
On This Page – Quick Medical Summary
Roman Kingsley, a 57-year-old high school teacher in Ohio, visited his doctor in early 2024 with one complaint: his blood sugar had spiked out of nowhere. He had no family history of diabetes, wasn’t overweight, and had actually been losing weight for months. His doctor treated it as standard new-onset Type 2 diabetes. Nine months later, he was diagnosed with Stage III pancreatic cancer.
His story is not rare. It is the story of pancreatic cancer.
As of January 2026, the 5-year survival rate for pancreatic cancer is 13% — nearly double what it was a decade ago, when it sat at just 6–7%. New mRNA vaccines, AI-powered detection tools, and KRAS-targeted therapies are shifting what is possible. This guide explains everything — clearly, honestly, and with the latest 2026 data.
What Is Pancreatic Cancer? Why Doctors Call It the “Silent” Disease
The Basics: Two Types, Very Different Outcomes
The pancreas is a glandular organ tucked deep behind the stomach. It has two critical jobs: producing digestive enzymes that break down food, and releasing hormones (including insulin and glucagon) that regulate blood sugar.
Pancreatic cancer occurs when abnormal cells in the pancreas grow uncontrolled and form tumors. There are two main types, and their survival rates are dramatically different:
| Feature | Exocrine (PDAC) | Endocrine (NET) |
|---|---|---|
| Frequency | ~90% of all cases | <10% of cases |
| Cell of origin | Enzyme-producing cells | Hormone-producing cells |
| Typical age | 65–74 | Wider age range |
| Aggressiveness | Very high | Generally slower |
| 5-Year Survival | ~10–13% all stages | ~54% overall |
Pancreatic ductal adenocarcinoma (PDAC) is the common, dangerous type. When people say “pancreatic cancer,” they mean PDAC. Pancreatic neuroendocrine tumors (PNETs or NETs) behave very differently and have a far better outlook.
Why Is Pancreatic Cancer So Hard to Catch Early?
The pancreas sits deep in the retroperitoneal space — surrounded by other organs, hidden from easy imaging. It produces no unique, early symptoms that would send a patient to their doctor sooner.
By the time pain, jaundice, or significant weight loss appears, the cancer has typically already grown large or spread. According to the National Cancer Institute, only 14.6% of pancreatic cancers are diagnosed at the localized (early) stage in the United States.
This is why every risk factor, every early warning sign, and every new detection tool in this guide matters enormously.
If you have a family history of cancer or inherited gene mutations (BRCA1, BRCA2, PALB2), use our free Genetic Risk Assessment Tool to evaluate your inherited cancer risk profile before your next appointment.
💡 What This Means For You: Pancreatic cancer is not caught late because of poor medical care. It is caught late because it is biologically silent until it is already serious. The sections below are designed to help you identify the subtle signals before they become obvious ones.
7 Warning Signs of Pancreatic Cancer That Are Easy to Dismiss
Why Symptoms Get Missed
One of pancreatic cancer’s most dangerous traits is that its early symptoms mimic dozens of common, non-serious conditions. Patients and doctors both may attribute these signs to IBS, gallstones, or acid reflux — and lose precious time.
The American Cancer Society notes that early pancreatic cancers often cause no signs or symptoms at all. By the time symptoms are noticeable, the tumor has usually grown large or spread outside the pancreas.
