On This Page – Quick Medical Summary
Can breast cancer actually be prevented? What the evidence says
If you noticed a new breast change — a lump, nipple discharge, or skin dimpling — use our Symptom Checker before reading further; those findings need clinical evaluation before any prevention conversation begins. Our guide to the first signs of breast cancer covers each symptom clinically. If you are here because a family member was recently diagnosed, a genetic test raised concern, or you want to know what you can realistically do to lower your risk, this article was written specifically for you.
Breast cancer prevention is more precisely described as risk reduction — no single action in this guide eliminates the possibility entirely. What the evidence clearly and consistently supports is that specific, measurable interventions shift your probability in clinically documented ways.
📊 Clinical Data Point: Approximately 1 in 8 U.S. women will develop invasive breast cancer over their lifetime. Source: National Cancer Institute SEER Program, 2026.
A meaningful proportion of breast cancer cases involves modifiable risk factors. Steps 1–5 apply to every woman. Steps 6–8 require a specialist conversation for women at elevated or high genetic risk — and those three steps are where the most preventable outcomes are currently being missed.
ℹ️ Medical Disclaimer: The genetic testing recommendations, chemoprevention medications, risk-reduction surgical options, and mammography screening schedules discussed in this article reflect current clinical guidelines as of 2026 and are provided for educational purposes only. Individual risk assessment, medication eligibility, surgical candidacy, and screening frequency depend on personal medical history, family history, comorbidities, and specialist evaluation. Consult a board-certified oncologist, gynecologist, or genetic counselor before acting on any clinical information in this article. Nothing in this article constitutes a personal diagnosis or treatment recommendation.
Understanding your breast cancer risk before you start: average vs. high risk
Your risk category determines which prevention steps are most clinically urgent for your specific situation — and which steps are optional versus essential.
The two risk categories that change which steps apply to you
Average-risk women — no confirmed BRCA1 or BRCA2 mutation, no personal history of atypical ductal hyperplasia or lobular carcinoma in situ (LCIS), and no first-degree relative diagnosed before age 50 — should focus on Steps 1–5 alongside standard mammography screening.
Elevated- and high-risk women — defined by a Gail Model 5-year risk score ≥1.7%, a Tyrer-Cuzick lifetime risk ≥20%, or confirmed BRCA carrier status — require Steps 6–8 in addition, under specialist oversight.
Review the full landscape of modifiable and non-modifiable breast cancer risk factors before your next appointment. To understand what these eight steps are working to prevent, our guide to breast cancer stages and survival rates explains exactly what early detection changes at each clinical stage.
📊 Clinical Data Point: Breast cancer is the most commonly diagnosed cancer among U.S. women. Source: CDC Breast Cancer Statistics, 2026 — current CDC breast cancer incidence and mortality data.
The 8 evidence-based steps at a glance — and who each one is for
The following steps represent the most evidence-supported strategies for breast cancer risk reduction, per current NCI and NCCN guidance — detailed in the NCI’s breast cancer prevention evidence summary:
- Exercise regularly — 150–300 minutes per week of moderate-intensity activity. All risk profiles.
- Limit or eliminate alcohol — dose-response risk begins below moderate intake. All risk profiles.
- Achieve a healthy body weight — critical after menopause; directly reduces circulating estrogen. All risk profiles.
- Follow an anti-inflammatory diet — Mediterranean pattern has the strongest observational evidence. All risk profiles.
- Breastfeed when possible — 12 or more cumulative months is the clinically meaningful threshold. All risk profiles.
- Pursue BRCA genetic testing if eligible — required for women at elevated or high risk before proceeding to Steps 7 and 8.
- Discuss chemoprevention eligibility — FDA-approved options that most eligible women are never offered.
- Optimize your screening protocol — your plan must match your risk category, not a generic age default.
Steps 1–5: lifestyle changes that move the needle on breast cancer risk
These five steps require no prescription, no genetic test result, and no referral. They are also the foundation that makes every specialist intervention in Steps 6–8 more effective.
