Roger, a 58-year-old from California, dismissed his slight weight loss and rising blood sugar as normal aging. His doctor agreed, saying “it probably doesn’t mean anything.” But Roger persisted, and testing revealed stage 2 pancreatic cancer—symptoms he’d been experiencing for months had been quietly escalating while being attributed to other causes. His story illustrates the silent nature of pancreatic cancer symptoms and why early recognition saves lives.
Pancreatic cancer symptoms often appear vague and easily dismissed, but doctors are trained to recognize seven critical warning signs that demand immediate evaluation. These pancreatic cancer warning signs include painless jaundice (yellowing of skin and eyes), unexplained weight loss exceeding 10 pounds, new-onset diabetes in adults over 50, persistent upper abdominal pain, middle to lower back pain unrelieved by position changes, extreme fatigue beyond normal tiredness, and digestive changes like bloating or oily stools.
The early signs of pancreatic cancer are notoriously subtle because the pancreas sits deep in the abdomen, making tumors difficult to detect until they grow large enough to press on surrounding organs or block ducts. Understanding what are the first signs of pancreatic cancer empowers patients to advocate for thorough evaluation when tracking symptoms using tools like a comprehensive symptom checker becomes essential.
⚠️ Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Consult qualified healthcare professionals for diagnosis, treatment, and personalized medical guidance regarding pancreatic cancer symptoms or any health concerns.
Critical Statistics Every Person Should Know
Why early detection of pancreatic cancer matters: The five-year survival rate for pancreatic cancer averages just 13% overall, but this number climbs dramatically to 44% when the disease is caught while still localized to the pancreas. According to the National Cancer Institute’s SEER program, approximately 67,440 Americans will receive a pancreatic cancer diagnosis in 2025, with an estimated 51,980 deaths—making it the third-leading cause of cancer-related mortality despite not being among the most common cancers.
The new-onset diabetes connection represents one of the most significant yet overlooked first signs of pancreatic cancer: Research published through the National Institutes of Health shows that 40-50% of pancreatic cancer patients develop diabetes 6-36 months before their cancer diagnosis, particularly adults over age 50 with no family history of diabetes. Monitoring unexpected metabolic changes through tools like a BMI calculator helps track concerning weight fluctuations that may accompany these pancreatic cancer symptoms.
Early recognition transforms outcomes: When patients and physicians recognize pancreatic cancer warning signs early, treatment options expand significantly, and surgical resection—the only potentially curative approach—becomes possible for localized disease according to Mayo Clinic’s Pancreatic Cancer Early Detection Research Program.
The 7 Critical Symptoms Doctors Never Ignore
The 7 Warning Signs That Demand Immediate Medical Attention
Physicians evaluate pancreatic cancer symptoms through a lens of urgency because the pancreas location deep behind the stomach makes tumors nearly impossible to detect through routine physical examination. The following seven pancreatic cancer warning signs represent the most clinically significant indicators that oncologists and gastroenterologists prioritize when assessing patients, according to the National Cancer Institute’s treatment guidelines.
1. Painless Jaundice (Yellowing Skin and Eyes)
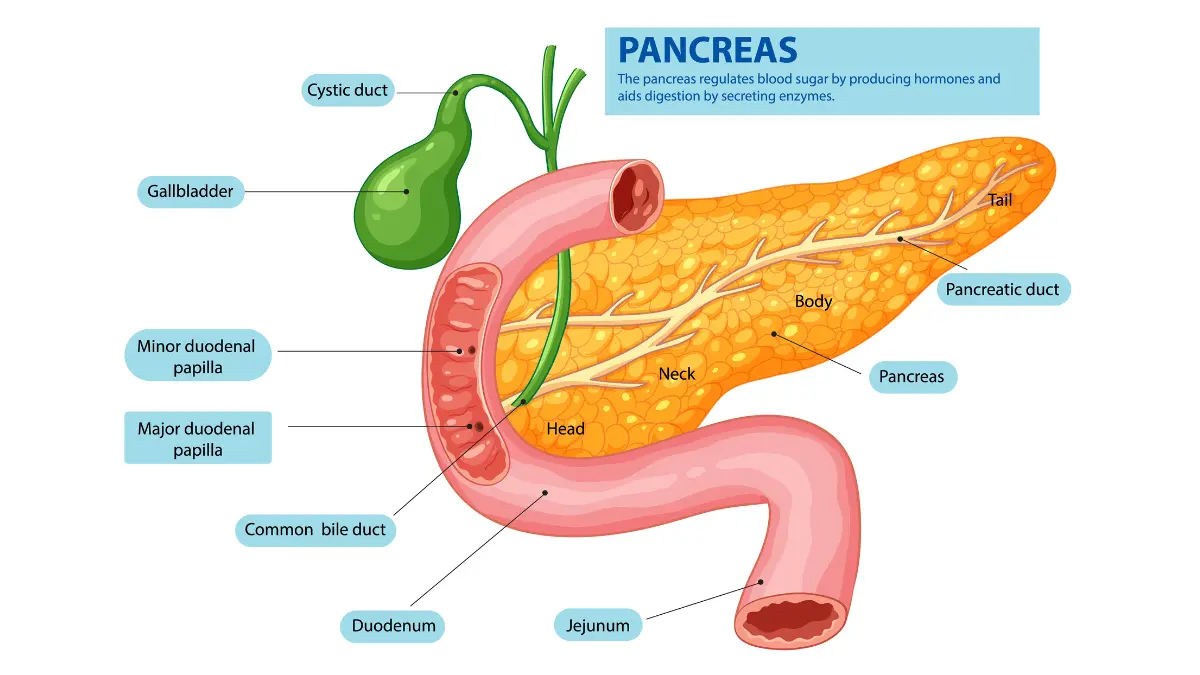
