
On This Page – Quick Medical Summary
In 2021, two-year-old Gavin Nielsen was diagnosed with DIPG — a brain tumor so aggressive his doctors estimated he had eight to eleven months to live. His mother, Ashlee, remembers saying, “He’s never going to get to go to kindergarten.” Today, in 2026, Gavin is alive and attending school — one of three long-term survivors from a landmark CAR-T clinical trial at Seattle Children’s Hospital.
DIPG (diffuse intrinsic pontine glioma) is one of the most devastating diagnoses in pediatric medicine. But for the first time in four decades, a wave of FDA approvals and clinical breakthroughs is rewriting what is possible for children and families facing this disease.
This guide gives you every critical fact — causes, symptoms, survival data, the first-ever FDA-approved drug, and how to access cutting-edge trials in 2026.
What Is DIPG?
DIPG stands for Diffuse Intrinsic Pontine Glioma — and every word in that name tells you something important about this tumor.
- Diffuse — The cancer cells spread through healthy brain tissue rather than forming a single contained mass. This makes surgical removal impossible.
- Intrinsic — The tumor grows inside the pons, not on its surface.
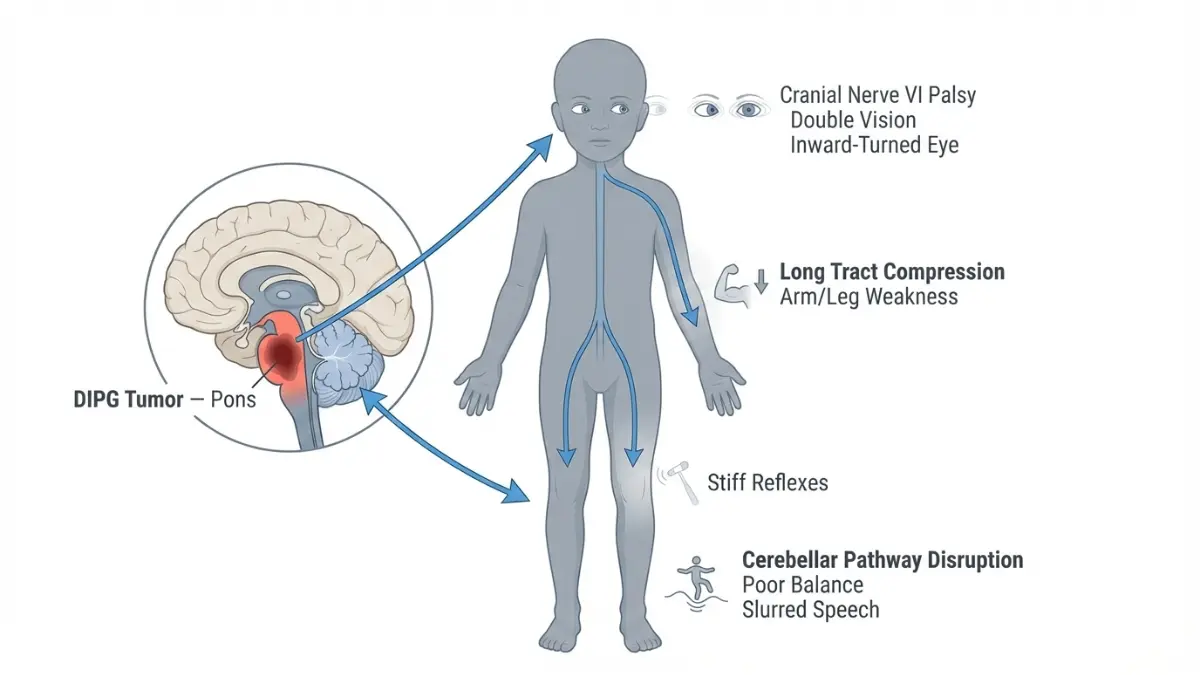
- Pontine — It arises in the pons, the part of the brainstem that controls breathing, heart rate, blood pressure, vision, hearing, and swallowing.
- Glioma — It originates in glial cells, the supportive and protective cells of the central nervous system.
According to the National Cancer Institute, approximately 300 children are diagnosed with DIPG in the United States each year. It primarily affects children aged 5 to 9, affects boys and girls equally, and is rare in adults.
DIPG vs. Diffuse Midline Glioma (DMG) — A Critical Distinction in 2026
In 2021, the World Health Organization (WHO) reclassified DIPG under the broader term Diffuse Midline Glioma (DMG), H3K27M-altered. This is not just a name change — it is clinically significant.
