PCOS Symptoms in Women: 7 Signs You Shouldn’t Ignore?
Polycystic ovary syndrome (PCOS) affects up to 10% of women of reproductive age, causing hormonal imbalances that disrupt cycles, metabolism, and appearance. The 7 key signs you shouldn’t ignore include irregular periods, excess hair growth, acne, weight gain struggles, fertility issues, fatigue, and dark skin patches—these often cluster together and worsen without attention. Early recognition helps prevent diabetes, heart risks, and infertility through simple tracking and clinician visits.
PCOS involves ovaries producing excess androgens (male hormones) alongside insulin resistance, leading to subtle symptoms many dismiss as stress or aging. Women often notice changes in their 20s or 30s, but delays in diagnosis average 2–5 years due to overlapping signs with normal variation. Use our Symptom Checker to log patterns before discussing with a doctor.
Consider Sarah’s story: A 28-year-old teacher ignored skipped periods and chin hair for three years, blaming work stress—until unexplained weight gain and failed conception attempts led to her PCOS diagnosis. Her case mirrors thousands where early flags get overlooked, turning manageable issues into fertility battles.
The 7 PCOS Symptoms You Shouldn’t Ignore
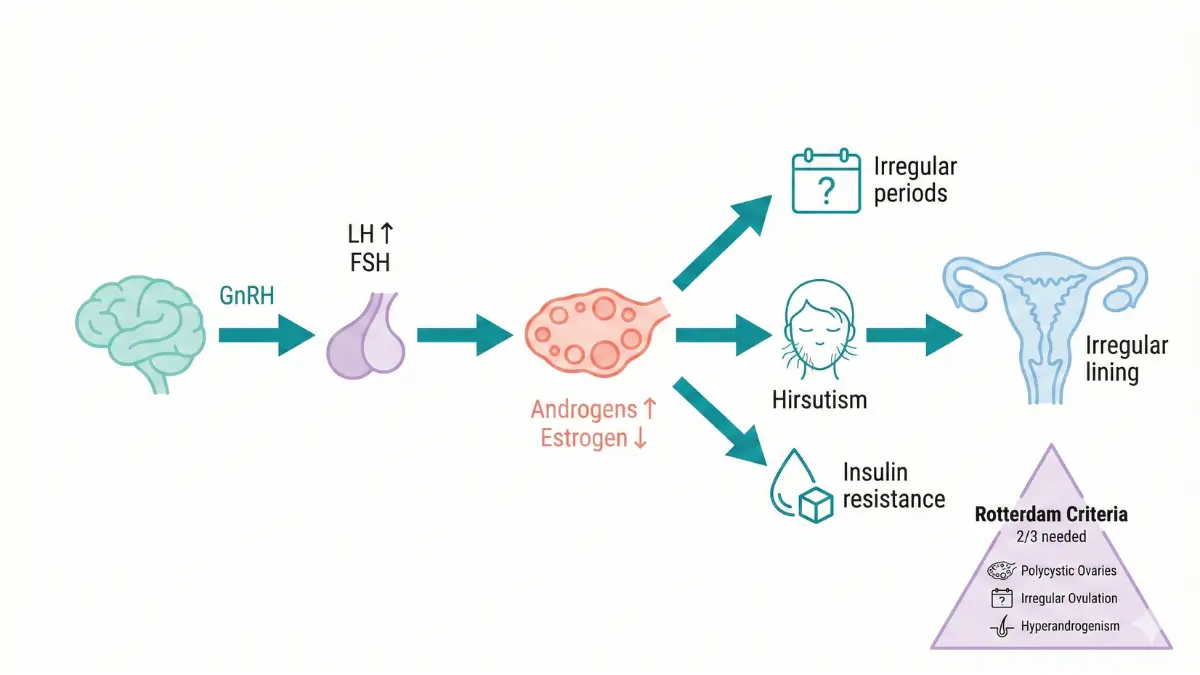
These signs stem from the Rotterdam criteria (needing 2 of 3: irregular ovulation, high androgens, polycystic ovaries on ultrasound), per international guidelines. They rarely appear alone—watch for clusters.
- Irregular or missed periods: Cycles longer than 35 days, fewer than 8–9 yearly, or absent flow signal anovulation. Track with our Ovulation Calculator to spot patterns.
