On This Page – Quick Medical Summary
Whatever brought you to this page, you are in the right place to understand what comes next.
Pancreatic cancer is one of the most frightening diagnoses in medicine, and the fear is not irrational — but a diagnosis is not a verdict, and what you do next genuinely matters. This guide is built to meet you wherever you are right now.
- If you were just diagnosed, start with the sections on stages and how treatment is decided. The single most useful early step is getting to a specialist who treats many of these cases.
- If you are caring for someone with pancreatic cancer, the sections on treatment, supportive care, and caregiving are written for you.
- If you have symptoms but have not seen a doctor, the symptoms and diagnosis sections will help you know what warrants prompt evaluation — and many of these symptoms have causes other than cancer.
- If you are already in treatment, you can jump to chemotherapy, targeted therapy, or clinical trials.
Pancreatic cancer is the third-leading cause of cancer death in the United States, and its statistics are sobering. They are also population averages — they describe a large group of people treated years ago, not your individual outcome. We will be honest about the numbers and equally honest about what they cannot tell you.
ℹ️ Medical Disclaimer: The symptoms, diagnostic criteria, staging system, survival statistics, surgical descriptions, chemotherapy and targeted-therapy information, radiation guidance, genetic-risk information, clinical-trial information, and supportive-care content in this article reflect current clinical guidelines and are for educational purposes only. They are not a diagnosis, a treatment recommendation, or a substitute for professional medical care. Individual decisions depend on your history, tumor type, stage, comorbidities, genetic profile, and the assessment of your specialists. Consult a board-certified oncologist and your treating team before acting on any information here.
What pancreatic cancer is — and why type matters
Understanding what kind of pancreatic cancer is present changes nearly everything that follows, including the outlook and the treatment.
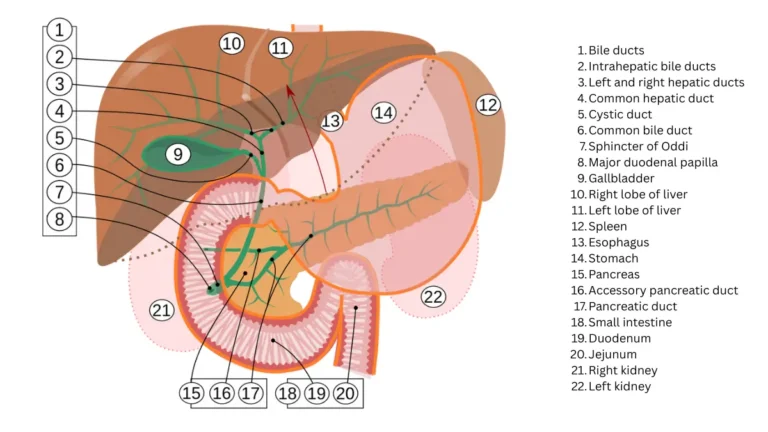
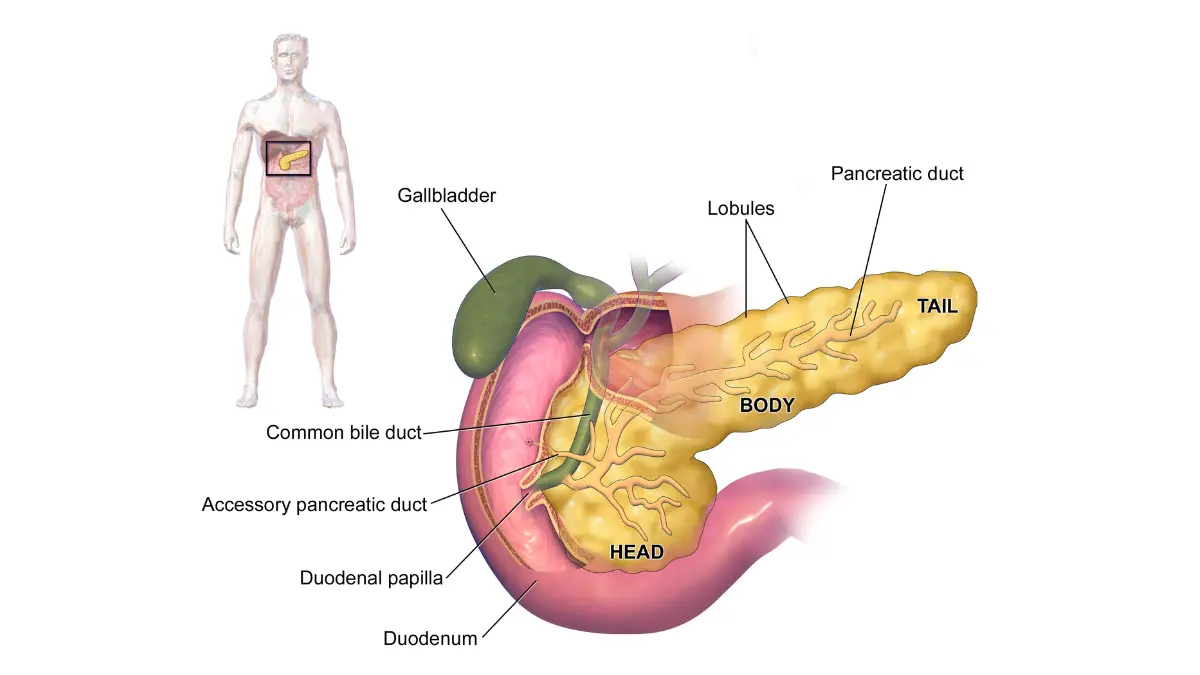
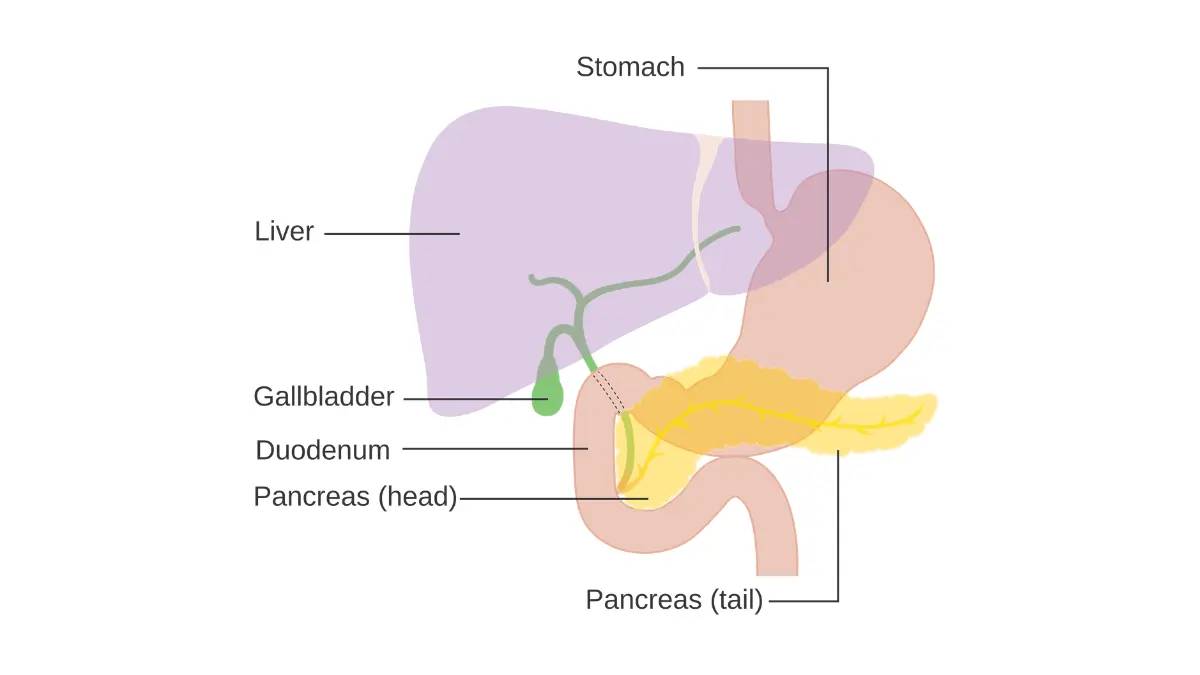
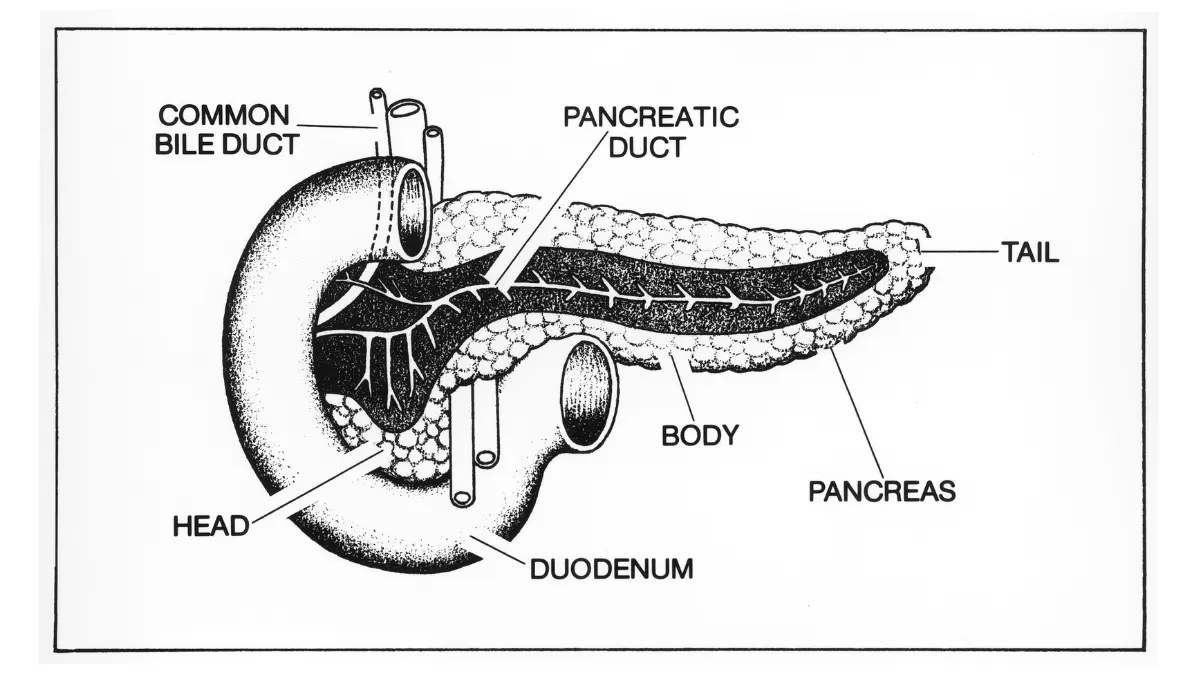
The pancreas is a gland about six inches long, tucked behind the stomach. It does two very different jobs: its exocrine cells make enzymes that digest food, and its endocrine cells (the islets) make hormones, including insulin, that control blood sugar.
Pancreatic cancer begins when cells in the pancreas grow out of control and form a tumor. Which cells start the cancer determines its type — and the two main types behave so differently that survival figures for one do not apply to the other.
Exocrine cancer (pancreatic ductal adenocarcinoma)
