
On This Page – Quick Medical Summary
Endometrial Cancer Bleeding: 9 Signs After Menopause You Should Never Ignore
Endometrial cancer bleeding after menopause is abnormal vaginal bleeding that occurs when cancer develops in the uterine lining, most commonly presenting as spotting, light bleeding, or heavier flow in women who have stopped menstruating. Any postmenopausal bleeding requires immediate medical evaluation, as 90% of women diagnosed with endometrial cancer experienced this warning sign before their diagnosis.
Margaret, a 63-year-old retired teacher, noticed light pink spotting on her underwear one morning—something she hadn’t experienced in over a decade since menopause. Initially dismissing it as perhaps a minor irritation, the spotting returned twice more over three weeks. Her decision to call her gynecologist likely saved her life. After a simple endometrial biopsy, Margaret was diagnosed with Stage I endometrial cancer. Because she sought care immediately when she recognized postmenopausal bleeding as a potential cancer warning sign, her treatment was successful, and she remains cancer-free two years later.
Margaret’s story illustrates a critical truth that every woman past menopause should know: bleeding after menopause is never normal. While the majority of postmenopausal bleeding cases stem from benign conditions like uterine polyps or vaginal atrophy, approximately 9% of women who experience this symptom receive an endometrial cancer diagnosis. This cancer of the uterine lining is the most common gynecologic malignancy in the United States, yet it remains one of the most treatable when caught early.
The challenge lies in recognizing the subtle signs. Unlike other cancers that may develop silently for years, endometrial cancer after menopause typically announces itself through abnormal bleeding—a biological alarm system that demands attention. Understanding what these warning signs look like, when they require urgent evaluation, and which risk factors increase your vulnerability can make the difference between early detection with a 95% five-year survival rate and late-stage diagnosis with significantly reduced outcomes.
This comprehensive guide examines the nine critical warning signs of endometrial cancer that appear after menopause, explains why each symptom occurs, and provides evidence-based guidance on when to seek medical care. Whether you’re experiencing symptoms yourself, using our Symptom Checker to assess concerning changes, or simply want to understand your risk factors through tools like our BMI Calculator, knowledge empowers you to take control of your gynecologic health. Remember: early recognition of uterine cancer symptoms can be lifesaving, and no symptom is too minor to discuss with your healthcare provider.
9 Warning Signs of Endometrial Cancer After Menopause
Recognizing the early signs of endometrial cancer can dramatically improve treatment outcomes and survival rates. These nine warning signs represent the most common presentations of uterine cancer after menopause, each requiring careful attention and prompt medical evaluation.
1. Vaginal Bleeding or Spotting (Most Common Sign)
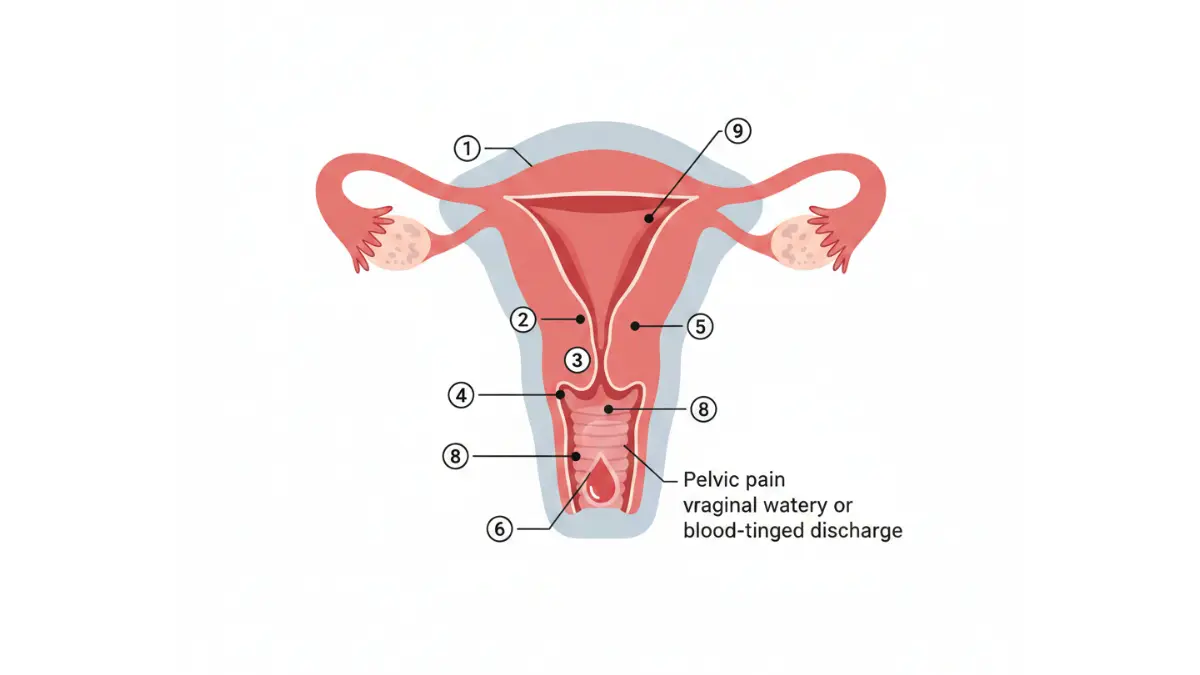
Postmenopausal bleeding endometrial cancer manifests as the primary symptom in approximately 90% of diagnosed cases, making it the single most important warning sign to recognize. This bleeding can appear in multiple forms: light pink spotting on underwear or toilet paper, watery blood-streaked discharge, intermittent brown spotting, or heavier flow resembling a period. The critical distinction is that any vaginal bleeding after you’ve completed menopause is abnormal and warrants immediate gynecologic evaluation, regardless of amount or duration.
