Brain Tumor Red Flags: 7 Signs Doctors Mistake for Common Conditions
Sarah Martinez, a 42-year-old marketing executive from Chicago, visited her doctor six times over 18 months complaining of morning headaches and occasional confusion. Each time, she was reassured it was stress, perimenopause, or tension headaches. By the time an MRI revealed a golf ball-sized brain tumor pressing against her frontal lobe, Sarah had lost precious months of treatment time. Her story isn’t unique—it represents a troubling pattern where brain tumor red flags are dismissed as everyday health complaints.
Brain tumor warning signs often mimic common conditions, leading to dangerous diagnostic delays. The seven most frequently misdiagnosed symptoms include new-pattern headaches (mistaken for migraines), adult-onset seizures (dismissed as fainting), vision changes (blamed on aging eyes), personality shifts (attributed to depression), memory problems (called “stress-related brain fog”), balance issues (misdiagnosed as vertigo), and one-sided weakness (explained as poor posture). According to the National Cancer Institute, approximately 25,000 Americans are diagnosed with malignant brain cancer annually, yet many experience months of misdiagnosis before detection.
Early recognition of brain tumor symptoms dramatically improves outcomes. Research from the University of Pittsburgh Medical Center shows that signs of brain tumor in adults can be subtle initially, progressively worsening as the tumor grows. Understanding which symptoms warrant immediate imaging—rather than reassurance—could mean the difference between treatable early-stage disease and advanced progression. If you’re experiencing persistent neurological changes that don’t respond to standard treatments, using a symptom checker can help document patterns before your doctor visit.
⚠️ Medical Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult qualified healthcare professionals for evaluation of symptoms. If you’re experiencing severe headaches, sudden vision loss, seizures, or altered consciousness, seek emergency medical attention immediately.
7 Brain Tumor Warning Signs Doctors Often Misdiagnose
Understanding the difference between ordinary symptoms and early brain tumor signs can save lives. These seven brain tumor red flags are frequently dismissed because they overlap with benign conditions, leading to diagnostic delays that affect treatment outcomes.
Sign #1: “New Normal” Headaches That Differ From Your Pattern
What Doctors Mistake It For: Migraines, tension headaches, stress-related pain
The Key Difference:
Brain tumor symptoms headache presents with distinct characteristics that separate it from typical headaches. Research from the National Institutes of Health examining 111 brain tumor patients found that only 48% experienced headaches, but when present, they showed specific patterns.
- Morning-dominant pain that wakes you from sleep or occurs immediately upon waking
- Progressive worsening over weeks or months, not episodic like migraines
- Resistance to over-the-counter pain relievers that normally work for you
- Accompanied by projectile vomiting without nausea preceding it
- Worsens with position changes like bending over, coughing, or straining
Why The Confusion Happens: According to Johns Hopkins Medicine research, 77% of brain tumor headaches mimic tension-type patterns, making them easily dismissed. Unlike migraine sufferers who typically have years of headache history, brain tumor first symptoms often include new-onset headaches in people over 40 with no prior headache disorder.
Red Flag Checklist:
- ✓ New headache pattern after age 50
- ✓ Headache severity increases over 2-4 weeks
- ✓ Pain awakens you between 1-5 AM
- ✓ Vomiting provides temporary relief
What This Means For You: If your headache pattern changes significantly or you develop new headaches alongside other neurological symptoms, request brain imaging rather than accepting a migraine diagnosis. Document your symptoms using our sleep calculator to track when headaches disrupt rest patterns.
Sign #2: First-Time Seizures in Adults With No Epilepsy History
What Doctors Mistake It For: Fainting spells, panic attacks, dissociative episodes, medication side effects
The Key Difference:
Adult-onset seizures are one of the most significant warning signs of brain tumor, particularly in individuals over 30. Studies from Duke University Brain Tumor Center show that brain tumor seizures occur in 60-100% of low-grade gliomas and 40-60% of high-grade tumors like glioblastoma.
- Focal seizures affecting one body part (hand twitching, facial movements)
- Temporal lobe seizures causing strange tastes, smells, or déjà vu sensations
- Consciousness alterations without full convulsions (staring spells, confusion)
- Post-seizure confusion lasting 15-30 minutes
Why The Confusion Happens: First seizures in adults are often attributed to stress, sleep deprivation, or undiagnosed epilepsy. Emergency departments frequently discharge patients after a single seizure without brain imaging, particularly if standard blood work and ECG are normal.
Red Flag Checklist:
- ✓ First seizure after age 20 with no family history of epilepsy
- ✓ Seizures affecting only one side of the body
- ✓ Seizure accompanied by severe headache
- ✓ Progressive increase in seizure frequency
What This Means For You: Any new-onset seizure in adulthood warrants immediate MRI evaluation, not just observation. Research from the University of California San Francisco confirms that seizures are often the first symptom leading to brain tumor diagnosis in adults.
Sign #3: Vision Changes Blamed on “Aging Eyes” or Digital Eye Strain
What Doctors Mistake It For: Presbyopia, dry eyes, computer vision syndrome, need for new glasses
The Key Difference:
Brain tumor vision problems differ fundamentally from ordinary age-related changes. While gradual near-vision decline is normal after 40, sudden or progressive vision symptoms warrant neurological investigation.
