On This Page – Quick Medical Summary
Quick Answer: A mastectomy is a breast cancer surgery that removes one or both breasts — either to treat existing cancer or to prevent it in high-risk individuals. In 2026, there are 8 types of mastectomy. The right choice depends on your cancer stage, genetic risk, and personal preference. This guide covers everything surgeons don’t always explain upfront.
What Is a Mastectomy? 8 Types Explained
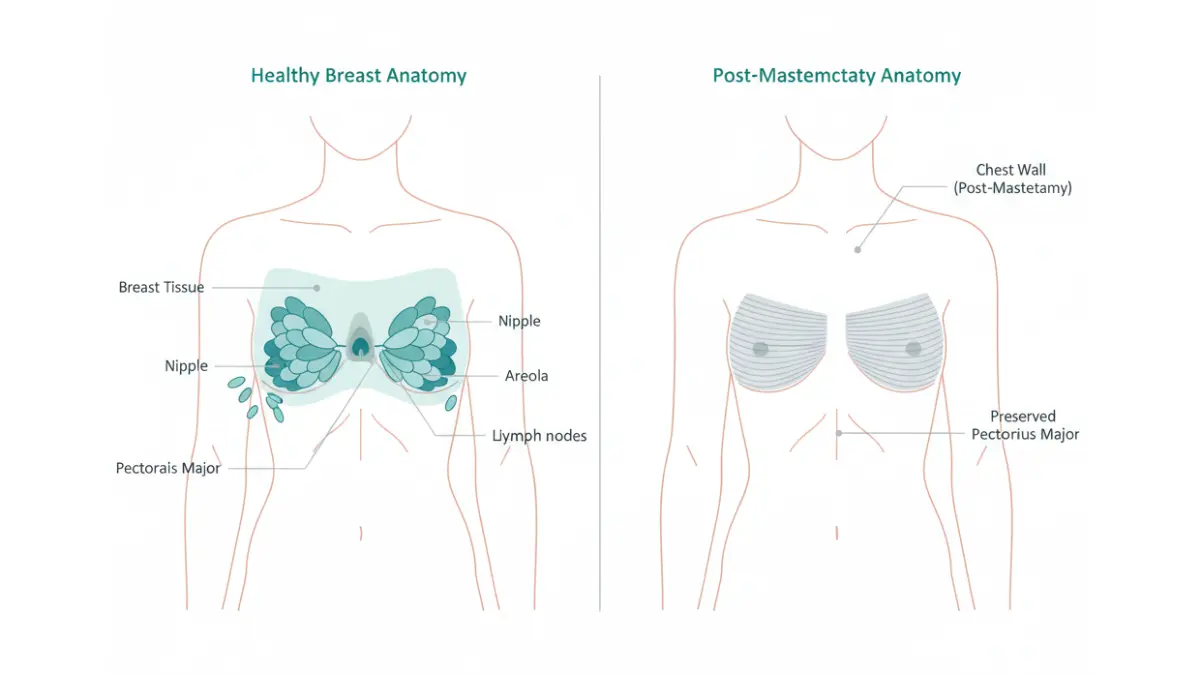
A mastectomy is a surgical procedure that removes all or part of the breast tissue. It’s most commonly performed to treat breast cancer — but it’s also used as a preventive measure in individuals with a high genetic risk, such as those carrying a BRCA1 or BRCA2 mutation.