The reclassification directly determines which FDA-approved treatments your child may now qualify for. Modeyso (dordaviprone), approved by the FDA in August 2025, is approved for H3K27M-mutant diffuse midline glioma — meaning families whose children were diagnosed under the older DIPG label still qualify, provided the tumor carries the H3K27M mutation.
💡 Key Takeaway: If your child was diagnosed with DIPG, ask your oncologist whether the tumor was tested for the H3K27M mutation. This single molecular test now determines eligibility for the first-ever FDA-approved systemic drug in the history of this disease.
If your child is showing neurological symptoms and you haven’t received a diagnosis yet, you can use our Symptom Checker as an initial reference before your appointment — though a pediatric neuro-oncologist’s evaluation is always essential.
DIPG Symptoms — Early Warning Signs Parents Must Not Miss
DIPG symptoms typically develop within three to four weeks before diagnosis — faster than almost any other pediatric cancer. Many parents report that their child seemed completely healthy, then deteriorated within a single month.
The Classic DIPG Triad
Doctors recognize a pattern of three symptom clusters that together suggest DIPG. About one in three children shows all three at diagnosis:
| Symptom Cluster | Clinical Term | Plain-Language Description |
|---|---|---|
| Eye movement problems | Cranial nerve palsy (abducens nerve VI) | Eye turns inward, double vision — usually the first sign to appear |
| Arm/leg weakness | Long-tract signs | One-sided limb weakness, exaggerated reflexes |
| Balance problems | Cerebellar dysfunction | Difficulty walking, clumsiness, slurred speech |
Full Symptom Checklist — Signs to Watch For
- Crossed eyes or double vision (diplopia) — often the very first symptom, present before anything else
- Drooping on one side of the face
- Headaches in the morning that improve after vomiting
- Difficulty chewing or swallowing
- Slurred or changed speech
- Weakness in arms or legs
- Stumbling, loss of balance, or difficulty walking
- Drooping eyelid on one side
- Behavioral changes or decline in school performance
⚠️ What Competitors Miss: Most health websites list symptoms as a generic list. What they don’t tell you is that the abducens palsy (inward-turning eye) is present in the vast majority of DIPG cases and appears before other symptoms. If your child’s eye unexpectedly turns inward, this is a medical red flag requiring same-day evaluation — not a “wait and see” situation.
How DIPG Is Diagnosed
DIPG is primarily diagnosed through brain MRI with gadolinium contrast. The tumor has a characteristic appearance on MRI — diffuse infiltration of the pons involving more than 50% of the pontine axial diameter — that allows experienced radiologists to identify it without always requiring a biopsy.
However, a stereotactic biopsy is now increasingly performed, and for good reason: it tests for the H3K27M mutation, which determines eligibility for Modeyso (dordaviprone). The National Cancer Institute provides detailed guidance on diagnostic tests used for DIPG at their dedicated pediatric brain tumor resource.
What Causes DIPG? The H3K27M Mutation Explained
No external cause, no environmental factor, and no inherited gene has been identified as the cause of DIPG. It is not caused by vaccines, diet, radiation exposure, or anything parents did or did not do.
DIPG results from a random mutation during childhood brain development — specifically during the period of rapid cell division in the brainstem between ages five and ten. When cells divide rapidly, errors in replicating genetic material are more likely. In DIPG, these errors alter the histone H3 protein in a way that disrupts normal gene regulation.