- Double vision (diplopia) that doesn’t improve by covering one eye
- Peripheral vision loss creating tunnel vision or blind spots
- Blurred vision that new prescriptions don’t correct
- Temporary vision blackouts lasting seconds (greyouts)
- Visual field defects affecting the same side in both eyes
Why The Confusion Happens: Primary care physicians and optometrists often address vision complaints without considering neurological causes. Tumors in the occipital lobe or pressing on optic pathways create specific visual field defects that differ from refractive errors.
Red Flag Checklist:
- ✓ Sudden double vision appearing over days or weeks
- ✓ One-sided vision loss in both eyes simultaneously
- ✓ Vision changes accompanied by morning headaches
- ✓ Difficulty judging distances or depth perception
What This Means For You: Request a comprehensive neurological evaluation if vision changes occur alongside other symptoms. Use our eye exam tool to document vision patterns, and ensure any eye care provider performs visual field testing beyond standard refraction.
Sign #4: Personality Changes Misdiagnosed as Depression or Anxiety
What Doctors Mistake It For: Major depression, anxiety disorders, bipolar disorder, stress-related mood changes
The Key Difference:
Frontal lobe tumors create distinctive personality alterations that differ from primary psychiatric conditions. Signs of brain tumor in adults often include behavioral changes that family members notice before the patient recognizes them.
- Apathy and decreased motivation without sadness
- Disinhibition leading to inappropriate social behavior
- Irritability and aggression uncharacteristic of baseline personality
- Emotional lability with rapid mood swings
- Loss of empathy and emotional responsiveness
Why The Confusion Happens: Mental health professionals may treat personality changes with antidepressants or mood stabilizers without considering organic brain pathology. Unlike depression, which typically includes pervasive sadness, brain tumor personality changes often manifest as apathy or inappropriate behavior without mood component.
Red Flag Checklist:
- ✓ Personality change occurring over weeks in someone over 40
- ✓ Behavioral shifts accompanied by headaches or cognitive changes
- ✓ No response to psychiatric medications after 6-8 weeks
- ✓ Family reports “not acting like themselves”
What This Means For You: Advocate for brain imaging before accepting long-term psychiatric treatment when personality changes emerge suddenly in midlife or later, particularly if accompanied by other neurological symptoms.
Sign #5: Memory Problems and Confusion Dismissed as Stress or “Brain Fog”
What Doctors Mistake It For: Age-related memory decline, stress-induced cognitive impairment, early dementia
The Key Difference:
Brain tumor early symptoms affecting cognition differ from normal memory lapses or dementia progression. According to University of Rochester Medical Center, memory problems from brain tumors typically progress over weeks to months, not years.
- Short-term memory loss affecting recent conversations or events
- Difficulty concentrating on previously manageable tasks
- Confusion about time, place, or people occurring episodically
- Word-finding difficulties and speech hesitations
- Executive function impairment affecting planning and organization
Why The Confusion Happens: Cognitive complaints in working adults are frequently attributed to multitasking, poor sleep, or perimenopause. Brain tumor symptoms in women are particularly likely to be misattributed to hormonal changes between ages 40-55.
Red Flag Checklist:
- ✓ Memory decline noticeable over 4-12 weeks
- ✓ Cognitive changes accompanied by headaches
- ✓ Confusion episodes with no clear trigger
- ✓ Difficulty with familiar tasks or routes
What This Means For You: Track cognitive changes systematically before appointments. Memory problems that worsen progressively over weeks—not years—require neuroimaging evaluation, not reassurance about “normal aging.”
Sign #6: Balance Problems and Dizziness Attributed to Inner Ear Issues
What Doctors Mistake It For: Benign paroxysmal positional vertigo (BPPV), vestibular neuritis, Ménière’s disease
The Key Difference:
Cerebellar and brainstem tumors create balance disturbances distinct from inner ear disorders. Brain tumor symptoms weakness often includes coordination problems that worsen over time.
- Unsteady gait requiring wall support or furniture stabilization
- Coordination loss affecting fine motor skills (buttoning shirts, writing)
- Clumsiness with frequent dropping of objects
- Non-spinning dizziness (imbalance rather than room spinning)
- Falls occurring without loss of consciousness
Why The Confusion Happens: ENT specialists treat dizziness with vestibular rehabilitation or medication trials before considering central nervous system causes. True vertigo (spinning sensation) suggests inner ear pathology, while imbalance without spinning indicates potential brain involvement.
Red Flag Checklist:
- ✓ Balance problems worsening over weeks
- ✓ Coordination issues affecting one side preferentially
- ✓ Dizziness accompanied by headaches or vision changes
- ✓ No improvement with vestibular therapy
What This Means For You: Request brain MRI if balance problems persist despite ear-focused treatments, especially when accompanied by other neurological symptoms. Balance issues related to brain tumors typically progress steadily rather than occurring in episodes.
Sign #7: One-Sided Weakness Blamed on Pinched Nerves or Poor Posture
What Doctors Mistake It For: Cervical radiculopathy, carpal tunnel syndrome, rotator cuff injury, sciatica
The Key Difference:
Malignant brain tumor signs and benign brain tumor symptoms both can cause focal weakness that differs from peripheral nerve compression. Brain-related weakness affects entire limbs or body sides, not specific nerve distributions.