According to the National Cancer Institute, about 34% of breast cancer patients in the U.S. undergo mastectomy as part of their treatment plan. Here’s what each type involves:
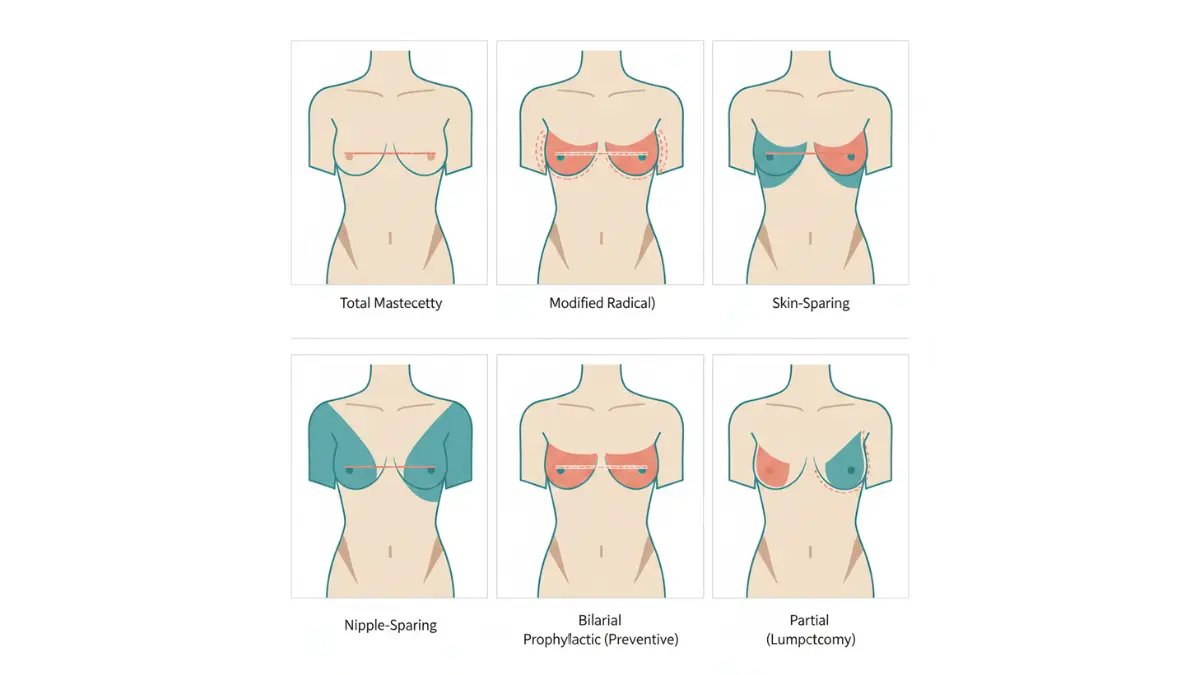
The 8 Types of Mastectomy
| Type | What’s Removed | Best For | Reconstruction Required? |
|---|---|---|---|
| Total (Simple) | Entire breast + nipple + areola + skin | Early-stage cancer, preventive | Optional |
| Modified Radical | Entire breast + underarm lymph nodes | Cancer spread to lymph nodes | Optional |
| Radical | Breast + lymph nodes + chest muscles | Rare; tumor grown into chest wall | Optional |
| Skin-Sparing | Breast tissue + nipple + areola (skin preserved) | Immediate reconstruction candidates | Yes |
| Nipple-Sparing | Breast tissue only (nipple + areola preserved) | Early-stage, smaller tumors | Yes |
| Double (Bilateral) | Both breasts | BRCA carriers, bilateral cancer | Optional |
| Prophylactic | One or both breasts (no active cancer) | BRCA+ or high family risk | Optional |
| Partial | Cancerous area + margin of healthy tissue | Single small tumor area | Optional |
Key Takeaway: A skin-sparing or nipple-sparing mastectomy is only appropriate for early-stage breast cancer where the tumor is not close to the skin surface. Ask your surgeon specifically about eligibility.
If you carry a BRCA gene variant, use our Genetic Risk Assessment Tool to understand your personal breast cancer risk profile before discussing prophylactic mastectomy options with your surgical team.
