
On This Page – Quick Medical Summary
Understanding Your Diagnosis & What 2025 Data Reveals
Small cell lung cancer survival rates vary dramatically from 3% for distant metastatic disease to 27-30% for localized tumors caught early, with 2025 bringing unprecedented hope through FDA-approved tarlatamab immunotherapy and combination treatments that have extended median survival to 25.3 months in extensive-stage patients. This represents the most significant treatment breakthrough in SCLC history, fundamentally changing what physicians can offer newly diagnosed patients.
Sarah’s Story: Finding Hope in 2025
When 58-year-old Sarah (name changed for privacy) received her extensive stage small cell lung cancer diagnosis in March 2024, her oncologist told her the median survival was 10-13 months with standard chemotherapy. Eighteen months later, Sarah is thriving on tarlatamab maintenance therapy after completing first-line treatment, representing a growing cohort of patients benefiting from advances outlined in the National Cancer Institute’s updated treatment guidelines. Her tumor markers remain undetectable, and she recently used our BMI Calculator to track her nutritional recovery during treatment, maintaining healthy weight despite chemotherapy side effects. “I was prepared for the worst, but the new immunotherapy options gave me my life back,” Sarah shares, emphasizing how 2025’s treatment landscape differs radically from even two years ago.
What Is Small Cell Lung Cancer?
Small cell lung cancer (SCLC) represents approximately 10-15% of all lung cancer cases, classified as a high-grade neuroendocrine tumor that grows and spreads more aggressively than non-small cell lung cancer. Small cell carcinoma cells appear smaller under microscopy with less cytoplasm, distinguishing them from other lung cancer types. This aggressive malignancy typically originates in the bronchi (central airways) and demonstrates rapid doubling time, often metastasizing to lymph nodes, liver, bones, adrenal glands, and brain before diagnosis. According to CDC lung cancer statistics, smoking causes approximately 95% of small cell lung cancer cases, making it largely preventable.
2025’s Game-Changing Breakthrough: Why This Year Is Different
November 19, 2025 marked a historic milestone when the FDA granted traditional approval to tarlatamab (Imdelltra) for extensive stage small cell lung cancer, making it the first bispecific T-cell engager approved for any solid tumor. The DeLLphi-304 trial demonstrated that patients receiving tarlatamab maintenance therapy after chemotherapy achieved a median overall survival of 25.3 months—nearly double historical outcomes. Additionally, durvalumab consolidation therapy for limited stage small cell lung cancer has extended median survival to 55.9 months, transforming SCLC prognosis from universally grim to cautiously optimistic. If you’re experiencing concerning respiratory symptoms, our Symptom Checker can help identify patterns worth discussing with your physician, though it cannot replace professional medical evaluation.
Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Small cell lung cancer treatment decisions should be made in consultation with board-certified oncologists familiar with your specific case, staging, and medical history. Always seek professional medical guidance for diagnosis and treatment.
Understanding Small Cell Lung Cancer Stages & Survival Rates
How Small Cell Lung Cancer Stages Determine Your Survival Odds
Stage at diagnosis remains the single most powerful predictor of small cell lung cancer prognosis, with localized disease offering 30-34% five-year survival compared to just 3-4% for distant metastatic spread. The National Cancer Institute staging system divides SCLC into two primary categories—limited stage and extensive stage—based on whether the cancer can be safely encompassed within a single radiation field. Understanding your specific stage helps you and your oncology team select the most effective small cell lung cancer treatment approach and set realistic expectations for outcomes.

Limited Stage Small Cell Lung Cancer (LS-SCLC): When Cancer Remains Confined
Limited stage small cell lung cancer means the tumor remains confined to one hemithorax (one side of the chest), potentially including the ipsilateral hilar lymph nodes, mediastinal nodes, and supraclavicular nodes on the same side. Approximately one-third of patients present with limited disease at diagnosis, making them candidates for curative-intent treatment combining chemotherapy with concurrent radiation therapy. Patients maintaining optimal health during treatment using tools like our Calorie Deficit Calculator often tolerate aggressive chemoradiation protocols more effectively.
Survival outcomes for limited stage small cell lung cancer have improved dramatically:
| Limited Stage Category | 5-Year Survival Rate | Median Survival (2025) | Treatment Approach |
|---|---|---|---|
| Localized (confined to lung) | 30-34% | 55.9 months with durvalumab | Chemoradiation + immunotherapy consolidation |
| Regional (lymph node spread) | 18-20% | 24-36 months | Concurrent chemoradiation + PCI |
| 3-Year Survival (modern protocols) | 56.5% | — | Platinum-etoposide + durvalumab |
*Data sources: SEER Cancer Statistics, ADRIATIC trial results *
The ADRIATIC trial published in 2024 revolutionized limited stage treatment, demonstrating that durvalumab (Imfinzi) consolidation therapy after chemoradiation extended median overall survival to an unprecedented 55.9 months. This represents more than a four-year median survival—unthinkable just five years ago for any small cell lung cancer stage. According to data tracked by SEER training modules, historical two-year disease-free survival for limited stage SCLC ranged only 10-25% before modern immunotherapy integration.
Extensive Stage Small Cell Lung Cancer (ES-SCLC): When Cancer Has Spread
Extensive stage small cell lung cancer describes disease that has spread beyond one hemithorax, involving both lungs, distant lymph nodes, or metastatic sites such as the liver, bones, brain, or adrenal glands. Approximately two-thirds of small cell lung cancer patients present with extensive disease, as SCLC’s aggressive biology often causes widespread dissemination before symptoms emerge. The CDC’s lung cancer overview emphasizes that extensive stage small cell lung cancer requires systemic chemotherapy as the backbone of treatment rather than localized radiation.