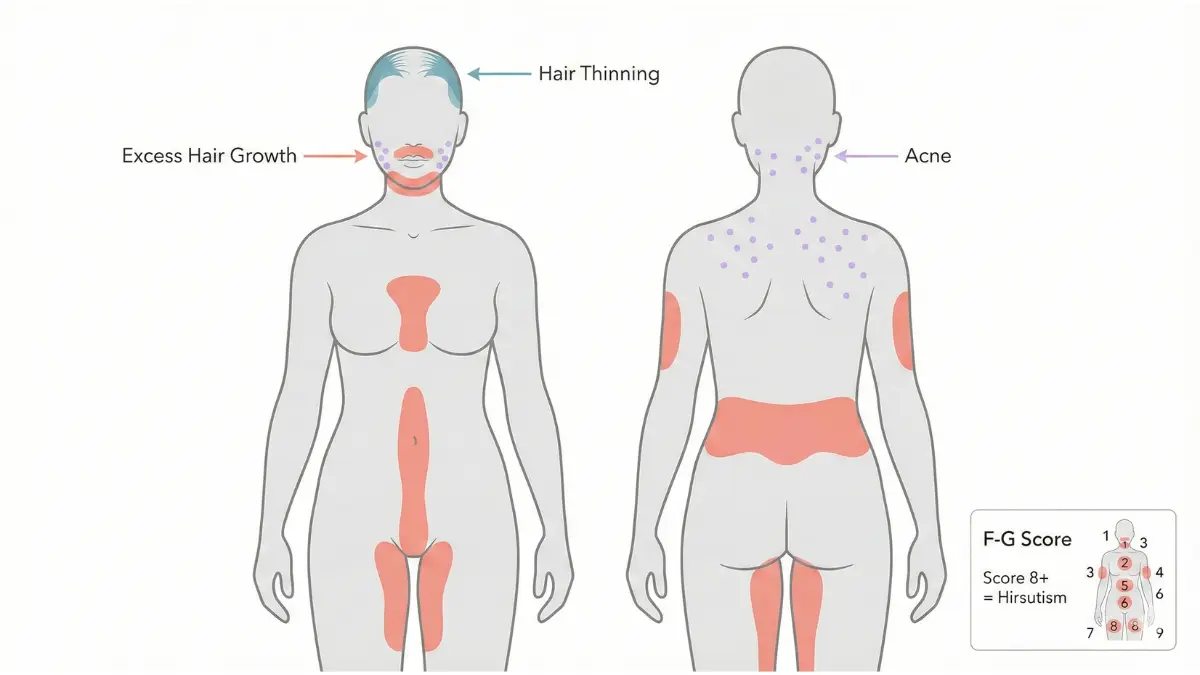
- Excess facial/body hair (hirsutism) and scalp thinning: Androgens cause coarse hair on chin, upper lip, chest; meanwhile, scalp hair thins like male-pattern baldness. Affects 70–80% of cases.
- Persistent acne and oily skin: Jawline cysts or back acne unresponsive to skincare often ties to hormone surges, not just teen years.
- Unexplained weight gain, especially belly fat: Insulin resistance drives central obesity; even normal-weight women face challenges. Check baselines via BMI Calculator or Body Fat Percentage Calculator.
- Fertility struggles or ovulation issues: Difficulty conceiving after 6–12 months often links to absent eggs. Explore our Pregnancy Due Date Calculator for planning.
- Fatigue, mood swings, and sleep issues: Constant tiredness or apnea-like snoring reflects metabolic strain; pair with our Sleep Calculator.
- Dark skin patches (acanthosis nigricans) and cravings: Velvety neck or armpit discoloration signals insulin problems; sugar urges follow. Monitor via Blood Sugar Converter.
Key takeaway: If 3+ signs persist 3–6 months, seek evaluation—early steps cut long-term risks by 50% per cohort data.
Why Diagnose PCOS Early? The Real Stakes
Untreated PCOS raises type 2 diabetes odds 3–7 fold, per NIH summaries, plus heart disease and endometrial cancer from unopposed estrogen. Mental health suffers too—twice the depression risk. Our Health Tips hub offers related metabolic guides.
Three Reading Modes Here:
- Simple: Spot the 7 signs above; see a doctor if clustered.