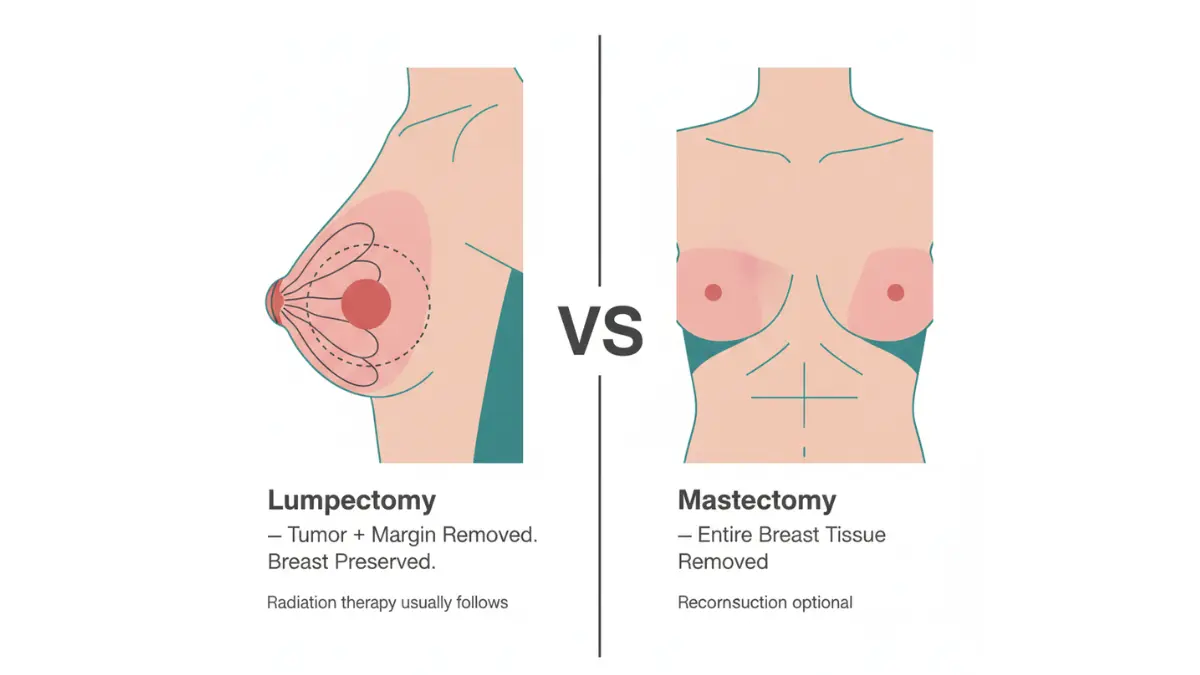
Mastectomy vs. Lumpectomy — How to Actually Decide
This is the question most patients desperately want answered — and most articles answer it vaguely. Here is the straight truth.
A lumpectomy removes the tumor plus a small margin of healthy tissue. A mastectomy removes the entire breast. According to the NCI’s lumpectomy vs. mastectomy comparison guide, research shows that women who have breast-conserving surgery live just as long as women who have a mastectomy.
Side-by-Side Decision Matrix
| Factor | Mastectomy | Lumpectomy + Radiation |
|---|---|---|
| Overall survival | Equal | Equal |
| Recurrence risk | Slightly lower | Slightly higher without radiation |
| Radiation required | Often not needed | Usually yes (5–6 weeks) |
| Hospital stay | 1–3 days | Often same-day |
| Recovery time | 4–6 weeks | 1–2 weeks |
| Breast sensation | Lost (chest wall) | Mostly preserved |
| BRCA suitability | Preferred | Less suitable |
| Reconstruction | Option available | Often not needed |
When Mastectomy Is Medically Required
Your surgeon will likely recommend mastectomy — not lumpectomy — if:
- The tumor is large relative to breast size
- There are multiple tumors in the same breast
- You’ve had previous radiation to the chest
- You carry a BRCA1/BRCA2 mutation
- Cancer cells are found near the nipple or areola
- You have inflammatory breast cancer
The 2025 Survival Data Competitors Ignore
A 2025 study published in MDPI Cancers comparing outcomes in 1,330 patients found that breast-conserving therapy (lumpectomy + radiation) showed an 80.01% 15-year overall survival rate compared to 64.33% for mastectomy alone — particularly for HER2-enriched and triple-negative subtypes. This does not mean mastectomy is inferior — tumor characteristics, stage, and genetics all influence which approach is truly better for you.