Survival statistics for extensive stage small cell lung cancer by spread pattern:
| Extensive Stage Category | 5-Year Survival Rate | Median Survival (2025) | Key Challenge |
|---|---|---|---|
| Stage 4 small cell lung cancer (distant metastases) | 3-4% | 25.3 months with tarlatamab | Early treatment resistance |
| Overall extensive stage | 7-9% | 12-18 months (chemotherapy alone) | Rapid progression |
| 3-Year Survival (immunotherapy era) | 17.6% | 15.9 months with atezolizumab | Maintaining response |
| 2025 Breakthrough | TBD | 25.3 months with maintenance tarlatamab | Game-changing BiTE therapy |
*Data sources: American Cancer Society SEER data, DeLLphi-304 trial *
The November 2025 FDA approval of tarlatamab represents a paradigm shift for extensive stage small cell lung cancer life expectancy, with the DeLLphi-304 maintenance trial showing median overall survival exceeding 25 months—nearly doubling historical outcomes. Patients receiving first-line platinum-etoposide chemotherapy plus atezolizumab (Tecentriq) immunotherapy followed by tarlatamab maintenance achieved 82% one-year survival rates. Monitoring your overall health metrics using our Body Fat Calculator helps track nutritional status during intensive treatment protocols.
What These Numbers Really Mean For You: Translating Statistics to Hope
Survival statistics represent population averages—not individual destinies. Your personal small cell lung cancer prognosis depends on multiple factors beyond stage: age, performance status, smoking cessation, genetic tumor characteristics, treatment response, and access to cutting-edge therapies like immunotherapy small cell lung cancer protocols. A 58-year-old non-smoker with excellent cardiovascular fitness and extensive stage disease treated with modern immunotherapy combinations has fundamentally different odds than a 75-year-old with severe COPD receiving chemotherapy alone.
Key factors that improve your odds beyond stage:
- Early treatment initiation within 2-4 weeks of diagnosis
- Access to immunotherapy (durvalumab, atezolizumab, tarlatamab)
- Clinical trial participation for experimental combinations
- Smoking cessation immediately upon diagnosis
- Nutritional optimization maintaining BMI >18.5 throughout treatment
- Prophylactic cranial irradiation reducing brain metastasis risk by 50%
- Performance status (ECOG 0-1 vs. 2-4 dramatically affects eligibility)
The National Cancer Institute’s patient treatment guide emphasizes that small cell lung cancer recurrence remains common even after successful initial treatment, with more than 50% of patients experiencing disease return within two years. However, 2025’s treatment landscape offers sequential therapy options that were unavailable even 18 months ago, transforming SCLC from uniformly fatal to a chronic disease management paradigm for some patients.
Recognizing Small Cell Lung Cancer Symptoms & The Critical Importance of Early Detection
Why Small Cell Lung Cancer Symptoms Often Appear Too Late
Small cell lung cancer symptoms rarely manifest in early stages, with most patients remaining asymptomatic until the tumor grows large enough to obstruct airways or metastasizes to distant organs. This biological stealth explains why approximately two-thirds of patients present with extensive stage disease at diagnosis, when five-year survival drops below 10%. According to MedlinePlus medical guidelines, SCLC’s aggressive doubling time of 30-50 days means symptoms can rapidly escalate from subtle to severe within weeks.
The most common initial small cell lung cancer symptoms include persistent cough that worsens over time and progressive shortness of breath, but these warning signs often mimic chronic bronchitis or COPD in longtime smokers. This diagnostic ambiguity delays critical treatment initiation by an average of 8-12 weeks, during which micrometastases establish themselves in liver, bones, and brain tissue. Monitoring your cardiovascular fitness using our Heart Rate Zone Calculator can help distinguish between exercise-related breathlessness and pathological dyspnea requiring medical evaluation.
Early-Stage Warning Signs: Subtle Symptoms You Cannot Ignore
Respiratory symptoms dominate early small cell lung cancer presentations:
- Chronic cough that persists beyond 3-4 weeks or changes in character (dry to productive)
- Hemoptysis (coughing up blood or blood-streaked mucus) occurring in 25-30% of cases
- Shortness of breath (dyspnea) with previously tolerable activities like climbing stairs
- Chest pain or discomfort that may worsen with deep breathing or coughing
- Wheezing or stridor indicating airway obstruction
- Recurrent respiratory infections (bronchitis or pneumonia) in the same lung region
- Hoarseness or voice changes persisting more than two weeks
Systemic small cell lung cancer symptoms suggesting metastatic spread:
- Unexplained weight loss exceeding 10 pounds in 1-2 months without dietary changes
- Extreme fatigue disproportionate to activity level
- Loss of appetite (anorexia) with food aversion
- Persistent low-grade fever without infection source
The National Cancer Institute patient guide emphasizes that any combination of respiratory symptoms lasting beyond three weeks in current or former smokers warrants immediate chest imaging. Using our Symptom Checker can help document symptom patterns before your physician appointment, though it cannot substitute for professional medical evaluation.
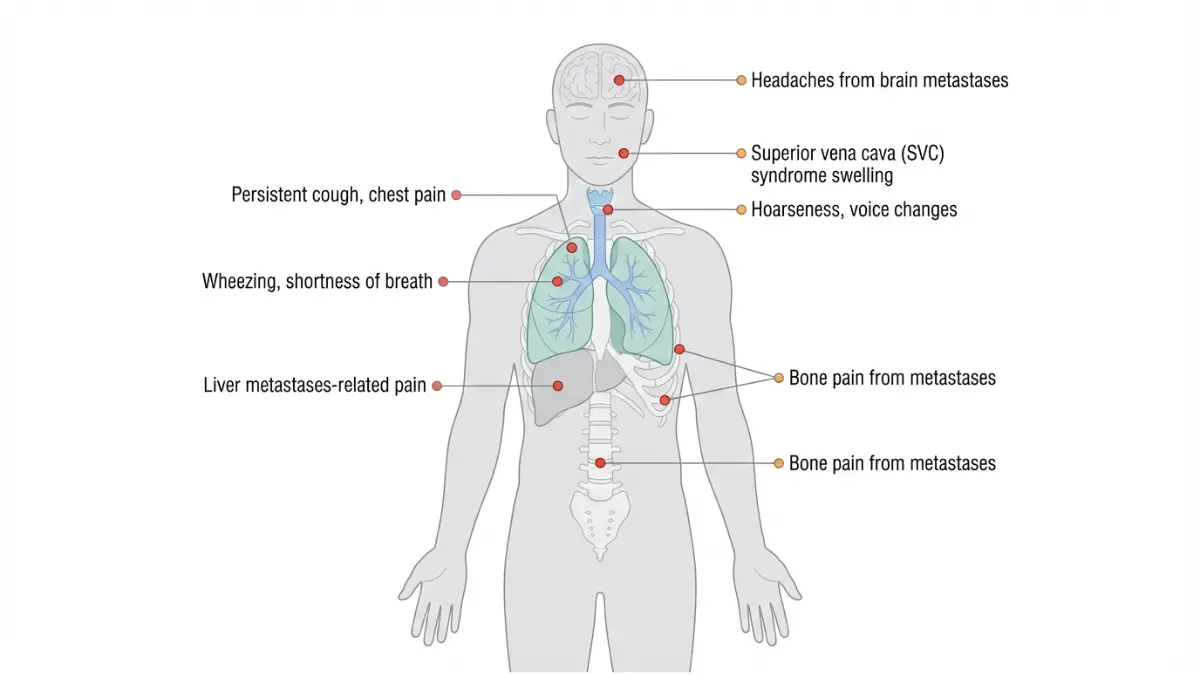
Advanced Small Cell Lung Cancer Symptoms: When Cancer Spreads
Superior vena cava syndrome represents one of the most dramatic small cell lung cancer symptoms, occurring in 10-15% of SCLC patients when mediastinal tumor growth compresses the major vein draining blood from the upper body. This oncologic emergency manifests as facial swelling, neck vein distension, upper chest visible venous collaterals, dyspnea, and orthopnea requiring urgent intervention. According to PMC case studies, recognition of these clinical signs must prompt immediate contrast-enhanced CT imaging and radiation therapy to decompress the SVC.