Most pancreatic cancers are exocrine, and the large majority of those are pancreatic ductal adenocarcinoma (PDAC), which starts in the cells lining the pancreatic ducts.
📊 Clinical Data Point: Pancreatic adenocarcinoma carries a five-year relative survival rate of about 8% across all stages — lower than the figure for pancreatic cancers overall, because adenocarcinoma is the most aggressive and most common form. (Source: American Cancer Society / Pancreatic Cancer Action Network, Cancer Statistics 2025.)
When this article refers to “pancreatic cancer” without qualification, it means PDAC, because that is what the overwhelming majority of patients face.
Pancreatic neuroendocrine tumors — a different disease
A smaller share of pancreatic cancers are pancreatic neuroendocrine tumors (pNETs), which arise from the hormone-making islet cells. These are a genuinely distinct disease, often slower-growing, with a meaningfully better outlook than adenocarcinoma.
If you have been told you have a pancreatic neuroendocrine tumor, the adenocarcinoma survival numbers in this article do not describe your situation, and you should ask your oncologist for pNET-specific information.
Why pancreatic cancer is so often found late
The pancreas sits deep in the abdomen, with no easy way to feel a tumor and no blood test that reliably catches early disease in the general population.
🔬 How It Works: Because the early tumor is small, hidden behind the stomach, and often painless, it can grow and even spread before it produces symptoms a person would notice. By the time jaundice or persistent pain appears, the cancer has frequently moved beyond the pancreas — which is why early detection is the central challenge of this disease.
That biology explains why the symptoms below matter, and why none of them should be ignored when they persist.
Early warning signs and symptoms of pancreatic cancer
Knowing the warning signs matters, with one honest caveat: early pancreatic cancer often causes no symptoms at all, and when symptoms do appear they frequently have causes far more common than cancer.
The most common symptoms of pancreatic cancer include:
- Jaundice — yellowing of the skin and the whites of the eyes, often the first noticeable sign of a tumor in the head of the pancreas
- Dark urine and pale, greasy, or floating stools
- Itchy skin (which can accompany jaundice)
- Pain in the upper abdomen that may spread to the middle of the back
- Unexplained weight loss and loss of appetite
- New-onset diabetes, especially appearing after age 50 in someone without typical risk factors
- Nausea, vomiting, or a feeling of fullness after small meals
- Fatigue
- Blood clots, which can occasionally be a first clue
If you are uncertain whether your symptoms warrant a visit, our Symptom Checker can help you think through next steps, though it does not replace a clinician’s evaluation.