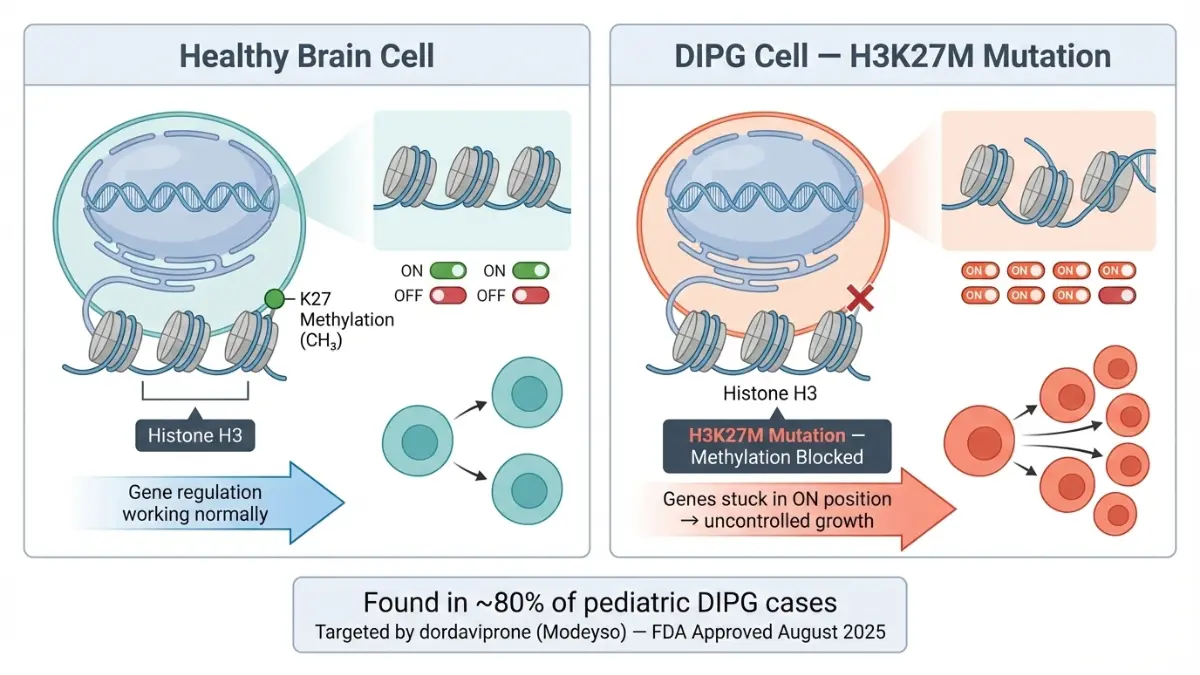
The H3K27M Mutation — Explained Simply
Think of the H3 histone protein as a switch that turns genes on and off. In approximately 80% of pediatric DIPG cases, a mutation called H3K27M permanently disrupts this switch, causing glial cells to divide uncontrollably. This is the biological engine driving tumor growth.
This mutation is now the primary molecular target for new therapies:
- Modeyso (dordaviprone) was specifically designed to reverse the effects of this mutation by restoring normal H3K27 methylation in tumor cells.
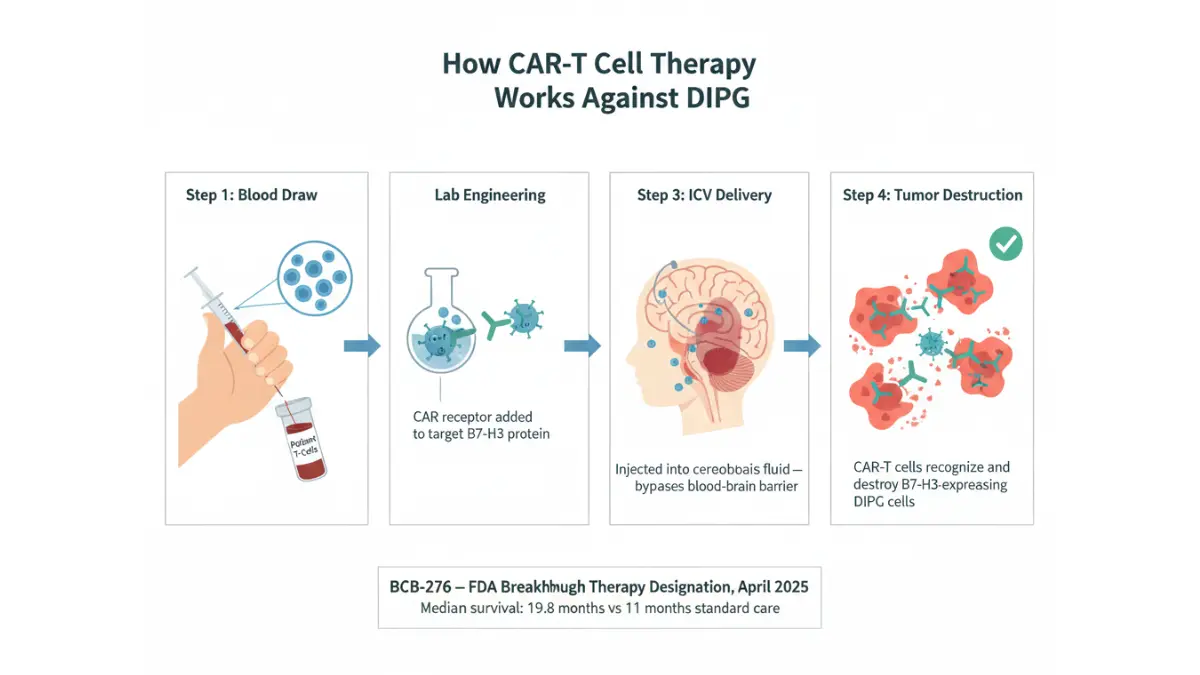
- BCB-276 CAR-T therapy targets B7-H3, a surface protein highly expressed on H3K27M-mutant tumor cells.