- Standard: Use linked tools to track; review stories and risks.
- Clinical: Rotterdam criteria noted; evidence from WHO/NHS guidelines prioritizes high-confidence signs.
Ignoring these turns reversible hormone glitches into chronic burdens, but awareness flips the script. For deeper dives, explore Genetic Risk Assessment Tool family factors.
How PCOS Shows Up in Your Cycle and Hormones
PCOS disrupts menstrual cycles through irregular ovulation and excess androgens, leading to patterns like cycles longer than 35 days or fewer than 9 per year. These changes signal anovulation, where eggs fail to release properly, per guidelines from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK). Track yours using our Ovulation Calculator to identify red flags early.
Hormonal signs often cluster, making them hard to dismiss as “normal.” International data shows 70-80% of women with PCOS experience these, varying by ethnicity and region. Early awareness cuts diagnostic delays from years to months.
How Does PCOS Affect Your Period and Ovulation?
PCOS commonly causes irregular, infrequent, or absent periods due to failed ovulation—cycles may stretch beyond 35 days, drop to under 9 yearly, or bring heavy bleeding (menorrhagia) lasting over 7 days. Light spotting between periods or severe cramps can also occur, though pain more often ties to co-existing issues like endometriosis.
- Oligomenorrhea: Fewer than 9 periods annually signals low hormone pulses needed for ovulation.
- Amenorrhea: No periods for 3+ months (secondary) raises endometrial cancer risk from unopposed estrogen.
- Polymenorrhea: Cycles under 21 days, though less common, disrupt hormone balance.
What this means for you: Log 3-6 months of cycles before your appointment. If patterns match, discuss with a gynecologist—our Symptom Checker helps organize details. Even regular-appearing cycles can hide anovulation, confirmed via labs or ultrasound.
Key takeaway: Fewer than 8-9 periods yearly warrants evaluation, as it doubles infertility risk per cohort studies.
7 Signs in Your Hormones and Hair-Skin Changes You Shouldn’t Ignore
Hyperandrogenism—elevated male hormones like testosterone—affects 60-80% of PCOS cases, driving visible changes beyond puberty. These differ from normal variation by sudden onset, progression, or distress, per Mayo Clinic overviews.
Facial and body hair growth (hirsutism) hits the chin, upper lip, chest, or back with coarse, dark strands—scoring systems like Ferriman-Gallwey rate severity above 8 as clinical. Scalp thinning follows female-pattern loss, with widening parts or crown recession from androgen sensitivity. Persistent acne clusters on jawline, chin, or back as cystic, oily breakouts resisting standard treatments.
What this means for you: Photograph changes monthly for your doctor. Lifestyle tweaks like our Protein Intake Calculator support hormone balance discussions. Regional differences matter—hirsutism appears more in Mediterranean or South Asian women.
Key takeaway: Androgen signs plus cycle issues confirm 70% of diagnoses; seek labs for free/total testosterone.
Clinical Snapshot: Rotterdam Criteria for Diagnosis
For clinicians: PCOS requires 2 of 3 criteria—oligo/anovulation, clinical/biochemical hyperandrogenism, polycystic ovarian morphology on ultrasound—after excluding mimics like thyroid disease. Strengths: widely adopted globally; limitations: ultrasound thresholds vary (e.g., 12+ follicles 2-9mm), ethnicity biases hirsutism scores, per NCBI reviews.
Evidence pyramid:
- High confidence: Cycle history + androgen levels (meta-analyses).
- Moderate: Ultrasound (operator-dependent).
- Limited: Self-reported symptoms alone.
WHO notes geopolitical variations—e.g., lean PCOS common in Asia vs obese in West—affecting presentation. Pair with metabolic screening via Blood Sugar Converter baselines.
Three Reading Modes Here:
- Simple: Watch for long cycles + hair/acne changes.
- Standard: Use tables/tools for tracking.
- Clinical: Apply Rotterdam with evidence tiers.
Explore our Health Tips for related hormone guides. Early hormone checks prevent 30-50% of downstream risks.
Metabolic, Weight, and Blood Sugar Clues That Point to PCOS
PCOS often reveals itself through unexplained weight gain, intense cravings, and stubborn belly fat—key signs of underlying insulin resistance and issues with blood sugar control. These metabolic warnings are seen in up to 70% of women with PCOS, regardless of their body size, and increase risks for prediabetes, heart disease, and type 2 diabetes, as detailed by the Centers for Disease Control and Prevention.