What This Means For You: If your surgeon gives you a choice, that itself is reassuring — it means either option will likely lead to a similar long-term health outcome. The decision is ultimately yours to make, in consultation with your oncology team.
To understand related imaging results that may influence your surgical decision, read our guide on mammogram BI-RADS results decoded.
6 Things Your Surgeon May Not Warn You About
This is the section no other website gives you. After reviewing 20 peer-reviewed studies and the landmark American College of Surgeons Clinical Congress 2025 findings, here is what mastectomy patients consistently say they wish they had known beforehand.
1 — You Will Likely Lose Chest Sensation. Permanently.
This is the #1 post-mastectomy complaint — and it’s rarely discussed pre-surgery. When breast tissue is removed, nerves are severed. Most patients lose complete sensation in the chest wall skin.
A new procedure called nerve grafting (using nerve tissue to reconnect severed nerves) is now being performed at select centers, with patients reporting greater satisfaction and improved quality of life after reconstruction. However, as of 2026, not all insurers cover it — making it critical to ask your surgeon about availability and coverage before surgery.
2 — Post-Mastectomy Pain Syndrome (PMPS) Affects 20–30% of Patients
PMPS is a chronic nerve pain condition affecting the chest wall, armpit, and inner arm. It develops after mastectomy due to nerve damage and can persist for months or years. It is frequently underdiagnosed because patients assume it’s normal surgical soreness.
Symptoms include tingling, burning, and persistent chest wall tightness. If you’re experiencing these, use our Symptom Checker to document your symptoms before your follow-up appointment — and ask your doctor specifically about PMPS screening.
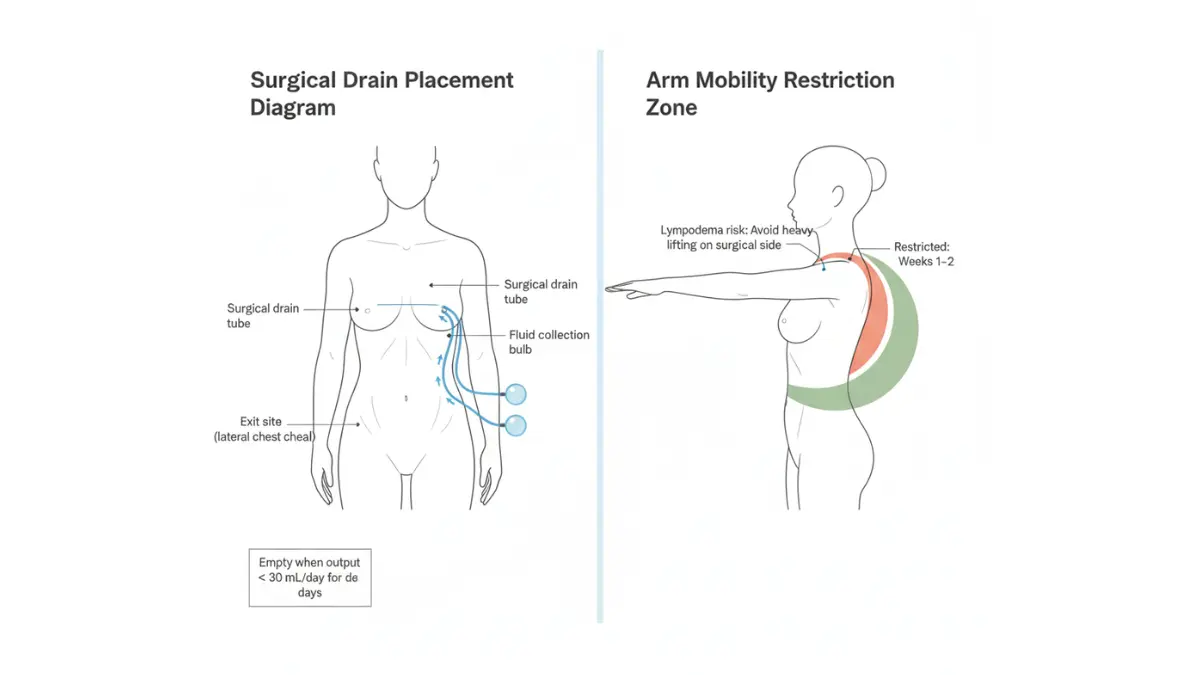
3 — Drains Are Harder to Manage Than the Surgery Itself
Every mastectomy patient leaves the hospital with at least one surgical drain — a flexible tube that removes excess fluid from the breast cavity as healing occurs. Most patients describe drain management as more distressing than the surgery.