| Metastatic Site | Small Cell Lung Cancer Symptoms | Frequency | Diagnostic Test |
|---|---|---|---|
| Brain | Headaches, seizures, confusion, weakness, vision changes, balance problems | 15-20% at diagnosis 60% eventually | Brain MRI with contrast |
| Bone | Localized bone pain, pathologic fractures, hypercalcemia, spinal cord compression | 30-40% | Bone scan or PET-CT |
| Liver | Right upper quadrant pain, jaundice, ascites, elevated liver enzymes | 20-30% | Abdominal CT or MRI |
| Adrenal glands | Often asymptomatic, adrenal insufficiency (rare), abdominal pain | 25-35% | Abdominal CT |
*Data compiled from SCLC metastatic patterns *
Paraneoplastic syndromes affect 10-20% of small cell carcinoma patients, producing small cell lung cancer symptoms unrelated to tumor location through hormone secretion or autoimmune responses. Syndrome of inappropriate antidiuretic hormone (SIADH) causes hyponatremia with confusion, nausea, and seizures, while Lambert-Eaton myasthenic syndrome produces proximal muscle weakness and autonomic dysfunction. These rare presentations sometimes precede radiographic tumor detection by months, making them crucial diagnostic clues.
Who Should Screen for Small Cell Lung Cancer: Updated 2025 Guidelines
The U.S. Preventive Services Task Force (USPSTF) recommends annual low-dose CT (LDCT) lung cancer screening for adults meeting all three criteria:
- Age 50-80 years (expanded from previous 55-80 guidelines)
- 20 pack-year smoking history or greater (one pack daily for 20 years, or two packs daily for 10 years)
- Current smoker or quit within past 15 years
According to the CDC’s lung cancer screening program, these updated 2021 guidelines aim to detect small cell lung cancer symptoms before they manifest, catching tumors at localized stages where 30% five-year survival becomes achievable. The National Cancer Institute screening data shows LDCT reduces lung cancer mortality by 20% compared to chest X-ray screening, though only 5-10% of eligible Americans currently undergo recommended screening.
Pack-year calculation formula: (Cigarettes per day ÷ 20) × Years smoked = Pack-years
For example: Smoking 1.5 packs daily for 15 years = (1.5 × 15) = 22.5 pack-years, qualifying for screening. Individuals should discuss screening benefits and risks with primary care providers, as screening also detects non-small cell lung cancer, which comprises 85% of lung malignancies. Assessing your family cancer risk using our Genetic Risk Assessment Tool may identify additional factors warranting earlier or more frequent screening.
When to Seek Immediate Medical Evaluation
Seek urgent evaluation within 24-48 hours if experiencing:
- Coughing up more than teaspoon-sized blood
- Sudden severe shortness of breath at rest
- Facial or neck swelling with prominent veins (SVC syndrome)
- New neurological symptoms (severe headache, seizure, confusion)
- Acute bone pain with inability to bear weight
Schedule appointment within one week for:
- Persistent cough lasting 3+ weeks
- Any hemoptysis (blood in sputum), even trace amounts
- Unexplained 10-pound weight loss
- New or worsening chest pain
- Hoarseness lasting 2+ weeks
Early detection of small cell lung cancer symptoms through screening and prompt evaluation of warning signs represents the most powerful survival predictor within your control, potentially shifting diagnosis from extensive stage (3% five-year survival) to limited stage (27-30% five-year survival).
2025 Breakthrough Treatments Transforming Small Cell Lung Cancer Survival
How New Small Cell Lung Cancer Treatments Are Rewriting the Survival Playbook
Small cell lung cancer treatment has undergone a revolutionary transformation in 2025, with the FDA’s traditional approval of tarlatamab small cell lung cancer therapy representing the first major survival breakthrough in over three decades. According to the FDA’s November 2025 approval announcement, this bispecific T-cell engager doubles median survival when used as maintenance therapy after first-line chemotherapy small cell lung cancer protocols. The treatment landscape now offers sequential therapy options—platinum-based chemotherapy, immunotherapy consolidation, targeted maintenance, and prophylactic cranial irradiation—that collectively extend life expectancy by years rather than months.