💡 H3K27M mutation testing should be requested at diagnosis. It is not automatically performed in all centers. This test is now a clinical necessity, not an optional add-on.
Is DIPG Hereditary?
No. DIPG does not follow an inheritance pattern and has not been linked to any inherited genetic syndrome. Parents of children with DIPG carry no elevated risk of passing the condition to other children. Families interested in understanding broader hereditary cancer risk patterns can explore our Genetic Risk Assessment Tool as a general educational reference — though this is unrelated to DIPG specifically.
DIPG Survival Rates — What the 2026 Data Actually Shows
The median survival for DIPG with standard radiation therapy is 9 to 11 months. This statistic has remained largely unchanged for four decades. It is an honest number — and it is no longer the full story.
2026 Survival Data by Treatment Type
| Treatment | Median Survival | Notable Outcomes |
|---|---|---|
| No treatment | ~6 months | — |
| Radiation therapy (standard) | 9–11 months | Temporary improvement; not curative |
| Dordaviprone/Modeyso (FDA-approved Aug 2025) | ORR 22%, DOR 10.3 months | First systemic drug ever approved; 73% maintained response ≥6 months |
| BCB-276 CAR-T (Phase 1 trial) | 19.8 months from diagnosis | 3 patients alive at 44, 45, and 52 months from diagnosis |
| CED — 124I-Omburtamab (MSK trial) | Multiple 3+ year survivors | One confirmed survivor beyond 10 years |
- Less than 10% of children survive beyond two years with standard treatment
- Five-year survival with standard care: below 1%
- In the BCB-276 CAR-T trial: three children alive past 44 months — outcomes that were not considered achievable five years ago
Factors That Affect DIPG Prognosis
- Presence of the H3K27M mutation (found in ~80% of cases)
- Age at diagnosis — younger children sometimes respond differently
- Speed of symptom onset — slower onset can indicate slightly less aggressive disease
- Access to clinical trials — this is the single most impactful modifiable factor in 2026
💡 “What This Means For You”: Survival statistics represent population averages — not individual destinies. Three children in the BCB-276 trial are alive at over four years. The Modeyso approval means there is now a real, FDA-approved oral drug available for the first time in the history of this disease. Clinical trial enrollment is no longer a last resort — it is a frontline strategy.
For more on how brain tumor diagnoses and reports are interpreted, our guide to reading an MRI report offers additional context for families navigating imaging results.
DIPG Treatment Options — From Radiation to FDA Breakthroughs in 2025–2026
This section contains information that no competitor article fully covers. Two separate FDA designations and one FDA approval occurred between April and August 2025 — and together they represent the most significant advancement in DIPG treatment in forty years.
Standard Treatment: Radiation Therapy
Radiation therapy remains the first-line treatment for all newly diagnosed DIPG patients. It uses high-energy beams to shrink the tumor and temporarily relieve symptoms.
- Works in over 90% of children to improve symptoms temporarily
- Response duration: approximately 6 to 9 months on average
- Not curative — tumor invariably progresses after radiation
- Proton beam radiation is available at some specialized centers and may reduce damage to surrounding healthy brain tissue
- Steroid medication (dexamethasone) is typically given alongside radiation to reduce brain swelling
🔴 EXCLUSIVE: Modeyso (Dordaviprone) — The First FDA-Approved Drug for DIPG/DMG
On August 6, 2025, the FDA granted accelerated approval to dordaviprone (Modeyso) — the first systemic therapy ever approved for H3K27M-mutant diffuse midline glioma. This is a historic milestone that ended a 40-year drought of approved treatments for this disease.