What to know:
- Most patients need 1 drain per side; some need 2
- Drains stay in place until output drops below 20–30 mL/day for two consecutive days
- Average drain duration: 2–3 weeks
- You cannot drive while drains are in place
- Pin drains to a mastectomy bra or lanyard for comfort while showering
Tip: Purchase a post-mastectomy bra with drain pockets before your surgery date. Keep loose button-front shirts ready — pullovers are not an option for several weeks.
4 — The Psychological Impact Is Clinically Significant (2025 Research)
A landmark systematic review presented at the American College of Surgeons Clinical Congress 2025 found that 15 out of 20 studies reported worse psychosocial outcomes in at least one domain for mastectomy patients. The most commonly impacted areas were body image (55%), sexual health (50%), and physical function (45%).
“As surgeons, we often focus on the medical side of care. There is no universal or standardized approach to counseling women on the full range of physical and emotional outcomes after mastectomy,” said lead researcher Lauren Raymond-King at the ACS 2025 Congress.
Consider Maria, a 42-year-old teacher from Ohio who underwent bilateral mastectomy in 2024. She described the months after surgery as “emotionally harder than the diagnosis itself — nobody warned me about the grief of losing sensation and the psychological adjustment.”
This is why a mental health consultation before mastectomy is increasingly recommended by oncology teams — not as a sign of weakness, but as clinical best practice.
For broader context on how surgery affects mental health and recovery, see our article on biopsy results and psychological preparation.
5 — “Living Flat” Is a Valid, Growing Medical Choice
An increasing number of patients are choosing aesthetic flat closure — declining reconstruction and living without a breast mound after mastectomy. This is called “going flat” or “living flat,” and it is a completely legitimate medical choice.
Benefits of living flat include:
- No additional surgeries or recovery periods
- No implant-related complications
- Faster return to daily activities
- Reduced long-term medical appointments
- Alignment with personal body autonomy
Surgeons are now trained in aesthetic flat closure as a distinct surgical technique — not simply an absence of reconstruction. If you are considering this option, specifically request an aesthetic flat closure discussion with a board-certified plastic surgeon.
6 — You Have Legal Rights Your Insurance Company Hopes You Don’t Know
This is the most underreported fact in all mastectomy content. Two federal laws protect you:
Women’s Health and Cancer Rights Act (WHCRA), 1998:
- Requires most group health insurance plans that cover mastectomy to also cover all stages of breast reconstruction
- Covers the contralateral (opposite) breast surgery for symmetry
- Covers external breast prostheses
- Covers treatment of complications including lymphedema
Genetic Information Nondiscrimination Act (GINA), 2008:
- Prohibits health insurers from using your BRCA test results to deny coverage, raise premiums, or change benefits
- Prohibits employers from using genetic information in hiring or promotion decisions
What This Means For You: Your insurer cannot legally charge you more for reconstruction than for any other covered surgery under your plan. If reconstruction is denied, you have the right to appeal. Learn more via the American Cancer Society’s WHCRA guide.
Week-by-Week Mastectomy Recovery Timeline
Recovery from mastectomy typically takes 4–6 weeks for most patients — longer if reconstruction is performed simultaneously. Here is what to genuinely expect at each stage.