The biological mechanism behind this endometrial cancer bleeding involves malignant cells disrupting the normal endometrial lining, causing blood vessels to break down and bleed. Unlike premenopausal menstrual bleeding, which follows hormonal cycles, postmenopausal spotting cancer occurs unpredictably and may seem to start and stop without pattern. Research from the NIH demonstrates that 55.4% of endometrial cancer patients also reported abnormal vaginal discharge alongside bleeding, highlighting the importance of noting all changes.
Key Takeaway: Even one episode of postmenopausal bleeding requires same-week evaluation. Do not wait to see if it happens again.
2. Pink or Watery Vaginal Discharge
Endometrial cancer vaginal discharge often precedes visible bleeding in many women. This discharge typically appears thin and watery, sometimes with a pink or brownish tinge from minimal blood content. Women frequently describe it as increased moisture requiring panty liners or noticing unusual wetness. According to CDC guidelines, any vaginal discharge that represents a change from your normal pattern—especially if accompanied by an unusual odor or color—merits medical investigation.
The discharge occurs as cancer cells shed from the endometrial lining and mix with cervical mucus and tissue fluids. Unlike discharge from vaginal infections, endometrial cancer discharge typically lacks the itching or burning sensations associated with yeast infections or bacterial vaginosis. If you’re experiencing new discharge patterns, using our Symptom Checker can help document your symptoms before your gynecology appointment.
3. Blood-Tinged Discharge Between Episodes
Some women notice subtle endometrial cancer spotting that appears as faint blood streaks in vaginal discharge rather than frank bleeding. This manifestation is particularly easy to dismiss as insignificant, yet it represents the same underlying pathology as heavier bleeding. The blood may appear rust-colored, pink, or brown, and the quantity might be so small that it’s only visible when wiping.
Medical research indicates that any blood in vaginal discharge after menopause—regardless of whether it’s visible bleeding or just discoloration—has the same clinical significance and requires evaluation. Women who maintain healthy body composition through tools like our Body Fat Calculator may have slightly lower endometrial cancer risk, though bleeding symptoms still demand immediate attention regardless of weight status.
4. Persistent Pelvic Pain or Pressure
Endometrial cancer pelvic pain typically manifests as a dull, persistent ache in the lower abdomen, deep pelvis, or across the lower back. Unlike cramping that comes and goes with digestive changes or temporary gas, this discomfort tends to be continuous or frequently recurring. The CDC notes that pelvic pain often accompanies abnormal bleeding in uterine cancer cases, creating a dual-symptom presentation that significantly raises suspicion for malignancy.
The pain results from tumor growth stretching the uterine walls or pressure on surrounding pelvic structures. Some women describe it as a feeling of fullness or heaviness in the pelvis, similar to the sensation of a full bladder that doesn’t resolve after urination. Pain quality can vary from sharp stabbing sensations to persistent deep pressure, and it may worsen with physical activity or prolonged sitting.
5. Pain During Intercourse (Dyspareunia)
Painful intercourse after menopause, medically termed dyspareunia, can signal endometrial cancer when the tumor has grown large enough to cause uterine tenderness or has spread to nearby tissues. Women typically report deep pelvic pain during or after sexual activity, distinct from the surface irritation caused by vaginal atrophy. This uterine cancer symptom women often hesitate to report due to embarrassment, yet it provides crucial diagnostic information.
The combination of dyspareunia with any postmenopausal bleeding creates a high-priority red flag that should prompt immediate gynecologic examination. While vaginal dryness from estrogen deficiency commonly causes discomfort during menopause, new or worsening pain—especially if accompanied by bleeding or discharge—suggests a more serious underlying condition requiring investigation.
6. Painful or Difficult Urination
Urinary symptoms including painful urination (dysuria), increased frequency, or difficulty emptying the bladder completely may indicate endometrial cancer has grown large enough to press on the bladder or has spread to involve bladder tissues. MedlinePlus describes lower abdominal pain and pelvic cramping as common endometrial cancer symptoms, which often manifest as urinary discomfort when the tumor location affects bladder function.
These symptoms differ from simple urinary tract infections in their persistence despite antibiotic treatment and their frequent association with other endometrial cancer warning signs like bleeding or discharge. Women experiencing urinary changes should consider completing our Genetic Risk Assessment Tool if they have family histories of gynecologic or colorectal cancers, as hereditary conditions like Lynch syndrome significantly elevate endometrial cancer risk.