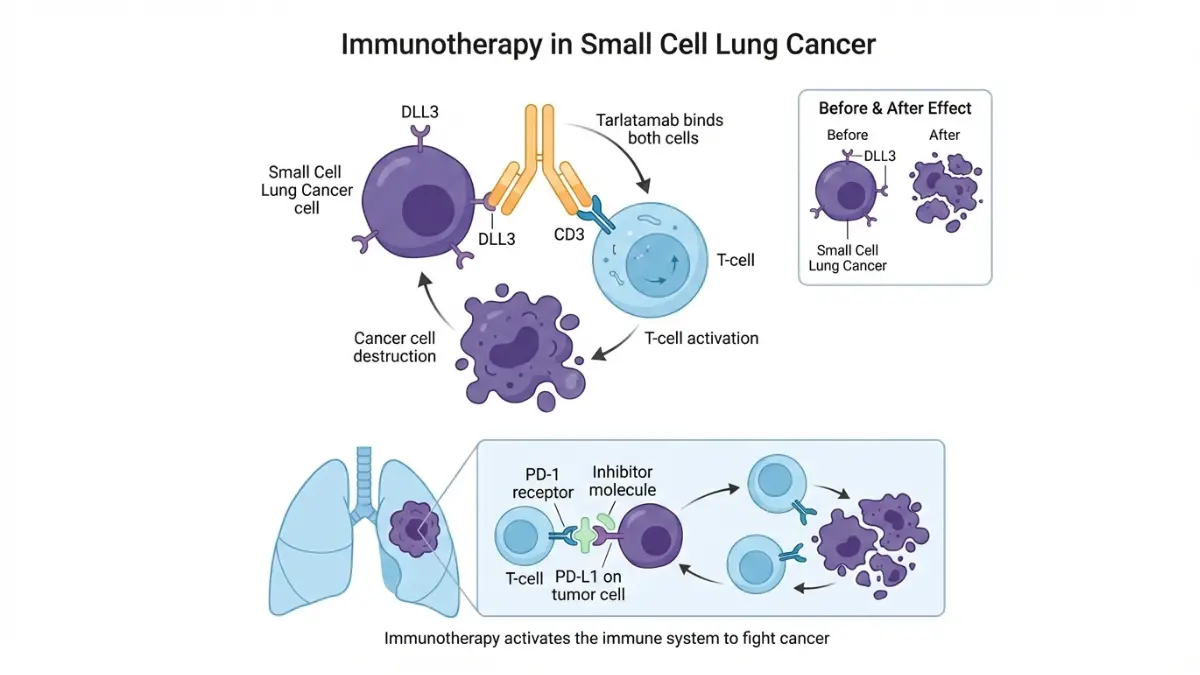
Tarlatamab (Imdelltra): The 2025 FDA-Approved Game-Changer
Tarlatamab represents the first bispecific T-cell engager (BiTE) approved for any solid tumor, engineered to simultaneously bind DLL3-expressing cancer cells and CD3-expressing T-cells, redirecting the immune system to destroy small cell carcinoma. On November 19, 2025, the FDA granted full traditional approval following the landmark DeLLphi-304 phase III trial, which demonstrated median overall survival of 25.3 months in extensive stage small cell lung cancer patients receiving tarlatamab maintenance after chemotherapy—compared to 13.3 months with chemotherapy alone.
Tarlatamab small cell lung cancer clinical trial results:
- 82% one-year survival rate (vs. 63% with chemotherapy alone)
- 40.4% objective response rate in second-line treatment
- Median progression-free survival: 4.9 months in heavily pretreated patients
- DLL3 expression detected in 85% of SCLC tumors, making most patients eligible
- Intravenous administration every two weeks following step-up dosing
Who qualifies for tarlatamab small cell lung cancer therapy? Adults with extensive stage small cell lung cancer whose disease progressed during or after platinum-based chemotherapy are eligible regardless of biomarker status. The treatment requires hospitalization for the first three infusions due to cytokine release syndrome risk, but subsequent doses can be administered outpatient. Patients maintaining strength during treatment using our Protein Intake Calculator to optimize muscle preservation often tolerate therapy with fewer dose reductions.
Immunotherapy for Small Cell Lung Cancer: Durvalumab & Atezolizumab
Immunotherapy small cell lung cancer protocols have become standard first-line treatment, with two FDA-approved checkpoint inhibitors demonstrating survival benefits when combined with platinum-etoposide chemotherapy. According to the NIH’s immunotherapy approval summary, these agents represent “the first novel treatments to demonstrate an improvement in overall survival in the front-line treatment of advanced SCLC in over 3 decades”.
| Drug Name | Mechanism | Indication | Survival Benefit | Key Side Effects |
|---|---|---|---|---|
| Durvalumab (Imfinzi) | PD-L1 inhibitor | Limited stage SCLC post-chemoradiation | Median OS: 55.9 months (consolidation) | Pneumonitis, thyroid dysfunction, diarrhea |
| Atezolizumab (Tecentriq) | PD-L1 inhibitor | First-line extensive stage SCLC | Median OS: 12.3 vs. 10.3 months | Immune-mediated hepatitis, fatigue, nausea |
| Tarlatamab (Imdelltra) | BiTE (DLL3 x CD3) | Second-line+ extensive stage SCLC | Median OS: 25.3 months (maintenance) | Cytokine release syndrome, pyrexia, dysgeusia |
*Data compiled from FDA approval documents and clinical trials *
Durvalumab consolidation therapy has become standard for limited stage small cell lung cancer patients who complete concurrent chemoradiation without progression. The ADRIATIC trial demonstrated that durvalumab extended median overall survival to 55.9 months—nearly five years—transforming limited stage disease from rapidly fatal to potentially curable. Atezolizumab plus carboplatin-etoposide received FDA approval in March 2019 for first-line extensive stage small cell lung cancer treatment, providing a modest but meaningful survival extension of approximately two months.
Chemotherapy for Small Cell Lung Cancer: The Platinum-Etoposide Backbone
Platinum-based chemotherapy small cell lung cancer protocols remain the foundation of both limited and extensive stage treatment, with the combination of cisplatin or carboplatin plus etoposide serving as standard since the 1980s. The National Cancer Institute treatment guidelines state that “the combination of platinum and etoposide is the most widely used standard chemotherapeutic regimen” based on level A1 evidence.