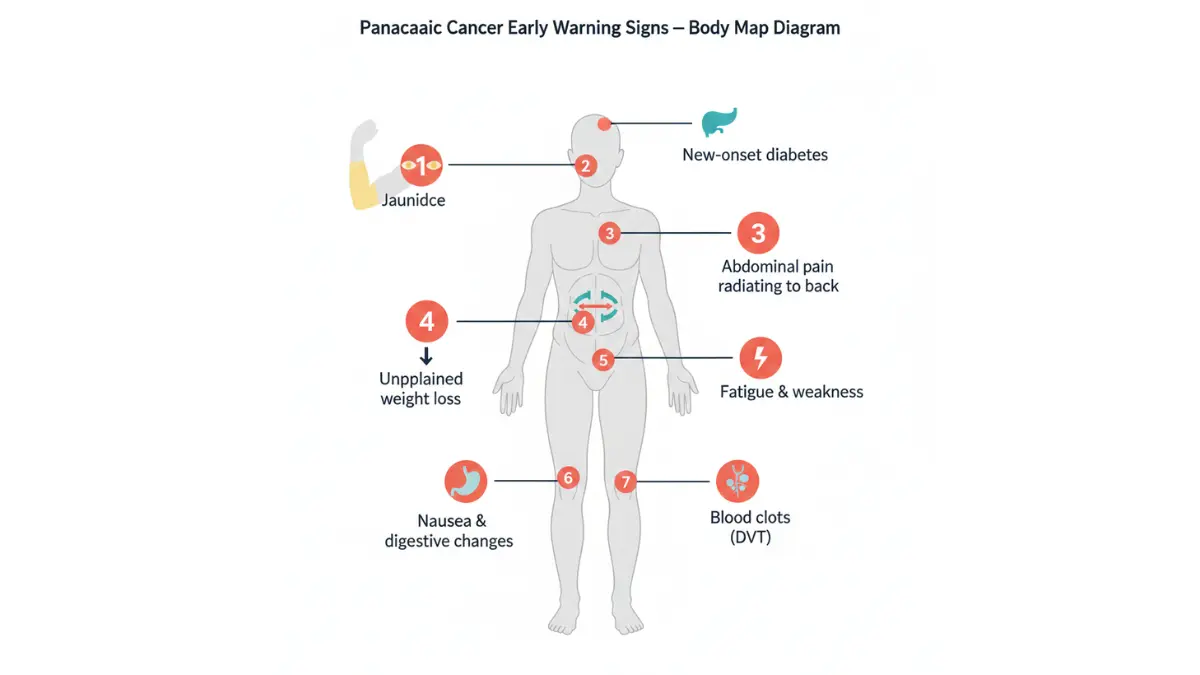
Here are the 7 warning signs — and why each one gets dismissed:
1. Jaundice (Yellowing of Eyes and Skin) Bilirubin builds up when a tumor in the head of the pancreas blocks the bile duct. It turns eyes and skin yellow, darkens urine to a brown color, and turns stools pale or gray. It is the earliest symptom in tumors located in the pancreatic head — but is often misattributed to hepatitis or gallstones.
2. New-Onset Diabetes After Age 50 — The Red Flag Doctors Are Now Watching This is the most underreported early warning sign in 2026. Research shows that people over 50 who develop sudden-onset diabetes — especially with weight loss and no typical Type 2 risk factors — have an eightfold higher risk of pancreatic cancer compared to the general population. Blood sugar abnormalities can appear 1–3 years before the tumor is formally diagnosed. The National Cancer Institute’s Cancer Currents Blog describes this window as a “critical opportunity” for earlier detection. If your blood sugar has recently changed, use our Blood Sugar Converter to track and document your readings before your next medical appointment.
3. Upper Abdominal Pain That Radiates to the Back A dull ache that begins in the upper abdomen and moves around to the mid-back is a classic pancreatic cancer symptom. It worsens after eating and may ease slightly when leaning forward. It is routinely dismissed as a muscle strain or herniated disc.
4. Unexplained Weight Loss Losing 10+ pounds without changing diet or exercise habits is a serious red flag. In pancreatic cancer, the tumor interferes with digestion and nutrient absorption, causing rapid, unintended weight loss. Unlike Type 2 diabetes, which typically involves weight gain, pancreatic cancer-associated diabetes involves weight loss — a key distinguishing feature.
5. Fatigue and Persistent Weakness Fatigue in pancreatic cancer is not ordinary tiredness. It is a disproportionate, persistent exhaustion unrelated to activity levels. Most patients dismiss this for months.
6. Nausea, Loss of Appetite, and Digestive Changes When the tumor obstructs the pancreatic duct, it prevents digestive enzymes from reaching the small intestine. This causes bloating, nausea, greasy or floating stools, and loss of appetite. These symptoms mirror IBS and are frequently not investigated further.
7. Blood Clots (Deep Vein Thrombosis) Pancreatic cancer increases the risk of blood clots in the legs (DVT) or lungs (pulmonary embolism). If you develop unexplained swelling, redness, and warmth in one leg — especially alongside any of the above symptoms — this combination warrants urgent evaluation. See our guide on blood clot symptoms and causes for more detail.
Symptom Comparison Table: Pancreatic Cancer vs. Common Mimics
| Symptom | Pancreatic Cancer | Gallstones | Type 2 Diabetes | IBS |
|---|---|---|---|---|
| Jaundice | ✅ Common (head tumors) | ✅ Possible | ❌ | ❌ |
| New-onset diabetes | ✅ Key red flag | ❌ | ✅ | ❌ |
| Weight loss (rapid) | ✅ Significant | Rare | ❌ (gain) | Mild |
| Back pain + abdominal | ✅ | ✅ | ❌ | ✅ |
| Pale stools + dark urine | ✅ | ✅ | ❌ | ❌ |
⚠️ Warning: If you have 3 or more of these symptoms simultaneously — especially new-onset diabetes with weight loss after age 50 — that combination warrants medical investigation, not reassurance. Use our Symptom Checker to document your symptoms clearly before your appointment.