What jaundice looks like
Jaundice happens when bilirubin — a yellow pigment the liver normally clears — builds up in the blood.
🔬 How It Works: A tumor in the head of the pancreas can press on the nearby bile duct, blocking the normal drainage of bile. Bilirubin then backs up into the bloodstream, turning the skin and eyes yellow, darkening the urine, and lightening the stool. Painless jaundice in an adult always deserves prompt medical evaluation.
Where pancreatic cancer pain is felt
The classic pattern is a dull ache in the upper abdomen, sometimes radiating straight through to the mid-back, and it may worsen after eating or when lying flat.
Back pain is common and usually has nothing to do with the pancreas — but back pain combined with unexplained weight loss, jaundice, or new digestive symptoms is worth raising with a doctor.
New-onset diabetes and unexplained weight loss
A sudden, unexplained case of type 2 diabetes in an older adult — particularly alongside weight loss — can occasionally be an early sign of pancreatic cancer rather than ordinary diabetes.
This does not mean new diabetes usually signals cancer; it rarely does. If you are tracking new blood-sugar readings, our Blood Sugar Converter can help you make sense of the units, but any sudden unexplained diabetes is worth discussing with your physician.
When to see a doctor now
⚠️ Clinical Warning: Painless jaundice, unexplained weight loss of more than a few pounds, or persistent upper-abdominal pain that radiates to the back are not symptoms to wait out. They have many possible causes, but each warrants prompt evaluation — and pancreatic and biliary problems are among the possibilities a doctor needs to rule out.
✅ Patient Action: If you have new painless jaundice, unexplained weight loss, or persistent upper-abdominal-to-back pain, see your primary care physician or a gastroenterologist promptly, and ask directly: “Could this be coming from my pancreas or bile duct, and what tests will rule that out?” You can read more in our guide to the early symptoms of pancreatic cancer.
Symptoms raise the question of risk — so it helps to know who is actually more likely to develop this cancer.
Risk factors, causes, and when pancreatic cancer runs in families
Knowing your risk factors helps you and your doctor decide whether extra vigilance makes sense — though most people who develop pancreatic cancer have no obvious cause.
A risk factor raises the odds of a disease without guaranteeing it. Some pancreatic cancer risk factors can be influenced; many cannot.
Risk factors you can influence
- Smoking — the single largest modifiable risk factor, roughly doubling the risk
- Obesity and physical inactivity
- Heavy, long-term alcohol use, largely through its link to chronic pancreatitis
- Chronic pancreatitis (long-standing inflammation of the pancreas)
- Type 2 diabetes, which is both a possible risk factor and, sometimes, an early sign
Because excess weight is a modifiable factor, understanding where you stand can help; our BMI Calculator offers a starting point for that conversation with your doctor.
Risk factors you can’t
- Age — most cases occur in older adults
- A family history of pancreatic cancer
- Certain inherited genetic syndromes (below)
- Being male (slightly higher risk) and, in the U.S., being Black, which is associated with higher incidence
📊 Clinical Data Point: Pancreatic cancer is most often diagnosed in people aged 65–74, and the median age at diagnosis is about 71. It accounts for roughly 3% of all new U.S. cancer diagnoses, and a person’s lifetime risk of developing it is about 1.7%. (Source: NCI SEER Cancer Stat Facts: Pancreatic Cancer, 2026.)
Hereditary syndromes and family history
A minority of pancreatic cancers — but an important minority — are linked to inherited gene mutations. Knowing about them can change screening for you and for your relatives.
Inherited conditions associated with higher pancreatic cancer risk include mutations in BRCA1 and BRCA2, PALB2, Lynch syndrome (mismatch-repair genes), Peutz-Jeghers syndrome (STK11), familial atypical multiple mole melanoma (CDKN2A), and hereditary pancreatitis (PRSS1).
🩺 Physician Note: Current guidelines emphasize that family history matters: having one or more close relatives with pancreatic cancer, or a known hereditary cancer syndrome, can justify genetic counseling and, in some cases, a specialized surveillance program. This is established clinical guidance, not a personal opinion.
Should you consider genetic counseling?
If pancreatic cancer or a known cancer syndrome runs in your family, genetic counseling can clarify your actual risk and whether testing or monitoring is appropriate.
✅ Patient Action: If you have two or more relatives with pancreatic cancer, or a known mutation such as BRCA in your family, ask your doctor for a referral to a genetic counselor and ask: “Do I qualify for germline genetic testing and a pancreatic surveillance program?” Our Genetic Risk Assessment Tool can help you organize your family history before that appointment, and our guide to understanding BRCA test results explains what a positive result means.
When risk or symptoms lead to a workup, the next step is understanding how pancreatic cancer is actually diagnosed.
How pancreatic cancer is diagnosed
Knowing what each test is for can make a frightening sequence of appointments feel more navigable — and help you ask better questions.
Diagnosing pancreatic cancer usually follows a sequence:
- Imaging to find and measure a suspicious mass
- A biopsy to confirm cancer cells and identify the type
- Blood markers and molecular testing to guide treatment
Imaging: CT, MRI, and the pancreatic protocol
A CT scan done with a dedicated “pancreatic protocol” (specific contrast timing) is the workhorse for finding a tumor and assessing whether it involves nearby blood vessels.
MRI, sometimes with a technique called MRCP, can give additional detail about the pancreatic and bile ducts. If you have received imaging results you don’t understand, our guide to making sense of an abnormal CT scan can help you prepare questions.
Endoscopic ultrasound and biopsy
Endoscopic ultrasound (EUS) uses a thin scope passed into the digestive tract to image the pancreas from very close range, and it can guide a needle to take a tissue sample.
🔬 How It Works: During EUS, an ultrasound probe at the tip of an endoscope sits just millimeters from the pancreas through the stomach or duodenum wall, producing detailed images of small tumors that a CT might miss — and allowing a fine-needle biopsy in the same procedure. A biopsy is what confirms the diagnosis; imaging alone cannot.
Waiting on biopsy results is one of the hardest parts of this process; our guide to biopsy result timelines explains what the report will and won’t say.
The CA 19-9 blood test — and its limits
CA 19-9 is a protein that is often elevated in pancreatic cancer, and it is widely misunderstood by patients.
🩺 Physician Note: CA 19-9 is not a diagnostic or screening test. It can be normal in people who do have pancreatic cancer (including those who genetically don’t produce it), and it can be elevated by non-cancer conditions such as a blocked bile duct. Guidelines use it mainly to track response to treatment over time, not to make the diagnosis.