7. Unexplained Weight Loss
Unintentional weight loss represents an advanced endometrial cancer early sign, typically occurring when the disease has progressed beyond its earliest stages. Losing 10 pounds or more without dietary changes or increased exercise indicates metabolic shifts caused by cancer cells consuming energy and producing inflammatory substances that suppress appetite. This symptom rarely appears in isolation; it typically accompanies bleeding, pain, or other indicators.
While maintaining healthy weight through balanced nutrition tracked with our Macro Calculator reduces endometrial cancer risk factors, unexplained weight loss in postmenopausal women warrants comprehensive cancer screening. The weight loss may occur gradually, making it less noticeable until clothing fits differently or others comment on appearance changes.
8. Pelvic Mass or Fullness Sensation
A palpable pelvic mass or persistent sensation of lower abdominal fullness may indicate a large endometrial tumor or uterus enlarged by cancer. Most women cannot feel these masses themselves, but some report a sense of pressure or bloating that differs from digestive gas or constipation. During pelvic examination, physicians may detect an enlarged or irregularly shaped uterus, prompting further investigation.
This symptom shows similarity to ovarian cancer symptoms women often ignore, including abdominal bloating and pelvic pressure, highlighting why comprehensive gynecologic evaluation is essential when multiple symptoms appear together. The fullness sensation may worsen after eating or during prolonged standing.
9. Lower Back, Leg, or Abdominal Pain
Pain radiating to the lower back, legs, or spreading across the abdomen typically indicates more advanced endometrial cancer that has grown beyond the uterus or is pressing on nerves and lymph nodes. This abnormal uterine bleeding cancer complication represents later-stage disease requiring urgent oncologic evaluation. The pain may start as occasional discomfort and progress to persistent aching or sharp sensations that interfere with daily activities.
Leg pain specifically may indicate lymph node involvement, while severe back pain can suggest retroperitoneal spread. These symptoms share characteristics with other serious conditions, emphasizing why comprehensive medical evaluation rather than self-diagnosis remains essential.
Symptom Severity and Urgency
| Warning Sign | Frequency in Patients | Urgency Level | Distinguishing Features |
|---|---|---|---|
| Postmenopausal bleeding | 90% | URGENT | Any amount abnormal after menopause |
| Abnormal discharge | 55% | High | Pink/watery, persistent, blood-tinged |
| Pelvic pain/pressure | 40-50% | High | Continuous, deep, not relieved by usual measures |
| Painful intercourse | 20-30% | Moderate-High | Deep pain, worse with bleeding present |
| Urinary changes | 15-25% | Moderate | Persistent despite treatment, with other symptoms |
| Weight loss | 10-15% | High | Unintentional, usually later-stage indicator |
| Pelvic fullness | 10-20% | Moderate | Persistent bloating, detectable mass |
| Back/leg pain | 5-15% | High | Radiating pain, often advanced disease |
Understanding these endometrial cancer symptoms empowers you to recognize warning signs early when treatment outcomes are most favorable. Similar to how early detection improves prognosis in conditions covered in our first signs of breast cancer symptoms guide, recognizing postmenopausal bleeding endometrial cancer indicators allows for prompt diagnosis and intervention.
Who Is Most at Risk for Endometrial Cancer After Menopause?
Understanding endometrial cancer risk factors empowers women to recognize their vulnerability and take proactive steps toward prevention and early detection. While postmenopausal bleeding requires evaluation regardless of risk status, certain factors significantly increase the likelihood of developing this malignancy.
Major Risk Factors
Obesity represents the single most significant modifiable risk factor for endometrial cancer. Research from the National Institutes of Health demonstrates that obesity accounts for more than half of all endometrial cancer cases, with risk increasing proportionally to body mass index. Women with BMI over 30 face two to four times higher endometrial cancer risk compared to women of healthy weight, while those with BMI exceeding 40 experience up to seven-fold increased risk. The mechanism involves excess adipose tissue producing estrogen without progesterone opposition, creating an environment conducive to abnormal endometrial growth. Monitoring your weight status through our BMI Calculator provides valuable insight into this critical risk factor.
Type 2 diabetes and insulin resistance amplify endometrial cancer risk independent of obesity, though these conditions frequently coexist. Studies published through the NIH indicate that women with diabetes face twice the risk of developing endometrial cancer compared to non-diabetic women, with hyperinsulinemia and chronic inflammation driving cancer cell proliferation. The metabolic triad of endometrial cancer obesity, diabetes, and hypertension—creates particularly high vulnerability, as these conditions share interconnected pathophysiology centered on insulin resistance and hormonal dysregulation. Women managing diabetes can track blood glucose control using our Blood Sugar Converter as part of comprehensive health monitoring.