Exercise and alcohol: the two steps with the strongest direct evidence
Regular physical activity of 150–300 minutes per week of moderate-intensity exercise is associated with a clinically meaningful reduction in breast cancer risk across large population studies, with the most pronounced benefit in post-menopausal women.
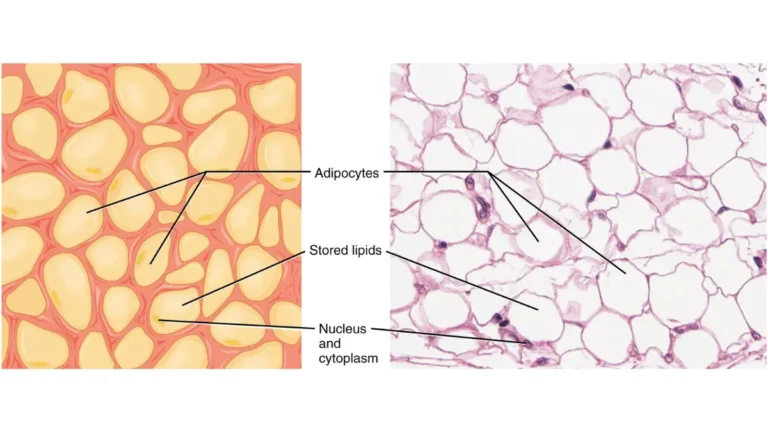
🔬 How It Works: After menopause, adipose (fat) tissue becomes the primary estrogen source through aromatization — enzymes in fat cells convert androgens into estrogen. More body fat means higher circulating estrogen, which drives hormone receptor-positive tumor growth. Reducing body fat through exercise directly reduces the primary remaining estrogen source in post-menopausal women — the precise mechanism behind the strongest lifestyle risk-reduction evidence.
Alcohol is classified as a Group 1 carcinogen by the International Agency for Research on Cancer specifically for breast cancer. The dose-response relationship begins below what most patients consider moderate intake — each additional drink per day incrementally raises risk. No safe intake threshold for breast cancer risk has been established.