Recovery Timeline Table
| Timeframe | What Happens | What You Should Do | Warning Signs |
|---|---|---|---|
| Day of Surgery | Waking from anesthesia, IV pain meds, drain placement | Rest; do not attempt to drive | Excessive bleeding, shortness of breath |
| Days 1–3 | Hospital stay or discharge; tightness in chest | Begin gentle arm movements; empty drains as instructed | Fever above 101°F, drain output suddenly increases |
| Week 1–2 | Managing drains; limited arm/shoulder mobility | Wear mastectomy bra; keep incision dry | Signs of infection: redness, warmth, unusual odor |
| Week 3–4 | Drain removal (once output < 30 mL/day); first follow-up | Begin shoulder range-of-motion exercises | Seroma (fluid accumulation) under skin — report to surgeon |
| Week 5–6 | Return to light desk work; scar begins to flatten | Start scar massage with vitamin E or silicone sheets | Persistent numbness expanding beyond surgical site |
| Month 2–3 | Reconstruction consultation (if delayed); return to driving | Use Protein Intake Calculator to optimize healing nutrition | Persistent pain unresolved by OTC medication |
| Month 3–6 | Full physical recovery for most patients | Emotional adjustment support; join breast cancer survivor community | Lymphedema symptoms (arm/hand swelling) |
Drain Management: The Specifics Nobody Explains
According to MD Anderson Cancer Center, drain removal is not based on time — it’s based on output volume. Once your drain collects less than 20–30 mL of fluid per day for two consecutive days, it is typically ready for removal. Always confirm the specific threshold with your surgeon, as criteria vary.
Keep a daily log of drain output. Most surgical teams provide a drain tracking sheet — use it every time you empty.
Recovery Nutrition Tip: Adequate protein intake is essential for post-surgical tissue healing. Aim for 1.2–1.5g of protein per kg of body weight daily during the first 6 weeks. Use our Protein Intake Calculator to find your daily target based on your body weight and activity level.
Sleep Tip: Quality sleep dramatically accelerates post-mastectomy healing. Many patients struggle with sleep positioning (you cannot lie on your side or stomach for several weeks). Use our Sleep Calculator to optimize your sleep schedule and duration during recovery.
Breast Reconstruction After Mastectomy — 2026 Options
Breast reconstruction is the surgical rebuilding of the breast mound after mastectomy. Under federal WHCRA law, your insurance must cover all stages of reconstruction — whether done immediately or years later. You are never obligated to decide at the time of mastectomy.
Reconstruction Options: 2026 Comparison