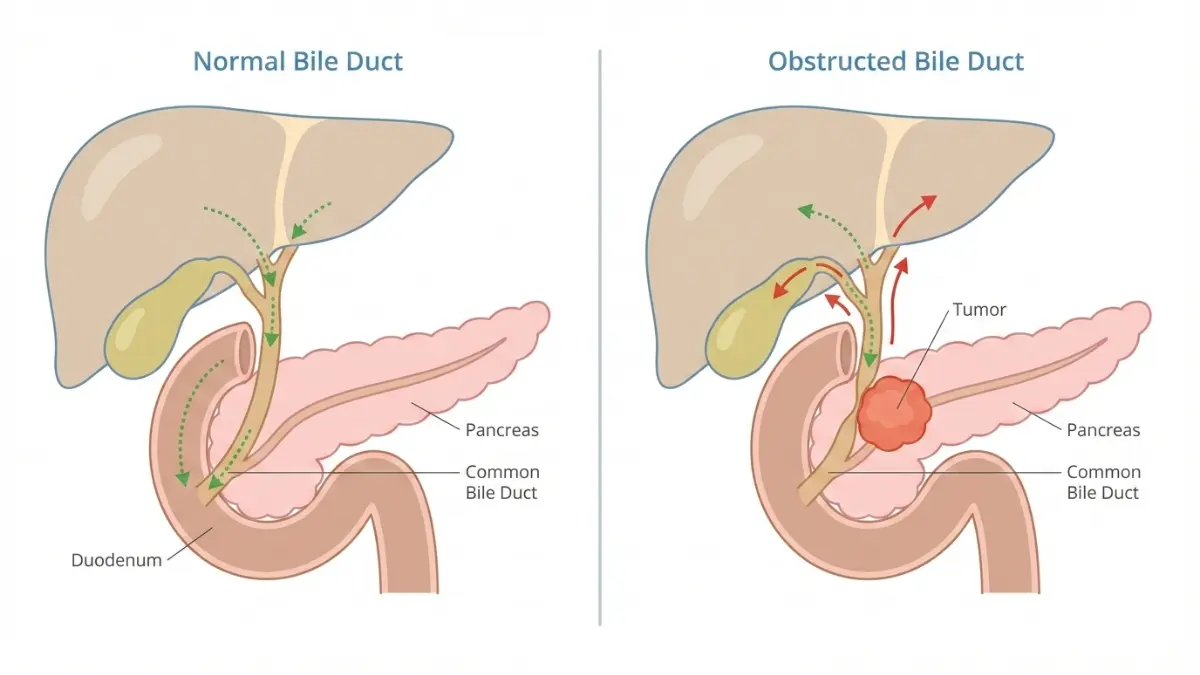
Jaundice stands as one of the earliest and most recognizable signs of pancreatic cancer in the head of the pancreas, where approximately 70% of pancreatic tumors originate. When tumors block the common bile duct—the tube carrying bile from liver to intestine—bilirubin accumulates in the bloodstream, causing the characteristic yellow discoloration of skin and whites of the eyes that the National Cancer Institute describes as a hallmark symptom of bile duct obstruction. Unlike jaundice caused by hepatitis or gallstones that typically presents with pain, pancreatic cancer jaundice often appears painless initially, making it particularly concerning to physicians.
Additional indicators accompanying jaundice:
- Dark, tea-colored urine
- Pale, clay-colored stools
- Severe itching (pruritus) across the body
- Nausea and loss of appetite
⚠️ What This Means For You: If you notice yellowing of your skin or eyes, especially combined with dark urine and pale stools, seek emergency medical evaluation within 24-48 hours. Request specific testing including liver function panels, imaging studies, and CA 19-9 tumor marker assessment through your healthcare provider.
2. Unexplained Weight Loss (10+ Pounds Without Trying)
Weight loss represents a cardinal symptom of pancreatic cancer, with research published through the National Institutes of Health showing that 85% of patients present with weight loss at diagnosis, and nearly half of early-stage patients exhibit preoperative weight loss. The mechanisms driving this early sign of pancreatic cancer include pancreatic exocrine insufficiency—when tumors prevent digestive enzyme production—combined with tumor-induced cachexia and decreased appetite. Tracking weight changes through tools like a BMI calculator or weight loss calculator helps identify concerning patterns requiring medical investigation.
Gender differences in weight loss presentation: Women frequently report progressive weight loss combined with bloating and early satiety, while men more commonly experience rapid weight loss exceeding 15 pounds within 2-3 months. Understanding these signs of pancreatic cancer in women versus signs of pancreatic cancer in men helps tailor symptom recognition strategies.
| Normal Weight Fluctuation | Concerning Weight Loss Pattern |
|---|---|
| 2-5 pounds over several months | 10+ pounds in 1-2 months without diet changes |
| Gradual, with identifiable cause | Rapid, unexplained, progressive |
| Appetite remains normal | Loss of appetite, early fullness |
| Energy levels stable | Accompanied by fatigue, weakness |
⚠️ What This Means For You: Document unintentional weight loss exceeding 10 pounds, especially when accompanied by changes in appetite or digestive function. Consult your physician to evaluate for pancreatic exocrine insufficiency and request comprehensive metabolic testing.
3. New-Onset Diabetes or Uncontrolled Blood Sugar
New-onset diabetes in adults over 50 with no family history represents one of the most significant yet frequently overlooked first signs of pancreatic cancer. Groundbreaking research published in the NIH’s journal system reveals that pancreatic tumors trigger diabetes through TGF-β signaling, which causes selective depletion of insulin-producing beta cells months before cancer diagnosis becomes clinically apparent. The National Institutes of Health confirms that 40-50% of pancreatic cancer patients develop glucose intolerance or frank diabetes 6-36 months preceding their diagnosis. Monitoring blood sugar levels with a blood sugar converter helps track metabolic changes that may signal underlying pancreatic dysfunction.