Body weight, diet, and breastfeeding: steps 3 through 5
Post-menopausal obesity is an independent breast cancer risk factor through the same aromatization mechanism described above. Women with a BMI above the healthy range after menopause carry significantly higher circulating estrogen than women at a healthy weight. Use our BMI Calculator to assess your current number and bring it to your next appointment for a targeted weight management discussion.
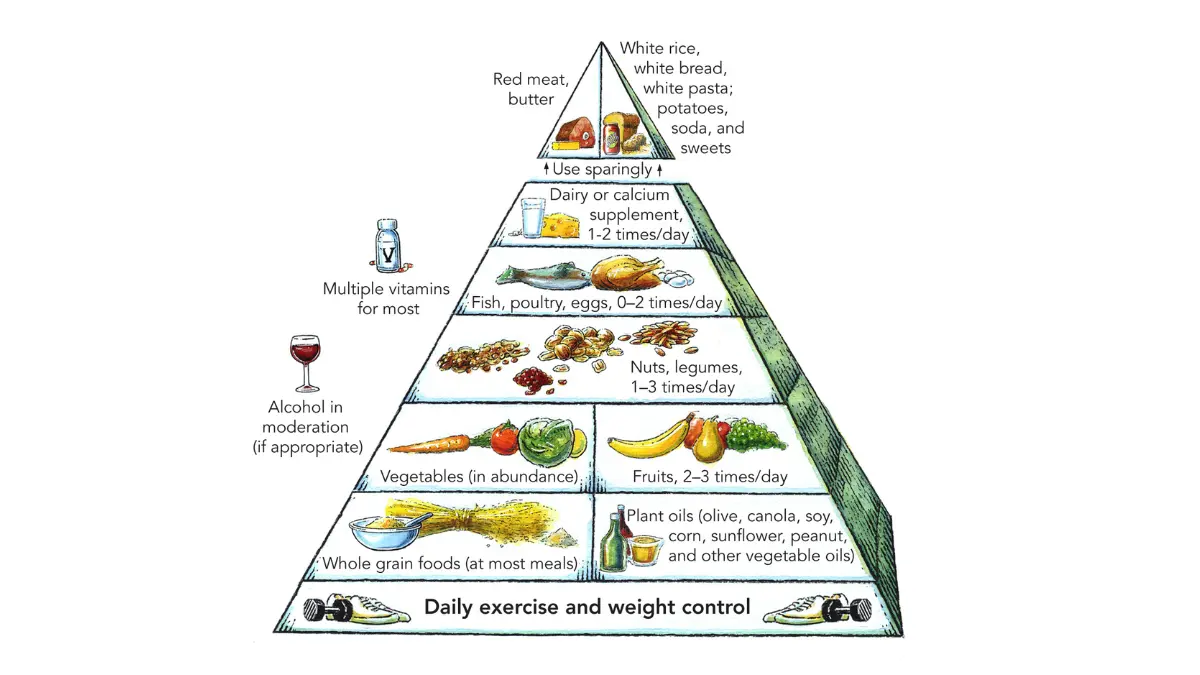
A Mediterranean dietary pattern — emphasizing vegetables, legumes, whole grains, olive oil, and fatty fish — carries the strongest observational evidence among dietary approaches for reduced breast cancer incidence. No single food prevents breast cancer; the overall dietary pattern is what the literature supports.
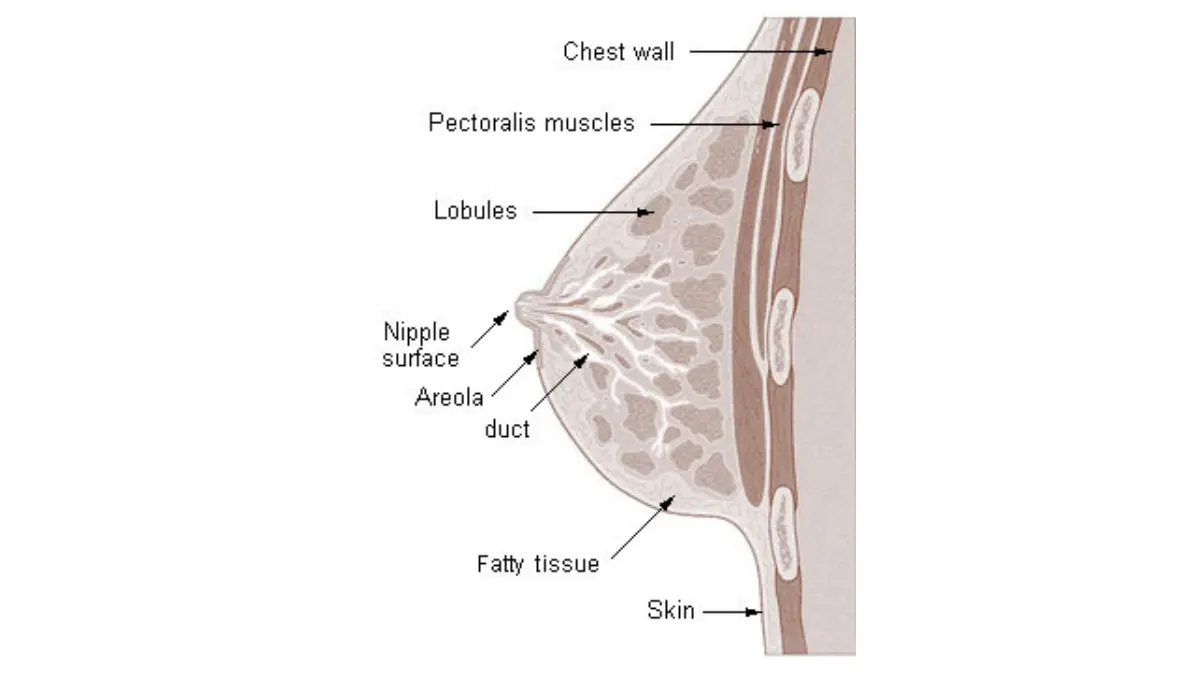
Breastfeeding for a cumulative 12 or more months is associated with reduced lifetime risk of hormone receptor-positive breast cancer, driven by suppression of ovulation and reduction of lifetime estrogen exposure through direct breast tissue differentiation during lactation.