- Hemiparesis affecting arm and leg on the same side
- Facial drooping on one side with limb weakness
- Numbness and tingling in entire left or right body half
- Grip strength loss without pain
- Foot drop or leg dragging while walking
Why The Confusion Happens: Orthopedic and spine specialists may focus on structural explanations for weakness, ordering spine imaging instead of brain MRI. Similar to how lung cancer symptoms can mimic respiratory infections, brain tumor weakness is often attributed to musculoskeletal causes.
Red Flag Checklist:
- ✓ Weakness affecting entire side of body simultaneously
- ✓ Progressive strength loss over days to weeks
- ✓ Weakness accompanied by facial drooping or speech changes
- ✓ No pain with the weakness
What This Means For You: One-sided weakness warrants emergency evaluation to rule out stroke, but if stroke is excluded, brain tumor must be considered. Document strength changes systematically and insist on comprehensive neurological examination.
| Symptom | Brain Tumor Presentation | Commonly Mistaken For | Key Distinguishing Feature |
|---|---|---|---|
| Headache | Morning-dominant, progressive worsening | Migraine, tension headache | Wakes from sleep, projectile vomiting |
| Seizure | Adult-onset, focal or generalized | Fainting, panic attack | First occurrence after age 20 |
| Vision | Double vision, field defects | Aging eyes, eye strain | Not corrected by new glasses |
| Personality | Apathy, disinhibition | Depression, anxiety | No sadness, behavioral not emotional |
| Memory | Rapid decline over weeks | Stress, early dementia | Progressive over weeks, not years |
| Balance | Non-spinning imbalance | BPPV, inner ear disorder | No spinning vertigo sensation |
| Weakness | Entire side affected | Pinched nerve | Arm and leg same side, no pain |
How Brain Tumor Symptoms Vary by Gender, Age, and Location
Brain tumor symptoms don’t present uniformly across all patients. Understanding how brain cancer symptoms differ based on gender, age, and tumor location helps explain why diagnosis is often delayed and why certain populations face higher misdiagnosis rates.
Gender-Specific Symptom Patterns
Brain Tumor Symptoms in Women
Female patients face unique diagnostic challenges when recognizing signs of brain tumor in adults. Research from the National Cancer Institute reveals that while males develop malignant brain tumors at higher rates, women’s symptoms are more frequently dismissed as hormonal fluctuations.