Red flags that distinguish cancer-related diabetes:
- Sudden diabetes diagnosis in lean adults over age 50
- Blood sugar difficult to control despite medication
- Weight loss accompanying the diabetes diagnosis
- No family history of diabetes
⚠️ What This Means For You: If you develop diabetes suddenly after age 50, especially with concurrent weight loss, request pancreatic imaging (CT or MRI) and CA 19-9 tumor marker testing. Early pancreatic cancer detection in this population improves outcomes significantly.
4. Persistent Upper Abdominal Pain
Pancreatic cancer abdominal pain typically presents as persistent discomfort in the upper abdomen that radiates toward the sides, often described by patients as a gnawing or burning sensation that steadily worsens. According to the American Cancer Society’s symptom guidelines, this pancreatic cancer stomach pain occurs when tumors grow large enough to press on surrounding organs or when cancer spreads to nerves around the pancreas. Using a symptom checker to document pain location, intensity, timing, and associated symptoms provides valuable diagnostic information for healthcare providers.
| Pancreatitis Pain | Pancreatic Cancer Pain |
|---|---|
| Sudden, severe onset | Gradual, progressively worsening |
| Sharp, stabbing quality | Dull, aching, gnawing sensation |
| Improves after acute episode | Persistent, continuous |
| Related to food/alcohol intake | Unrelated to eating patterns |
5. Middle to Lower Back Pain (Unrelieved by Position Change)
Pancreatic cancer back pain develops when tumors in the body or tail of the pancreas grow large enough to press on the nerve bundles of the celiac plexus, creating referred pain between the shoulder blades or in the mid-to-lower back region. Oncologists recognize this as a concerning symptom because the pain characteristically fails to improve with position changes, physical therapy, or standard analgesics—distinguishing it from mechanical back problems. Key distinguishing feature: The pain often intensifies when lying flat and improves slightly when sitting up or leaning forward, a pattern that signals retroperitoneal involvement requiring immediate evaluation.
⚠️ What This Means For You: Back pain that persists for more than 2-3 weeks without injury, combined with any digestive symptoms or weight loss, warrants comprehensive evaluation including pancreatic imaging. Track your symptoms carefully and maintain adequate nutrition using tools like a macro calculator to ensure proper nutrient intake during the diagnostic process.
6. Extreme Fatigue and Weakness
Pancreatic cancer fatigue differs fundamentally from normal tiredness—it represents profound, unrelenting exhaustion that fails to improve with rest and progressively interferes with daily activities. Research through the National Institutes of Health examining fatigue in pancreatic cancer patients identified that anemia, pain, and significant weight loss (exceeding 16 kg in six months) correlate strongly with severe fatigue perception. The University of Pennsylvania’s research demonstrates that pancreatic enzyme deficiency leads to malnutrition and subsequent energy depletion even when patients maintain adequate food intake. Assessing overall health status through a body fat percentage calculator alongside tracking energy levels helps identify concerning nutritional decline patterns.
Clinical factors underlying extreme fatigue:
- Anemia from tumor-related bleeding
- Malnutrition due to enzyme deficiency
- Tumor-produced inflammatory cytokines
- Poor sleep quality from pain
⚠️ What This Means For You: Fatigue that prevents normal activities, especially combined with other pancreatic cancer symptoms like weight loss or abdominal discomfort, requires thorough medical investigation including complete blood count, metabolic panels, and consideration of pancreatic evaluation.
7. Digestive Changes (Bloating, Floating Stools, Loss of Appetite)
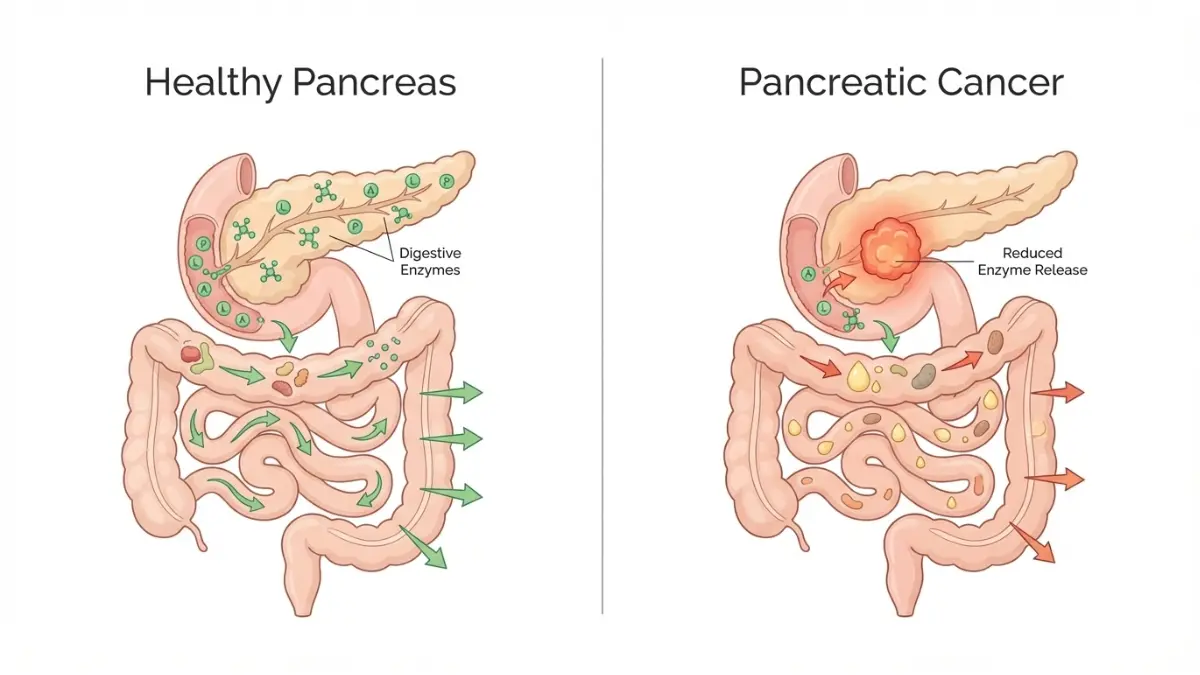
Pancreatic cancer bloating and distinctive stool changes occur when tumors disrupt pancreatic enzyme production, leading to pancreatic exocrine insufficiency. The NIH’s research on pancreatic exocrine insufficiency defines steatorrhea—fatty, floating stools that appear oily or clay-colored—as the hallmark sign of inadequate fat digestion resulting from lipase and trypsin levels falling below 5-10% of normal. These what are the first signs of pancreatic cancer digestive manifestations include persistent bloating, excessive gas, diarrhea alternating with constipation, and foul-smelling stools that float due to high fat content. Maintaining proper nutrition becomes critical, and tools like a calorie deficit calculator help ensure adequate intake despite digestive challenges.