✅ Patient Action: Before your next OB-GYN appointment, track your average weekly exercise minutes for two weeks. If you are consistently below 150 minutes, ask specifically: “Given my breast cancer risk profile, what is my target for weekly moderate-intensity activity, and do I qualify for a structured exercise program referral?”
Step 6: do you qualify for BRCA genetic testing? What to ask your doctor
BRCA genetic testing is the prevention step most frequently delayed — and for high-risk women, it is the one decision that unlocks the most clinically powerful interventions in Steps 7 and 8. A positive result is not a cancer diagnosis. It is the map that makes prevention possible at a specialist level.
The NCCN criteria that determine who should be referred for BRCA testing
NCCN guidelines recommend referral for BRCA1 and BRCA2 counseling and testing for women who meet at least one of the following criteria:
- A first-degree relative diagnosed with breast cancer at age 50 or younger.
- Two or more relatives on the same side of the family with breast cancer at any age.
- A personal or family history of ovarian, fallopian tube, or primary peritoneal cancer.
- A family member with a known pathogenic BRCA1 or BRCA2 variant.
- Ashkenazi Jewish ancestry with any first- or second-degree relative with breast or ovarian cancer.
- A personal diagnosis of triple-negative breast cancer at age 60 or younger.
- A male relative with a breast cancer diagnosis.
Before your genetics appointment, use our Genetic Risk Assessment Tool to identify which criteria apply to your family history. Then calculate your 5-year and lifetime risk estimate using the NCI Breast Cancer Risk Assessment Tool — the same Gail Model instrument used in clinical practice to determine chemoprevention eligibility.
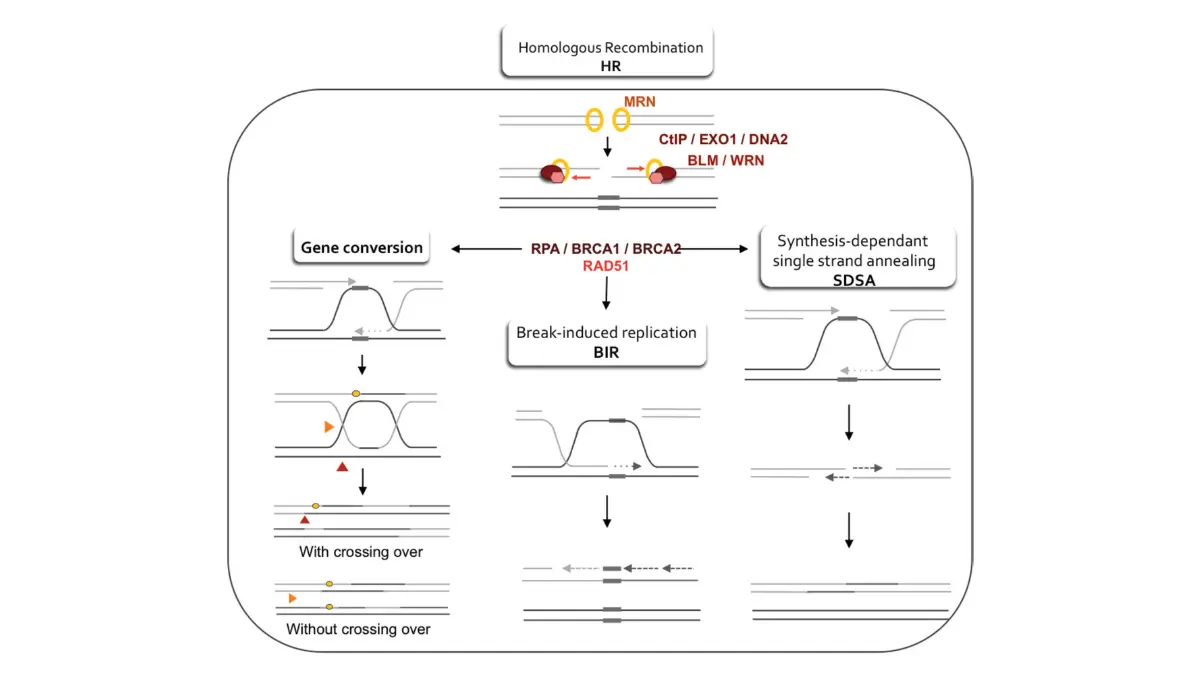
🔬 How It Works: BRCA1 and BRCA2 encode proteins that repair double-strand DNA breaks through homologous recombination. A pathogenic variant in either gene impairs this repair function — damaged DNA accumulates over time, genomic instability increases, and the probability of tumor initiation rises substantially across a lifetime. This mechanism explains why confirmed BRCA carriers face a lifetime breast cancer risk far above the population average.
What a positive BRCA1 or BRCA2 result means for your prevention plan
