On This Page – Quick Medical Summary
The Life-Saving Truth About Stage 1 Lung Cancer
When Sarah’s doctor called about her routine chest CT scan results, she braced for the worst. A tiny 9mm nodule had appeared in her right lung. Six weeks after minimally invasive surgery, she walked out cancer-free—joining the growing number of Americans whose early detection transformed what was once a death sentence into a highly curable condition.
Stage 1 lung cancer survival rate reaches 90% when caught early, with the smallest tumors showing cure rates approaching 95%. According to the National Cancer Institute’s SEER database, localized lung cancer patients diagnosed between 2015-2021 achieved a 64.7% five-year survival rate—a dramatic improvement from just a decade ago. For stage 1A1 tumors measuring 1 centimeter or less, survival rates climb even higher, reaching 90% at five years and maintaining 97% survival at two years.
Why 2025 Changes Everything for Early Detection
The January 2025 NCCN Guidelines expanded screening eligibility, potentially saving thousands of additional lives annually. Combined with artificial intelligence-enhanced CT scanning that reduces false positives by 70%, more Americans than ever can access life-saving early detection.
What makes stage 1 different: The cancer remains confined to the lung with no lymph node involvement. This localization allows for surgical removal with curative intent—something impossible once the disease spreads.
Survival Rates That Give Real Hope
| Stage | Tumor Size | 5-Year Survival | 2-Year Survival |
|---|---|---|---|
| IA1 | ≤1 cm | 90% | 97% |
| IA2 | 1-2 cm | 85% | 94% |
| IA3 | 2-3 cm | 80% | 92% |
| IB | 3-4 cm | 73% | 89% |
*Source: American Cancer Society 2025 data *
Recent screening studies reveal even more encouraging outcomes. Research published in Cancer Network found that patients with stage 1 lung cancer detected through low-dose CT screening—particularly tumors 10mm or smaller—achieved 95% ten-year survival rates. Among those who underwent surgery within one month of diagnosis, survival jumped to 92%.
The Asymptomatic Danger Most People Miss
Here’s the catch: 54% of early-stage lung cancer patients experience zero symptoms. You can have a growing tumor and feel completely healthy, which is why understanding your screening eligibility matters more than waiting for warning signs.
This explains why screening guidelines now prioritize risk factors over symptoms. The U.S. Preventive Services Task Force recommends annual screening for adults aged 50-80 with a 20 pack-year smoking history, but many Americans who qualify remain unscreened.
What This Means For You: If you’re over 50 with smoking history, getting screened isn’t optional—it’s the difference between a 90% cure rate and a far grimmer prognosis. Understanding your baseline health through tools like a BMI calculator can help contextualize your overall cancer risk, especially since maintaining optimal weight reduces cancer recurrence risk by up to 30%.
The window for catching lung cancer at its most curable stage is narrow. But with 2025’s expanded screening access and improved detection technology, that window is wider than ever.
Decoding Stage 1—Not All Early Cancers Are Equal
What Makes Stage 1A Different from Stage 1B?
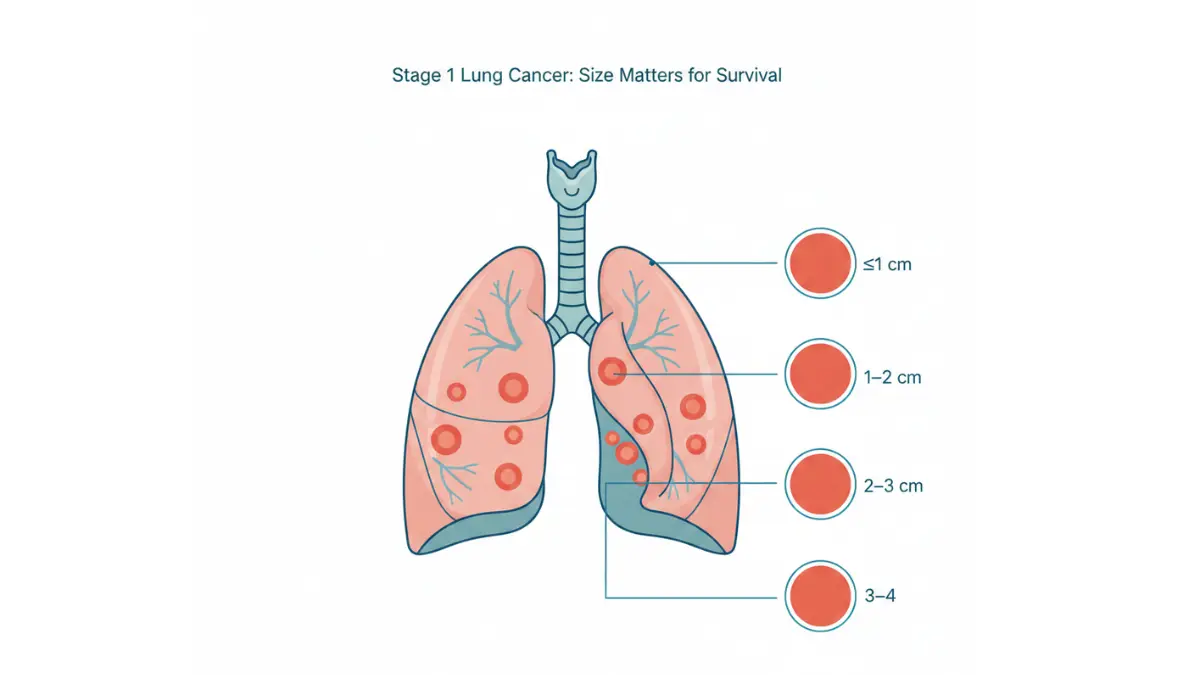
Stage 1 lung cancer isn’t a single diagnosis—it’s a spectrum with dramatically different survival rates depending on tumor size and characteristics. The American Joint Committee on Cancer’s TNM system divides stage 1 into six distinct subcategories, each with unique treatment approaches and outcomes.