Visual indicators demanding evaluation:
- Stools that float and are difficult to flush
- Oily film or sheen visible in toilet water
- Pale, clay-colored bowel movements
- Unexplained bloating after normal portions
⚠️ What This Means For You: Persistent digestive changes lasting more than 2-3 weeks, especially steatorrhea combined with weight loss, require evaluation for pancreatic exocrine insufficiency. Request fecal elastase testing and pancreatic imaging if symptoms persist despite dietary modifications.
Gender-Specific & High-Risk Populations
How Pancreatic Cancer Symptoms Differ Across Populations
Understanding how pancreatic cancer symptoms manifest differently across gender, age, and ethnic populations enables more targeted recognition of early signs of pancreatic cancer and improves detection rates among high-risk groups. The National Cancer Institute’s SEER database reveals critical disparities in both incidence and mortality patterns that healthcare providers use to assess individual risk profiles.
Symptoms in Women vs. Men
Gender influences both the presentation and recognition of signs of pancreatic cancer in women compared to signs of pancreatic cancer in men, with men experiencing 26% higher incidence rates than women according to SEER population statistics (15.5 per 100,000 males versus 12.3 per 100,000 females). Research indicates this disparity may partially stem from higher historical tobacco use among men, though biological factors including hormonal influences on pancreatic tissue also contribute.
| Symptom Presentation | Women More Likely To Experience | Men More Likely To Experience |
|---|---|---|
| Primary Symptoms | Digestive issues, bloating, nausea | Back pain as initial symptom |
| Weight Loss Pattern | Gradual with appetite changes | Rapid, dramatic (15+ pounds) |
| Pain Description | Diffuse abdominal discomfort | Localized upper abdominal pain |
| Associated Symptoms | Early satiety, food aversion | Jaundice presentation earlier |
| Diagnostic Timing | Often diagnosed at younger age in neuroendocrine variants | Typically diagnosed around age 70 |
Women frequently report pancreatic cancer symptoms including progressive bloating and early fullness that may be initially attributed to gynecological or gastrointestinal conditions, delaying pancreatic evaluation. Men more commonly present with pancreatic cancer back pain and rapid weight loss as prominent first signs of pancreatic cancer. Tracking these gender-specific patterns through an ideal weight calculator or body fat calculator helps identify concerning deviations requiring medical assessment.
Age-Related Risk Factors
Age represents the single strongest demographic risk factor for pancreatic cancer, with incidence rising dramatically after age 45 and peaking in the 65-74 age bracket. According to the American Cancer Society, approximately two-thirds of pancreatic cancer patients receive their diagnosis at age 65 or older, with the average age at diagnosis reaching 70 years. The National Cancer Institute’s SEER program data confirms that pancreatic cancer remains relatively rare before age 45, with lifetime risk at approximately 1.6% for both men and women.
Age-specific pancreatic cancer warning signs patterns:
- Under 50: Young-onset cases typically linked to hereditary genetic syndromes including BRCA1/BRCA2 mutations, Lynch syndrome, or familial atypical multiple mole melanoma (FAMMM) syndrome
- 50-64 years: New-onset diabetes emerges as critical early detection opportunity, particularly in lean individuals without family history
- 65+ years: Classic symptom presentation including jaundice, weight loss, and abdominal pain becomes more common
Research published through the National Institutes of Health identifying inherited pancreatic cancer genes emphasizes that BRCA2 mutation carriers face a 3.5-7% lifetime pancreatic cancer risk compared to 1.6% in the general population, with relatives developing disease approximately 10 years earlier than sporadic cases. Individuals with family history should utilize a genetic risk assessment tool to evaluate hereditary cancer syndrome probability and discuss genetic testing with healthcare providers.
Ethnic and Racial Disparities
Stark racial disparities characterize pancreatic cancer incidence and mortality, with the SEER database documenting that non-Hispanic Black Americans experience the highest rates at 17.9 per 100,000 for men and 15.4 per 100,000 for women—representing 50-90% higher incidence than non-Hispanic White populations. Groundbreaking research through the NIH examining ethnic and racial disparities in pancreatic cancer mortality identifies that Black/African American individuals face approximately 50% higher mortality rates and experience more aggressive cachexia (severe weight loss and muscle wasting) compared to other racial groups.
Factors contributing to disparities include:
- Disproportionate poverty and insurance access barriers
- Lower rates of surgical resection (20-40% less likely to undergo curative surgery)
- Diagnosis at younger ages and more advanced stages
- Higher prevalence of risk factors including diabetes and obesity
- Geographic distance from specialized pancreatic cancer centers
⚠️ What This Means For You: Black Americans and other high-risk populations experiencing any pancreatic cancer symptoms should proactively request comprehensive evaluation including CA 19-9 tumor markers and pancreatic imaging, particularly when new-onset diabetes or unexplained weight loss occurs. Utilizing health resources like a BMI calculator to monitor body composition changes and accessing health guidance helps facilitate early conversations with healthcare providers about pancreatic cancer risk factors.
Research published through the NIH examining racial disparities emphasizes that early diagnosis and treatment of cachexia may represent a critical avenue to improve health equity and survival outcomes in disproportionately affected populations. Advocating for equitable access to screening, genetic counseling through a genetic risk assessment tool, and timely diagnostic imaging remains essential for reducing mortality gaps.