BRCA1 mutations are more frequently associated with triple-negative breast cancer — estrogen receptor-negative tumors that do not respond to hormonal chemoprevention agents such as tamoxifen. BRCA2 mutations more commonly drive hormone receptor-positive tumors, making SERM-based chemoprevention a more targeted option for BRCA2 carriers specifically.
Lifetime breast cancer risk for confirmed BRCA1 carriers is substantially above the population average — published estimates in current literature cite ranges of approximately 55–72% for BRCA1 and 45–69% for BRCA2.
For a complete clinical walkthrough of the testing process, variant classification, and surveillance recommendations, see what a BRCA-positive result means for your health decisions.
✅ Patient Action: If you meet one or more of the criteria above, ask your OB-GYN or primary care physician: “Based on my family history, should I be referred to a board-certified genetic counselor for BRCA1/2 sequencing and deletion/duplication analysis?” Request a clinical referral — not a self-ordered direct-to-consumer test — because a certified genetic counselor interprets variants of uncertain significance and builds your personalized surveillance plan based on the complete result.
Step 7: FDA-approved drugs that reduce breast cancer risk — are you a candidate?
Most women who qualify for chemoprevention have never been told it exists. This is the most underutilized evidence-based intervention in breast cancer prevention — and for eligible women, it represents a clinically significant risk reduction that lifestyle changes alone cannot replicate.
Tamoxifen and raloxifene: who qualifies and what the evidence shows
The FDA has approved two selective estrogen receptor modulators (SERMs) — tamoxifen and raloxifene — as chemoprevention agents for women at elevated risk of developing breast cancer, based on clinical trial evidence demonstrating significant reduction in hormone receptor-positive tumor incidence.
Tamoxifen (Nolvadex) is approved for both pre- and post-menopausal women who meet the Gail Model eligibility threshold — a 5-year risk score of ≥1.7% — or who carry a BRCA2 mutation with hormone receptor-positive family history. Key contraindications include personal history of deep vein thrombosis, pulmonary embolism, or endometrial cancer.
Raloxifene (Evista) is approved for post-menopausal women only, with a comparable risk-reduction profile to tamoxifen for ER-positive tumors and a more favorable DVT risk profile in clinical trials. Menopausal status — not age alone — determines eligibility for raloxifene over tamoxifen.