Pancreatic Cancer Survival Rates 2026 — The Real Numbers
What “5-Year Survival Rate” Actually Means
A 5-year relative survival rate compares people with pancreatic cancer to people of the same age in the general population. If the rate is 43%, it means those patients are 43% as likely to be alive at 5 years compared to someone without cancer.
These numbers do NOT predict individual outcomes. They are population-level averages based on patients diagnosed 5+ years ago — before many of today’s treatments existed.
The 2026 Survival Data (Updated: January 2026)
Overall 5-year survival rate for pancreatic cancer: 13%
This figure, confirmed by the American Cancer Society’s Cancer Facts & Figures 2026, represents a near-doubling from the 7% rate seen just a decade ago. It is a meaningful sign of progress — driven by better imaging, improved chemotherapy combinations, and centralized surgical care.
Pancreatic Cancer Survival Rates by Stage (NCI SEER Data, 2026)
| Stage | Description | 5-Year Relative Survival |
|---|---|---|
| Localized (Stage I–II) | Confined to pancreas | ~43.6% |
| Regional (Stage III) | Spread to nearby lymph nodes or tissue | ~15.3% |
| Distant (Stage IV) | Spread to liver, lungs, or distant organs | ~3.2% |
| All Stages Combined | — | 13% |
| Neuroendocrine Tumors (NET) | Rare type, slower growing | ~54% |
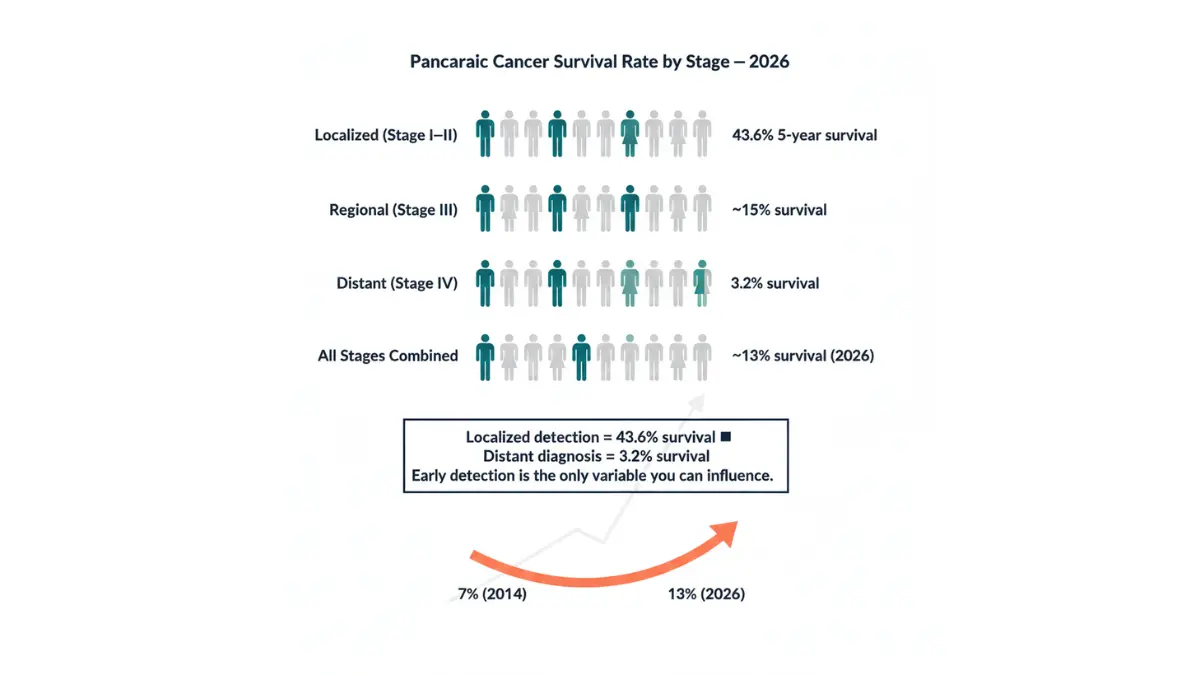
According to the NCI SEER Cancer Statistics database, only 14.6% of patients are diagnosed at the localized stage — yet that early group has a 43.6% survival rate. The survival difference between Stage I and Stage IV is more than 40 percentage points.