Why PCOS Makes Weight and Metabolism Feel ‘Stuck’
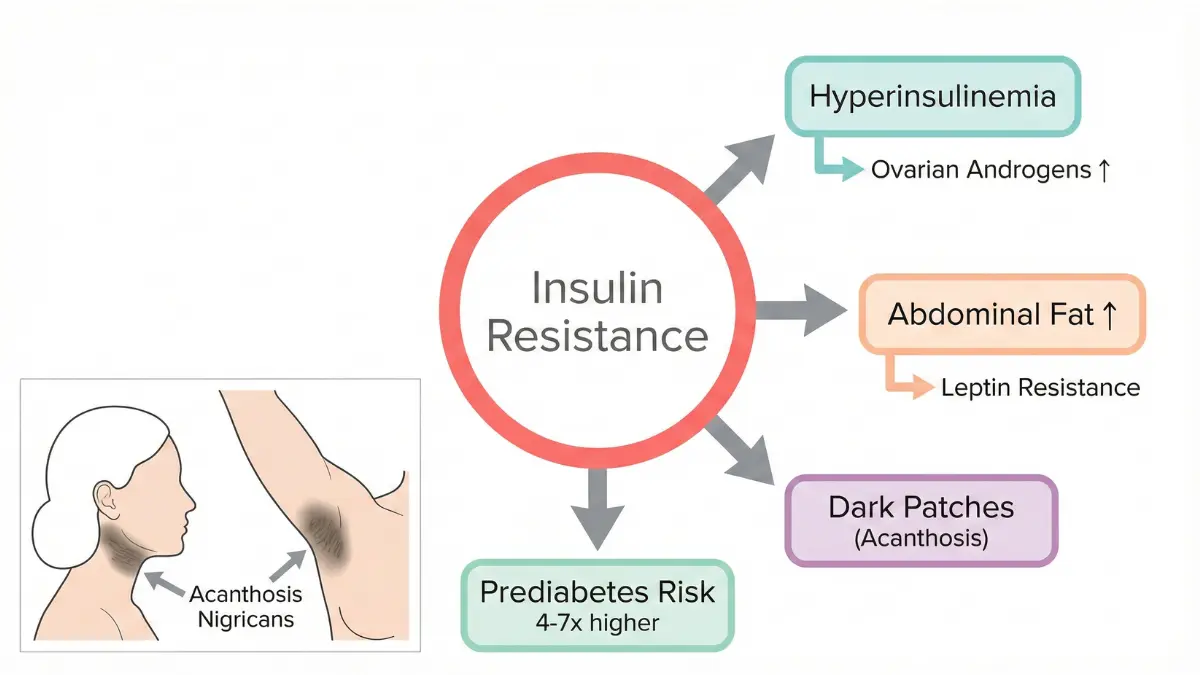
Insulin resistance—the inability of cells to respond properly to insulin—means the body produces even more insulin, which triggers the ovaries to release excess androgens (male hormones) and signals the body to store more abdominal fat. This cycle makes weight gain especially in the belly (“PCOS belly”) common, even for women who eat well and exercise consistently.
- Rapid, unexplained weight gain (especially around the waist), despite healthy eating and staying active.
- Persistent fatigue and low energy, regardless of sleep quality.
- Fierce sugar or carb cravings, tied to fluctuating blood sugar.
- Difficulty losing weight despite lifestyle changes (calories, exercise adjustments).
- Family history of diabetes, high cholesterol, or high blood pressure.
Take a quick check with the BMI Calculator or the Body Fat Percentage Calculator to track baseline numbers for your next clinic visit—regular monitoring can catch changes early.
What this means for you: If your weight, cravings, and energy seem “stuck,” use the Weight Loss Calculator and the Calorie Deficit Calculator as practical self-assessment tools, then discuss results with a healthcare provider.
Early Blood Sugar and Cardiovascular Warning Signs
Insulin resistance often produces less obvious symptoms, but some warning signs include:
- Dark, velvety skin patches on the neck, armpits, or groin (acanthosis nigricans).