Early Detection & Diagnosis Process
How to Detect Pancreatic Cancer Early: Tests Doctors Recommend
Understanding how to detect pancreatic cancer early remains the greatest challenge in improving survival outcomes, yet recognizing pancreatic cancer warning signs and pursuing appropriate diagnostic testing when symptoms emerge offers the best opportunity for successful intervention. The National Cancer Institute’s research programs emphasize that no universal screening tests currently exist for average-risk populations, making symptom awareness and targeted high-risk surveillance essential strategies.
Why Early Detection Is So Difficult
The pancreatic cancer early detection challenge stems from multiple anatomical and biological factors that allow tumors to grow undetected until reaching advanced stages. The pancreas location deep behind the stomach and other abdominal organs makes physical examination impossible and prevents routine imaging from detecting small lesions. Research published through the NIH examining endoscopic ultrasound effectiveness confirms that even CT scans miss 25-67% of pancreatic cancers smaller than 2 centimeters, highlighting why symptomatic presentation typically indicates more advanced disease.
The absence of reliable blood-based screening tests compounds detection difficulties, as the most commonly used biomarker CA 19-9 lacks sufficient sensitivity for early-stage disease. According to NIH research analyzing CA 19-9 clinical utility, serum levels demonstrate only 79-81% sensitivity and 82-90% specificity in symptomatic patients, while producing too many false positives in asymptomatic populations to serve as an effective screening tool. Promising advances include the National Cancer Institute’s research on liquid biopsy techniques that analyze microRNA signatures, achieving 91-97% accuracy when combined with CA 19-9 testing in validation studies.
Diagnostic Tests and Procedures
When pancreatic cancer symptoms warrant investigation, physicians employ a structured diagnostic approach combining blood tests, imaging studies, and tissue confirmation. Understanding this process helps patients advocate effectively for thorough evaluation when first signs of pancreatic cancer appear.
Comprehensive pancreatic cancer diagnosis typically includes:
- CA 19-9 tumor marker blood test – Elevated levels (>37 U/mL) combined with weight loss exceeding 20 pounds and jaundice provide nearly 100% specificity for pancreatic cancer diagnosis in symptomatic patients according to NIH biomarker research. Track metabolic changes using a weight loss calculator to provide precise data during medical consultations.
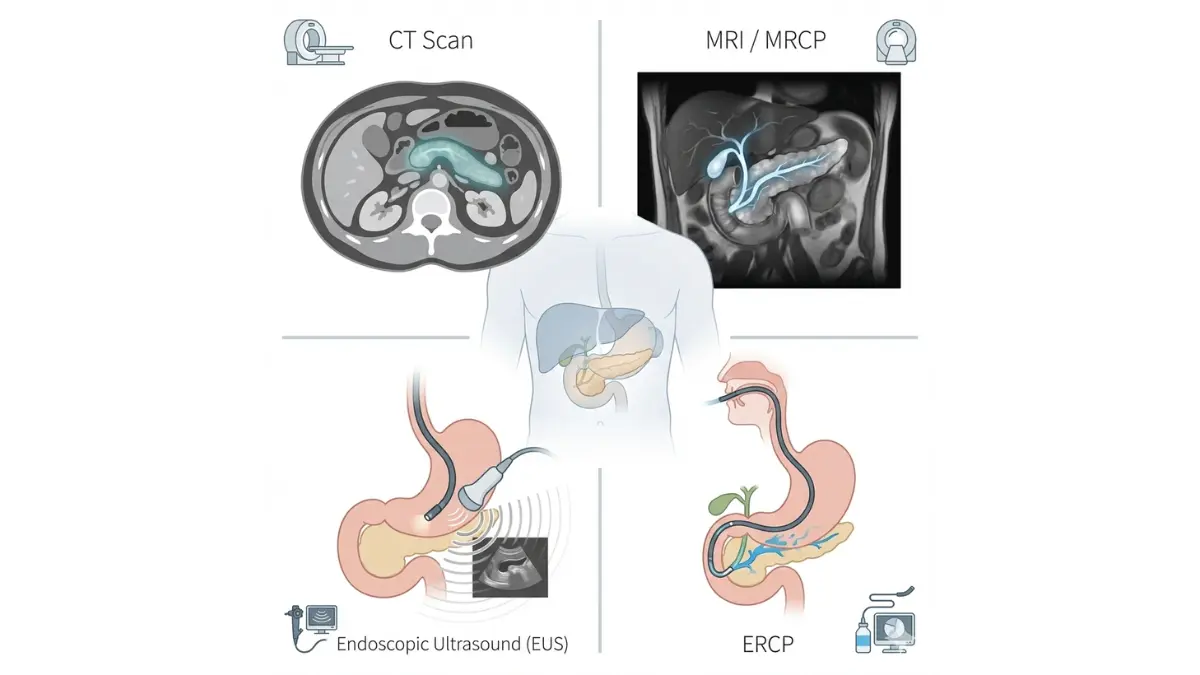
- CT (computed tomography) imaging – Contrast-enhanced pancreatic protocol CT scans represent the initial imaging modality for evaluating suspected pancreatic masses, though sensitivity drops to 33-75% for tumors under 1 centimeter. The University of Chicago research confirms that CT and MRI imaging form the diagnostic foundation when combined with clinical presentation.
- Endoscopic ultrasound (EUS) – The NIH identifies EUS as the most sensitive imaging modality for detecting pancreatic lesions, achieving 94% overall sensitivity and detecting tumors as small as 2-5 millimeters that other imaging misses. EUS proves particularly valuable when CT scans show indeterminate findings, with 85% sensitivity for detecting tumors not visible on standard imaging.
- ERCP (endoscopic retrograde cholangiopancreatography) – This specialized procedure evaluates pancreatic duct abnormalities and obtains pancreatic juice samples for cytologic analysis, particularly useful in very early-stage pancreatic cancer when imaging remains inconclusive according to NIH research on ERCP diagnostic roles.