Molecular and genetic testing of the tumor
Beyond confirming cancer, modern care looks at the tumor’s biology and the patient’s inherited genetics.
Molecular profiling (next-generation sequencing of the tumor) and germline genetic testing can reveal targetable mutations and inherited risk — and current guidelines recommend this testing for appropriate patients, especially those with advanced disease.
Getting to a high-volume specialist
Where you are treated affects outcomes, and this is one of the most actionable facts in this entire article.
✅ Patient Action: Ask your physician for a referral to a high-volume pancreatic cancer center, and ask: “Should my tumor undergo molecular profiling, and should I have germline genetic testing?”
Once cancer is confirmed, the next question is its stage — how far it has spread.
The stages of pancreatic cancer, explained simply
Stage describes how far the cancer has spread, and for pancreatic cancer one practical question matters even more than the stage number: can the tumor be removed with surgery?
How staging works
Doctors stage pancreatic cancer using the TNM system, which assesses the size and extent of the tumor (T), whether it has reached nearby lymph nodes (N), and whether it has metastasized to distant organs (M).
These combine into overall stages from 0 (the earliest, confined to the top layer of cells) to IV (spread to distant sites such as the liver or lungs).
Stages 0 to IV at a glance
| Stage | What it generally means | Key clinical detail |
|---|---|---|
| Stage 0 | Abnormal cells confined to the duct lining (in situ) | Rarely found; not yet invasive |
| Stage I | Cancer is limited to the pancreas | Most likely to be resectable |
| Stage II | Larger tumor and/or nearby lymph nodes involved | Often still operable |
| Stage III | Tumor involves major nearby blood vessels | Usually locally advanced, not immediately resectable |
| Stage IV | Cancer has spread to distant organs | Metastatic; treated with systemic therapy |
Source note: staging definitions follow the AJCC TNM system as applied in NCCN Guidelines (v1.2025). Confirm your specific stage with your care team.
The category that matters most: resectable, borderline, locally advanced, metastatic
For treatment planning, surgeons sort pancreatic cancer into four groups based on whether and how the tumor can be removed:
- Resectable — the tumor can be removed surgically
- Borderline resectable — removal is possible but uncertain; chemotherapy first may make surgery feasible
- Locally advanced — the tumor involves major blood vessels and usually cannot be safely removed
- Metastatic — the cancer has spread to distant organs and is treated with whole-body therapy
🩺 Physician Note: This resectability category, more than the stage number alone, drives the treatment plan. Two people described as having “stage III” disease can face very different paths depending on exactly which blood vessels are involved and whether chemotherapy can shrink the tumor enough to operate.
Why two people at “the same stage” can face different plans
Resectability depends on the tumor’s precise relationship to nearby arteries and veins, your overall health, and how the cancer responds to initial treatment — which is why individualized assessment by a surgical team is essential.
✅ Patient Action: Ask your team — ideally a multidisciplinary tumor board — “Is my cancer resectable, borderline resectable, locally advanced, or metastatic, and what does that mean for whether I can have surgery?”
Stage and resectability shape the numbers patients most want to understand — survival.
Pancreatic cancer survival rates — what the numbers really mean
Survival statistics are the figures most people search for first, and they deserve to be presented accurately and in context — because read without context, they mislead.
The overall five-year survival rate
📊 Clinical Data Point: The five-year relative survival rate for pancreatic cancer is about 13% across all stages combined. This figure has held steady for three consecutive years, and pancreatic cancer remains the third-leading cause of cancer death in the U.S., projected to become the second by around 2030. (Source: American Cancer Society, Cancer Facts & Figures 2026, drawing on NCI SEER data.)
📊 Clinical Data Point: In 2026, an estimated 67,530 Americans will be diagnosed with pancreatic cancer and about 52,740 will die from it. (Source: American Cancer Society, Cancer Facts & Figures 2026 / NCI SEER Cancer Stat Facts.)
That word “relative” matters, and it is worth understanding before any of these numbers can be read correctly.
🔬 How It Works: A relative survival rate compares people with pancreatic cancer to people in the general population of the same age over the same period. A 13% five-year relative survival rate means people with the disease are, on average, about 13% as likely as people without it to still be alive five years after diagnosis. It is a population average, not a clock counting down for any individual.
Survival by stage at diagnosis
Stage at diagnosis changes the outlook dramatically, which is exactly why earlier detection is so important.
| Stage at diagnosis (SEER grouping) | 5-year relative survival | Key clinical detail |
|---|---|---|
| Localized (confined to the pancreas) | About 44% | Only ~15% of cases are found this early |
| Regional (spread to nearby tissue/nodes) | About 17% | Often treated with chemotherapy and sometimes surgery |
| Distant (spread to distant organs) | About 3% | Treated with systemic therapy; outcomes vary widely |
Source note: SEER relative survival by stage, based on cases diagnosed 2015–2021 (ACS) and 2016–2022 (SEER Stat Facts). These describe groups, not individuals.
The gap between those rows is the entire argument for early detection — and the reason the resectability question matters so much.
📊 Clinical Data Point: When pancreatic cancer is caught at its earliest stage (stage IA) and removed, five-year survival can exceed 80% — underscoring how much earlier detection changes outcomes. (Source: Blackford et al., Journal of the National Cancer Institute, 2020, as cited by the Pancreatic Cancer Action Network.)
Survival differs by more than stage
Stage is the strongest single factor, but it is not the only one. Age, overall health, and the biology of the tumor all shape outcomes.
🩺 Physician Note: Survival generally declines with older age at diagnosis, in part because older patients may be less able to tolerate the most intensive treatments. Other factors that influence an individual’s outlook include performance status (overall fitness), whether the tumor can be removed with clear margins, how the cancer responds to chemotherapy, and the presence of targetable mutations — none of which a single population statistic can capture.
📊 Clinical Data Point: Survival outcomes also differ by group: the five-year relative survival rate for Black patients with pancreatic cancer is about 11%, somewhat lower than the overall figure, consistent with disparities seen across many cancers. (Source: American Cancer Society / Pancreatic Cancer Action Network, 2025.)
Why these numbers lag today’s treatments
A five-year survival figure necessarily describes people diagnosed at least five years ago, treated with the tools available then.
🩺 Physician Note: Treatments have advanced since the patients in these statistics were treated — including a first-line chemotherapy regimen approved in 2024 and targeted options for specific mutations. Newer therapies and better supportive care mean a person diagnosed today may have a different experience than these historical figures suggest, even though they remain the best population estimates available.
There is also a real, if modest, upward trend over time, which the statistics do capture.
📊 Clinical Data Point: Over the past decade, the overall five-year survival rate for pancreatic cancer rose from about 7% to 13% — slow progress, but real and measurable. (Source: American Cancer Society / Pancreatic Cancer Action Network.)
What survival statistics can’t tell you
A population average cannot account for your specific stage, your tumor’s biology, your overall health and fitness for treatment, or your access to specialized care.