Brain tumor symptoms in women between ages 40-55 often overlap with perimenopause presentations, leading physicians to attribute cognitive changes, mood swings, and fatigue to hormonal shifts rather than neurological pathology. Women report longer times to diagnosis partly because headaches, memory problems, and emotional changes are normalized as “stress” or “hormonal imbalance.” Additionally, women with brain tumor warning signs may delay seeking care due to caregiving responsibilities and tendency to minimize their own symptoms.
Brain Tumor Symptoms in Men
Males experience higher incidence rates of malignant brain tumor signs across all age groups, including childhood. According to NIH-funded research, sex-based biological differences influence both tumor development and symptom progression.
Brain tumor symptoms in men are more likely to include aggressive behavioral changes and seizures as presenting symptoms. Men also demonstrate different symptom reporting patterns—they’re less likely to mention cognitive or emotional changes initially, instead focusing on physical symptoms like headaches or weakness. This reporting bias can delay recognition of frontal lobe tumors that primarily affect personality and executive function.
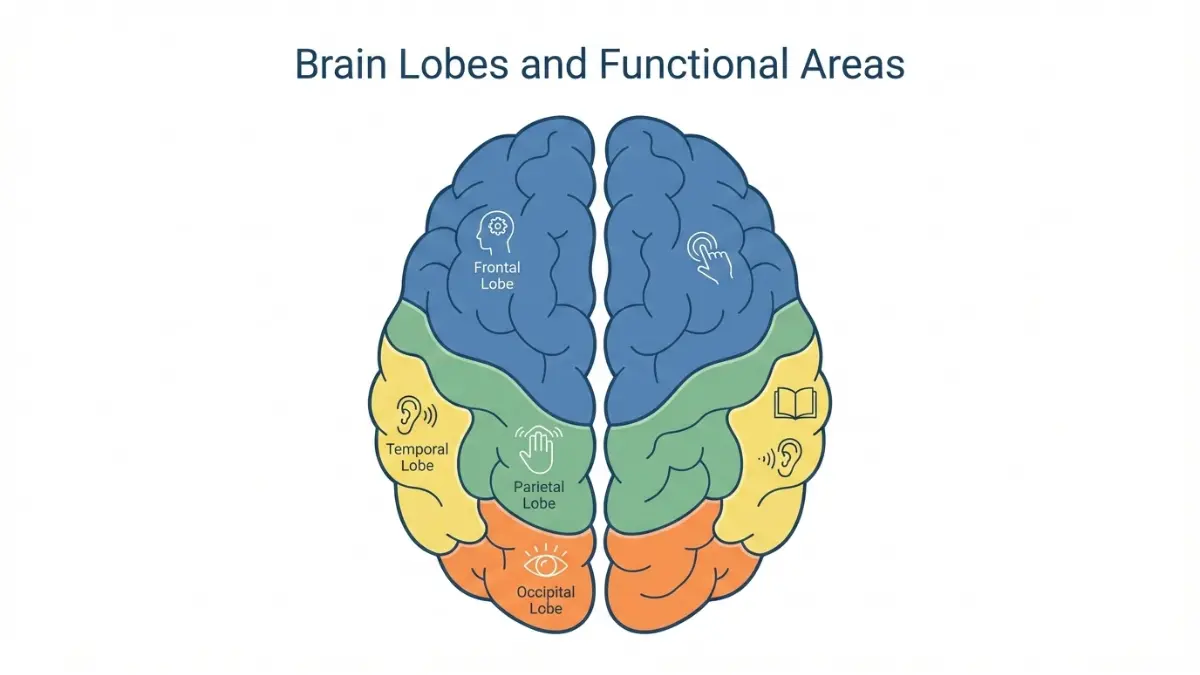
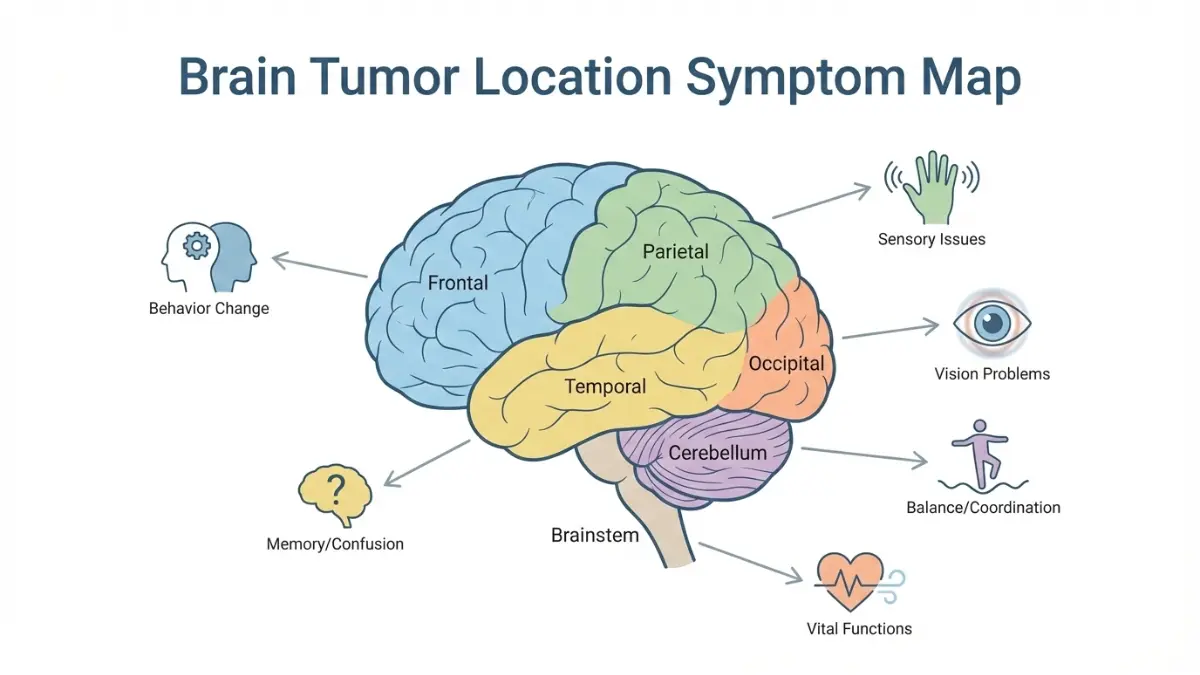
Symptoms Based on Tumor Location
Brain tumor symptoms by location follow predictable patterns based on which brain regions are affected. Understanding these patterns helps differentiate benign brain tumor symptoms from malignant presentations and explains why doctors might initially mistake neurological symptoms for other conditions.
| Brain Region | Functions Controlled | Specific Symptoms | Often Mistaken For |
|---|---|---|---|
| Frontal Lobe | Personality, judgment, movement | Personality changes, speech difficulty, weakness on one side | Depression, psychiatric disorder, stroke |
| Parietal Lobe | Sensation, spatial awareness | Numbness, difficulty with spatial tasks, reading/writing problems | Peripheral neuropathy, vision problems |
| Temporal Lobe | Memory, hearing, language | Memory loss, hearing changes, seizures with strange sensations | Alzheimer’s, anxiety, ear problems |
| Occipital Lobe | Vision processing | Vision loss, visual hallucinations, reading difficulty | Eye disease, migraine aura, optical nerve issues |
| Cerebellum | Balance, coordination | Unsteady gait, fine motor problems, dizziness | Inner ear disorder, vertigo, vitamin D deficiency |
| Brainstem | Vital functions, cranial nerves | Swallowing difficulty, facial weakness, breathing problems | Bell’s palsy, stroke, ALS |
Research from Duke University Brain Tumor Center emphasizes that left-brain versus right-brain tumor location creates distinctly different symptom profiles. Left-hemisphere tumors typically cause language and analytical thinking problems, while right-hemisphere tumors affect spatial processing and creative functions.