Why These Numbers Are Already Outdated — In a Good Way
These statistics are based on patients diagnosed in 2015–2021, before:
- mRNA personalized vaccines entered Phase 2 trials
- KRAS inhibitors received FDA Breakthrough Therapy Designation
- AI-powered early detection tools achieved 99.6% accuracy
- The Mayo Clinic’s chemo-first protocol was published (February 2026)
Today’s newly diagnosed patients are entering a treatment landscape that the survival statistics above do not yet capture.
💡 What This Means For You: If you or a loved one has just been diagnosed, the survival rates you read online are not your future. They are a picture of the past. New treatments discussed in Section 5 are changing these numbers in real time. Also see our related guide on sarcoma cancer survival and detection for comparison with other rare cancer types.
How Pancreatic Cancer Is Diagnosed — 2026’s New Detection Tools
The Standard Diagnostic Pathway
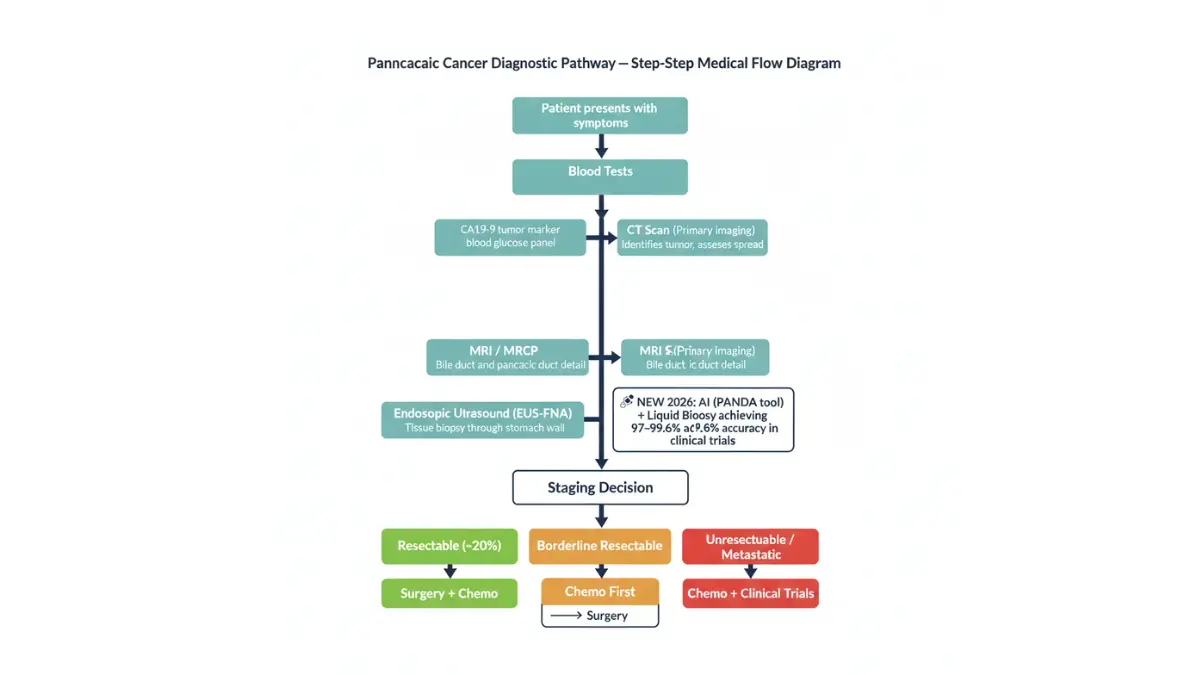
When a patient presents with symptoms or risk factors, the diagnostic workup typically follows this sequence:
- Blood tests — CA19-9 (tumor marker) + standard panel including blood sugar levels
- CT scan — First-line imaging to detect tumors, assess spread, determine resectability
- MRI / MRCP — Additional detail on bile/pancreatic ducts
- Endoscopic Ultrasound (EUS-FNA) — Ultrasound through the stomach wall; allows direct biopsy
- Staging — Tumor classified as localized, regional, or distant; surgical suitability assessed
Key Term: Resectable vs. Unresectable
This is the most important surgical distinction in pancreatic cancer:
| Classification | What It Means | Treatment Path |
|---|---|---|
| Resectable | Tumor can be surgically removed (~20% of patients) | Surgery → Chemotherapy |
| Borderline Resectable | Tumor contacts major blood vessels; surgery possible with preparation | Chemo first → Surgery |
| Locally Advanced (Unresectable) | Tumor has invaded major vessels; surgery not possible | Chemo + Radiation |
| Metastatic | Spread to liver, lungs, or distant organs | Chemotherapy, clinical trials |
The 2026 Diagnostic Breakthroughs No Competitor Is Reporting
New Blood Test: 97% Accuracy for Early-Stage Detection
A 2025 study involving nearly 1,000 participants found that combining a liquid biopsy (detecting circulating tumor DNA in blood) with the CA19-9 tumor marker test identified early-stage pancreatic cancer with 97% accuracy. This combination test is advancing toward clinical use and could soon be incorporated into routine screening for high-risk individuals.