- Biopsy confirmation – EUS-guided fine needle aspiration provides tissue diagnosis with high sensitivity and specificity, enabling pathological confirmation before treatment initiation.
⚠️ What This Means For You: Timeline expectations vary by test availability—initial CA 19-9 results typically return within 3-5 days, CT imaging schedules within 1-2 weeks, while EUS procedures may require 2-4 weeks at specialized centers. Utilizing a symptom checker to document symptom progression during diagnostic evaluation helps physicians prioritize urgent cases.
Screening Recommendations for High-Risk Individuals
The National Cancer Institute’s surveillance guidelines recommend annual pancreatic screening only for individuals meeting specific high-risk criteria, as screening average-risk populations produces excessive false positives without mortality benefit. Current recommendations published through National Comprehensive Cancer Network protocols target three primary high-risk groups.
Who qualifies for pancreatic cancer screening:
- Hereditary genetic syndrome carriers – Individuals with BRCA1, BRCA2, PALB2, or ATM mutations face 3.5-13 fold increased pancreatic cancer risk, warranting annual MRI/EUS surveillance beginning at age 50 or 10 years younger than the youngest family member’s diagnosis. The National Cancer Institute’s genetic testing resources explain that Lynch syndrome, Peutz-Jeghers syndrome, and familial atypical multiple mole melanoma syndrome also elevate risk substantially.
- Strong family history – Two or more first-degree relatives with pancreatic cancer, regardless of identified genetic mutations, qualify for surveillance according to cancer genetics risk assessment guidelines published by the National Cancer Institute. Access a genetic risk assessment tool to evaluate whether family history warrants genetic counseling.
- Chronic pancreatitis patients – Long-standing pancreatic inflammation increases cancer risk 13-fold, particularly in hereditary pancreatitis with PRSS1 mutations.
⚠️ What This Means For You: If you meet high-risk criteria, request referral to a specialized pancreatic surveillance program offering annual contrast-enhanced MRI with magnetic resonance cholangiopancreatography (MRCP) or EUS examination. The University of Chicago’s early detection program exemplifies centers providing comprehensive surveillance protocols.
The Role of New-Onset Diabetes as an Early Warning
New-onset diabetes in adults over 50 represents a critical yet underutilized opportunity for pancreatic cancer early detection, as research demonstrates that 40-50% of patients develop glucose intolerance 6-36 months before diagnosis. The NCI’s search for early detection biomarkers emphasizes that sudden diabetes combined with weight loss should trigger immediate pancreatic evaluation.
Red flags demanding pancreatic imaging:
- Diabetes diagnosis after age 50 in lean individuals (BMI <25)
- Diabetes combined with 10+ pounds unintentional weight loss
- Poorly controlled blood sugar despite medication
- No family history of diabetes
⚠️ What This Means For You: If you develop diabetes suddenly after age 50, especially with concurrent weight loss tracked through a BMI calculator or calorie deficit calculator, explicitly request pancreatic protocol CT or MRI imaging in addition to standard diabetes management. The National Cancer Institute emphasizes that adding annual CA 19-9 blood tests to diabetes monitoring may improve early-stage pancreatic cancer detection in this population.
Stages, Survival Rates & Treatment Overview
Understanding Pancreatic Cancer Stages and Prognosis
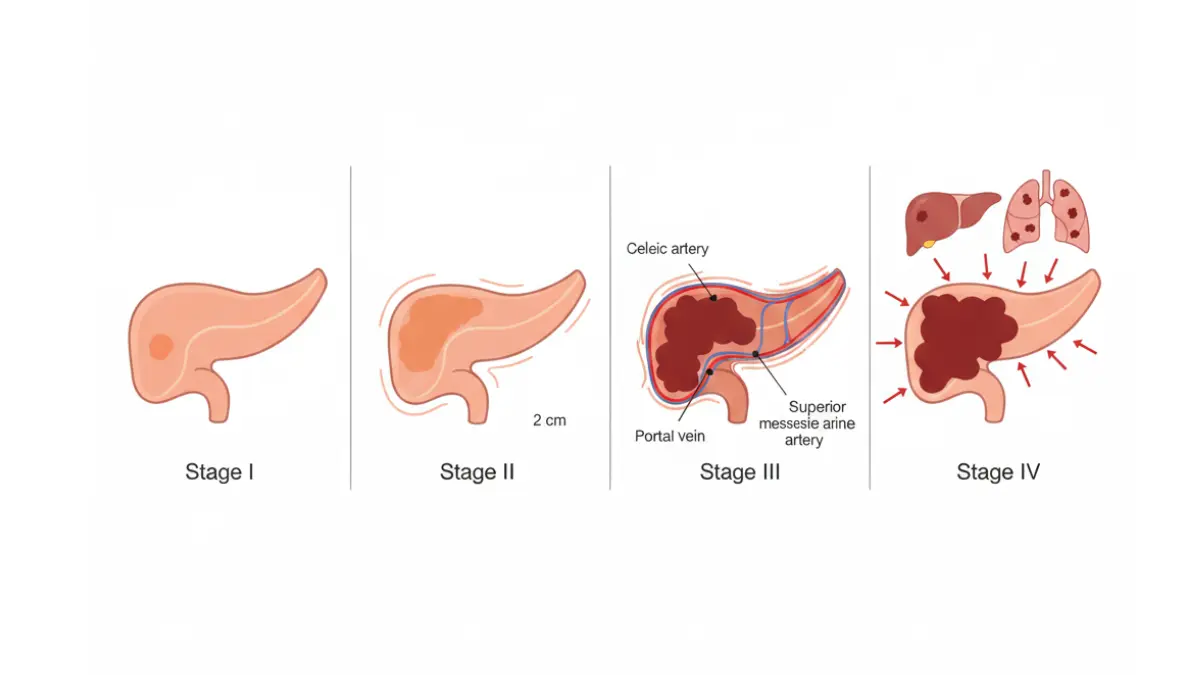
Pancreatic cancer stages provide the critical framework for determining treatment options and expected outcomes when patients present with pancreatic cancer symptoms. The TNM (tumor, node, metastasis) staging system developed by the American Joint Committee on Cancer evaluates tumor size and location, lymph node involvement, and distant metastasis to categorize disease from stage 0 through stage 4.