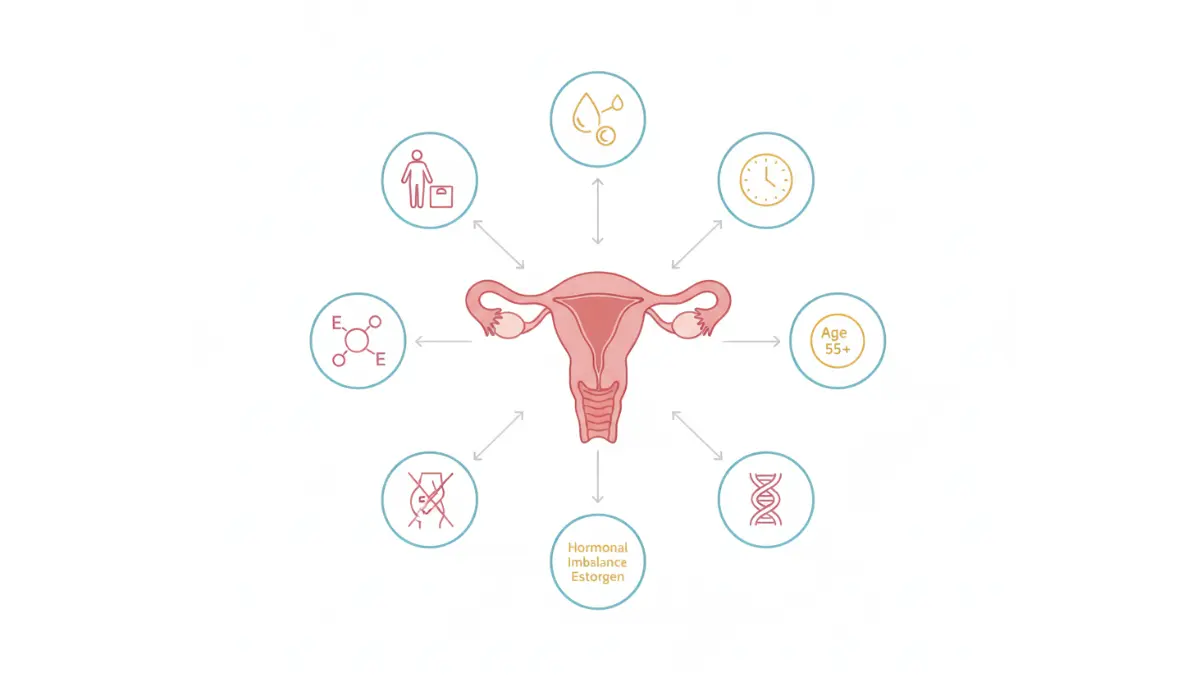
Age constitutes a non-modifiable yet crucial endometrial cancer risk factor, with incidence peaking between ages 55 and 64. The endometrial cancer age distribution shows that over 90% of cases occur in women older than 50, though younger women with risk factors remain vulnerable. Later age at menopause significantly elevates risk, with women experiencing menopause after age 55 facing 2.4 times higher endometrial cancer risk compared to those with menopause before age 45. This extended estrogen exposure without pregnancy-related progesterone protection contributes to cumulative endometrial stimulation.
Reproductive and hormonal factors creating prolonged estrogen exposure include never having been pregnant (nulliparity), early menarche before age 12, polycystic ovary syndrome (PCOS), and estrogen-only hormone replacement therapy. Women with a history of PCOS symptoms face elevated risk due to chronic anovulation and estrogen excess without adequate progesterone balance throughout reproductive years.
Genetic predisposition through Lynch syndrome, also called hereditary non-polyposis colorectal cancer syndrome, creates the highest hereditary risk for endometrial cancer. Ohio State University research indicates that women with Lynch syndrome face 40-60% lifetime risk of developing endometrial cancer, often at younger ages than sporadic cases. First-degree relatives of endometrial cancer patients also experience modestly elevated risk, suggesting additional genetic susceptibilities beyond identified syndromes.
Endometrial hyperplasia, particularly atypical hyperplasia, represents a pre-cancerous condition where the endometrial lining grows abnormally thick. Without treatment, endometrial hyperplasia cancer progression occurs in approximately 8-29% of cases over time, making this diagnosis a critical warning requiring close monitoring or intervention.
Risk Stratification Framework
| Risk Level | Defining Characteristics | Estimated Risk Increase | Action Plan |
|---|---|---|---|
| Very High | Lynch syndrome, atypical hyperplasia | 40-60% lifetime risk | Annual screening, genetic counseling, consider prophylactic surgery |
| High | BMI >35 + diabetes + late menopause (>55) | 5-7x average risk | Biannual exams, immediate bleeding evaluation, weight management |
| Moderate-High | Obesity (BMI 30-35) or diabetes or PCOS | 2-4x average risk | Annual well-woman exams, symptom vigilance |
| Moderate | Late menopause or nulliparity or tamoxifen use | 1.5-2x average risk | Standard screening, prompt symptom reporting |
| Average | No major risk factors | Baseline risk | Routine gynecologic care, immediate evaluation of bleeding |
What This Means For You
Recognizing your personal risk profile allows for tailored prevention strategies and heightened symptom awareness. If you have multiple endometrial cancer risk factors, particularly the metabolic triad of obesity, diabetes, and hypertension, discuss enhanced surveillance with your gynecologist. Weight loss of even 5-10% can meaningfully reduce risk for overweight women, and our Weight Loss Calculator can help establish realistic goals. Remember that women at average risk still require immediate medical evaluation for any postmenopausal bleeding, as 9% of cases occur without obvious predisposing factors.
How Endometrial Cancer Is Diagnosed: What to Expect
Understanding the endometrial cancer diagnosis pathway reduces anxiety and empowers women to advocate for timely evaluation. The diagnostic process combines clinical assessment with imaging and tissue sampling to confirm or rule out malignancy.