Age-Related Presentation Differences
Early brain tumor symptoms manifest differently across age groups. Adults over 50 with new-onset seizures have significantly higher probability of brain tumor than younger adults with the same symptom. Conversely, headache as a presenting symptom is more common in younger adults and children, though it’s also more likely to be dismissed as benign in these populations.
Understanding your personal risk factors through tools like our genetic risk assessment can help contextualize symptom significance, particularly if you have family history of brain tumors or previous radiation exposure.
When To Demand Immediate Medical Attention
Emergency Brain Tumor Symptoms: When 24-Hour Delay Could Be Dangerous
Recognizing the difference between symptoms requiring immediate emergency care versus scheduled medical evaluation can be life-saving. Understanding how to know if you have a brain tumor means knowing when to act urgently versus when to document symptoms for scheduled appointments.

Symptoms Requiring Emergency Room Visit
Research from the National Institutes of Health examining 205 brain tumor patients first diagnosed in emergency departments found that 59.5% presented with focal neurological signs, 24.9% with altered mental status, and 14.6% with severe headache. These presentations warrant immediate evaluation.
Seek emergency care immediately for:
- “Thunderclap” headache – sudden, severe headache reaching maximum intensity within seconds to minutes
- First-time seizure at any age, especially if accompanied by confusion lasting more than 15 minutes
- Sudden vision loss in one or both eyes, or new-onset double vision
- Severe confusion or disorientation – not recognizing familiar people or places
- Loss of consciousness or fainting episodes with no clear cause
- Projectile vomiting with severe headache and no stomach illness
- Sudden weakness or numbness on one side of the body resembling stroke symptoms
- Difficulty speaking or understanding speech that appears suddenly
- Severe balance problems preventing walking without support
What This Means For You: Similar to recognizing heart attack warning signs, emergency brain tumor red flags require immediate imaging. Emergency departments can perform rapid CT scans within minutes and arrange urgent MRI if needed. Don’t wait for morning or for symptoms to worsen—these presentations indicate potential increased intracranial pressure or hemorrhage.
Symptoms Requiring Doctor Visit Within 48-72 Hours
Not all warning signs of brain tumor constitute emergencies, but progressive or persistent symptoms require prompt scheduled evaluation. According to MedlinePlus, certain symptom patterns signal the need for neurological assessment within days.
Schedule urgent appointments for:
- Progressive morning headaches that worsen over 2-4 weeks
- Personality or mood changes noticed by family members over recent weeks
- Memory decline affecting work performance or daily activities
- Gradual vision changes not explained by new glasses prescription
- Persistent nausea especially if worse in mornings
- Coordination problems developing over weeks
- Hearing changes in one ear with no infection
- Unexplained fatigue despite adequate sleep patterns
Use our symptom checker to document symptom patterns systematically before your appointment, including frequency, timing, severity, and any triggering factors.
How to Advocate for Yourself
Many patients experiencing brain tumor diagnosis symptoms face initial dismissal before receiving proper imaging. Armed with specific language and questions, you can advocate effectively for appropriate evaluation.
What to say to your doctor:
- “These symptoms are new and progressively worsening, not episodic like my usual [condition]”
- “I’ve documented these symptoms over [timeframe] and they’re not responding to [previous treatments]”
- “Given my age and symptom pattern, I’d like to rule out serious neurological causes before assuming this is benign”
- “What specific findings would prompt you to order brain imaging?”
Questions to ask:
- “What are we looking for with conservative treatment, and what would indicate it’s not working?”
- “How long should I wait before returning if symptoms don’t improve?”
- “If this were your family member with these symptoms, what would you recommend?”
- “Can you document in my chart that I requested imaging and your clinical reasoning for deferring it?”
When to request imaging: Adults over 40 with new-onset headaches, anyone with first-time seizures, progressive neurological symptoms lasting more than 2-4 weeks, or symptoms that don’t match typical patterns for diagnosed conditions warrant MRI evaluation. CT scans miss some brain tumors, so specifically request MRI with and without contrast when possible.
Second opinion guidance: If your symptoms persist despite treatment or your concerns are dismissed without thorough neurological examination, seek evaluation from a neurologist rather than continuing with primary care alone. Just as cancer symptoms across various types require specialized evaluation, brain cancer symptoms warrant specialist assessment.
| Urgency Level | Symptoms | Action Timeframe |
|---|---|---|
| Emergency (ER) | Thunderclap headache, first seizure, sudden weakness, altered consciousness, sudden vision loss | Within 1-2 hours |
| Urgent (Doctor Visit) | Progressive headaches, personality changes, persistent vomiting, gradual weakness | Within 24-72 hours |
| Scheduled (Specialist) | Persistent symptoms after 4-6 weeks treatment, symptoms not matching diagnosis | Within 1-2 weeks |
| Monitor & Document | Intermittent mild headaches, occasional memory lapses (without progression) | Track and reassess in 2-4 weeks |
Diagnosis, Testing & What Comes Next
From Symptoms to Diagnosis: Understanding Brain Tumor Detection
Once brain tumor red flags prompt medical evaluation, understanding the diagnostic pathway helps patients navigate what can feel like an overwhelming process. Modern neuroimaging and tissue analysis provide detailed information about tumor type, grade, and treatment options.