For a detailed clinical comparison of both agents, see tamoxifen vs. aromatase inhibitors for breast cancer risk reduction.
Aromatase inhibitors and the shared decision-making conversation
Aromatase inhibitors — specifically exemestane (Aromasin) and anastrozole (Arimidex) — are approved for post-menopausal high-risk women and have demonstrated clinically significant risk reduction in major prevention trials. They cannot be used in pre-menopausal women because residual ovarian estrogen production overrides the aromatase-blocking effect in women with intact ovarian function.
🩺 Physician Note: In my clinical practice, the chemoprevention conversation is the one most frequently skipped by primary care physicians — not out of negligence, but because they were not trained in eligibility assessment during residency. I regularly see women in their late 40s with Gail Model scores well above 1.7% who have never had this conversation. If you have a significant family history or a calculated risk score at or above the threshold, the specific question to ask is: “Am I a candidate for tamoxifen, raloxifene, or an aromatase inhibitor for breast cancer risk reduction?” — not “Is there anything I should be doing?” — because the latter rarely gets a chemoprevention answer. — Dr. Nathaniel J. Hargrove, MD, Oncology
⚠️ Clinical Warning: Tamoxifen carries an increased risk of endometrial cancer and thromboembolic events in some populations. Aromatase inhibitors carry musculoskeletal side effects and accelerated bone density loss. These risks are manageable with appropriate screening and monitoring — but eligibility determination requires a formal evaluation by a board-certified oncologist or gynecologic oncologist who can assess your contraindication profile before prescribing.
✅ Patient Action: If your Gail Model 5-year risk score is ≥1.7% or you carry a confirmed BRCA variant, ask your next appointment: “Am I eligible for FDA-approved chemoprevention, and which agent is appropriate for my menopausal status and contraindication profile?” This is a specific question that will reliably produce a chemoprevention-focused answer.
Step 8: optimizing your screening plan based on your risk profile
Mammography screening is not prevention in the traditional sense — it does not stop a tumor from forming. It ensures that if one does develop, it is found at the earliest, most treatable stage. For women at average risk, that distinction is academic. For women at high risk, optimizing the type and frequency of screening is a genuine prevention strategy.
Average-risk women: when to start and how often
The American Cancer Society recommends that average-risk women begin annual mammography at age 40 — a recommendation based on the survival benefit of detecting tumors before they become clinically palpable. Current USPSTF guidelines similarly recommend screening beginning at age 40, with frequency determined in shared decision-making between patient and provider.Any updates issued in 2026 supersede prior versions — see American Cancer Society breast cancer screening guidelines.
For the complete appointment-by-appointment walkthrough of what to expect at each stage, see our guide to breast cancer mammogram screening age and frequency.
📊 Clinical Data Point: Screening mammography in average-risk women beginning at age 40 is associated with a reduction in breast cancer mortality compared to no screening. Source: American Cancer Society, 2026.
High-risk women: when to add breast MRI to your screening schedule
Women with confirmed BRCA1 or BRCA2 mutations, a lifetime risk ≥20% by Tyrer-Cuzick modeling, or a personal history of chest radiation between ages 10 and 30 should receive annual breast MRI screening protocol in addition to — not instead of — annual mammography. The standard NCCN recommendation for confirmed BRCA carriers is to begin this combined protocol between ages 25 and 30.
Dense breast tissue independently reduces mammographic sensitivity and is itself an independent breast cancer risk factor. Women whose mammogram report notes heterogeneously dense or extremely dense breast tissue may benefit from supplemental ultrasound or MRI — a conversation that should happen with your gynecologist or breast specialist. Our full clinical breakdown of dense breast tissue and cancer risk explains the ACR density classification system in patient-facing language.
✅ Patient Action: At your next mammogram appointment, specifically request your BI-RADS breast density category from the radiologist’s report. If your report notes “heterogeneously dense” or “extremely dense” tissue, ask your gynecologist: “Given my breast density and risk profile, should I be referred for supplemental ultrasound or breast MRI screening, and is this covered under my current plan?” Women with ACA-compliant plans may be entitled to supplemental screening at no cost depending on risk classification.
