
- Red, warm, swollen, or discharging incision
- Foul-smelling vaginal discharge
- Chest pain or shortness of breath (possible pulmonary embolism)
- Swelling or pain in one leg (possible blood clot)
- Severe worsening abdominal pain
- Persistent dark or hopeless feelings (postpartum depression)
Do not wait for your 6-week appointment if any of these symptoms appear. Early treatment prevents serious complications.
C-Section vs. Vaginal Birth + VBAC Guide
Making an informed birth plan means understanding both paths — not just one. Here is what the evidence actually shows.
Head-to-Head Comparison
| Factor | C-Section | Vaginal Birth |
|---|---|---|
| Surgery type | Major abdominal surgery | Natural process |
| Average OR / labor time | 45–60 min (surgery) | 6–24+ hrs (labor) |
| Hospital stay | 2–4 days | 1–2 days |
| Recovery (full) | 6–12 weeks | 2–6 weeks |
| Main pain type | Post-surgical incision pain | Labor/perineal pain |
| Blood clot risk | Higher | Lower |
| Future pregnancy impact | Accreta, adhesion risk | Lower risk |
| Breastfeeding start | Slight delay common | Immediate |
| Baby breathing at birth | Higher temporary risk | Lower |
| Baby gut microbiome | Different bacterial seeding | Vaginal flora exposure |
Bottom line: Neither delivery method is universally “better.” The right choice is always the one that is safest for your specific clinical situation.
What Is VBAC — and Is It Right for You?
VBAC (Vaginal Birth After Cesarean) means attempting vaginal delivery in a subsequent pregnancy after a previous c-section.
According to ACOG’s Cesarean Birth guidelines, 60–80% of women who attempt VBAC are successful.
You are a strong VBAC candidate if:
- Your previous c-section used a low transverse uterine incision (the most common type)
- You are carrying a single baby
- Your pelvis is adequately sized
- You have no new medical conditions that contraindicate labor
- Your hospital has continuous fetal monitoring and immediate surgical capability
VBAC is generally not recommended if:
- You had a classical (vertical) uterine incision
- You have placenta previa or accreta
- You have had 2 or more prior uterine surgeries
- There has been a prior uterine rupture
What This Means For You: If you have had one c-section with a low transverse incision, do not assume your next delivery must also be a c-section. Raise VBAC eligibility at your first prenatal appointment in your next pregnancy — ideally with an OB experienced in VBAC management.
For women tracking fertility and planning their next pregnancy after a c-section, our Ovulation Calculator can support conception timing. Most OB-GYNs recommend waiting 18–24 months after a c-section before attempting another pregnancy to allow full uterine healing.
For further reading on recovery from major surgeries and post-operative milestones, our guide on hip replacement surgery recovery explores comparable healing timelines from a different surgical perspective.
11 FAQs: Real Questions Real Mothers Ask
Q1: How long does a c-section take?
A standard, uncomplicated c-section takes 45–60 minutes from first incision to final suture. However, if complications arise — such as significant adhesions from a prior surgery, excessive bleeding, or unusual fetal positioning — the procedure can extend to 2 hours or more, and in rare cases may require conversion to general anesthesia.
Q2: Is a c-section painful?
You will not feel pain during the surgery due to spinal or epidural anesthesia. You will feel pressure, tugging, and sometimes cold sensations when your baby is delivered. Post-operatively, the first 3–4 days are typically the most painful. Most pain is well-managed with ibuprofen, acetaminophen, and short-term prescription medication. Breastfeeding-safe options are available.
Q3: How long is c-section recovery?
Surface incision healing takes 4–6 weeks. Your uterine incision heals in approximately 3 months. Full internal scar maturation can take up to 12 months. Most women return to most daily activities by 6–8 weeks, but high-impact exercise should not resume before 12 weeks and only with OB clearance.
Q4: Can I walk after a c-section?
Yes — and early walking is strongly encouraged. Most women are helped out of bed for their first assisted walk within 24 hours of surgery. Early ambulation reduces blood clot risk, restarts bowel function, and has been shown to shorten overall recovery time. Walking around the room is very different from going up stairs or walking outside; start slowly.
Q5: How many c-sections can you have?
There is no universal maximum, but most OB-GYNs advise against more than 3 c-sections due to escalating risks with each procedure. Each additional cesarean increases the likelihood of placenta accreta, extensive adhesions, bladder injury, and severe hemorrhage. Women considering a 4th or higher c-section should consult a maternal-fetal medicine specialist and deliver at a tertiary care center.
Q6: What is a gentle c-section?
A gentle (family-centered) c-section is a modified cesarean protocol that includes immediate skin-to-skin contact, delayed cord clamping, a clear surgical drape so parents can see the birth, and a slower, more controlled baby delivery. It is available at many major U.S. hospitals but must be requested in advance. It is not appropriate for emergency cesareans.
Q7: When can I drive after a c-section?
Most U.S. physicians clear patients to drive at 4–6 weeks, once they can perform an emergency stop without pain and are no longer taking narcotic pain medication. Do not drive if you are still on prescription opioids, regardless of time elapsed. Always confirm with your doctor before driving.
Q8: What are the long-term risks of a c-section?
Long-term risks include isthmocele (cesarean scar defect causing pelvic pain and fertility issues), internal adhesions (scar tissue that complicates future surgeries), chronic incision pain (affecting ~18% of women at 3 months), and placenta accreta spectrum in future pregnancies — a risk that rises meaningfully with each repeat cesarean.
Q9: Can I breastfeed after a c-section?
Yes. Breastfeeding can begin in the recovery room, often within an hour of delivery. The football hold and side-lying position are most comfortable because they keep the baby’s weight off the incision. A slight delay in milk “coming in” (Days 3–5 rather than Day 2–3) is normal after cesarean delivery due to the absence of hormonal labor signals, but does not prevent successful breastfeeding.
Q10: What is VBAC?
VBAC stands for Vaginal Birth After Cesarean. It refers to a vaginal delivery in a pregnancy following a previous c-section. The American College of Obstetricians and Gynecologists (ACOG) reports that 60–80% of women who attempt VBAC succeed. Eligibility depends primarily on the type of prior uterine incision, current pregnancy characteristics, and hospital capabilities.
Q11: Does a c-section affect future pregnancies?
Yes. Each c-section incrementally increases the risk of placenta previa, placenta accreta spectrum, uterine rupture, and adhesion-related complications in subsequent pregnancies. These risks are manageable with proper prenatal planning, early ultrasound screening for abnormal placentation, and delivery at an appropriately resourced facility. Waiting 18–24 months after a c-section before conceiving again is the most important protective step.
Medical References & Sources
This article is based on the following peer-reviewed and authoritative sources:
- CDC National Vital Statistics Reports, Vol. 74, No. 1 — March 2025 — 2023 U.S. cesarean rate data
- ACOG — Cesarean Birth Patient FAQ — Clinical guidelines on c-section indications and VBAC
- American Medical Association — What Doctors Wish Patients Knew About C-Sections (2025) — 2025 clinical insights and HCA protocol data
- NHS — Caesarean Section Overview — UK clinical recovery standards
- PMC — The Rising Global Cesarean Section Rates: A Scoping Review, Nov 2025 — 42 studies, 2015–2025 evidence synthesis
- WHO — Caesarean Section Global Data — Global rate projections to 2030
For personalized medical guidance, always consult your board-certified OB-GYN or maternal-fetal medicine specialist. MyMedicineAdvisor.com provides evidence-based educational health content reviewed by credentialed international medical experts.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.