- Increased thirst and urination patterns.
- Family history of type 2 diabetes or heart disease.
Using the Blood Sugar Converter can help translate fingerstick numbers into patterns your doctor can review.
The National Institutes of Health further notes untreated insulin resistance raises the risk of metabolic syndrome, cardiovascular disease, and prediabetes by 4-7 times. Managing blood sugar and heart health is critical for long-term outcomes.
Sleep, Fatigue, and Mood as Metabolic Clues
Many with PCOS experience chronic tiredness and disrupted sleep quality, with a higher frequency of sleep apnea and insomnia—especially in those with higher body mass index. Disturbed sleep patterns may worsen fatigue, irritability, and cravings.
- Sleep Calculator: Utilized for identifying healthy patterns; optimizing routine can boost energy and metabolic function.
- Heart Rate Zone Calculator: Useful for designing safe, effective exercise plans, since movement helps balance insulin and improve mood.
Key takeaway: If you struggle with weight that won’t budge, unexplained fatigue, cravings, or dark skin patches, ask for a full metabolic workup—including glucose, insulin, HbA1c, and lipid profile. Document results with our Symptom Checker for your next appointment.
For additional information about the metabolic risks linked to PCOS, review this NIH overview.
Fertility, Pregnancy, and Long-Term Health Risks of Ignoring PCOS Symptoms
PCOS affects fertility in up to 70-80% of cases due to irregular ovulation, but many women conceive successfully with targeted support like lifestyle changes or medications. Ignoring these signs raises risks for pregnancy complications like gestational diabetes and long-term issues including type 2 diabetes and heart disease, as outlined by the Eunice Kennedy Shriver National Institute of Child Health and Human Development.
Early intervention restores ovulation in 50-70% of women, per cohort studies, preventing escalation to advanced treatments. Track your cycle with the Ovulation Calculator to discuss patterns with a specialist.
What PCOS Means for Fertility and Ovulation
PCOS disrupts egg maturation and release, leading to anovulation—where follicles grow but fail to ovulate—making conception harder after 6-12 months of trying. Even with regular periods, subtle hormone imbalances can hide this issue.
- Fewer than 9 periods yearly or cycles over 35 days signal low ovulation rates.
- Elevated androgens block follicle development, per Rotterdam criteria.
- Lean PCOS (normal BMI) still carries 40-50% infertility risk.
What this means for you: If trying to conceive, log fertile windows using the Pregnancy Due Date Calculator and seek evaluation after 6 months (or sooner if over 35). The National Institute of Diabetes and Digestive and Kidney Diseases recommends prompt fertility screening.
Key takeaway: Lifestyle alone restores ovulation in 30-50% of cases; combine with clinician-guided ovulation induction for best odds.
Pregnancy Outcomes and Complications Linked to PCOS
Women with PCOS face higher risks during pregnancy, though not all experience them—close monitoring reduces complications significantly. Gestational diabetes occurs 2-3 times more often due to insulin resistance.
Use the Fetal Growth Percentile Calculator alongside prenatal scans to track development—share with your OB-GYN. The Pregnancy Weight Gain Calculator supports healthy gains amid PCOS challenges.
What this means for you: Request early glucose screening at 12-16 weeks if PCOS-diagnosed. Metformin continuation may lower risks, per guidelines.
Long-Term Health Risks If PCOS Symptoms Are Ignored
Untreated PCOS elevates lifetime risks: type 2 diabetes (4-7x), cardiovascular disease (2-4x), high cholesterol, hypertension, and endometrial cancer from chronic anovulation. Depression and anxiety affect 35-60%, compounding metabolic strain.
- Metabolic: Progresses to prediabetes in 30-40% by age 40.
- Cardiovascular: Atherosclerosis risk doubles with insulin resistance.
- Cancer: Endometrial hyperplasia risk triples without progesterone protection.
- Mental health: Twice the odds of severe mood disorders.
Monitor via BMR Calculator for energy needs and Ideal Weight Calculator for targets—discuss annual labs (A1c, lipids, BP).
Clinical note: Screening intervals vary—every 1-3 years per NIH, adjusted for BMI and family history. Strengths: broad applicability; limitations: lacks ethnicity-specific thresholds.