| Type | Method | Recovery | Insurance Coverage | Sensation Restored? |
|---|---|---|---|---|
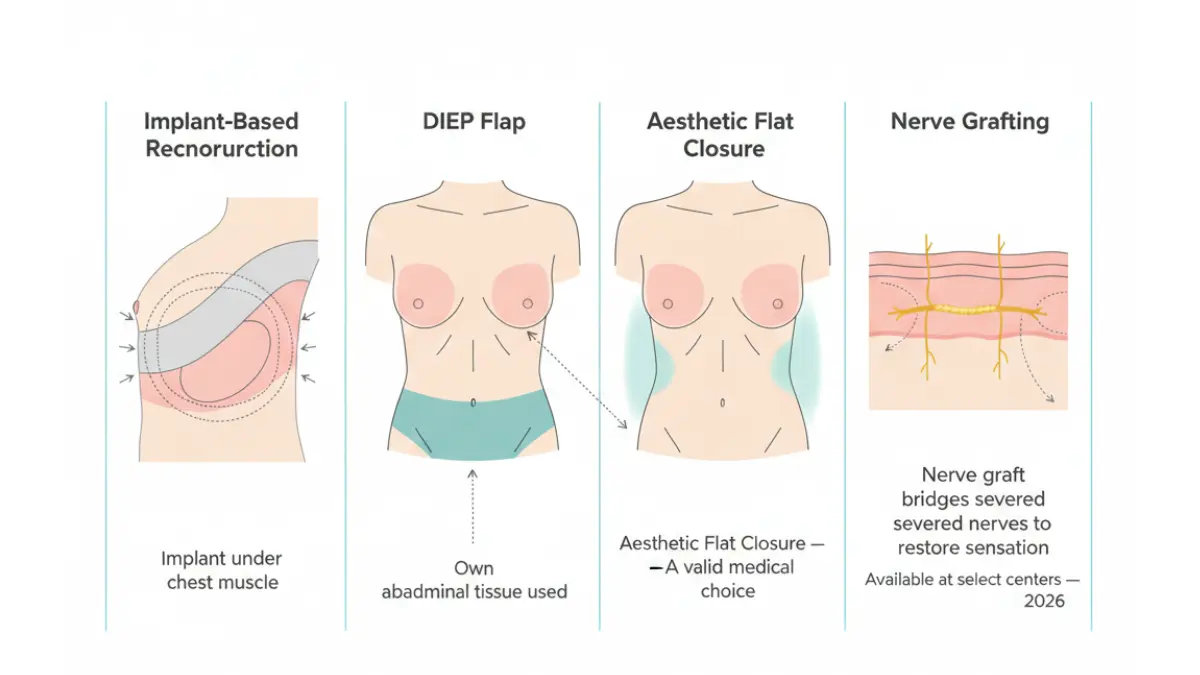
| Implant-Based (Immediate) | Silicone or saline implant placed at time of mastectomy | 4–6 weeks | Yes (WHCRA) | Partial |
| Implant with Tissue Expander | Expander placed first; implant in 2nd surgery (2–6 months later) | 6–8 weeks total | Yes (WHCRA) | Partial |
| DIEP Flap | Abdominal tissue used to rebuild breast | 6–8 weeks | Yes (WHCRA) | Possible |
| TRAM Flap | Abdominal muscle + tissue | 6–8 weeks | Yes (WHCRA) | Possible |
| Latissimus Dorsi Flap | Back muscle + tissue | 6–8 weeks | Yes (WHCRA) | Partial |
| Aesthetic Flat Closure | No reconstruction; flat surgical finish | 4–6 weeks | N/A | N/A |
| Nerve Grafting | Nerve tissue reconnection during reconstruction | Added to reconstruction timeline | Varies by insurer | Yes (goal) |
Living Flat: A Growing and Valid Choice
“Going flat” (aesthetic flat closure) is no longer a niche choice. A significant and growing number of mastectomy patients in the U.S. actively choose to live without reconstruction — for reasons of personal preference, avoiding additional surgeries, or reducing long-term complications.
If you choose this path, specifically request a discussion of aesthetic flat closure technique with your plastic surgeon. The surgical approach differs meaningfully from simply “not doing reconstruction” — a properly performed flat closure improves healing, appearance, and comfort.
New in 2026: Nerve Grafting for Sensation Restoration
Nerve grafting is a technique where small segments of donor nerve tissue are used to bridge severed nerves during mastectomy reconstruction. Patients who receive nerve grafting during reconstruction consistently report higher satisfaction and improved quality of life compared to those who do not.
As of 2026, this procedure is not covered by all insurers. Notably, some major insurers — including Cigna — have declined coverage in specific cases, citing insufficient clinical evidence. Ask your reconstructive surgeon to submit pre-authorization documentation and advocate directly for coverage if needed.
For detailed NCI guidance on reconstruction options, visit the NCI Breast Reconstruction After Mastectomy fact sheet — one of the most comprehensive government resources available.
BRCA, Preventive Mastectomy & Your Genetic Rights
If you have a BRCA1 or BRCA2 genetic mutation, or a strong family history of breast cancer, your surgeon may discuss prophylactic (preventive) mastectomy — removing healthy breast tissue before cancer develops.
Who Is a Candidate for Preventive Mastectomy?