Key facts about Modeyso:
- Approved for: Adults and children aged 1 year and older with H3K27M-mutant DMG (includes DIPG) with progressive disease after prior therapy
- How it works: Modeyso activates the mitochondrial enzyme ClpP, triggering cancer cell death. It also blocks the DRD2 dopamine receptor that promotes tumor growth. Together, these two mechanisms restore normal H3K27 methylation — directly reversing the core molecular defect of DIPG.
- Efficacy: Overall response rate (ORR) of 22% across 50 patients in five clinical trials; median duration of response 10.3 months; 73% of responders maintained response for six months or longer; 27% maintained response for twelve months or longer
- How taken: Oral capsule, once weekly, taken on an empty stomach. Weight-based dosing applies for children.
- Common side effects: Fatigue, headache, nausea/vomiting, and musculoskeletal pain — most were Grade 1 or 2 in severity
- Important note: This is an accelerated approval. Continued approval depends on results from the ongoing Phase 3 ACTION confirmatory trial (NCT05580562)
The American Association for Cancer Research (AACR) confirmed this is the first FDA approval of any targeted therapy for H3K27M-mutant DMG — a disease that previously had no approved drugs of any kind.
💡 “What This Means For You”: If your child’s DIPG has progressed after radiation, and the tumor carries the H3K27M mutation, Modeyso is now an FDA-approved option. Ask your oncologist directly: “Does my child qualify for dordaviprone?”
CAR-T Cell Therapy — BCB-276 Receives FDA Breakthrough Designation (April 2025)
On April 22, 2025, the FDA granted Breakthrough Therapy Designation to BCB-276 — BrainChild Bio’s B7-H3-targeting CAR-T cell therapy — for pediatric DIPG. A second designation, RMAT (Regenerative Medicine Advanced Therapy), followed in May 2025.
What the data shows (Phase 1 BrainChild-03 trial, published in Nature Medicine):
- 21 children and young adults with DIPG received CAR-T infusions directly into the cerebrospinal fluid (intracerebroventricular delivery)
- Median overall survival: 19.8 months from diagnosis — compared to 11 months with radiation alone
- Three patients remain alive at 44, 45, and 52 months from diagnosis — outcomes previously considered impossible
- Treatment was well tolerated even with hundreds of repeated doses over multiple years
- A Phase 2 pivotal trial is planned for enrollment in 2025–2026 to support FDA approval
Meanwhile, researchers at Stanford University demonstrated a separate GD2-targeting CAR-T approach where 9 of 11 patients showed clinical benefit, 4 had tumor volume reduced by over 50%, and 1 patient achieved a complete response. You can read more about related pediatric cancer breakthroughs in our article on neuroblastoma treatments in children.
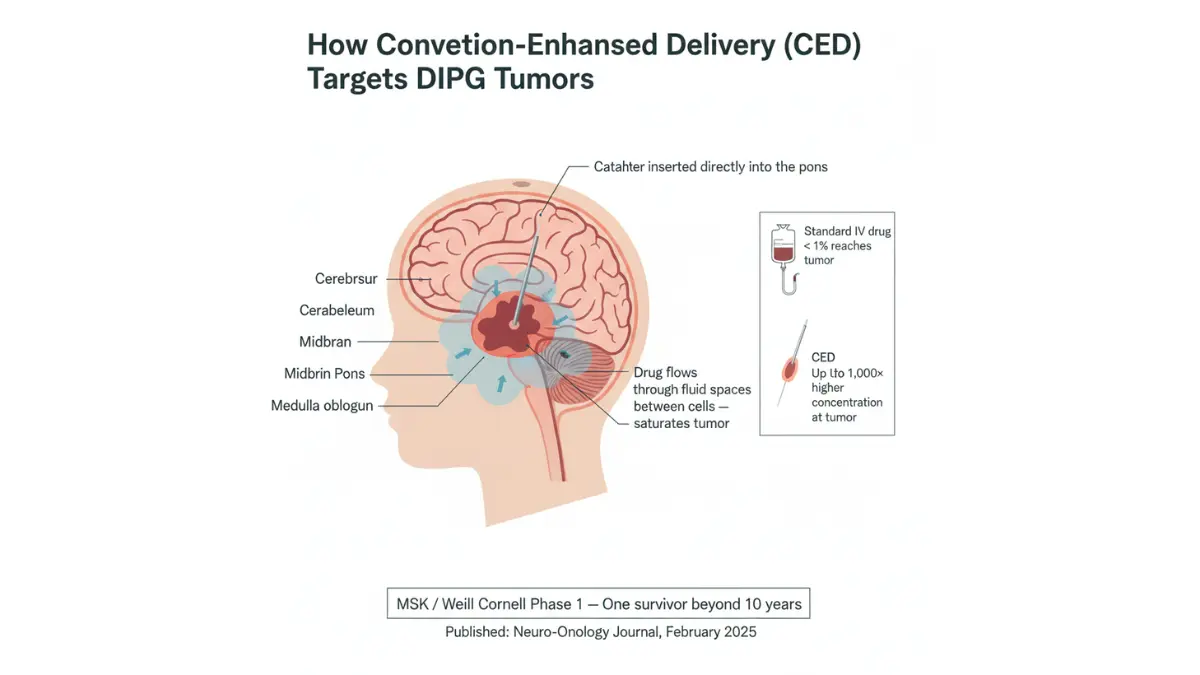
Convection-Enhanced Delivery (CED) — The 10-Year Survivor Milestone
Researchers at Memorial Sloan Kettering (MSK) and Weill Cornell Medicine published Phase 1 results in February 2025 showing that directly infusing a targeted radioimmunotherapy drug (124I-Omburtamab) into the brainstem via CED produced drug concentrations 1,000 times higher at the tumor site compared to systemic delivery.