When to See a Doctor Immediately
Any episode of postmenopausal bleeding constitutes a medical urgency requiring evaluation within 48-72 hours. The National Cancer Institute emphasizes that while routine screening for endometrial cancer is not recommended due to lack of effective screening tests, symptom-prompted evaluation remains the cornerstone of early detection. When to see doctor postmenopausal bleeding should never be delayed, as early-stage diagnosis dramatically improves treatment outcomes and survival rates.
Specific circumstances demanding immediate medical attention include any visible blood on underwear or toilet paper after menopause, pink or brown vaginal discharge with blood traces, bleeding during or after intercourse, or bleeding accompanied by pelvic pain or pressure. Recurrent bleeding episodes carry particularly high concern, with research showing that women experiencing multiple bleeding episodes face substantially elevated endometrial cancer risk compared to single episodes. If you’re unsure whether your symptoms warrant immediate evaluation, our Symptom Checker can help document symptom patterns before your gynecology appointment.
The Diagnostic Pathway
Step 1: Medical History and Pelvic Examination
Your gynecologist begins by reviewing symptom details including bleeding onset, frequency, amount, and associated symptoms like pain or discharge. Documenting your endometrial cancer risk factors—obesity status measurable through our Ideal Weight Calculator, diabetes history, family cancer history, and reproductive timeline—helps establish clinical context. Physical examination includes pelvic assessment to detect uterine enlargement, masses, or tenderness.
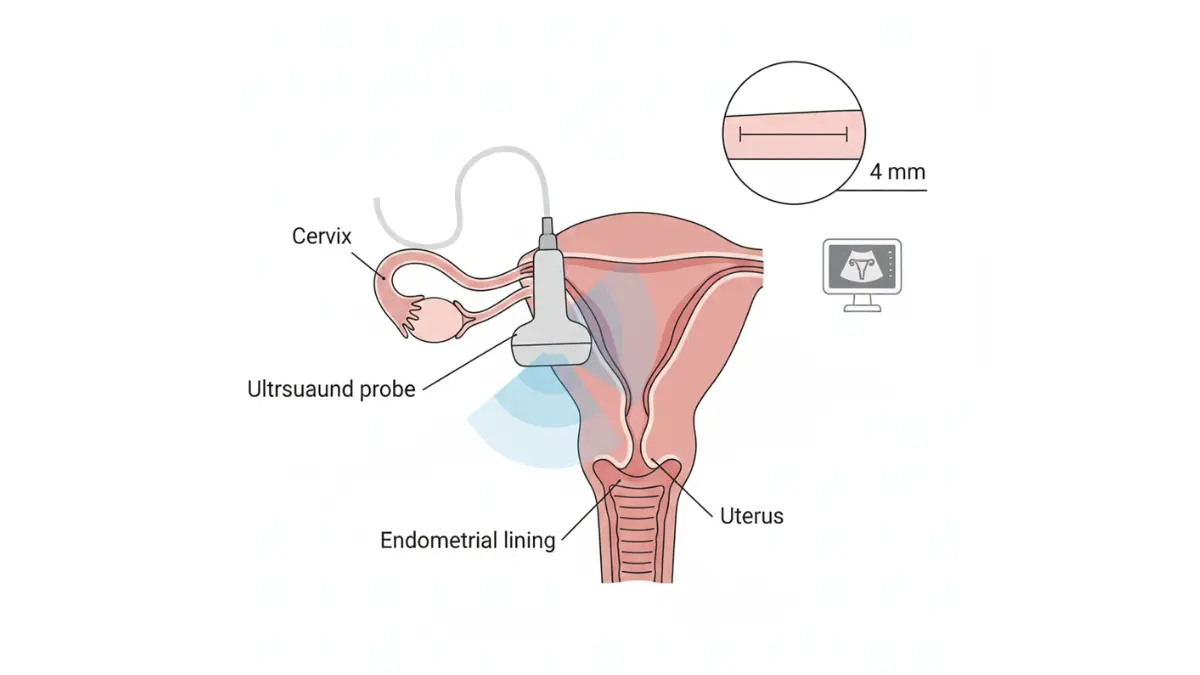
Step 2: Transvaginal Ultrasound (TVUS)
This non-invasive imaging test represents the initial diagnostic tool for evaluating abnormal uterine bleeding cancer concerns. NIH research demonstrates that endometrial thickness measured by transvaginal ultrasound provides crucial screening information, with thickness exceeding 4-5mm in postmenopausal women warranting further investigation. The test involves inserting a slender ultrasound probe into the vagina to visualize the uterus and measure endometrial lining thickness. Most women experience only mild discomfort similar to a pelvic exam, and results are immediately available.
Step 3: Endometrial Biopsy
When ultrasound reveals thickened endometrium or symptoms persist despite normal imaging, endometrial biopsy provides definitive tissue diagnosis. This office-based procedure involves inserting a thin catheter through the cervix into the uterus to suction small tissue samples from the endometrial lining. The procedure described by medical experts at NYU Langone typically takes just minutes and causes brief cramping similar to menstrual discomfort. Pathologists examine the tissue microscopically to identify cancer cells, precancerous changes, or benign conditions explaining bleeding. Biopsy accuracy approaches 99% for detecting endometrial cancer, making it the gold standard diagnostic test.