PANDA AI Tool: Outperforming Human Radiologists
Researchers developed an AI system called PANDA (Pancreatic Cancer Detection with Artificial Intelligence) that analyzes standard, non-contrast CT scans. Trained on over 3,000 patients and validated across 10 medical centers with 6,000+ patients, PANDA achieved an AUC of 98.6–99.6% — significantly outperforming average radiologists in both sensitivity and specificity for detecting PDAC.
If you are at elevated risk, ask your oncologist about clinical trials for these emerging detection tools via the NCI’s clinical trials database for pancreatic cancer treatment.
💡 What This Means For You: These new detection tools are NOT yet standard care nationwide. But if you are at high risk — family history, BRCA mutation, or new-onset diabetes after 50 — asking your doctor specifically about EUS surveillance or access to liquid biopsy trials could be the decision that saves your life.
Pancreatic Cancer Treatment in 2026 — A New Era
The Standard Foundation: What Still Works
Treatment depends on the stage and the patient’s health. The current standard options include:
Surgery (for ~20% of patients):
- Whipple Procedure (Pancreaticoduodenectomy) — Removes the head of the pancreas, part of the small intestine, the gallbladder, and part of the stomach. Complex, high-risk, but the only potentially curative option.
- Distal Pancreatectomy — Removes the body and tail; used for tumors in those locations.
- Total Pancreatectomy — Full removal; requires lifelong insulin and enzyme replacement.
Chemotherapy Regimens:
- FOLFIRINOX — The most potent first-line regimen for fit patients with metastatic disease; ~11 months median survival
- NALIRIFOX — Newer standard from the NAPOLI-3 trial; modest survival advantage over gemcitabine + nab-paclitaxel
- Gemcitabine + nab-paclitaxel — Standard option, especially for patients who cannot tolerate FOLFIRINOX
Radiation Therapy:
- SBRT (Stereotactic Body Radiation Therapy) — High-precision radiation for locally advanced, unresectable tumors; used to shrink tumors before surgery or manage pain
The 2026 Breakthroughs: What’s Changing Everything
mRNA Cancer Vaccines — The Most Exciting Development in Decades
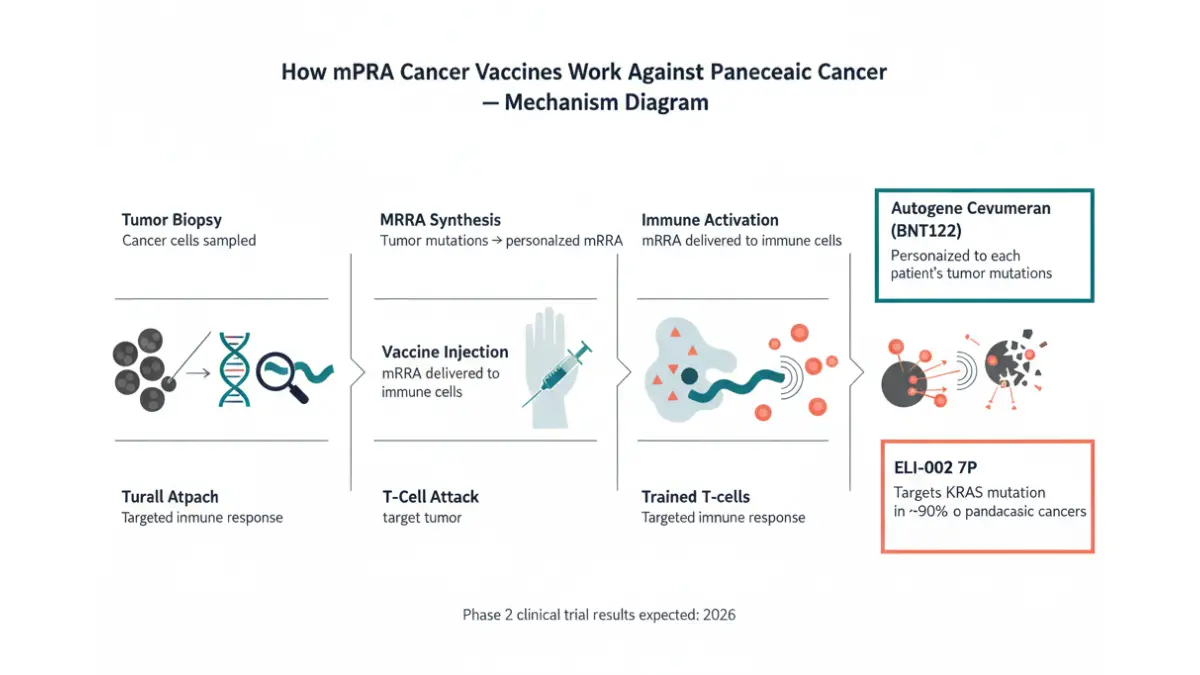
Like the COVID-19 vaccines, mRNA therapeutic cancer vaccines program the immune system to recognize and destroy cancer cells. Unlike COVID vaccines (which prevent infection), these vaccines are given after diagnosis to prevent recurrence or delay progression.