Standard chemotherapy small cell lung cancer protocols:
- Cisplatin 75-80 mg/m² IV day 1 + Etoposide 100-120 mg/m² IV days 1-3
- Carboplatin AUC 5-6 IV day 1 + Etoposide 100-120 mg/m² IV days 1-3
- Treatment cycles: Every 21 days for 4-6 cycles
- Response rate: 60-80% in chemotherapy-naïve patients
- Median duration of response: 3-4 months without maintenance therapy
No survival advantage has been consistently demonstrated with increased dose intensity, alternating regimens, or maintenance chemotherapy beyond 4-6 cycles when used without immunotherapy. However, chemotherapy serves as the essential backbone enabling immunotherapy small cell lung cancer combinations that extend survival. Staying properly hydrated during intensive chemotherapy using our Water Intake Calculator helps minimize nephrotoxicity from platinum agents and supports optimal treatment delivery.
Radiation Therapy & Prophylactic Cranial Irradiation (PCI)
Concurrent chemoradiation represents the gold standard for limited stage small cell lung cancer treatment, with ClinicalTrials.gov studies demonstrating superior survival compared to sequential approaches. Radiation therapy typically delivers 45 Gy in 30 twice-daily fractions or 60-70 Gy in once-daily fractions during cycles 2-3 of chemotherapy. Thoracic radiation targets the primary tumor and involved mediastinal lymph nodes, achieving local control rates exceeding 80% when combined with platinum-etoposide.
Prophylactic cranial irradiation (PCI) reduces brain metastasis risk by approximately 50% in patients achieving complete or partial response to initial therapy. According to NIH meta-analyses, PCI “improves survival to a significant degree in small-cell lung cancer patients” beyond its established role preventing brain metastases. Research published in PMC journals demonstrates that PCI reduces brain metastases rates from approximately 60% to 30% and increases three-year overall survival by approximately 5%.
PCI administration details:
- Timing: 4-6 weeks after completing chemotherapy in responding patients
- Dose: 25 Gy in 10 fractions (most common) or 30 Gy in 15 fractions
- Target: Whole brain irradiation
- Candidates: Limited stage patients with complete/partial response; selected extensive stage patients
- Side effects: Fatigue, hair loss, memory changes, cognitive decline (10-20% long-term)
The role of PCI in extensive stage small cell lung cancer remains controversial, with ongoing ClinicalTrials.gov studies evaluating its benefit in the immunotherapy era. Some oncologists now recommend brain MRI surveillance rather than routine PCI for extensive stage disease, particularly in older adults at higher neurotoxicity risk.
When Surgery Is an Option for Small Cell Lung Cancer
Surgical resection plays an extremely limited role in small cell lung cancer treatment, reserved for the rare patient (less than 5%) presenting with stage I disease (T1-2N0M0) discovered incidentally. Even in highly selected surgical candidates, post-operative adjuvant chemotherapy remains mandatory due to SCLC’s propensity for micrometastatic spread. Most patients undergo biopsy procedures for diagnosis rather than therapeutic surgery, as small cell lung cancer stages at presentation typically involve extensive local or distant spread precluding resection.
What This Means For You: Your Treatment Decision Roadmap
Navigating small cell lung cancer treatment requires partnering with thoracic oncologists experienced in the latest protocols. Your treatment plan depends on stage, performance status, organ function, and access to immunotherapy and clinical trials. Adequate rest during treatment cycles using our Sleep Calculator supports immune function and treatment tolerance.
Essential questions to ask your oncology team:
- What is my exact stage, and am I limited or extensive stage?
- Should I receive immunotherapy (durvalumab or atezolizumab) with first-line chemotherapy?
- Am I a candidate for tarlatamab maintenance therapy after chemotherapy?
- Are there clinical trials testing new small cell lung cancer treatments I should consider?
- Should I receive prophylactic cranial irradiation, and when?
- What is my expected timeline: chemotherapy duration, radiation schedule, maintenance therapy?
- How do we monitor for small cell lung cancer recurrence after treatment?
- What support services (nutrition, social work, palliative care) are available?
The 2025 treatment paradigm now offers sequential therapies that can extend survival from months to years, transforming patient conversations from “how long do I have?” to “how do we maximize quality and quantity of life?”.
Understanding Small Cell Lung Cancer Causes, Risk Factors & Prevention Strategies
The Primary Culprit: Tobacco Smoking and Small Cell Lung Cancer
Smoking tobacco represents the overwhelming cause of small cell lung cancer, responsible for approximately 95-98% of all SCLC cases according to NIH epidemiological data. Small cell lung cancer causes are dominated by tobacco carcinogens, with the strongest association among all lung cancer subtypes—even stronger than squamous cell carcinoma. The CDC’s lung cancer risk factor analysis emphasizes that “tobacco smoke, radon, and other things can increase your risk,” but tobacco dwarfs all other small cell lung cancer causes combined.
Pack-year smoking history directly correlates with small cell carcinoma risk:
- Less than 10 pack-years: Minimal SCLC risk (similar to never-smokers)
- 20-30 pack-years: Moderate risk, screening recommended starting age 50
- 30-50 pack-years: High risk, representing typical SCLC patient profile
- 50+ pack-years: Very high risk, with 15-20x elevated incidence compared to never-smokers

Menthol cigarettes carry equivalent or greater risk compared to non-menthol varieties, as the cooling sensation enables deeper inhalation and longer breath-holding, increasing carcinogen exposure to small airways where SCLC originates. The earlier you began smoking—particularly before age 15—the higher your lifetime small cell lung cancer risk due to prolonged exposure during critical lung development periods. Evaluating your baseline metabolic health using our BMR Calculator helps establish personalized wellness goals when beginning smoking cessation.
Secondhand smoke exposure increases small cell lung cancer causes by approximately 20-30% in never-smokers who live with active smokers for decades. Children exposed to household tobacco smoke face elevated risks extending into adulthood, even if they never personally smoke. According to research published in PMC journals on smoking cessation, “people who continue to smoke after a diagnosis of early-stage lung cancer almost double their risk of dying” compared to those who quit immediately.
Environmental & Occupational Small Cell Lung Cancer Causes
Radon gas represents the second-leading cause of lung cancer in the United States after tobacco, accounting for approximately 21,000 annual lung cancer deaths. A CDC epidemiological study in New Jersey found “the trend for increasing risk for lung cancer with increasing radon exposure was statistically significant,” with the relative risk coefficient ranging 0-8.0% per working level month. Radon, a colorless and odorless radioactive gas produced by uranium decay, accumulates in basements and poorly ventilated lower levels of homes.