Two people with the same stage and the same statistics can have very different courses. The number is a starting point for a conversation, not a prediction of your future.
It is also worth knowing that survival statistics are calculated from the moment of diagnosis. For people who respond well to treatment and remain well, the outlook tends to improve the longer they have already survived — another reason the figure at diagnosis does not fix anyone’s path.
✅ Patient Action: Ask your medical oncologist: “Given my specific stage, biology, and overall health, what outcomes are realistic for me, and am I a candidate for surgery or a clinical trial?” You can compare survival data directly at the NCI’s SEER Cancer Stat Facts page and the American Cancer Society’s survival rates page.
Numbers set the context; what you can do about them is treatment.
How pancreatic cancer treatment is decided
The treatment plan for pancreatic cancer follows a clear logic, and understanding that logic helps you understand your own path.
The first question: can it be removed?
Featured-answer format: Surgery offers the only realistic chance of cure for pancreatic cancer, but it is possible in fewer than one in five patients, because most cancers are found after they have spread beyond the point where they can be safely removed. For everyone else, treatment aims to extend life and control symptoms.
That single question — is the tumor resectable? — organizes everything that follows.
Resectable disease: surgery and chemotherapy
If the cancer can be removed, the plan usually combines surgery with chemotherapy (often after the operation, called adjuvant therapy) to lower the chance it returns.
🩺 Physician Note: For patients who can have surgery, guidelines support adjuvant chemotherapy — modified FOLFIRINOX has been shown to improve overall survival compared with older regimens in fit patients after resection. Your oncologist will weigh the regimen against your recovery and overall health.
Borderline and locally advanced: chemotherapy first
When the tumor is borderline resectable or locally advanced, doctors often give chemotherapy (and sometimes radiation) first — called neoadjuvant therapy — to try to shrink it.
The goal is to convert a borderline tumor into one that can be removed with clear margins, which gives the best chance of long-term control.
Metastatic disease: systemic therapy and goals of care
When pancreatic cancer has spread to distant organs, treatment shifts to whole-body (systemic) therapy aimed at extending life, easing symptoms, and preserving quality of life.
This is also where molecular and germline testing matters most, because it can open targeted options and trials.
Building your multidisciplinary team
The best pancreatic cancer care is delivered by a team, not a single doctor.
✅ Patient Action: Ask to have your case reviewed by a multidisciplinary pancreatic team — surgical, medical, and radiation oncology together — and ask: “Which treatment path am I on, and why?” The NCI’s patient guide to pancreatic cancer treatment explains each option in plain language.
Each path begins with a treatment modality — and surgery is where we start.
Surgery for pancreatic cancer: the Whipple and beyond
For patients whose cancer can be removed, surgery is the centerpiece of treatment — and knowing what it involves can make a daunting decision clearer.
Surgery is reserved for cancers that are resectable or that have become resectable after chemotherapy, because removing the tumor only helps if all visible cancer can be taken out. Which operation you have depends on where in the pancreas the tumor sits.
The Whipple procedure
The Whipple procedure (pancreaticoduodenectomy) is the most common operation for tumors in the head of the pancreas, where most pancreatic cancers arise.
🔬 How It Works: In a Whipple, the surgeon removes the head of the pancreas along with the duodenum (the first part of the small intestine), the gallbladder, part of the bile duct, and sometimes part of the stomach — then reconnects the remaining pancreas, bile duct, and stomach to the intestine so digestion can continue. It is one of the most complex operations in abdominal surgery, often lasting many hours, and typically followed by a hospital stay of one to two weeks.
Some centers offer minimally invasive or robotic versions of the Whipple for selected patients, though the operation remains major surgery regardless of the approach.
Distal and total pancreatectomy
For tumors in the body or tail of the pancreas, a distal pancreatectomy removes the left side of the pancreas, usually along with the spleen.
A total pancreatectomy — removing the entire pancreas — is performed less often and means lifelong, insulin-dependent diabetes plus permanent enzyme replacement, because the body loses all of its insulin- and enzyme-producing tissue.
Removing the tumor completely: why margins matter
The goal of pancreatic surgery is not just to remove the tumor but to remove it with a clear edge of healthy tissue around it.
🩺 Physician Note: Surgeons describe an “R0” resection as one with no cancer cells at the cut edges, and an “R1” resection as one with microscopic cancer at the margin. Achieving an R0 resection is strongly associated with better outcomes, which is one reason chemotherapy before surgery is increasingly used for borderline tumors — to improve the chance of a clean removal. In some borderline cases, surgeons also remove and reconstruct a segment of involved vein to achieve that clear margin.
What recovery actually involves
Recovery from pancreatic surgery typically takes weeks to months, with a hospital stay followed by a gradual return to normal eating and activity.
Fatigue, changes in appetite, and adjustments to digestion are common in the recovery period. Because this is major surgery, complications can occur and are watched for closely.
⚠️ Clinical Warning: Possible complications of pancreatic surgery include a leak of pancreatic fluid from the surgical connection (a pancreatic fistula), delayed emptying of the stomach, bleeding, and infection. These are managed by the surgical team, and this is a major reason to have the operation at a center that performs many of them. Report fever, worsening abdominal pain, or persistent vomiting after surgery promptly.
Life after pancreatic surgery
🩺 Physician Note: After pancreatic surgery, many patients need pancreatic enzyme replacement to digest food properly, and some develop diabetes because the pancreas makes insulin. These are manageable with medication and dietary support, and your care team will monitor for them, along with regular follow-up imaging to watch for recurrence.
Why surgeon and center volume matter
The complexity of pancreatic surgery means experience makes a measurable difference.
✅ Patient Action: Seek a surgeon at a high-volume pancreatic center, and ask directly: “How many pancreatic resections does this center perform each year, and what are your complication and mortality rates?” Higher surgical volume is consistently associated with better outcomes for this complex operation.
Surgery is rarely the whole plan — chemotherapy does much of the work of controlling this cancer.
Chemotherapy for pancreatic cancer: regimens and what to expect
Chemotherapy is central to pancreatic cancer treatment at nearly every stage, whether before surgery, after surgery, or as the main treatment for advanced disease.
Which regimen a person receives depends heavily on their overall fitness, often described by doctors as “performance status.”
🔬 How It Works: Performance status is a simple scale (commonly the ECOG scale, from 0 to 4) that describes how well a person can carry out daily activities. Someone who is fully active (ECOG 0–1) can usually tolerate the most intensive regimens, while someone with more limitation may be better served by a gentler option. Chemotherapy choice in pancreatic cancer depends on this fitness assessment at least as much as on the cancer itself.