The Four Stages Explained
The SEER training program documents how pancreatic cancer staging directly influences surgical eligibility and treatment planning. Understanding these stages helps patients comprehend their diagnosis and advocate for appropriate care when tracking symptoms through a symptom checker during the diagnostic process.
The critical distinction between resectable, borderline resectable, and unresectable disease determines whether surgery—the only potentially curative approach—remains viable according to National Cancer Institute treatment guidelines. Tumors invading major arteries or extensively involving the superior mesenteric vein typically preclude surgical resection.
Survival Rate Context
The pancreatic cancer survival rate varies dramatically based on disease stage at diagnosis, with American Cancer Society data from SEER showing that localized disease carries 44% five-year survival versus only 3% for metastatic disease. These survival rates represent averages from thousands of patients diagnosed between 2014-2020, not predictions for any individual patient. Recent treatment advances including combination chemotherapy regimens (FOLFIRINOX and gemcitabine plus nab-paclitaxel) have improved outcomes beyond these historical statistics.
Understanding relative survival rates: The National Cancer Institute explains that relative survival compares pancreatic cancer patients to the general population, accounting for age and other health factors unrelated to cancer. One-year survival reaches 46% overall, while ten-year survival remains at approximately 2% across all stages combined. Maintaining optimal nutritional status through tools like a protein intake calculator and macro calculator supports better treatment tolerance and outcomes.
Treatment Approaches Overview
The National Cancer Institute’s comprehensive treatment protocols outline multimodal therapeutic strategies tailored to disease stage and patient fitness.
Primary treatment modalities include:
- Whipple procedure (pancreaticoduodenectomy) – The gold standard surgery for early-stage pancreatic cancer located in the pancreatic head, as University of California San Francisco’s surgical oncology program details, involves removing the pancreatic head, duodenum, gallbladder, and portion of the bile duct with subsequent reconstruction. UC San Diego research shows this complex procedure takes 4-6 hours and offers the only curative potential for resectable disease.
- Chemotherapy and radiation – The NCI treatment guidelines identify combination chemotherapy (FOLFIRINOX or gemcitabine/nab-paclitaxel) as primary treatment for locally advanced and metastatic disease, with chemoradiation often used for borderline resectable tumors.
- Targeted therapy and immunotherapy – Research through the National Cancer Institute’s drug development programs demonstrates that KRAS inhibitors combined with chemotherapy substantially extend survival in mice models, with human clinical trials ongoing. However, NIH research on immunotherapy trials acknowledges that checkpoint inhibitors and vaccine strategies have shown limited efficacy in pancreatic cancer due to the tumor’s immunosuppressive microenvironment.
- Clinical trials for advanced cases – The National Cancer Institute maintains comprehensive trial databases exploring novel therapeutic combinations and biomarker-directed treatments.
⚠️ What This Means For You: Questions to ask your oncology team include: “What is my specific TNM stage?” “Am I a surgical candidate?” “Which chemotherapy regimen do you recommend and why?” “Are there clinical trials appropriate for my situation?” Using a genetic risk assessment tool may identify hereditary mutations qualifying you for targeted therapy trials.
Quality of Life and Symptom Management
Palliative care integration at diagnosis—not just end-of-life—significantly improves quality of life according to Johns Hopkins research on concurrent palliative interventions that showed nurse-led symptom management reduced psychological distress while maintaining treatment tolerance. The NIH’s research on palliative care effectiveness emphasizes aggressive pain control, nutritional support with pancreatic enzyme replacement, and early hospice discussions as essential components of comprehensive pancreatic cancer care. Maintaining adequate caloric intake through a calorie deficit calculator and proper hydration via a water intake calculator helps combat cachexia and preserves strength during treatment.
Action Steps & Prevention Strategies
What You Can Do Today to Protect Your Health
Recognizing pancreatic cancer symptoms early and implementing evidence-based prevention strategies dramatically improves outcomes, though most symptoms have benign causes that warrant evaluation rather than panic.
Immediate Action Steps If You Have Symptoms
If you’re experiencing any pancreatic cancer warning signs described in this article, take these priority steps immediately:
- Document all symptoms with dates and severity – Track symptom progression using a comprehensive symptom checker and note patterns related to eating, position changes, or time of day.
- Schedule appointment with your primary care physician within 1 week – Present documented symptoms and explicitly request pancreatic evaluation if you have concerning combinations like jaundice with weight loss, new diabetes after age 50, or persistent back pain with digestive changes.
- Request specific diagnostic tests – Ask for CA 19-9 tumor marker blood test, pancreatic protocol CT imaging, comprehensive metabolic panel, and liver function tests based on your symptom constellation.
- Bring complete family medical history documentation – The National Cancer Institute emphasizes that family history of pancreatic, breast, ovarian, or colorectal cancers may indicate hereditary syndromes requiring genetic evaluation through a genetic risk assessment tool.
⚠️ Don’t wait for symptoms to worsen—early intervention saves lives. What are the first signs of pancreatic cancer often appear vague initially but progress steadily, making prompt medical evaluation essential when multiple symptoms cluster together.
Lifestyle Modifications to Reduce Risk
While certain pancreatic cancer risk factors like age and genetics remain unmodifiable, research through the National Institutes of Health demonstrates that lifestyle interventions can reduce pancreatic cancer risk by more than 50% when combining healthy dietary patterns with other protective behaviors.