Two approaches are now in active trials:
1. Autogene Cevumeran (BNT122) — Personalized mRNA Vaccine Developed through a BioNTech/Genentech collaboration, this vaccine is custom-made for each patient using the mutational profile of their specific tumor. In a Phase 1 trial at Memorial Sloan Kettering, it stimulated immune responses in 50% of patients with no serious side effects. A Phase 2 randomized trial is now underway. Learn more about the ongoing clinical research at Memorial Sloan Kettering’s mRNA vaccine trial page.
2. ELI-002 2P/7P (KRAS-Targeted “Off-the-Shelf” Vaccine) This vaccine targets mutant KRAS — the gene mutation present in 90% of all pancreatic cancers. In the Phase 1 AMPLIFY-201 trial, patients with robust T-cell immune responses had median relapse-free survival that was not reached (meaning most were still alive and cancer-free at 19.7 months of follow-up) compared to just 3.02 months in patients with weak responses (HR = 0.12, p = 0.0002). The Phase 2 randomized trial completed enrollment; results are expected in 2026.
“What we’re seeing across multiple mRNA vaccine studies is that we are able to engage an immune response, and that does seem to correlate with good outcomes.” — Dr. Zev Wainberg, MD Anderson Cancer Center
KRAS Inhibitors — Targeting the “Undruggable” Gene
For decades, KRAS was considered impossible to block with drugs. That has now changed. New drugs targeting specific KRAS mutations (especially G12D, present in over 40% of PDAC) are now in active clinical development:
- Zoldonrasib (RMC-9805) — FDA granted Breakthrough Therapy Designation in January 2026 for KRAS G12D-mutated cancers
- Phase I trial combining a KRAS vaccine with dual immune checkpoint blockade (published in Nature Communications, 2026) showed increased cytotoxic T-cell infiltration in tumor tissue — the immune system actually reaching and attacking the cancer
The challenge is that PDAC often develops resistance to KRAS inhibitors. Current research at MD Anderson and other centers is focused on combination strategies to overcome this resistance.
The Mayo Clinic February 2026 Paradigm Shift
A major study published in February 2026, conducted across 1,400+ patients at Mayo Clinic’s Minnesota, Arizona, and Florida campuses, found that giving chemotherapy before surgery (neoadjuvant therapy) — even in patients previously classified as candidates for immediate surgery — significantly improved survival outcomes.
This challenges decades of standard practice. The implication: more patients should receive chemotherapy first, regardless of initial staging, to maximize their chance of long-term survival.
“Chemotherapy first, even in cases thought to be more straightforward, provides patients with the best opportunity for long-term survival.” — Dr. Zhi Ven Fong, Surgical Oncologist, Mayo Clinic Arizona (February 2026)
2026 Treatment Overview Table
| Treatment | Who It’s For | 2026 Status |
|---|---|---|
| Whipple Surgery | Resectable (~20%) | Chemo-first protocol now preferred |
| FOLFIRINOX | Metastatic, fit patients | Gold standard first-line |
| NALIRIFOX | Metastatic | New standard option |
| Gemcitabine + nab-paclitaxel | Metastatic, lower fitness | Standard alternative |
| mRNA Vaccine (BNT122) | Post-surgery high-risk | Phase 2 underway |
| ELI-002 7P KRAS Vaccine | KRAS-mutated (90%) | Phase 2 results expected 2026 |
| KRAS Inhibitors (RMC-9805) | KRAS G12D-mutated | FDA BTD granted Jan 2026 |
| Checkpoint Inhibitors | MSI-H tumors (~1–2%) | FDA-approved for this subtype |
💡 What This Means For You: The survival statistics you read online — 13% overall — are based on patients diagnosed before these treatments existed in trials. Today’s newly diagnosed patients are the first generation to access mRNA vaccines, KRAS inhibitors, and AI-guided early detection simultaneously. These numbers will look different in 5 years.