An oncologist’s perspective: the most important step most patients skip
I want to be direct with you about something I see in my practice every week.
Why most high-risk women never get the conversation they deserve
The chemoprevention conversation — the one about tamoxifen, raloxifene, and aromatase inhibitors — almost never happens in primary care. Not because primary care physicians don’t care, but because most were not trained in breast cancer risk assessment during residency and don’t have the clinical workflow to calculate Gail Model scores at a routine annual visit. I see patients in their late 40s and early 50s with BRCA2 mutations who have been told for years to “just keep getting your mammograms” — when they qualified for chemoprevention at 43. I have seen the same pattern with BRCA-positive patients who were never referred for supplemental MRI because their gynecologist assumed standard mammography was sufficient.
This is not a failure of medicine. It is a failure of information access.
The one action that changes everything
The most impactful thing you can do after reading this guide is not a lifestyle change — though those matter. It is scheduling one preventive health appointment in the next two weeks and arriving with a calculated risk score from the NCI Breast Cancer Risk Assessment Tool and a specific question: “Based on my family history and my risk score, should I be referred for genetic counseling, and am I a candidate for chemoprevention?”
That single question — asked of the right specialist — has changed clinical outcomes for patients in my practice who had no idea these options existed.
🩺 Physician Note: A positive BRCA result, a Gail Model score above 1.7%, or a mammogram report noting extremely dense breast tissue are not reasons to panic. They are reasons to escalate your care from passive monitoring to active, evidence-based prevention. The tools to act on that information exist, are FDA-approved, and are covered by most insurance plans. The only barrier for most patients is not having this conversation. — Dr. Nathaniel J. Hargrove, MD, Oncology
Frequently asked questions about breast cancer prevention
1. Can breast cancer actually be prevented, or just detected early?
Breast cancer prevention is more accurately described as risk reduction — no single intervention guarantees immunity. However, a meaningful proportion of invasive breast cancer cases involves modifiable risk factors, meaning lifestyle changes, chemoprevention, and optimized screening can substantially reduce both the likelihood of developing breast cancer and the probability it progresses undetected. Consult a board-certified oncologist to determine which steps are most relevant to your risk profile.
2. What are the main modifiable risk factors for breast cancer?
The most clinically significant modifiable risk factors are physical inactivity, excess body weight after menopause (which drives adipose estrogen production), alcohol intake at any level, combined hormone therapy use, and not breastfeeding. Non-modifiable factors — age, dense breast tissue, inherited gene mutations — cannot be changed but can be addressed through chemoprevention, enhanced screening, or risk-reducing surgery. Consult a board-certified gynecologist to stratify your specific profile.
3. What foods are evidence-based for breast cancer prevention?
No individual food prevents breast cancer. A Mediterranean dietary pattern — emphasizing vegetables, legumes, whole grains, olive oil, and fatty fish — carries the strongest observational evidence among dietary approaches for reduced incidence. Soy-based foods with naturally occurring phytoestrogens are not contraindicated in most patients, including survivors. Consult a registered dietitian alongside your oncologist before making significant changes if you carry a breast cancer diagnosis.
4. Does drinking alcohol increase breast cancer risk even at low levels?
Yes. Alcohol is classified as a Group 1 carcinogen for breast cancer by the International Agency for Research on Cancer. The dose-response relationship begins below the level most patients consider significant — each additional drink per day incrementally raises risk through acetaldehyde-mediated DNA damage and elevation of circulating estrogen. No intake level has been established at which breast cancer risk is zero. Consult a board-certified oncologist when assessing your personal risk threshold.