Evidence-based risk reduction strategies include:
- Quit smoking immediately – The National Cancer Institute’s comprehensive smoking cessation guidelines confirm that tobacco use accounts for 20-35% of pancreatic cancer cases, with risk declining substantially within 5-10 years after quitting. Access federal smoking cessation resources offering counseling, nicotine replacement therapy, and behavioral support programs proven effective in cancer prevention.
- Maintain healthy weight through proper nutrition – NIH research on dietary patterns shows that a “Prudent” diet rich in vegetables, fruits, fish, poultry, whole grains, and low-fat dairy reduces pancreatic cancer risk by approximately 50% compared to Western diets high in red meat, processed foods, and refined sugars. Calculate optimal caloric needs using a calorie deficit calculator and track macronutrient balance through a macro calculator to achieve and maintain your ideal weight.
- Limit alcohol consumption – Excessive alcohol intake increases chronic pancreatitis risk, which elevates pancreatic cancer likelihood 13-fold according to NIH prevention research. Moderate consumption to ≤1 drink daily for women or ≤2 drinks for men.
- Engage in regular physical activity – The National Cancer Institute’s prevention overview identifies regular exercise as protective against multiple cancer types including pancreatic cancer, particularly when combined with weight management. Track fitness progress through a heart rate zone calculator or pace calculator to optimize cardiovascular benefits.
- Manage metabolic syndrome components – Research published through the NIH demonstrates that recovering from metabolic syndrome—characterized by high blood pressure, elevated blood sugar, excess abdominal fat, and abnormal cholesterol—reduces pancreatic cancer risk substantially. Monitor metabolic health using a BMI calculator, body fat calculator, and blood sugar converter to track improvements.
Final Reassurance
Knowledge empowers action, not fear. Most digestive symptoms, weight changes, and abdominal discomfort have benign explanations unrelated to pancreatic cancer. However, understanding the specific combinations that concern physicians—painless jaundice, new diabetes after 50, unexplained weight loss exceeding 10 pounds, persistent pain patterns—enables you to advocate effectively for thorough evaluation when warranted.
Early recognition of first signs of pancreatic cancer transforms outcomes, as SEER data documents that five-year survival rates reach 44% for localized disease compared to just 3% for metastatic disease. Explore additional health guidance and resources at MyMedicineAdvisor.com to support your wellness journey and empower informed health decisions.
Frequently Asked Questions About Pancreatic Cancer Symptoms
1. What are the first signs of pancreatic cancer?
The first signs of pancreatic cancer typically include unexplained weight loss (10+ pounds), new-onset diabetes after age 50, persistent upper abdominal pain, and subtle digestive changes like bloating or loss of appetite. Painless jaundice (yellowing skin and eyes) often appears as an early warning sign when tumors block the bile duct.
2. Does pancreatic cancer cause back pain?
Yes, pancreatic cancer back pain occurs in 25-50% of patients, typically presenting as middle to lower back pain that worsens when lying flat and improves when leaning forward. This pain results from tumors pressing on nerve bundles and doesn’t respond to typical pain relievers or position changes.
3. How does pancreatic cancer cause weight loss?
Pancreatic cancer weight loss happens through three mechanisms: tumors disrupt pancreatic enzyme production preventing proper food digestion, cancer cells produce inflammatory substances causing cachexia (muscle wasting), and patients often lose appetite due to early satiety and nausea. Weight loss exceeding 10 pounds without trying warrants immediate evaluation.
4. Can pancreatic cancer be detected early?
Pancreatic cancer early detection remains challenging because the pancreas sits deep behind the stomach, making tumors invisible during physical exams. No routine screening exists for average-risk individuals, but high-risk people with family history or genetic mutations (BRCA1/2) should undergo annual MRI/EUS surveillance starting at age 50.
5. What is the connection between diabetes and pancreatic cancer?
New-onset diabetes pancreatic cancer connection affects 40-50% of patients who develop glucose intolerance 6-36 months before cancer diagnosis. Pancreatic tumors trigger diabetes through disruption of insulin-producing cells. Adults over 50 who suddenly develop diabetes without family history should request pancreatic imaging.
6. Are pancreatic cancer symptoms different in women and men?
Yes, signs of pancreatic cancer in women more commonly include digestive issues, bloating, and gradual weight loss, while signs of pancreatic cancer in men typically present with back pain as the initial symptom and more rapid dramatic weight loss. Men experience 26% higher incidence rates than women overall.
7. What does pancreatic cancer jaundice look like?
Pancreatic cancer jaundice appears as yellowing of the skin and whites of the eyes, accompanied by dark tea-colored urine, pale clay-colored stools, and severe itching across the body. Unlike hepatitis-related jaundice, pancreatic cancer jaundice typically presents painlessly initially, making it particularly concerning to physicians.
8. How long can you have pancreatic cancer without knowing?
Most people have pancreatic cancer for months to years without knowing because early-stage tumors rarely cause symptoms. Approximately 90% of pancreatic cancers lack symptoms until reaching advanced stages. The average time from symptom onset to diagnosis ranges from 4-8 months.
9. What are the survival rates for pancreatic cancer?
Pancreatic cancer survival rate varies by stage: localized disease has 44% five-year survival, regional spread drops to 16%, and distant metastasis has only 3% five-year survival. Overall five-year survival averages 13%, but recent treatment advances are improving these outcomes beyond historical statistics.
10. Who is at highest risk for pancreatic cancer?
Highest-risk groups include adults over 65, smokers (20-35% of cases), individuals with family history or genetic mutations (BRCA1/2, Lynch syndrome), chronic pancreatitis patients (13-fold increased risk), and Black Americans who experience 50-90% higher incidence than other racial groups.
11. When should I see a doctor about potential pancreatic cancer symptoms?
See a doctor immediately if you experience painless jaundice, new diabetes after age 50 with weight loss, unexplained weight loss exceeding 10 pounds in 1-2 months, persistent upper abdominal or back pain lasting 2+ weeks, or digestive changes including floating oily stools. Document symptoms and request specific pancreatic evaluation including CA 19-9 testing and imaging.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