Known environmental and occupational small cell lung cancer causes:
- Radon gas – Second-leading cause; testing recommended for all homes, especially basements
- Asbestos exposure – The EPA’s carcinogenicity assessment identifies asbestos as causing both lung cancer and mesothelioma from inhalation
- Arsenic contamination – Drinking water and occupational exposure in smelting industries
- Diesel exhaust – Long-term exposure in transportation and mining occupations
- Uranium and radioactive ores – Mining occupations with elevated lung cancer rates
- Silica dust and coal dust – Industrial occupations causing lung inflammation and carcinogenesis
- Chromium and nickel compounds – Metal working and electroplating industries
Synergistic effects amplify risk when multiple exposures combine, particularly smoking plus radon or asbestos. Smokers exposed to asbestos have “a greater than additive increased” lung cancer risk compared to either exposure alone. General health monitoring using our Ideal Weight Calculator helps track overall wellness during occupational exposure or remediation efforts.
Small Cell vs Non-Small Cell Lung Cancer: Critical Differences
Understanding small cell vs non small cell lung cancer distinctions helps patients comprehend why treatment approaches differ dramatically between the two types.
| Characteristic | Small Cell Lung Cancer (SCLC) | Non-Small Cell Lung Cancer (NSCLC) |
|---|---|---|
| Prevalence | 10-15% of lung cancers | 85-90% of lung cancers |
| Cell appearance | Small cells with scant cytoplasm under microscopy | Larger cells with more cytoplasm |
| Growth rate | Extremely aggressive; doubling time 30-50 days | Slower growth; doubling time 100-400 days |
| Metastatic spread | Early widespread dissemination (66% extensive at diagnosis) | More localized initially (60% candidates for surgery) |
| Smoking association | 95-98% caused by smoking (strongest link) | 85% caused by smoking |
| Staging system | Limited vs. extensive (2 categories) | TNM staging (I-IV with subcategories) |
| Primary treatment | Chemotherapy + radiation + immunotherapy | Surgery + chemotherapy + targeted therapy |
| 5-year survival | 7% overall (27% localized, 3% distant) | 28% overall (64% localized, 9% distant) |
*Comparison data compiled from clinical guidelines *
Small cell vs non small cell lung cancer treatment paradigms differ fundamentally because SCLC is considered a systemic disease at diagnosis requiring chemotherapy, while early-stage NSCLC is primarily a localized disease amenable to surgical resection. The small cell carcinoma subtype’s neuroendocrine features make it initially more chemotherapy-sensitive than NSCLC, but resistance develops rapidly. Exploring comprehensive health resources in our Health Tips section provides additional cancer prevention strategies beyond lung-specific recommendations.
Prevention Strategies That Reduce Small Cell Lung Cancer Risk
Smoking cessation remains the single most powerful prevention strategy, with lung cancer risk declining progressively after quitting. According to Smokefree.gov’s health benefits data, “quitting smoking will prevent new DNA damage from happening and can even help repair the damage that has already been done”. The Smokefree.gov program offers free personalized quit plans, text message support, and live coaching to help smokers overcome tobacco dependence.
Lung healing timeline after smoking cessation:
- 20 minutes: Heart rate and blood pressure drop to normal levels
- 12 hours: Carbon monoxide levels in blood return to normal
- 2-3 months: Circulation improves and lung function increases
- 1-9 months: Coughing and shortness of breath decrease
- 1 year: Coronary heart disease risk reduced by 50%
- 5 years: Stroke risk reduced to that of non-smokers
- 10 years: Lung cancer death rate drops to about half that of continuing smokers
- 15 years: Coronary heart disease risk equivalent to never-smokers
Additional small cell lung cancer prevention strategies:
- Avoid secondhand smoke – Request smoke-free environments at work and home
- Test for radon – All homes should undergo radon testing; remediate if levels exceed 4 pCi/L
- Use occupational protective equipment – Respirators and ventilation in high-risk workplaces
- Reduce asbestos exposure – Professional abatement for older homes with asbestos-containing materials
- Filter air quality – HEPA filtration systems reduce indoor particulate exposure
- Annual LDCT screening – High-risk individuals (50-80 years, 20+ pack-years) should undergo low-dose CT screening
Even after small cell lung cancer diagnosis, immediate smoking cessation improves outcomes significantly. Research demonstrates that quitting smoking after diagnosis increases survival time, reduces treatment complications, improves chemotherapy efficacy, and enhances quality of life. Visiting MyMedicineAdvisor regularly provides ongoing support with evidence-based health tools and cancer prevention resources.
Living With Small Cell Lung Cancer – Navigating Recurrence, Follow-Up Care & Long-Term Support
Understanding Small Cell Lung Cancer Recurrence: Why It Happens and What to Expect
Small cell lung cancer recurrence affects more than 50% of patients, with most relapses occurring within the first two years after completing initial treatment. According to NIH research on SCLC relapse patterns, “22% of patients experienced CNS [central nervous system] recurrence, with a similar incidence in both LS and ES SCLC (19% vs. 23%)”. This high small cell lung cancer recurrence rate reflects the tumor’s aggressive biology and propensity for micrometastatic spread that exists before diagnosis despite appearing localized on imaging.
Small cell lung cancer recurrence patterns typically manifest as distant metastases rather than local regrowth, most commonly involving the brain, liver, bones, and opposite lung. Brain metastases represent the most concerning recurrence site, occurring in 60-80% of patients who do not receive prophylactic cranial irradiation. The National Cancer Institute’s treatment guidelines emphasize that “some tests will continue to be done from time to time after treatment has ended” to detect small cell lung cancer recurrence early when intervention options remain available.
Standard surveillance schedule for detecting small cell lung cancer recurrence:
- Months 0-12: Chest CT with contrast every 3 months; brain MRI every 3-6 months
- Months 13-24: Chest CT every 3-4 months; brain MRI every 6 months
- Years 3-5: Chest CT every 6 months; brain MRI annually
- Beyond 5 years: Individualized based on risk factors and symptoms
Symptoms suggesting possible small cell lung cancer recurrence include new or worsening cough, hemoptysis, chest pain, unexplained weight loss, bone pain, neurological changes, or persistent fatigue. The National Cancer Institute’s survivorship resources recommend all cancer survivors have follow-up care that includes “regular medical check-ups” to monitor for late effects and recurrence.