Patient vignette: Maria, 32, dismissed irregular cycles until fertility testing revealed PCOS—lifestyle changes plus letrozole led to a healthy pregnancy, averting diabetes progression seen in delayed cases.
Three Reading Modes Here:
- Simple: PCOS raises fertility/pregnancy risks; see a doctor early.
- Standard: Review tables, tools, and action steps.
- Clinical: Evidence tiers and screening guidelines noted.
Check our Health Tips for metabolic support. Proactive steps slash risks by 50%+.
How to Tell If Your Symptoms Might Be PCOS (And What to Do Next)
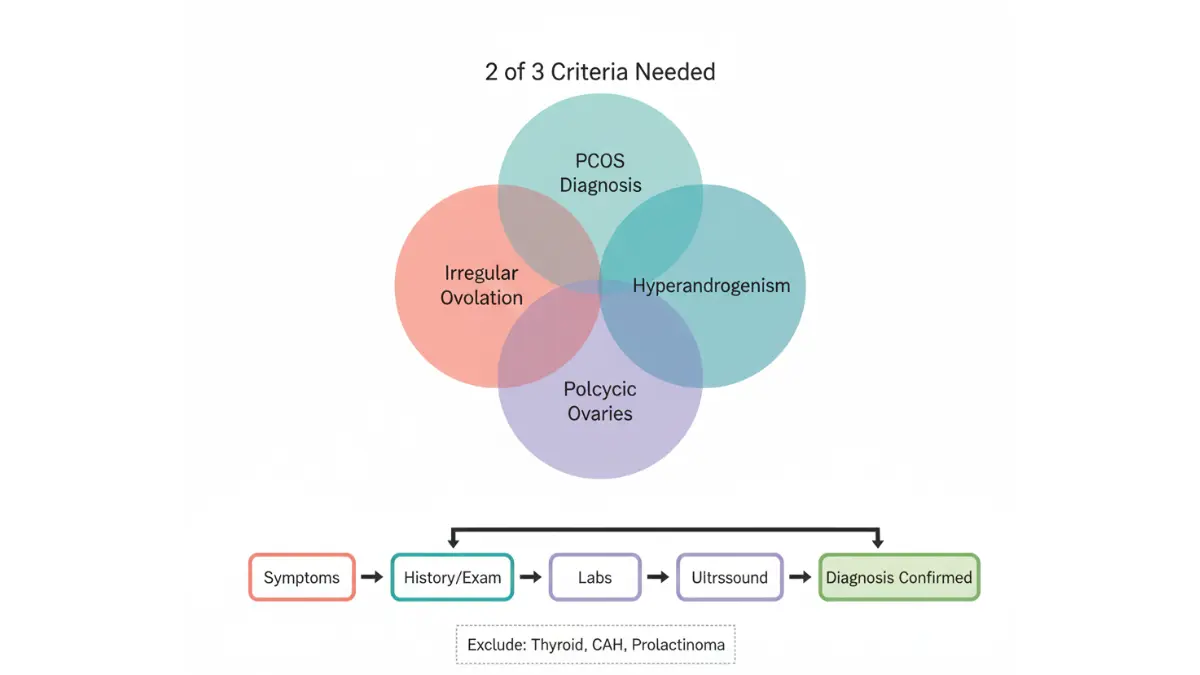
PCOS diagnosis requires at least two of three Rotterdam criteria—irregular ovulation, hyperandrogenism, and polycystic ovaries—after ruling out mimics like thyroid issues or adrenal disorders. One symptom alone isn’t enough, but persistent clusters over 3-6 months warrant evaluation, per National Center for Biotechnology Information reviews. Start logging with our Symptom Checker to prepare for your clinician.
Distinguishing PCOS from normal ups-and-downs saves years of delay—average diagnosis lag is 2-5 years globally. Use tools like the Genetic Risk Assessment Tool to note family patterns before your visit.
PCOS vs Normal Variation – When to Worry
A single skipped period or mild acne might be stress-related, but PCOS shows clusters persisting 3+ months: irregular cycles plus hair growth or weight struggles signal evaluation time.
Checklist: Yes to 3+? See a doctor promptly
- Cycles longer than 35 days or fewer than 9 yearly.
- New coarse facial/chest hair or scalp thinning.
- Jawline acne unresponsive to skincare.
- Unexplained central weight gain despite efforts.