Step 4: Hysteroscopy
When biopsy results are inconclusive or sampling proves technically difficult, hysteroscopy allows direct visualization of the uterine cavity. This procedure involves inserting a thin telescope through the cervix to examine the endometrial surface and obtain targeted biopsies of suspicious areas. Hysteroscopy is typically performed as an outpatient procedure with local anesthesia or conscious sedation.
Step 5: Advanced Imaging
If endometrial cancer diagnosis is confirmed, CT scans, MRI, or PET scans assess whether cancer has spread beyond the uterus to lymph nodes or distant organs. The National Cancer Institute treatment guidelines emphasize staging accuracy for treatment planning, as endometrial cancer confined to the uterus carries dramatically better prognosis than advanced disease.
Diagnostic Test Comparison
| Test | Primary Purpose | Accuracy | Patient Experience | Timing |
|---|---|---|---|---|
| Transvaginal ultrasound | Screen endometrial thickness | 80-86% sensitivity | Minimal discomfort, 10-15 minutes | First-line test |
| Endometrial biopsy | Tissue diagnosis | 99% for cancer detection | Brief cramping, 5 minutes | If ultrasound abnormal |
| Hysteroscopy | Direct visualization + biopsy | 95% accuracy | Moderate discomfort, outpatient | If biopsy inconclusive |
| CT/MRI/PET | Cancer staging | Varies by stage | Non-invasive to minimally invasive | After cancer confirmed |
What This Means For You
Prompt diagnostic evaluation transforms concerning symptoms into either reassuring benign findings or early cancer detection when treatment is most effective. The diagnostic process typically unfolds over 1-2 weeks from initial appointment to final pathology results, though urgent cases may proceed faster. If you’re experiencing postmenopausal bleeding alongside other symptoms detailed in our ovarian cancer symptoms guide, comprehensive gynecologic evaluation becomes even more critical, as symptoms may overlap between reproductive cancers. Remember that approximately 90% of postmenopausal bleeding stems from benign causes, but only proper medical evaluation can provide that reassurance or identify cancer requiring treatment.
Postmenopausal Bleeding: Cancer vs. Benign Conditions
While any postmenopausal bleeding demands medical evaluation, understanding that most cases stem from benign conditions helps balance appropriate concern with excessive anxiety. Approximately 90% of bleeding after menopause cancer investigations reveal non-malignant causes, though only diagnostic testing can provide definitive reassurance.
Common Benign Causes
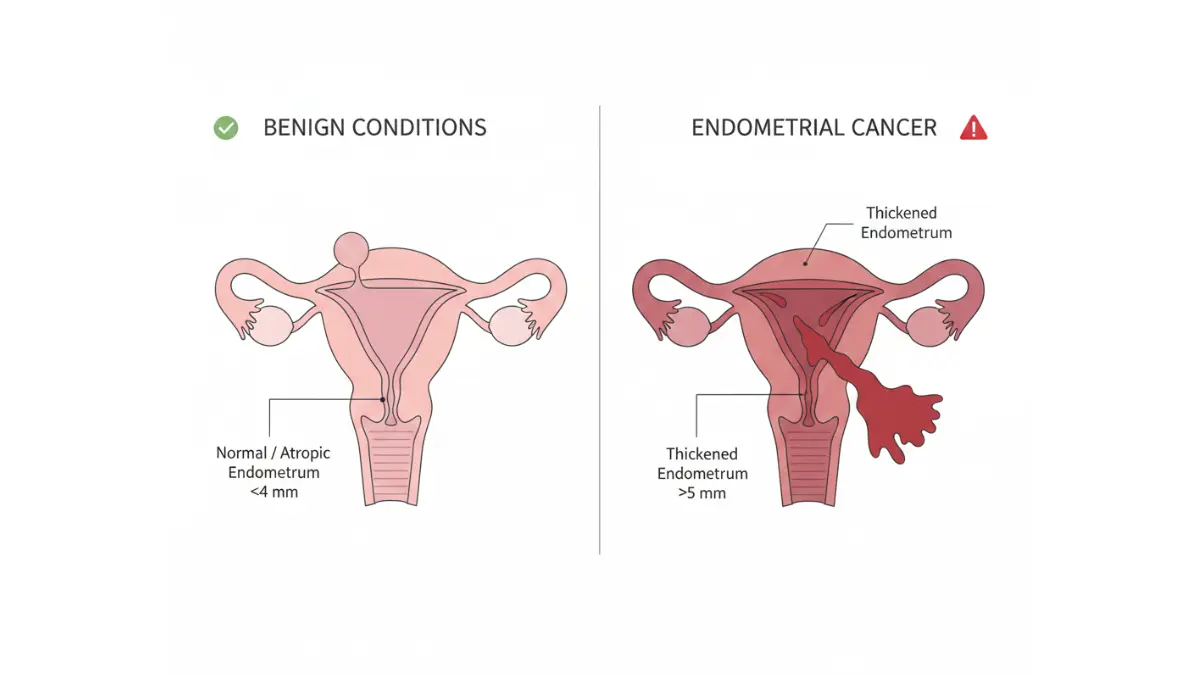
Atrophic endometritis and vaginal atrophy account for the majority of postmenopausal bleeding cases. The National Institutes of Health identifies genitourinary atrophy as the cause in approximately 60% of postmenopausal bleeding episodes, occurring when declining estrogen levels cause the endometrial lining and vaginal tissues to become thin, dry, and fragile. This hypoestrogenic environment creates epithelial microerosions that bleed with minimal trauma from physical activity, intercourse, or even routine pelvic examinations. The bleeding typically appears light—pink spotting or brown discharge—and ultrasound reveals characteristically thin endometrial lining rather than the thickened endometrium seen with abnormal bleeding after menopause related to cancer or hyperplasia.