The results were extraordinary:
- Three long-term survivors from a 50-patient Phase 1 trial
- One survivor confirmed beyond 10 years — the longest DIPG survivor documented in this type of trial
- Seven different dose levels all demonstrated safety in children
- A Phase 2 trial is now underway at MSK
The TarGeT Umbrella Trial — 24 Global Centers, Open Now
TarGeT (Targeted Pediatric High-Grade Glioma Therapy) is a groundbreaking Phase 2 molecularly guided umbrella trial that matches each child’s treatment to the specific genetic profile of their tumor.
- Open at Nationwide Children’s Hospital (Columbus, Ohio) and expanding to 24 CONNECT consortium sites globally
- Eligible patients: ages 12 months to 39 years with newly diagnosed H3K27M+ HGG/DIPG
- All cases reviewed by a global panel of genomics, pathology, and neuro-oncology experts
- Each participant first receives six weeks of standard radiation, then receives targeted therapy matched to their tumor’s molecular profile
To find open trials for DIPG in 2026, search directly on ClinicalTrials.gov using the terms “DIPG” or “diffuse midline glioma.”
DIPG Treatment Quick-Reference Table
| Treatment | Status (2026) | Eligible Patients | Where to Access |
|---|---|---|---|
| Radiation therapy | Standard of care | All newly diagnosed | Any major pediatric oncology center |
| Modeyso (dordaviprone) | FDA approved Aug 6, 2025 | H3K27M+ DMG/DIPG, age 1+, progressive disease | Oncology pharmacy (prescription required) |
| BCB-276 CAR-T | Phase 2 trial (enrolling) | DIPG/DMG, age 1–26 | Seattle Children’s + planned expansion sites |
| CED (124I-Omburtamab) | Phase 2 ongoing | DIPG children | MSK / Weill Cornell New York |
| TarGeT Umbrella Trial | Open for enrollment | H3K27M+ HGG, age 1 month–39 years | Nationwide Children’s + 24 global sites |
After a DIPG Diagnosis — Your 72-Hour Action Plan
This section covers what no competitor article does: what to actually do in the days immediately after a DIPG diagnosis.
Receiving a DIPG diagnosis for your child may be the most devastating experience a parent will ever face. The medical system moves fast. Here is a clear, step-by-step guide for the first 72 hours.
Step 1: Request H3K27M Mutation Testing Immediately
This is the single most important action. The H3K27M test determines whether your child qualifies for Modeyso (dordaviprone) — the first FDA-approved drug for this disease. Not all centers automatically perform this test at diagnosis. Ask explicitly: “Has the tumor been tested for the H3K27M mutation?”
Step 2: Seek a Second Opinion at a Dedicated Pediatric Neuro-Oncology Center
DIPG treatment planning should involve specialists with focused experience in this tumor type. You are entitled to a second opinion, and the best centers will welcome it.