Diagnostic Process Timeline
The path from initial symptoms to confirmed brain tumor diagnosis symptoms typically follows a structured progression, though timing varies based on symptom severity and healthcare access patterns.
Step 1: Primary Care Evaluation (Week 1)
- Neurological examination assessing reflexes, coordination, vision, and cognitive function
- Documentation of symptom timeline and progression
- Initial differential diagnosis considering non-tumor causes
- Referral to neurology or direct imaging order
Step 2: Neuroimaging (Weeks 1-3)
- MRI with and without contrast remains the gold standard for detecting brain tumor early symptoms
- CT scans may be performed first in emergency settings but can miss smaller lesions
- Advanced MRI sequences identify tumor characteristics and surrounding brain structures
Step 3: Specialist Consultation (Weeks 2-4)
- Neuro-oncologist or neurosurgeon reviews imaging
- Discussion of preliminary findings and next steps
- Biopsy planning if diagnosis unclear from imaging alone
Research from the National Institutes of Health examining diagnostic delays found the median time from first symptom to diagnosis averaged 14 weeks, with significant variation based on initial symptom presentation and whether patients presented to emergency departments versus primary care.
Imaging and Testing Explained
MRI vs. CT Scan: When Each Is Used
Magnetic resonance imaging provides superior detail for brain cancer symptoms assessment compared to computed tomography. According to SEER training modules, MRI can distinguish tumor boundaries, identify multiple lesions, and characterize tissue types without radiation exposure.
MRI advantages:
- Detects tumors as small as 3-5mm
- Shows relationship to critical brain structures
- Multiple sequences (T1, T2, FLAIR, diffusion) reveal different tumor properties
- Contrast enhancement patterns help differentiate tumor types
CT scan limitations:
- May miss low-grade gliomas and posterior fossa tumors
- Less soft tissue detail
- Radiation exposure considerations
- Useful primarily for emergency detection of bleeding or severe swelling
Biopsy Procedures and Tissue Analysis
When imaging cannot definitively determine whether a lesion represents malignant brain tumor signs versus benign brain tumor symptoms, tissue sampling becomes necessary. Stereotactic needle biopsy involves precise computer-guided sampling through small skull openings, while open surgical biopsy occurs during tumor removal procedures.
Pathologists analyze cellular architecture, growth patterns, and molecular markers to establish diagnosis and grade according to World Health Organization classification systems.
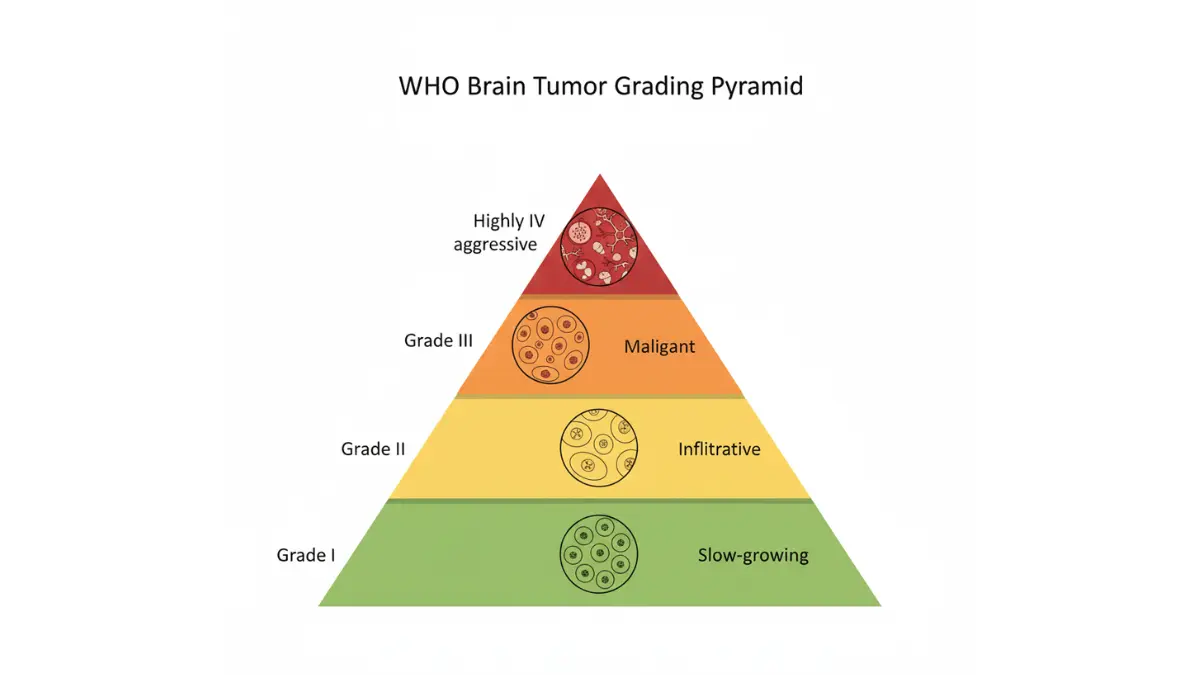
Grading Systems: Understanding Your Results
Brain tumors are classified by cell type (astrocytoma, meningioma, etc.) and WHO grade (I-IV), which indicates biological aggressiveness rather than tumor size.