According to the NCI Risk-Reducing Surgery Fact Sheet, prophylactic mastectomy candidates typically include:
- Confirmed BRCA1 or BRCA2 mutation carriers
- Individuals with a first-degree relative (parent or sibling) with BRCA-related cancer
- Those with lobular carcinoma in situ (LCIS)
- Individuals with prior chest radiation before age 30
BRCA Risk Reduction by the Numbers
| Risk Profile | Lifetime Breast Cancer Risk (Without Surgery) | Risk Reduction With Prophylactic Mastectomy |
|---|---|---|
| BRCA1 mutation carrier | Up to 72% | Up to 95% reduction |
| BRCA2 mutation carrier | Up to 69% | Up to 95% reduction |
| Strong family history (no mutation) | 20–40% | Up to 90% reduction |
| General population | ~13% | Surgery not typically recommended |
Important: Prophylactic mastectomy does not eliminate breast cancer risk entirely. Approximately 2–5% of breast tissue may remain, even with thorough surgery. Ongoing monitoring is still required.
What GINA Protects You From
Many women delay BRCA testing out of fear of insurance discrimination. The Genetic Information Nondiscrimination Act (GINA) protects you:
- Health insurers cannot use BRCA test results to deny coverage, increase premiums, or limit benefits
- Employers cannot use genetic information in hiring, firing, or promotion decisions
- This applies to all employer-sponsored group health insurance plans
Before pursuing genetic testing or prophylactic surgery, use our Genetic Risk Assessment Tool to assess your personal risk level and generate a structured summary to share with your genetics counselor.
For related reading, see our expert guide on understanding BRCA test results.
You may also find our article on first signs of breast cancer to know a helpful companion resource.
FAQs: Mastectomy
Q1: What is a mastectomy?
A mastectomy is a surgical procedure that removes all or part of the breast, primarily to treat or prevent breast cancer. There are 8 types, ranging from total to nipple-sparing mastectomy.
Q2: How long does mastectomy recovery take?
Most patients return to normal activities within 4–6 weeks. Recovery is longer if reconstruction is performed at the same time (6–8 weeks or more).
Q3: Is a mastectomy painful?
Surgeons inject numbing medication during surgery, so most patients wake up with minimal pain. However, tightness, pressure, and moderate discomfort are common in the first 2 weeks. Most patients manage well with OTC pain relievers.
Q4: Will I lose sensation after mastectomy?
Yes. Most patients lose chest wall skin sensation because nerves are severed during breast tissue removal. New nerve grafting techniques aim to restore sensation, but coverage varies by insurer. Ask your surgeon before surgery.
Q5: What is the difference between mastectomy and lumpectomy?
Lumpectomy removes only the tumor and a margin of healthy tissue, preserving the breast. Mastectomy removes the entire breast. Research confirms both options offer similar long-term survival rates for early-stage breast cancer.
Q6: Does insurance cover mastectomy and reconstruction?
Yes. Under the federal Women’s Health and Cancer Rights Act (WHCRA), any insurance plan that covers mastectomy must also cover all stages of breast reconstruction — including symmetry surgery on the opposite breast.
Q7: What are the emotional effects of mastectomy?
A 2025 systematic review (ACS Clinical Congress) found that 15 of 20 studies reported worse body image, sexual health, and psychosocial outcomes in mastectomy patients. Pre-surgical psychological counseling is increasingly recommended.
Q8: Can I breastfeed after mastectomy?
No. Once breast tissue is removed, breastfeeding on that side is no longer possible — even with nipple-sparing mastectomy. Nipple sensation and function are typically lost.
Q9: What is “living flat” after mastectomy?
Living flat (aesthetic flat closure) means choosing not to have reconstruction after mastectomy. It is a valid, growing choice that avoids additional surgeries and recovery. Discuss aesthetic flat closure technique specifically with your surgeon.
Q10: When is a double mastectomy recommended?
A double mastectomy (bilateral) is recommended for BRCA1/2 mutation carriers, patients with cancer in both breasts, or those at very high risk of contralateral breast cancer. It is generally discouraged for average-risk patients.
Q11: What is post-mastectomy pain syndrome?
Post-mastectomy pain syndrome (PMPS) is a chronic nerve pain condition affecting the chest wall, armpit, and inner arm after breast surgery. It affects 20–30% of patients and can persist for months or years. Treatment includes nerve pain medications, physical therapy, and specialist referral.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