Top DIPG centers in the United States:
- St. Jude Children’s Research Hospital — Memphis, TN
- Seattle Children’s Hospital — Seattle, WA (BCB-276 CAR-T trial site)
- MSK / Weill Cornell — New York, NY (CED trial site)
- Dana-Farber / Boston Children’s — Boston, MA
- Nationwide Children’s Hospital — Columbus, OH (TarGeT trial hub)
Step 3: Search for Clinical Trials Your Child Qualifies For
Use ClinicalTrials.gov and search “diffuse intrinsic pontine glioma” or “diffuse midline glioma.” Filter by age, mutation status, and treatment history. Many trials enroll patients at or shortly after diagnosis — not only at progression.
Step 4: Ask Your Oncologist About Modeyso Eligibility
For children with progressive disease after radiation, dordaviprone (Modeyso) is now FDA-approved. Ask directly: “Does my child meet the criteria for dordaviprone?” Your oncologist can prescribe it if your child is aged 1 or older and the H3K27M mutation is confirmed.
Step 5: Connect With DIPG Advocacy Resources
Organizations like the DIPG Advocacy Group (dipg.org) provide trial navigation support, family connections, and funding resources for families who cannot access major centers.
Step 6: Begin Palliative Care Early — It Is Not Giving Up
Early palliative and supportive care improves quality of life and does not replace curative treatment. It addresses pain, nausea, neurological symptoms, and family support — alongside all other treatments. Ask for a palliative care referral at diagnosis, not at end of life.
For families navigating a serious brain tumor diagnosis, our articles on brain tumor warning signs and glioblastoma treatment data provide related context on high-grade glioma management.
Frequently Asked Questions About DIPG
1. What does DIPG stand for?
DIPG stands for Diffuse Intrinsic Pontine Glioma. It is an aggressive brain tumor growing inside the pons region of the brainstem, primarily affecting children aged 5–9.
2. Is DIPG curable in 2026?
DIPG has no confirmed cure as of 2026. However, FDA-approved Modeyso and CAR-T trials have produced unprecedented long-term survivors, with three children now alive past 44 months in one trial.
3. What are the first signs of DIPG?
The earliest sign is usually an eye movement problem — specifically an inward-turning eye (abducens palsy). Balance problems and facial weakness typically follow within days to weeks.
4. What is the DIPG survival rate?
With standard radiation, median survival is 9–11 months. In the 2025 BCB-276 CAR-T trial, three children remain alive at 44–52 months from diagnosis.
5. Is there a new FDA-approved drug for DIPG?
Yes. The FDA granted accelerated approval to dordaviprone (Modeyso) on August 6, 2025 — the first systemic drug ever approved for H3K27M-mutant diffuse midline glioma (DIPG/DMG).
6. What is the H3K27M mutation in DIPG?
It is a mutation in the histone H3 protein found in ~80% of pediatric DIPG cases. It drives uncontrolled tumor growth and is now the primary target of FDA-approved Modeyso and several experimental therapies.
7. Can DIPG occur in adults?
DIPG is rare in adults but does occur. The 2021 WHO reclassification to diffuse midline glioma (DMG) encompasses adult cases. Modeyso is approved for patients aged 1 year and older.
8. Is DIPG hereditary?
No. DIPG is not inherited and has no known environmental risk factors. It results from a random mutation during brain development and cannot be predicted or prevented.
9. How is DIPG diagnosed?
Diagnosis is primarily through brain MRI with gadolinium contrast. A stereotactic biopsy to test for the H3K27M mutation is increasingly recommended, as this mutation determines drug eligibility.
10. What are the best hospitals for DIPG treatment in the USA?
Leading centers include St. Jude Children’s Research Hospital, Seattle Children’s Hospital, MSK/Weill Cornell, Dana-Farber/Boston Children’s, and Nationwide Children’s Hospital.
11. Are DIPG clinical trials open in 2026?
Yes. The TarGeT umbrella trial (24 global centers), BCB-276 Phase 2 CAR-T trial, and CED trials at MSK are all active. Search ClinicalTrials.gov using “DIPG” or “diffuse midline glioma” for current openings.
⚠️ Medical Disclaimer: This article is for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment recommendations. Always consult a licensed pediatric oncologist or neuro-oncologist for guidance specific to your child’s condition and individual clinical circumstances.
Reviewed by the mymedicineadvisor.com Medical Advisory Panel | Published February 2026 | Sources: National Cancer Institute (cancer.gov), American Association for Cancer Research (AACR), Memorial Sloan Kettering Cancer Center, Seattle Children’s Hospital, Nationwide Children’s Hospital, FDA.gov
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.