5. Does breastfeeding actually lower breast cancer risk?
Yes. Breastfeeding for a cumulative total of 12 or more months is associated with a reduction in lifetime breast cancer risk, particularly for hormone receptor-positive tumors. The mechanism involves suppression of ovulation during lactation, reduced lifetime estrogen exposure, and direct differentiation of breast epithelial cells. Women at elevated risk should discuss duration targets with their OB-GYN, as the protective effect scales with cumulative breastfeeding duration.
6. What does a positive BRCA1 or BRCA2 result actually mean?
A positive BRCA1 or BRCA2 result confirms you carry a pathogenic variant that substantially elevates lifetime breast cancer risk above the population average. It is not a cancer diagnosis — it is the clinical information needed to build an active prevention plan. BRCA1 is more associated with triple-negative tumors; BRCA2 with hormone receptor-positive tumors. Next steps include specialist evaluation, possible chemoprevention, supplemental MRI screening, and discussion of prophylactic surgical options. Consult a board-certified genetic counselor and oncologist immediately after receiving your results.
7. What is chemoprevention for breast cancer and who qualifies?
Chemoprevention refers to FDA-approved medications — tamoxifen, raloxifene, exemestane, and anastrozole — shown to significantly reduce hormone receptor-positive breast cancer incidence in high-risk women. Eligibility is based on a Gail Model 5-year risk score at or above the NCCN-designated threshold or confirmed BRCA2 carrier status. Menopausal status determines which agent is appropriate. Consult a board-certified oncologist or gynecologic oncologist to assess your eligibility before starting any agent.
8. Who qualifies for a risk-reducing prophylactic mastectomy?
Prophylactic mastectomy is considered for women with confirmed pathogenic BRCA1 or BRCA2 variants, a lifetime risk above 20–25% by Tyrer-Cuzick modeling, or a personal history of lobular carcinoma in situ with additional high-risk features. It reduces breast cancer risk by approximately 90% in BRCA carriers based on available evidence. It is not appropriate for average-risk women. Consult a board-certified oncologist and genetic counselor before making this decision.
9. When should average-risk women start annual mammograms?
Current American Cancer Society guidelines recommend annual mammography beginning at age 40 for average-risk women. USPSTF guidelines similarly recommend screening from age 40, with individualized frequency in shared decision-making. Women with dense breast tissue or elevated family history may qualify for earlier screening. Discuss your specific start date with your gynecologist or primary care physician at your next annual visit.
10. Can I reduce my breast cancer risk if it runs strongly in my family?
Yes — and for women with a strong family history, the highest-impact steps are specifically Steps 6–8: BRCA genetic testing and counseling, chemoprevention eligibility assessment, and supplemental MRI screening. Steps 1–5 contribute meaningfully but are insufficient alone when significant hereditary risk is present. Family history does not determine clinical destiny — it determines the urgency of the specialist conversation. Consult a board-certified genetic counselor and oncologist to build a prevention plan matched to your specific history.
11. Are any supplements evidence-based for breast cancer prevention?
No supplement has demonstrated breast cancer prevention efficacy in randomized controlled trial data as of current published evidence. Vitamin D insufficiency is associated with elevated risk in observational studies, but supplementation alone has not been confirmed as preventive in controlled trials. No supplement replaces the evidence base of the eight steps in this guide. Consult a board-certified oncologist before beginning any supplementation protocol marketed for cancer risk reduction.
Your next step: one appointment that changes your prevention trajectory
The eight steps in this guide range from things you can begin today — reducing alcohol, increasing weekly exercise, calculating your BMI — to clinical decisions that require a specialist. The dividing line is your risk category.
If you have not calculated your Gail Model risk score, do that this week. If your score is at or above the chemoprevention threshold, or if you meet any NCCN criteria for BRCA testing, schedule a preventive health appointment specifically to ask the questions in the Patient Action callouts above.
For the broader clinical picture of what early detection through optimized screening changes at every stage, see our complete guide to breast cancer survival rates by stage.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.




{kind=link}