For deeper reading on how cancer treatments compare across types, see our related guides on Stage 1 lung cancer survival, liver cancer first signs and symptoms, and bowel cancer symptoms never to ignore.
Risk Factors, Prevention & 5 Actions to Take Right Now
Who Gets Pancreatic Cancer? The 2026 Risk Profile
Pancreatic cancer cases are rising globally — and a significant part of that rise is linked to modifiable lifestyle factors, particularly in the United States. The obesity epidemic, rising rates of Type 2 diabetes, and an aging population are driving a projected surge toward becoming the second-leading cause of cancer death in the US by 2030.
Pancreatic Cancer Risk Factors
| Modifiable (You Can Change These) | Non-Modifiable (You Cannot Change These) |
|---|---|
| Smoking (2–3× higher risk) | Age 65–74 (peak diagnosis window) |
| Obesity / BMI above 30 | Family history (2+ first-degree relatives) |
| Type 2 diabetes (long-standing) | BRCA1, BRCA2, PALB2 mutations |
| Chronic pancreatitis (often alcohol-related) | Ashkenazi Jewish ancestry |
| Heavy alcohol consumption | Lynch syndrome |
| Sedentary lifestyle | African American or Black ethnicity |
2026 Alert: Rising incidence is increasingly documented in younger adults (under 55) and women — linked to rising obesity rates and metabolic disease, as confirmed by research published in PMC’s 2025 global burden of disease analysis.
If your BMI is above 30, obesity is a clinically recognized independent risk factor for pancreatic cancer. Use our free BMI Calculator to assess where you stand, and our Weight Loss Calculator to set evidence-based targets if reduction is appropriate.
The Obesity–Diabetes–Smoking Triangle
These three modifiable risk factors do not operate in isolation. They create compounding risk:
- Obesity promotes chronic inflammation and insulin resistance
- Insulin resistance leads to high circulating insulin levels, which promote cell growth — including cancer cell growth
- Smoking is the single strongest modifiable risk factor and accounts for approximately 20–25% of all pancreatic cancer cases
- Long-standing Type 2 diabetes (5+ years) doubles the risk of developing pancreatic cancer
The convergence of all three in the same patient creates a risk profile that specialists now flag for closer monitoring.
5 Actions to Take Right Now If You Are At Risk or Recently Diagnosed
1. Request Genetic Testing Immediately If you have two or more first-degree relatives who have had pancreatic cancer, or if you carry BRCA1, BRCA2, or PALB2 mutations, you qualify for high-risk surveillance programs. These programs use EUS and MRI to screen for early-stage disease. Use our Genetic Risk Assessment Tool to document your family cancer history before your appointment.
2. Ask for Clinical Trial Access at Every Decision Point The Pancreatic Cancer Action Network (PanCAN) recommends clinical trial enrollment at diagnosis and at every treatment decision. Many of the most effective emerging therapies — including mRNA vaccines and KRAS inhibitors — are only accessible via trials. Find active trials at the NCI clinical trials database.
3. Seek a High-Volume Pancreatic Cancer Center Research consistently shows that patients treated at hospitals performing high volumes of Whipple procedures and pancreatic cancer surgeries have measurably better outcomes. Do not accept treatment at a low-volume facility without seeking a specialist opinion first.
4. Ask About Biomarker and Genomic Testing Every pancreatic cancer patient should have their tumor genomically profiled. Mutations in BRCA1/2 make patients eligible for PARP inhibitor maintenance therapy (olaparib). Rare NRG1 fusions make patients eligible for zenocutuzumab, an FDA-approved targeted therapy. KRAS G12D mutations may qualify patients for new inhibitor trials.
5. Prioritize Nutritional Support Early Cancer-associated malnutrition (cachexia) affects a majority of pancreatic cancer patients and reduces the ability to tolerate chemotherapy. Early involvement of an oncology-specialized dietitian is not optional — it is a survival variable. Use our Protein Intake Calculator to understand your baseline protein needs during active treatment.