Palliative Care & Quality of Life: Essential Support Throughout Your Journey
Palliative care significantly improves small cell lung cancer life expectancy and quality of life when integrated early in the disease course, contrary to misconceptions that palliative care equals “giving up”. Research published in PMC journals on palliative care effectiveness demonstrates that “treatment of patients with lung cancer in the Department of palliative care leads to a significant improvement in overall quality of life,” with measurable improvements in physical function, emotional health, and even pulmonary function after just two weeks.
Palliative care benefits for SCLC patients include:
- Symptom management – Pain control, dyspnea relief, nausea reduction, fatigue management
- Emotional support – Depression and anxiety treatment, existential distress counseling
- Care coordination – Integration between oncology, primary care, and specialty services
- Family support – Caregiver education, anticipatory guidance, bereavement services
- Treatment decision-making – Values clarification, goals of care discussions, advance directives
According to NIH palliative care studies, “early palliative care improves life quality, mood, and pulmonary function” in lung cancer patients, with statistically significant benefits across physical, emotional, and functional domains. Palliative care complements cancer treatment rather than replacing it, addressing the whole person beyond tumor control.
Nutrition & Lifestyle Strategies During Small Cell Lung Cancer Treatment
Optimal nutrition becomes critically important during SCLC treatment, as chemotherapy and radiation frequently cause appetite loss, taste changes, nausea, and unintentional weight loss. The National Cancer Institute’s nutrition guidance for cancer patients recommends “lots of whole grains, fruits and vegetables, modest amounts of protein, and small amounts of sugar, alcohol, salt, and unhealthy fats” for general health, but treatment-related needs may differ.
Evidence-based nutrition strategies for SCLC patients:
- Protein requirements: 1.0-1.5 grams per kilogram body weight daily to preserve muscle mass during treatment
- Caloric needs: 25-30 calories per kilogram body weight to prevent malnutrition
- Frequent small meals: 6-8 small meals/snacks rather than 3 large meals when appetite is poor
- High-protein foods first: Eat beans, chicken, fish, meat, yogurt, and eggs when appetite is strongest
- Anti-inflammatory foods: Omega-3 fatty acids from fish, flaxseed, walnuts may reduce inflammation
- Hydration: 8-12 cups of fluid daily, more during chemotherapy to prevent kidney damage
The NCI’s comprehensive nutrition guide titled “Eating Hints: Before, During and After Cancer Treatment” provides practical meal planning strategies tailored to treatment side effects. Using our Macro Calculator helps determine personalized protein, carbohydrate, and fat targets based on your current weight and treatment phase, ensuring adequate nutrition without overwhelming restricted appetites.
Lifestyle modifications that support treatment tolerance:
- Gentle exercise – Walking 10-20 minutes daily maintains cardiovascular fitness and reduces fatigue
- Sleep hygiene – 7-9 hours nightly supports immune function; use our Sleep Calculator to optimize timing
- Stress reduction – Meditation, yoga, support groups decrease cortisol and improve outcomes
- Smoking cessation – Immediate and sustained benefits even after diagnosis
Maintaining your ideal body weight using our Ideal Weight Calculator provides a benchmark for nutritional adequacy, as weight loss exceeding 10% during treatment correlates with worse small cell lung cancer prognosis and reduced treatment tolerance.
Financial & Insurance Navigation: Understanding Small Cell Lung Cancer Treatment Costs
Small cell lung cancer treatment costs range from $10,000 to $200,000+ depending on stage, treatment duration, and complications, with chemotherapy costing $1,000-$12,000 per monthly cycle and immunotherapy significantly higher. Medicare Part B typically covers 80% of outpatient cancer services including chemotherapy and radiation after a $257 deductible, leaving patients responsible for 20% coinsurance. Medicare Part D covers oral chemotherapy medications, while Medicare Part A covers inpatient hospitalization costs.
Financial resources and assistance programs:
- Patient assistance programs – Pharmaceutical manufacturers offer free/reduced-cost medications for qualifying patients
- CancerCare Co-Payment Assistance – Helps with insurance premiums, copays, and related costs
- NCI Clinical Trials – Experimental treatments provided at no cost, often with travel support
- Social Security Disability – Expedited approval for metastatic cancer diagnoses
- Hospital financial counselors – Negotiate payment plans and identify charity care eligibility
Insurance coverage strategy: Review your policy’s out-of-pocket maximum early in treatment, as most SCLC patients exceed this threshold within the first few months, after which all covered services become free for the remainder of the plan year.
Essential Questions to Ask Your Oncology Team
Advocating for yourself requires asking detailed questions about your specific small cell lung cancer prognosis, treatment options, and follow-up plan:
- What is my exact stage (limited vs. extensive) and what does that mean for my prognosis?
- Am I a candidate for immunotherapy (durvalumab, atezolizumab, tarlatamab) and clinical trials?
- What is my expected treatment timeline: how many chemotherapy cycles, radiation duration, maintenance therapy?
- Should I receive prophylactic cranial irradiation, and what are the cognitive risks?
- How will we monitor for small cell lung cancer recurrence after treatment ends?
- What symptoms require urgent evaluation versus routine follow-up?
- What survivorship resources are available: nutrition counseling, support groups, palliative care?
- When should my family consider hospice evaluation if treatment stops working?
Mark’s Story: Living With Hope in 2025
Mark (name changed), a 62-year-old retired teacher diagnosed with extensive stage small cell lung cancer in January 2024, initially received a median survival estimate of 10-12 months with standard chemotherapy. Twenty months later, Mark remains cancer-free after completing platinum-etoposide chemotherapy, atezolizumab immunotherapy, and transitioning to tarlatamab maintenance therapy. “The diagnosis felt like a death sentence,” Mark reflects, “but 2025’s treatment options gave me time to see my daughter’s wedding and welcome my first grandchild.”
Mark’s quality of life remains excellent—he walks three miles daily, volunteers at his local library, and maintains his weight within normal range using dietary planning from our Macro Calculator. His oncologist monitors for small cell lung cancer recurrence with quarterly CT scans and semiannual brain MRIs, but Mark focuses on living fully rather than waiting for relapse. “Cancer changed my priorities,” he says, “but the new treatments gave me a future I never expected to have.”