FOLFIRINOX and modified FOLFIRINOX
Featured-answer format: FOLFIRINOX is a combination of four chemotherapy drugs — fluorouracil (5-FU), leucovorin, irinotecan, and oxaliplatin — given on a two-week cycle for pancreatic cancer in patients fit enough to tolerate it. A “modified” version (mFOLFIRINOX) reduces doses to lessen side effects.
FOLFIRINOX is one of the more effective regimens but also one of the most demanding, so it is generally reserved for patients in good overall condition (ECOG 0–1).
Gemcitabine plus nab-paclitaxel
The combination of gemcitabine and nab-paclitaxel (albumin-bound paclitaxel) is another standard regimen, often used for patients who may not tolerate the more intensive FOLFIRINOX.
🩺 Physician Note: Guidelines recommend gemcitabine plus nab-paclitaxel as a preferred option for patients whose performance status (overall fitness) makes the most aggressive regimens unsuitable, including many with an ECOG status of 2. The choice between regimens depends heavily on how well a person is doing overall, not on the cancer alone.
NALIRIFOX — the newest first-line option
📊 Clinical Data Point: NALIRIFOX — a combination of liposomal irinotecan, oxaliplatin, fluorouracil, and leucovorin — received FDA approval on February 13, 2024 as a first-line treatment for metastatic pancreatic adenocarcinoma. In the phase 3 NAPOLI-3 trial, which compared it against gemcitabine plus nab-paclitaxel, median progression-free survival was 7.4 months versus 5.6 months. (Source: FDA; NAPOLI-3 trial as reflected in ESMO 2025 guidance.)
🔬 How It Works: The “liposomal” form of irinotecan in NALIRIFOX wraps the drug in a tiny fatty bubble, which can improve how the medication is delivered to tumor cells and how long it circulates. NAPOLI-3 was the first formally positive phase 3 trial in metastatic pancreatic cancer in roughly a decade, which is why it changed first-line options.
Neoadjuvant versus adjuvant chemotherapy
Chemotherapy given before surgery (neoadjuvant) aims to shrink the tumor and treat unseen spread; chemotherapy after surgery (adjuvant) aims to reduce the chance of recurrence.
For patients who have surgery, modified FOLFIRINOX given afterward has been shown to improve overall survival compared with older single-drug regimens, and is a standard option for those well enough to receive it.
When the first treatment stops working
Pancreatic cancer often eventually progresses on a first regimen, and there are second-line options depending on what was used first.
🩺 Physician Note: Sequencing matters: patients who received a gemcitabine-based regimen first may be offered a fluorouracil-based combination (including liposomal irinotecan) next, and vice versa. The right second-line choice depends on prior treatment, remaining fitness, and any targetable mutations identified through molecular testing.
Side effects and how they’re managed
⚠️ Clinical Warning: Pancreatic chemotherapy regimens can cause significant side effects — including low blood counts (raising the risk of infection, anemia, and bleeding), fatigue, nausea, diarrhea, mouth sores, hair thinning, and nerve damage (neuropathy) from oxaliplatin that can become dose-limiting. These are actively managed with dose adjustments, anti-nausea medicines, and sometimes growth-factor support, and side effects should always be reported promptly rather than endured silently.
✅ Patient Action: Ask your medical oncologist: “Which chemotherapy regimen fits my performance status and my tumor’s biomarkers, and what are the trade-offs in effectiveness and side effects?” Our general guide to chemotherapy and its side effects explains what to expect during treatment.
Chemotherapy is sometimes paired with radiation in selected situations.
Radiation therapy and chemoradiation: when they’re used
Radiation has a real but selective role in pancreatic cancer, and being honest about its limits is part of using it well.
When radiation is part of the plan
Radiation therapy may be used in combination with chemotherapy in certain locally advanced cases, or after surgery when the surgical margin was not fully clear.
🩺 Physician Note: Evidence on radiation in locally advanced pancreatic cancer is mixed. A major trial (LAP-07) found no clear survival benefit from adding conventional chemoradiation after gemcitabine, though it may improve local control of the tumor and delay symptoms. Guidelines reserve it for specific situations rather than applying it routinely.
Chemoradiation and SBRT
Stereotactic body radiation therapy (SBRT) delivers focused, high-dose radiation over a few sessions and is used in selected patients, often within clinical trials or specialized programs. You can learn more about how treatment works in our overview of radiation therapy.
Radiation for symptom control
Radiation can also be used palliatively — to relieve pain or address local problems caused by the tumor — independent of any attempt to cure.
✅ Patient Action: If radiation is being considered, ask a radiation oncologist: “Does radiation add survival benefit in my specific situation, or is it primarily for local control or symptom relief?”
Beyond standard chemotherapy and radiation, a patient’s tumor biology can open additional, more targeted options.
Targeted therapy, immunotherapy, and biomarker testing
This is one of the most empowering sections for any patient, because it points to options many people never learn to ask about.
Why biomarker testing matters for everyone
Featured-answer format: Current guidelines recommend that patients with pancreatic cancer — especially advanced disease — have both molecular profiling of the tumor and germline (inherited) genetic testing. Testing can reveal mutations that open targeted therapy or clinical trials that standard chemotherapy would miss.
The case for testing is concrete, not theoretical.
📊 Clinical Data Point: Roughly 10% of pancreatic cancers carry a standard-of-care biomarker that points to an approved targeted treatment, and broader molecular profiling identifies a potentially actionable alteration in up to about 25% of cases. (Source: peer-reviewed molecular-profiling analyses, e.g., Nature Medicine 2025; Frontiers in Oncology, 2021.)
🔬 How It Works: Two kinds of test work together. Somatic next-generation sequencing reads the DNA of the tumor itself to find mutations driving that cancer, while germline testing reads inherited DNA from a blood or saliva sample to find mutations you were born with. Guidelines now treat both as standard for advanced pancreatic cancer, because each can change treatment.
BRCA, PALB2, and PARP inhibitors
📊 Clinical Data Point: Inherited (germline) BRCA mutations occur in roughly 4–7% of pancreatic cancer patients. For those whose metastatic cancer has not progressed after at least 16 weeks of platinum-based chemotherapy, the FDA approved the PARP inhibitor olaparib (Lynparza) as maintenance therapy in December 2019; in the POLO trial, median progression-free survival was 7.4 months with olaparib versus 3.8 months with placebo. (Source: FDA; POLO trial; NCI.)
🔬 How It Works: Cells normally have two systems to repair damaged DNA. A BRCA (or PALB2) mutation knocks out one of them, and a PARP inhibitor like olaparib blocks the backup — so the cancer cell can no longer fix its DNA and dies, while healthy cells with both systems intact are largely spared. This is why these tumors are also especially sensitive to platinum-based chemotherapy, and why testing must come first: an FDA-approved companion test confirms the BRCA mutation before olaparib is used.
MSI-H, mismatch-repair deficiency, and immunotherapy
A small subset of pancreatic cancers are “microsatellite instability-high” (MSI-H) or mismatch-repair deficient, and these can respond to immunotherapy.