💡 What This Means For You: You cannot reverse a BRCA mutation. But you can quit smoking, reduce obesity risk, manage blood sugar, and ensure you are seen at the right institution by the right specialists. These are not minor decisions — they are the difference between early-stage and late-stage diagnosis.
Frequently Asked Questions About Pancreatic Cancer
Q1: What is the survival rate for pancreatic cancer in 2026?
As of January 2026, the overall 5-year survival rate is 13% — nearly double the rate from a decade ago. When caught at the localized stage, survival climbs to approximately 43.6%.
Q2: What are the very first signs of pancreatic cancer?
The earliest and most frequently missed signs include new-onset diabetes after age 50 (especially with weight loss), subtle upper abdominal discomfort that radiates to the back, and unexplained fatigue. Jaundice is often the first visible sign in tumors in the head of the pancreas.
Q3: Can pancreatic cancer be cured if caught early?
Yes, in some cases. When the tumor is small, localized, and surgically resectable (approximately 20% of diagnoses), surgery followed by chemotherapy offers the possibility of long-term remission. The 5-year survival rate for localized disease is approximately 43.6%.
Q4: Is new-onset diabetes a warning sign of pancreatic cancer?
In some cases, yes. Older adults (50+) with sudden-onset diabetes — particularly without weight gain, typical risk factors, and alongside weight loss — have an eightfold higher risk. This does not mean every new diabetic has cancer, but it warrants careful clinical evaluation including discussion of pancreatic imaging.
Q5: What is the difference between resectable and unresectable pancreatic cancer?
Resectable means the tumor can be surgically removed because it has not invaded major blood vessels — approximately 20% of patients. Unresectable means the tumor cannot be safely removed due to vascular involvement or metastatic spread. Treatment shifts from surgery to chemotherapy and clinical trials.
Q6: How quickly does pancreatic cancer spread?
Pancreatic cancer is one of the most aggressive cancers. PDAC typically spreads to the liver, peritoneum, and lungs. It can progress from a localized to a metastatic stage within weeks to months. This speed is why early detection matters disproportionately more than in many other cancers.
Q7: What is the Whipple procedure?
The Whipple procedure (pancreaticoduodenectomy) is the main surgical option for pancreatic cancer in the head of the pancreas. It removes the head of the pancreas, part of the small intestine, the gallbladder, and the lower portion of the stomach, then reconnects the remaining digestive organs.
Q8: What are the new treatments for pancreatic cancer in 2026?
The most significant 2026 developments include: the ELI-002 KRAS-targeted vaccine (Phase 2 results expected), personalized mRNA vaccines (autogene cevumeran), FDA Breakthrough Therapy Designation for KRAS G12D inhibitor zoldonrasib, and the Mayo Clinic chemo-first surgical protocol published in February 2026.
Q9: What does pancreatic cancer pain feel like?
Most patients describe a persistent, dull ache in the upper abdomen or middle back. It often worsens after eating and may ease slightly when leaning forward or curling into a fetal position. Unlike gallstone pain, it is typically constant rather than colicky.
Q10: What is a KRAS mutation and why does it matter for treatment?
KRAS is a gene that, when mutated, drives uncontrolled cell growth. Over 90% of pancreatic cancers carry a KRAS mutation. For decades this mutation was “undruggable” — but new inhibitors like zoldonrasib and vaccines targeting mutant KRAS are now in active trials, making it the most targeted area of 2026 research.
Q11: Should I get a second opinion for pancreatic cancer?
Yes — always. Pancreatic cancer requires highly specialized surgical, oncological, and supportive care. The difference between a high-volume specialist center and a general hospital can directly impact survival. PanCAN and the NCI both strongly recommend obtaining a specialist opinion, ideally at a comprehensive cancer center.
Summary: Pancreatic cancer remains one of the most challenging diagnoses in oncology — but the landscape in 2026 looks meaningfully different from even five years ago. The 5-year survival rate has nearly doubled to 13%, early warning signs like new-onset diabetes are being taken more seriously, and mRNA vaccines targeting the KRAS mutation that drives 90% of cases are now in Phase 2 trials. The most important thing any patient or family member can do is act quickly, seek specialist care, and ask about clinical trials at every decision point.
📋 Medical Disclaimer: This article is for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a licensed and qualified healthcare professional regarding any medical condition or health concern. The information in this article reflects data available as of February 2026 and is subject to change as new research emerges.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