Stories like Mark’s represent the transforming reality of small cell lung cancer life expectancy in 2025, where sequential therapy options extend survival from months to years for carefully selected patients. While small cell lung cancer remains an aggressive malignancy with high recurrence rates, advances in immunotherapy small cell lung cancer protocols and targeted maintenance treatments offer genuine hope. Visit MyMedicineAdvisor regularly for updated health resources, evidence-based tools, and comprehensive cancer care information to support your journey.
Frequently Asked Questions About Small Cell Lung Cancer
1. What is the survival rate for small cell lung cancer?
Small cell lung cancer survival rates range from 3% to 30% at five years depending on stage at diagnosis. Localized limited stage disease offers 27-30% five-year survival, regional spread drops to 18%, and distant metastatic extensive stage disease has only 3-4% five-year survival. With 2025’s new treatments including tarlatamab and durvalumab immunotherapy, median survival has extended to 25-55 months in selected patients compared to historical 10-13 months.
2. What are the early warning signs of small cell lung cancer?
Early small cell lung cancer symptoms include persistent cough lasting 3+ weeks, coughing up blood (hemoptysis), progressive shortness of breath, chest pain worsening with deep breathing, unexplained weight loss exceeding 10 pounds, extreme fatigue, hoarseness persisting beyond two weeks, and recurrent respiratory infections. Unfortunately, SCLC rarely causes symptoms in early stages, which explains why two-thirds of patients present with extensive stage disease at diagnosis.
3. How is small cell lung cancer treated in 2025?
Small cell lung cancer treatment in 2025 combines platinum-etoposide chemotherapy with immunotherapy (durvalumab or atezolizumab), followed by maintenance therapy with tarlatamab for extensive stage disease or radiation consolidation for limited stage disease. Tarlatamab, FDA-approved November 2025, represents the first bispecific T-cell engager for solid tumors and doubles median survival to 25.3 months. Prophylactic cranial irradiation reduces brain metastasis risk by 50%.
4. What causes small cell lung cancer?
Smoking tobacco causes 95-98% of small cell lung cancer cases, with the strongest association among all lung cancer types. Other causes include radon gas exposure (second-leading cause), asbestos exposure, arsenic contamination, diesel exhaust, uranium mining, silica dust, and chromium compounds. Secondhand smoke increases risk by 20-30% in never-smokers living with active smokers for decades.
5. What is the difference between limited and extensive stage small cell lung cancer?
Limited stage small cell lung cancer means the tumor remains confined to one side of the chest within a single radiation field, offering 27-30% five-year survival with combined chemoradiation and immunotherapy consolidation. Extensive stage small cell lung cancer indicates spread beyond one hemithorax to both lungs, distant lymph nodes, or metastatic sites (liver, bones, brain), with only 3-7% five-year survival despite aggressive systemic chemotherapy and immunotherapy.
6. How long can you live with extensive stage small cell lung cancer?
Extensive stage small cell lung cancer life expectancy has improved dramatically in 2025, with median survival reaching 25.3 months for patients receiving tarlatamab maintenance therapy after first-line chemotherapy plus immunotherapy—nearly double historical outcomes. Without modern treatments, median survival remains 10-13 months. Three-year survival has increased to 17.6% with immunotherapy protocols, and 82% of patients receiving tarlatamab reach the one-year milestone.
7. What is tarlatamab and how does it help small cell lung cancer?
Tarlatamab (Imdelltra) is the first FDA-approved bispecific T-cell engager for extensive stage small cell lung cancer, receiving traditional approval November 19, 2025. It simultaneously binds DLL3-expressing cancer cells and CD3-expressing T-cells, redirecting your immune system to destroy tumors. Clinical trials show 25.3 months median overall survival when used as maintenance therapy after chemotherapy, with 82% one-year survival and 40.4% objective response rates in second-line treatment.
8. What is the difference between small cell and non-small cell lung cancer?
Small cell lung cancer grows extremely aggressively with 30-50 day doubling time versus 100-400 days for non-small cell lung cancer. SCLC represents 10-15% of lung cancers with 95-98% caused by smoking, while NSCLC comprises 85-90% with 85% smoking-related. SCLC uses limited/extensive staging and requires chemotherapy-first treatment, while NSCLC uses TNM staging (I-IV) and prioritizes surgical resection for early stages. Five-year survival is 7% for SCLC versus 28% for NSCLC overall.
9. Does small cell lung cancer always come back?
Small cell lung cancer recurrence affects more than 50% of patients, typically within the first two years after completing treatment. Brain metastases represent the most common recurrence site (60-80% without prophylactic cranial irradiation), followed by liver, bones, and opposite lung. However, 2025’s sequential therapy options—chemotherapy, immunotherapy consolidation, and targeted maintenance with tarlatamab—are improving recurrence-free survival rates beyond historical data, with some patients remaining disease-free for 3-5+ years.
10. Can you prevent small cell lung cancer?
Smoking cessation remains the most powerful prevention strategy, reducing lung cancer risk progressively after quitting, with 50% reduction at 10 years and near-baseline risk at 15 years. Additional prevention includes avoiding secondhand smoke, testing homes for radon gas (second-leading cause), using occupational respiratory protection against asbestos and diesel exhaust, and annual low-dose CT screening for high-risk individuals aged 50-80 with 20+ pack-year smoking history. Even after diagnosis, immediate smoking cessation improves survival and treatment outcomes.
11. What factors improve small cell lung cancer prognosis beyond stage?
Small cell lung cancer prognosis improves with early treatment initiation within 2-4 weeks of diagnosis, access to immunotherapy and clinical trials, immediate smoking cessation, excellent performance status (ECOG 0-1), maintaining BMI above 18.5 throughout treatment, receiving prophylactic cranial irradiation, younger age (under 65), female gender, and absence of significant comorbidities like COPD or heart disease. Sequential modern therapies—platinum-etoposide, checkpoint inhibitors, and tarlatamab maintenance—can extend survival from months to years in carefully selected patients.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