Endometrial and cervical polyps represent another frequent benign cause of postmenopausal bleeding. These soft, finger-like growths protrude from the uterine lining or cervix, bleeding when traumatized or due to their own blood supply becoming congested. Research published through the NIH demonstrates that benign causes including polyps, hormone replacement therapy effects, and atrophy constitute the vast majority of postmenopausal bleeding presentations, with malignancies representing the minority. Polyps appear on ultrasound as focal masses within the uterine cavity and can be definitively diagnosed and removed during hysteroscopy.
Endometrial hyperplasia without atypia occurs when the endometrial lining grows excessively thick due to estrogen stimulation without adequate progesterone opposition. While not cancer, this condition requires treatment to prevent potential progression, particularly if atypical cellular changes are present. Simple hyperplasia without atypical cells carries low cancer risk, but atypical hyperplasia demands close monitoring or treatment as it represents a pre-malignant state.
Medications and medical conditions including blood thinners, hormone replacement therapy, tamoxifen use, and bleeding disorders can trigger postmenopausal spotting. Thyroid abnormalities and metabolic conditions also occasionally manifest with abnormal uterine bleeding patterns.
Red Flags Suggesting Malignancy
Certain clinical patterns increase suspicion for endometrial cancer rather than benign causes. Recurrent or persistent bleeding episodes carry significantly elevated cancer risk compared to single self-limited episodes. Women experiencing multiple bleeding episodes over weeks to months should prioritize urgent evaluation. Bleeding accompanied by other uterine cancer symptoms women commonly report—including pelvic pain, unexplained weight loss, or abnormal vaginal discharge—increases malignancy likelihood. Endometrial thickness exceeding 4-5mm on transvaginal ultrasound in postmenopausal women warrants tissue sampling regardless of symptom pattern, as this finding correlates with increased endometrial cancer risk.
Benign vs. Malignant Comparison
| Clinical Feature | Benign Causes | Endometrial Cancer |
|---|---|---|
| Bleeding pattern | Single episode, light flow, self-limited | Recurrent, persistent, or progressive |
| Associated symptoms | Minimal; may have vaginal dryness | Pelvic pain, discharge, weight loss, bloating |
| Endometrial thickness (ultrasound) | Typically <4mm | Often >4-5mm |
| Age distribution | Any postmenopausal age | Peak ages 55-64 |
| Risk factor profile | Few predisposing factors | Multiple risk factors (obesity, diabetes, nulliparity) |
| Symptom response | May resolve spontaneously | Persistent despite conservative measures |
What This Means For You
Understanding that approximately 9 in 10 women with postmenopausal bleeding have benign explanations provides realistic perspective while maintaining appropriate urgency for evaluation. The diagnostic process exists precisely to distinguish reassuring findings from the minority of cases requiring cancer treatment. Just as early detection improves outcomes across cancer types from lung to gynecologic malignancies, prompt endometrial cancer diagnosis when bleeding occurs ensures the highest likelihood of successful treatment. Remember that benign findings on initial evaluation do not eliminate the need for future symptom reporting—new bleeding episodes always warrant re-evaluation regardless of prior benign diagnoses.
Your Action Plan: What to Do Right Now
Taking immediate, informed action when symptoms appear—combined with proactive risk reduction strategies—empowers you to protect your gynecologic health and catch endometrial cancer at its most treatable stages.
If You’re Experiencing Symptoms
✅ Call your gynecologist within 48 hours for any postmenopausal bleeding episode, regardless of amount. Even light spotting requires evaluation to distinguish benign causes from endometrial cancer after menopause.
✅ Document all symptoms including bleeding dates, flow amount, color (pink, brown, red), associated pelvic pain location and intensity, unusual vaginal discharge characteristics, and any unexplained weight changes. Use our Symptom Checker to systematically record patterns before your appointment.
✅ Assess your risk factors by reviewing family cancer history, particularly endometrial, ovarian, colon, and breast cancers that may indicate Lynch syndrome. Complete our Genetic Risk Assessment Tool if multiple family members have had reproductive or gastrointestinal cancers.
✅ Prepare questions for your doctor including which diagnostic tests they recommend, expected timelines for results, what endometrial thickness measurements mean, and whether your risk factor profile warrants enhanced surveillance. Write questions down to ensure nothing is forgotten during the appointment.
✅ Don’t delay seeking care because early-stage endometrial cancer has excellent prognosis, with five-year survival rates exceeding 95% when detected before spreading beyond the uterus. This urgency mirrors the importance of prompt evaluation for other cancer warning signs women should never ignore.