📊 Clinical Data Point: MSI-H or mismatch-repair-deficient tumors make up roughly 1–3% of pancreatic cancers, and these patients may benefit from the immune checkpoint inhibitor pembrolizumab, which carries a tumor-agnostic FDA approval for such cancers. (Source: NCCN Guidelines v1.2025; FDA; peer-reviewed analyses.)
🔬 How It Works: Mismatch-repair-deficient tumors accumulate large numbers of mutations, which makes them look more “foreign” to the immune system. Checkpoint inhibitors like pembrolizumab release a brake on immune cells so they can recognize and attack those tumors — an approach that works in only the small share of pancreatic cancers with this feature. You can read more in our overview of how immunotherapy works.
NTRK, RET, BRAF, KRAS — rarer but actionable
Other uncommon but targetable findings are concentrated in the minority of tumors without a KRAS mutation.
| Biomarker | Approx. frequency in PDAC | Targeted option | Key clinical detail |
|---|---|---|---|
| Germline BRCA1/2, PALB2 | ~4–7% | Olaparib (maintenance); platinum chemo | Confirmed by companion test; FDA-approved 2019 |
| MSI-H / dMMR | ~1–3% | Pembrolizumab | Tumor-agnostic approval |
| NTRK fusion | <1% | Larotrectinib, entrectinib | Enriched in KRAS wild-type; high response rates |
| RET fusion | <1% | Selpercatinib | Tumor-agnostic approval |
| BRAF V600E | ~1% (KRAS wild-type) | Dabrafenib + trametinib | More often studied in trials |
| KRAS mutation | ~90% | Mostly investigational | G12D most common; RAS inhibitors in trials |
Source note: frequencies and options per NCCN Guidelines (v1.2025), FDA labeling, and peer-reviewed molecular analyses (ASCO Educational Book; Nature Medicine 2025). Targeted options apply only when the matching biomarker is present.
🩺 Physician Note: The KRAS gene is mutated in about 90% of pancreatic cancers and was long considered “undruggable.” Drugs targeting specific KRAS mutations — including the G12D form most common in pancreatic cancer — are an active and promising area of research, but most remain investigational and are accessed through clinical trials rather than as standard care.
Germline testing and your family
Germline testing does not only guide your treatment — a positive result can alert blood relatives to their own risk and the option of screening.
✅ Patient Action: Ask your oncologist and a genetic counselor: “Has my tumor had molecular profiling, and have I had germline genetic testing — and if a mutation is found, what targeted treatments or trials does it open for me, and what does it mean for my family?” You can review the FDA’s olaparib approval details at the FDA’s drug approval page.
Testing also opens the door to clinical trials and emerging treatments.
Clinical trials and new treatments worth knowing about
For a cancer where standard outcomes remain limited, clinical trials are not a last resort — they are a mainstream, guideline-encouraged option that can offer access to tomorrow’s treatments today.
Why trials matter in pancreatic cancer
Many of the advances in pancreatic cancer — including newer regimens and targeted drugs — reached patients through clinical trials.
🩺 Physician Note: Guidelines encourage considering a clinical trial at many points in pancreatic cancer care, including at the time of diagnosis, not only after standard options are exhausted. Asking about trials early keeps the most options open, and patients whose tumors lack a KRAS mutation in particular are strong candidates to consider trials of targeted agents.
How to find and evaluate a trial
Trials are available at academic centers and through national networks, and eligibility depends on factors such as your stage, prior treatments, and tumor biology.
What’s on the horizon
⚠️ Clinical Warning: Emerging approaches — including KRAS-targeted drugs, therapeutic vaccines, and novel drug combinations — are genuinely promising but remain investigational and are not yet standard of care. Be cautious of any source presenting unproven treatments as established cures.
✅ Patient Action: Ask your treating oncologist: “Is there a clinical trial I’m eligible for right now?” You can also search current studies at the NIH’s ClinicalTrials.gov pancreatic cancer listings.
Whatever the treatment path, supportive care runs alongside it from the very beginning.
Managing symptoms: nutrition, pain, and supportive care
Supportive care is not an afterthought or a sign of giving up — it is a core part of treatment that protects quality of life from day one.
Pancreatic enzymes and eating well
Many patients with pancreatic cancer cannot properly digest food because the pancreas isn’t releasing enough enzymes, leading to weight loss and discomfort.
🔬 How It Works: Pancreatic enzyme replacement therapy supplies the digestive enzymes the pancreas would normally make, taken with meals, so the body can absorb fats and nutrients. Working with an oncology dietitian can make a meaningful difference in strength and weight during treatment.
Managing pain and digestive symptoms
Pain from pancreatic cancer can often be controlled well, including with medication and, in some cases, a procedure called a celiac plexus block that interrupts pain signals.
Digestive symptoms and blockages can sometimes be relieved with stents placed to keep the bile duct or intestine open.
Managing diabetes and weight loss
Because the pancreas controls blood sugar, diabetes and unintended weight loss are common and treatable parts of the picture, managed alongside cancer treatment.
Palliative care from the start — not just end-of-life
🩺 Physician Note: Palliative care is specialized support focused on symptoms and quality of life, and it is appropriate alongside active cancer treatment — not only at the end of life. Evidence across cancers shows that early palliative care can improve quality of life, and it is a sign of good care, not surrender.
✅ Patient Action: Ask your oncologist: “Can I see palliative care now, alongside my treatment, to help manage symptoms and quality of life?”
Caring for the person — and the people who love them — is the final piece.
Coping, caregiving, and questions for your care team
Pancreatic cancer affects whole families, and the people supporting a patient need care and tools too.
Supporting someone with pancreatic cancer
Practical help — driving to appointments, managing medications, keeping track of questions — often matters as much as emotional support.
Listening without trying to fix everything, and following the patient’s lead on how much to discuss, is often what helps most.
Looking after the caregiver
🩺 Physician Note: Caregiver strain is real and well-documented, and caregivers who neglect their own health are less able to sustain support over time. Accepting help, using respite resources, and tending to your own medical and emotional needs is part of caring well for someone else.
The questions to bring to every appointment
Walking into appointments with written questions helps you get the information you need when emotions run high.
Useful questions include: What is my exact diagnosis and stage? Is surgery possible? What is the goal of this treatment? What are the side effects? Am I a candidate for a clinical trial? Has my tumor had molecular and germline testing?
✅ Patient Action: Download our free Questions to Ask Your Oncology Team checklist and appointment tracker to bring to every visit — it keeps the conversations organized and makes sure nothing important gets missed.
Pancreatic cancer: frequently asked questions
1. What are the first signs of pancreatic cancer?
Early pancreatic cancer often causes no symptoms. When signs do appear, the most common include painless jaundice (yellow skin and eyes), unexplained weight loss, upper-abdominal pain that may spread to the back, loss of appetite, and sometimes new-onset diabetes. Many of these have other, more common causes, but persistent symptoms should be evaluated promptly by a physician.