- Grade I: Slow-growing, well-defined borders, potential for surgical cure
- Grade II: Infiltrative growth, higher recurrence risk, may progress to higher grades
- Grade III: Malignant features including rapid cell division and abnormal nuclei
- Grade IV: Highly aggressive with necrosis and abnormal blood vessel formation (includes glioblastoma)
Benign vs. Malignant Differentiation
The distinction between benign brain tumor symptoms and malignant presentations involves more than growth rate. Benign tumors like meningiomas typically have well-defined borders and don’t invade surrounding tissue, though their location can still cause serious symptoms. Malignant tumors infiltrate adjacent brain tissue, making complete surgical removal challenging.
Latest Research and Expert Consensus
International Perspectives on Early Detection
Neuro-oncology experts worldwide emphasize that earlier detection of warning signs of brain tumor correlates with improved outcomes, particularly for grades II and III tumors where complete resection before progression offers best prognosis.
Dr. Patrick Wen, Director of the Center for Neuro-Oncology at Dana-Farber Cancer Institute, notes that advances in molecular profiling now guide treatment decisions beyond traditional grading systems. Tumors with certain genetic mutations respond differently to therapies regardless of grade.
Emerging Detection Methods (2024-2025 Research)
Recent NIH-funded studies explore blood-based biomarkers for early brain tumor detection, though none are yet clinically validated for screening. Liquid biopsy approaches analyzing circulating tumor DNA show promise but remain investigational.
Advanced MRI techniques including perfusion imaging, spectroscopy, and diffusion tensor imaging provide functional information beyond structural anatomy. These methods help distinguish tumor tissue from treatment effects and identify aggressive tumor regions for targeted biopsy.
Study Limitations and Transparency
Current brain tumor diagnostic research faces limitations including small sample sizes, single-institution studies, and lack of diverse population representation. Most imaging studies are conducted at academic medical centers, potentially limiting generalizability to community settings. Conflict of interest disclosures indicate imaging technology companies frequently sponsor diagnostic research studies.
| Test | Purpose | Timeframe | Strengths | Limitations |
|---|---|---|---|---|
| MRI with contrast | Primary diagnostic imaging | 1-2 weeks | High detail, no radiation | Expensive, requires stillness |
| CT scan | Emergency screening | Same day | Fast, widely available | Misses small tumors, radiation |
| Stereotactic biopsy | Tissue diagnosis | 2-4 weeks | Definitive cell type | Invasive, sampling error risk |
| Molecular testing | Treatment planning | 1-2 weeks | Guides therapy choices | Limited availability, cost |
| Functional MRI | Pre-surgical planning | 1-2 weeks | Maps critical regions | Requires patient cooperation |
Living With Suspicion & Taking Action
What This Means For You: Practical Next Steps
Understanding brain tumor red flags empowers you to act decisively when symptoms warrant attention, while avoiding unnecessary anxiety over benign conditions. Knowledge transforms concern into constructive action.
If You’re Experiencing These Symptoms
Immediate Action Checklist:
- ✓ Document symptom patterns systematically – Note when symptoms occur, their severity (scale 1-10), duration, and any triggers or relieving factors
- ✓ Track temporal relationships – Record whether headaches wake you from sleep, if vision problems worsen throughout the day, or if symptoms progress week-over-week
- ✓ Photograph or video observable symptoms – Document facial asymmetry, gait problems, or coordination difficulties to show healthcare providers
- ✓ Compile your medical history – List current medications, previous diagnoses, family history of neurological conditions or cancer
- ✓ Prepare specific questions – Write down concerns before appointments to ensure nothing gets overlooked during limited consultation time
Symptom Journal Template for Doctor Visits:
Create a structured log including date, time, specific symptom, severity rating, associated symptoms, and impact on daily function. This documentation proves invaluable when brain tumor diagnosis symptoms overlap with common conditions, helping physicians recognize patterns requiring imaging.
Questions to Prepare:
- “Given my symptom pattern, what neurological conditions are you considering?”
- “At what point would brain imaging be warranted?”
- “What specific changes would prompt you to escalate evaluation?”
- “Should I return immediately if symptoms worsen, or wait for scheduled follow-up?”
Lifestyle Factors and Risk Assessment
Risk Factors You Cannot Control
According to research from the National Cancer Institute, the only well-established risk factor for brain tumor development in adults is therapeutic ionizing radiation exposure, particularly childhood radiation for leukemia or previous brain tumors. Age also influences risk, with incidence increasing through the seventh decade for most tumor types.
When Family History Matters:
Most brain tumors occur sporadically without hereditary patterns. However, certain genetic syndromes including neurofibromatosis, Li-Fraumeni syndrome, and tuberous sclerosis increase risk significantly. If you have family history of these conditions or multiple relatives with brain cancer, assessment through our genetic risk calculator can help contextualize your personal risk profile.