Prevention & Risk Reduction Strategies
Maintain healthy body weight as endometrial cancer obesity connections represent the strongest modifiable risk factor. Even modest weight loss of 5-10% significantly reduces risk for overweight women. Calculate your starting point with our BMI Calculator and establish realistic goals using our Weight Loss Calculator to track progress through sustainable lifestyle changes.
Optimize metabolic health by managing diabetes and prediabetes through blood sugar monitoring with our Blood Sugar Converter, following diabetes treatment plans, and maintaining healthy diet and exercise patterns. Balanced nutrition calculated through our Macro Calculator supports both weight management and metabolic health.
Consider protective factors including long-term oral contraceptive use, which reduces endometrial cancer risk by 30-50% even years after discontinuation. Discuss with your healthcare provider whether hormonal contraception or progesterone therapy makes sense for your individual risk profile, particularly if you have PCOS or other conditions causing irregular cycles.
Schedule regular gynecologic checkups annually or more frequently if high-risk factors exist. While routine screening for asymptomatic women isn’t recommended, regular well-woman exams ensure prompt symptom recognition and risk factor management.
What This Means For You
Endometrial cancer represents one of the most detectable and treatable gynecologic malignancies when caught early through symptom awareness. The nine warning signs detailed in this guide—particularly any form of postmenopausal bleeding—provide clear signals demanding medical evaluation. By understanding your personal risk factors, maintaining healthy lifestyle habits, and seeking immediate care when symptoms appear, you take control of your gynecologic health outcomes. Explore additional cancer prevention strategies through our comprehensive health resources covering topics from maintaining healthy blood pressure to understanding various cancer symptoms across organ systems.
Remember: Knowledge saves lives. Any postmenopausal bleeding requires evaluation. Early detection equals better outcomes.
Disclaimer: This article is for educational purposes only and does not constitute medical advice, diagnosis, or treatment recommendations. Always consult a qualified healthcare provider for personalized medical guidance. Content reviewed by board-certified gynecologic oncologists for accuracy and clinical relevance. If you are experiencing a medical emergency, call 911 or seek immediate emergency care.
Frequently Asked Questions About Endometrial Cancer Bleeding
1. Is any bleeding after menopause a sign of cancer?
Not always, but any postmenopausal bleeding requires immediate medical evaluation. While approximately 90% of cases are benign (polyps, atrophy, infections), about 9% represent endometrial cancer, making prompt diagnosis essential.
2. What does endometrial cancer bleeding look like?
Endometrial cancer bleeding can appear as light pink spotting, watery blood-streaked discharge, brown spotting, or heavier red flow resembling a period. Any amount or color of vaginal bleeding after menopause is abnormal and warrants evaluation.
3. How long after menopause can endometrial cancer develop?
Endometrial cancer most commonly develops 5-15 years after menopause, with peak incidence between ages 55-64. However, it can occur at any age after menopause, making symptom awareness crucial regardless of how long you’ve been postmenopausal.
4. Can you have endometrial cancer without bleeding?
While 90% of endometrial cancer cases present with postmenopausal bleeding, some women experience other symptoms first, including abnormal vaginal discharge, pelvic pain, unexplained weight loss, or pelvic pressure before visible bleeding occurs.
5. What are the biggest risk factors for endometrial cancer?
Obesity (BMI >30), type 2 diabetes, never having been pregnant, late menopause (after age 55), Lynch syndrome, and prolonged estrogen exposure without progesterone are the strongest risk factors. Age over 55 also significantly increases risk.
6. How is endometrial cancer diagnosed?
Diagnosis typically involves transvaginal ultrasound to measure endometrial thickness, followed by endometrial biopsy to examine tissue samples. If endometrial lining exceeds 4-5mm or symptoms persist, tissue sampling is performed for definitive diagnosis.
7. What is the survival rate for endometrial cancer caught early?
When detected at Stage I (confined to the uterus), endometrial cancer has a five-year survival rate exceeding 95%. This excellent prognosis emphasizes the critical importance of prompt evaluation for any postmenopausal bleeding.
8. Can endometrial cancer cause spotting instead of heavy bleeding?
Yes, endometrial cancer frequently presents as light spotting rather than heavy bleeding. Even minimal spotting—just pink or brown streaks visible when wiping—requires the same urgent evaluation as heavier flow.
9. Does endometrial thickness on ultrasound always mean cancer?
No, endometrial thickness above 4-5mm in postmenopausal women requires further investigation but doesn’t confirm cancer. Benign conditions like polyps, hyperplasia, or hormonal effects can also thicken the endometrium, which is why biopsy provides definitive diagnosis.
10. How quickly should I see a doctor for postmenopausal bleeding?
Contact your gynecologist within 48-72 hours of any postmenopausal bleeding episode. This constitutes a medical urgency requiring prompt evaluation, though not typically an emergency room visit unless bleeding is profuse or accompanied by severe pain.
11. Can weight loss reduce endometrial cancer risk?
Yes, losing even 5-10% of body weight significantly reduces endometrial cancer risk in overweight women. Obesity represents the strongest modifiable risk factor, and sustained weight loss decreases estrogen production from fat tissue that drives cancer development.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