- Fatigue, cravings, or dark skin patches.
- Difficulty conceiving after 6-12 months.
- Family history of diabetes/PCOS.
What this means for you: Track symptoms daily via Symptom Checker—print for your appointment. The Centers for Disease Control and Prevention urges early checks to avert metabolic risks.
Key takeaway: Clusters >3 symptoms raise PCOS odds 5-10x; don’t wait for “perfect” proof.
How Doctors Actually Diagnose PCOS (Clinical Mode)
Diagnosis blends history, exam, labs, and imaging—never one test alone.
- History and exam: Cycle logs, androgen signs (hirsutism score), BMI, acanthosis nigricans.
- Labs: Testosterone (free/total), LH/FSH ratio, fasting glucose/insulin, thyroid (TSH), prolactin, 17-OH progesterone to exclude congenital adrenal hyperplasia.
- Ultrasound: 12+ follicles (2-9mm) per ovary or ovarian volume >10mL—but not required if other criteria met.
Evidence pyramid:
- High: History + labs (meta-analyses).
- Moderate: Ultrasound (observer variability).
- Limited: Symptoms alone.
The National Institute of Diabetes and Digestive and Kidney Diseases stresses excluding mimics first.
Practical Next Steps – What This Means For You
Turn suspicion into action with these steps:
- Track 3-6 months: Cycles, weight, hair/acne photos, energy via Sleep Calculator.
- Prep questions: “Do I meet Rotterdam criteria? Screen for diabetes/heart risks?”
- Request baseline labs: Hormones, metabolic panel, lipids—use Blood Sugar Converter for home trends.
- Lifestyle baselines: Calculate needs with BMR Calculator, Macro Calculator, or Water Intake Calculator.
Emotional note: PCOS is common (1 in 10 women), manageable, and not your fault—many thrive post-diagnosis. Explore Health Tips for support.
Three Reading Modes Here:
- Simple: Check 3+ symptoms; book a doctor.
- Standard: Use checklist/table/tools.
- Clinical: Rotterdam + differential table.
Patient vignette: Lisa, 29, tracked irregular cycles and acne via app—labs confirmed PCOS, starting metformin restored regularity in 3 months, averting fertility delays.
Evidence-Based PCOS Management: Lifestyle, Treatment Options, and When to Be Concerned
Managing PCOS involves a combination of lifestyle changes and medical treatments tailored to symptoms and personal goals like fertility or metabolic health. International evidence-based guidelines, including the 2023 consensus from the Endocrine Society, recommend lifestyle modifications as the foundation, with medicines to regulate cycles, reduce androgen effects, and improve fertility.
Lifestyle Actions That Help PCOS Symptoms
Even modest weight loss (5–10%) improves insulin resistance, lowers androgen levels, and can restore ovulation. Behavioral strategies—goal-setting, self-monitoring, and problem solving—enhance adherence.
- Nutrition: Balanced macros, limiting simple carbs and processed foods improve blood sugar control. Use our Macro Calculator and Keto Calculator to plan meals with the right balance.
- Physical activity: Moderate cardio plus strength training recommended. Safely optimize exercise with the Heart Rate Zone Calculator and Pace Calculator.
- Sleep and stress: Improve using techniques monitored by the Sleep Calculator, which helps regulate circadian rhythms disrupted in PCOS.
What this means for you: Incorporate small, sustainable changes with these tools to boost metabolic and mood outcomes. Share progress with your healthcare provider during follow-ups.
Medical Treatment Options and What They Target
Medicines aim to regulate cycles, reduce androgen effects, and assist fertility:
- Hormonal contraceptives (birth control pills, patches, rings): First-line for menstrual irregularities, hirsutism, and acne. They reduce androgen production and protect the endometrium, lowering cancer risk. Not suitable if trying to conceive.
- Metformin: For insulin resistance and metabolic abnormalities, especially in women with prediabetes or type 2 diabetes. It can support menstrual regularity but has limited effect on hair or fertility alone. Used as a second-line fertility adjunct.
- Ovulation induction: Clomiphene citrate and letrozole remain first-line for inducing ovulation in women seeking pregnancy; letrozole has shown higher live-birth rates.