Modifiable Factors:
Unlike some cancers where lifestyle modifications reduce risk substantially, primary brain tumor early symptoms cannot be prevented through diet, exercise, or avoiding specific environmental exposures with current scientific evidence. Cell phone use, power line proximity, and dietary nitrates—despite widespread concern—lack convincing epidemiological support as causative factors.
What You Can Control:
- Prompt evaluation of new symptoms prevents diagnostic delays
- Adequate sleep helps distinguish fatigue-related cognitive issues from progressive neurological symptoms
- Stress management reduces symptom misattribution, as anxiety can mimic or amplify warning signs of brain tumor
- Regular health monitoring including tracking changes with tools like our BMI calculator helps establish health baselines
Moving Forward With Confidence
A Story of Early Detection:
Michael Chen, a 52-year-old software engineer, noticed subtle coordination problems while typing over three weeks. Unlike colleagues who dismissed it as “getting older,” Michael documented his symptoms and requested neurological evaluation. MRI revealed a grade II oligodendroglioma. Because detection occurred before significant growth, surgeons achieved complete resection, and Michael returned to work within six weeks. Five years later, he remains tumor-free with quarterly monitoring.
Your Empowerment Plan:
Recognizing signs of brain tumor in adults doesn’t mean living in fear—it means staying informed and acting appropriately when patterns emerge. Most headaches are benign. Most memory lapses reflect normal aging or stress. But progressive, unexplained neurological symptoms deserve thorough evaluation.
Trust your instincts when something feels persistently wrong. Similar to recognizing other cancer warning signs, early detection of brain tumor symptoms offers the best opportunity for favorable outcomes. You know your body better than anyone—advocate assertively when symptoms don’t match reassurances you receive.
Key Takeaways:
- Progressive symptoms matter more than single episodes – Worsening over weeks signals need for imaging
- New symptoms after age 40 warrant closer attention – Adult-onset seizures or headache pattern changes require evaluation
- Combination symptoms raise concern – Headache plus vision changes plus personality shifts demand urgent assessment
- Documentation strengthens your case – Systematic symptom tracking helps physicians recognize patterns
- Second opinions are your right – If concerns are dismissed without examination or testing, seek specialist evaluation
The difference between timely diagnosis and dangerous delay often comes down to patient persistence and informed self-advocacy. Understand the red flags, document changes systematically, and insist on appropriate evaluation when brain tumor warning signs align with your experience.
Frequently Asked Questions About Brain Tumor Warning Signs
1. What are the first warning signs of a brain tumor?
The first warning signs typically include new-pattern headaches (especially morning headaches), personality changes, memory problems, or vision disturbances. Adult-onset seizures and progressive one-sided weakness are also early red flags that doctors often initially misdiagnose.
2. Can you have a brain tumor with no symptoms?
Yes, small benign tumors like meningiomas can remain asymptomatic for years and are sometimes discovered incidentally during imaging for unrelated reasons. However, as tumors grow, they eventually cause symptoms by pressing on brain structures.
3. What does a brain tumor headache feel like?
Brain tumor headaches are typically worse in the morning, wake you from sleep, progressively worsen over weeks, and don’t respond to typical pain relievers. They often occur with projectile vomiting and worsen with position changes like bending over.
4. How long can you have a brain tumor before symptoms show?
Slow-growing benign tumors can exist for months to years before causing noticeable symptoms, while aggressive malignant tumors may produce symptoms within weeks of development. The timeline depends on tumor location, size, and growth rate.
5. Are brain tumor symptoms constant or do they come and go?
Brain tumor symptoms are typically progressive and persistent, worsening over time rather than coming and going episodically. This progressive pattern distinguishes them from migraines or other benign conditions that fluctuate.
6. Can stress cause brain tumor symptoms?
Stress cannot cause brain tumors, but it can produce symptoms that mimic brain tumor warning signs including headaches, memory problems, and difficulty concentrating. However, stress-related symptoms don’t progressively worsen over weeks like tumor symptoms do.
7. At what age are brain tumors most common?
Brain tumors have two peak incidence periods: childhood (ages 3-12) and older adulthood (ages 55-65). However, they can occur at any age, with certain types more common in specific age groups.
8. Can a blood test detect a brain tumor?
No, standard blood tests cannot detect brain tumors. Diagnosis requires neuroimaging (MRI or CT scan) and often tissue biopsy for confirmation. Blood-based biomarkers are under research but not yet clinically available.
9. Do brain tumors show up on CT scans?
CT scans can detect many brain tumors, especially larger ones, but MRI is superior for detecting small tumors and those in certain brain regions. Some low-grade tumors may be missed on CT but visible on MRI.
10. What is the survival rate for brain tumors?
Survival rates vary dramatically by tumor type and grade, ranging from over 90% five-year survival for benign meningiomas to 6-7% for glioblastoma. Early detection, tumor location, patient age, and overall health significantly impact outcomes.
11. Can brain tumors be prevented?
Most brain tumors cannot be prevented as their causes remain largely unknown. The only established preventable risk factor is avoiding unnecessary radiation exposure to the head, particularly in childhood. Lifestyle factors have not been proven to reduce brain tumor risk.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