2. Where is pancreatic cancer pain felt?
Pancreatic cancer pain is typically felt in the upper abdomen and may radiate straight through to the middle of the back. It can worsen after eating or when lying flat. Back pain alone is rarely pancreatic, but back pain combined with weight loss or jaundice deserves medical evaluation.
3. Can new-onset diabetes be a sign of pancreatic cancer?
Occasionally, yes. Sudden, unexplained type 2 diabetes in an older adult without typical risk factors — especially alongside weight loss — can sometimes be an early sign of pancreatic cancer. This is uncommon, but the combination is worth raising with your doctor. Discuss any new diagnosis with your physician.
4. What causes pancreatic cancer?
Most cases have no single identifiable cause. Known risk factors include smoking (the largest modifiable risk), obesity, chronic pancreatitis, heavy alcohol use, type 2 diabetes, older age, family history, and certain inherited syndromes such as BRCA mutations. Risk factors raise the odds but do not guarantee the disease.
5. Is pancreatic cancer hereditary?
A minority of cases are linked to inherited gene mutations, including BRCA1, BRCA2, PALB2, Lynch syndrome, and others. If you have multiple relatives with pancreatic cancer or a known hereditary syndrome, genetic counseling can clarify your risk. Ask your doctor whether you qualify for germline testing and surveillance.
6. How is pancreatic cancer diagnosed?
Diagnosis usually involves imaging (a CT scan with pancreatic protocol, sometimes MRI), endoscopic ultrasound to image the tumor closely and take a biopsy, and a biopsy to confirm cancer. The CA 19-9 blood test may support monitoring but is not used to make the diagnosis. Confirm your results and next steps with your specialist.
7. What does a high CA 19-9 mean?
CA 19-9 is a protein often elevated in pancreatic cancer, but it is not a diagnostic or screening test. It can be normal in people who have the cancer and elevated by non-cancer conditions like a blocked bile duct. Doctors mainly use it to track treatment response. Interpret any result with your oncology team.
8. What are the stages of pancreatic cancer?
Pancreatic cancer is staged 0 through IV using the TNM system, based on tumor size, lymph-node involvement, and distant spread. Just as important is the resectability category — resectable, borderline resectable, locally advanced, or metastatic — which determines whether surgery is possible. Ask your team which category applies to you.
9. What does “resectable” mean?
“Resectable” means the tumor can be removed surgically, which offers the best chance of long-term survival. “Borderline resectable” means removal is uncertain and chemotherapy first may help; “locally advanced” usually means surgery isn’t safely possible; “metastatic” means the cancer has spread to distant organs. Ask your surgeon which applies to you.
10. What is the survival rate for pancreatic cancer?
The five-year relative survival rate is about 13% across all stages combined. By stage, it is roughly 44% for localized disease, 17% for regional, and 3% for distant disease. These are population averages from people treated years ago and do not predict any individual’s outcome. Discuss your specific situation with your oncologist.
11. What is the life expectancy for stage 4 pancreatic cancer?
Stage IV (metastatic) pancreatic cancer has a five-year relative survival rate of about 3%, and it is treated with systemic therapy aimed at extending life and controlling symptoms. Individual outcomes vary widely based on biology, treatment response, and overall health, and newer therapies continue to expand options. Talk with your oncologist about your specific prognosis.
12. Can pancreatic cancer be cured?
Surgery offers the only realistic chance of cure, but it is possible in fewer than one in five patients, because most cancers are found after spreading. For others, treatment focuses on extending life and quality of life. Whether surgery is an option depends on your stage and resectability — ask your surgical team.
13. What is the Whipple procedure?
The Whipple procedure (pancreaticoduodenectomy) removes the head of the pancreas along with the duodenum, gallbladder, part of the bile duct, and sometimes part of the stomach, then reconnects the organs. It is the standard operation for resectable tumors in the head of the pancreas. Discuss candidacy and center experience with a surgical oncologist.
14. What is the difference between FOLFIRINOX and NALIRIFOX?
FOLFIRINOX combines fluorouracil, leucovorin, irinotecan, and oxaliplatin. NALIRIFOX is similar but uses liposomal irinotecan (a specially formulated version) and was FDA-approved in 2024 for first-line metastatic disease. Both are intensive regimens for fit patients, and the choice depends on your health and your oncologist’s assessment. Discuss which fits your situation.
15. Should I get biomarker or genetic testing?
Current guidelines recommend molecular profiling of the tumor and germline genetic testing for pancreatic cancer patients, particularly with advanced disease. Testing can uncover mutations — such as BRCA — that open targeted treatments or clinical trials, and can inform your relatives’ risk. Ask your oncologist whether your tumor and germline have been tested.
16. Are there new treatments for pancreatic cancer?
Yes. Recent advances include the 2024 approval of the NALIRIFOX regimen and targeted options like olaparib for inherited BRCA mutations. KRAS-targeted drugs, vaccines, and novel combinations are in active clinical trials but remain investigational. Ask your oncologist about new options and whether a trial fits your situation.
Your next step after reading this
If you have read this far, you are likely frightened, exhausted, or carrying the weight of a decision for someone you love — and that is an entirely human response to a hard disease. You now understand more than most people do walking into their first appointment, and that understanding is something you can use.
Pancreatic cancer is serious, and this guide has not pretended otherwise. But the path forward is real: get an accurate diagnosis and stage, find out whether surgery is possible, make sure your tumor and your genes are tested, and ask about clinical trials.
The single most important thing you can do before your next appointment is to get to a high-volume pancreatic cancer center and ask one question: “Is my cancer resectable, and has my tumor had molecular and germline testing?” That conversation shapes everything that follows.
To go deeper on specific topics, see our guides to the early symptoms of pancreatic cancer, chemotherapy and its side effects, and how immunotherapy works. And download our free Questions to Ask Your Oncology Team checklist to bring to every visit.
Everything in this article is drawn from primary authorities — the NCI, SEER, the American Cancer Society, the NCCN, ASCO, and the FDA — and every clinical figure was verified against those sources, with its date shown, so you can trust what you are reading and check it yourself. We tell you plainly when a number is a population average and when a treatment is still being studied, because the most useful thing we can offer a patient making real decisions is the truth, sourced and in context.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: Internal Medicine (2010); Clinical Pharmacology (2013) Experience: 15 years | Location: San Francisco, California Education: BS Molecular Biology, Caltech (2000); MD/PhD, UCSF School of Medicine (2007);…

Board Certifications: Preventive Medicine (2010); Public Health & General Preventive Medicine (2010) Experience: 15 years | Location: Washington, DC Education: BA Public Policy, Georgetown University (2001); MD, George…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.