- Anti-androgens (spironolactone, cyproterone acetate): Used for hair and acne but contraindicated during pregnancy. Topical Eflornithine cream and laser therapies complement but don’t replace medications.
- Surgery (laparoscopic ovarian drilling): Occasionally used when medicines fail, normalizing hormone secretion.
What this means for you: Discuss goals with your provider to customize treatment. If fertility is desired, ovulation inducers plus lifestyle changes remain foundational. If not, hormonal contraceptives effectively manage symptoms.
Mental Health, Quality of Life, and When to Seek Urgent Care
PCOS significantly impacts mood, body image, and quality of life. Anxiety and depression affect 35-60% of women with PCOS. Address these openly with your care team.
Watch for red flags requiring urgent care:
- Severe pelvic or abdominal pain
- Excessive bleeding or spotting
- Thoughts of self-harm or severe depression
- Signs of metabolic emergency (rapid weight gain, vision changes)
If these occur, seek emergency help promptly. For ongoing support, request referrals to dietitians, endocrinologists, and mental health professionals.
Clinical Note – Guideline Changes and Emerging Frontiers
PCOS diagnosis and treatment guidelines evolve. The latest international evidence-based guideline (2023) emphasizes personalized care, lifestyle first, and cautious pharmacologic use. Emerging treatments, such as gut microbiome interventions and inositol supplements, hold promise but need further study.
Three Reading Modes:
- Simple: Lifestyle changes first; medicines tailored to needs.
- Standard: Use calculators and tools; know treatment options.
- Clinical: Follow updated guidelines and evidence tiers.
For deeper learning, explore our Health Tips hub. Remember, managing PCOS proactively improves long-term health and quality of life.
Frequently Asked Questions About PCOS Symptoms
1. What are the most common early signs of PCOS in women?
Irregular periods, excess facial/body hair, acne, weight gain struggles, fertility issues, fatigue, and dark skin patches often cluster early.
2. How is PCOS diagnosed?
Doctors use Rotterdam criteria: 2 of 3 features (irregular ovulation, high androgens, polycystic ovaries) after ruling out mimics like thyroid disease via history, labs, and ultrasound.
3. Can PCOS be cured?
No cure exists, but symptoms improve with lifestyle changes, medications, and monitoring—many women manage it effectively long-term.
4. Can women with PCOS get pregnant?
Yes, most can with lifestyle tweaks or ovulation induction like letrozole; success rates exceed 70% in early treatment.
5. Do I need birth control pills if I have PCOS?
Pills regulate cycles, reduce hair/acne, and protect the endometrium if not trying to conceive; alternatives exist for fertility goals.
6. Does PCOS always cause weight gain or obesity?
No, but insulin resistance drives central weight gain in 50-70%; lean PCOS occurs in 20-30%, especially in Asian populations.
7. What lifestyle changes help manage PCOS symptoms?
5-10% weight loss via balanced macros, exercise, and sleep restores ovulation in 30-50%; track with Macro Calculator.
8. How does PCOS affect mental health?
Anxiety/depression risk doubles due to hormones, body image, and fatigue; screening and therapy improve outcomes.
9. When should I see a doctor for possible PCOS?
If 3+ symptoms (irregular cycles, hair growth, acne) persist 3-6 months, or fertility delays occur—use Symptom Checker to log.
10. What are long-term risks of untreated PCOS?
Type 2 diabetes (4-7x risk), heart disease, endometrial cancer; early management cuts risks by 50% per NIH data.
11. Can diet alone reverse PCOS symptoms?
Diet aids insulin control and ovulation but works best with exercise/meds; low-GI plans help 40-60%—plan via Keto Calculator.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Obstetrics & Gynecology (2003); Reproductive Endocrinology (2008) Experience: 22 years | Location: Pune, India Education: MBBS, Armed Forces Medical College (2000); MD OB-GYN, All India Institute…

Board Certifications: Internal Medicine (1998); Endocrinology, Diabetes & Metabolism (2001) Experience: 27 years | Location: Chennai, India Education: MBBS, Madras Medical College (1995); MD Internal Medicine, CMC Vellore…

Board Certifications: Registered Dietitian Nutritionist (RDN, 2009); Certified Specialist in Obesity and Weight Management (2013) Experience: 16 years | Location: Ahmedabad, India Education: BSc Food & Nutrition, MS…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.