Understanding these differences matters because a 9mm tumor (stage 1A1) carries a 90% five-year survival rate, while a 3.5cm tumor (stage 1B) drops to 73%—a 17-point survival gap.
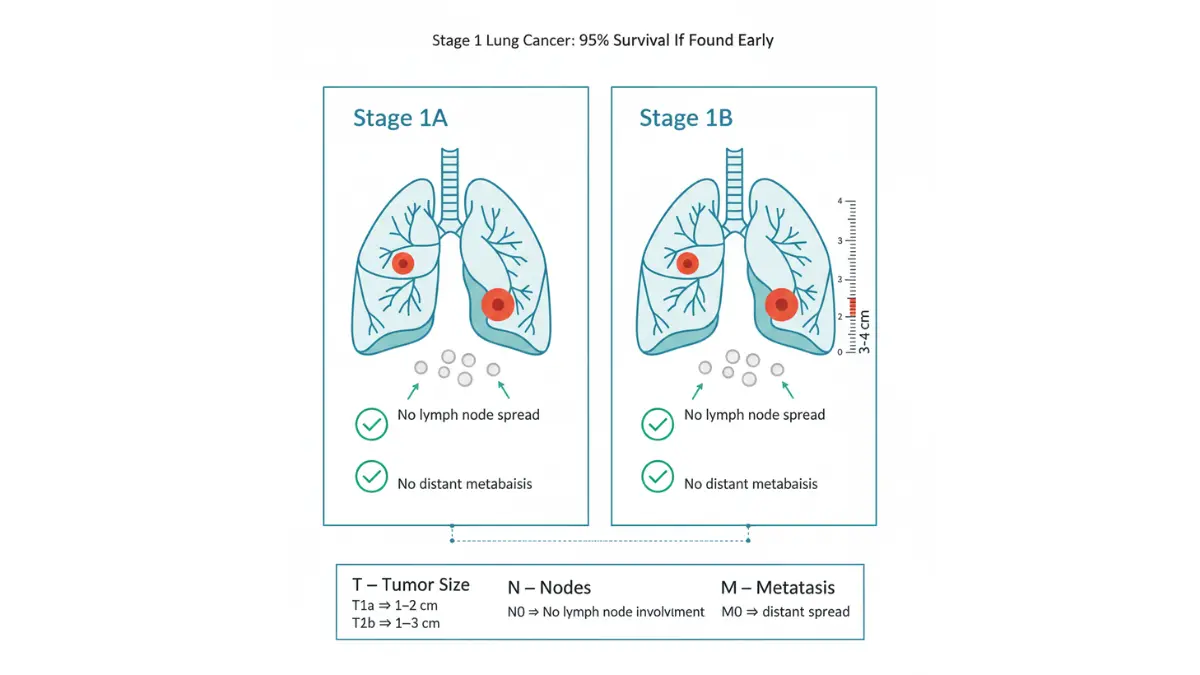
Stage 1A: The Most Curable Category
Stage 1A tumors remain 3 centimeters or smaller and show no lymph node involvement. The National Cancer Institute’s TNM classification system further subdivides this into three critical levels:
Stage 1A1 (T1a N0 M0):
- Tumor ≤1 cm (about the size of a pea)
- 90% five-year survival rate
- Often detected only through screening CT scans
- Minimally invasive adenocarcinoma qualifies here regardless of total lesion size
Stage 1A2 (T1b N0 M0):
- Tumor >1 cm but ≤2 cm (size of a grape)
- 85% five-year survival rate
- May still be asymptomatic in 60% of patients
Stage 1A3 (T1c N0 M0):
- Tumor >2 cm but ≤3 cm (size of a walnut)
- 80% five-year survival rate
- Transition point where symptoms become more common
Stage 1B: Larger But Still Localized
Stage 1B (T2a N0 M0):
- Tumor >3 cm but ≤4 cm
- 73% five-year survival rate
- More likely to require adjuvant therapy after surgery
| Stage | Tumor Size | 5-Year Survival | Typical Symptoms | Treatment Approach |
|---|---|---|---|---|
| 1A1 | ≤1 cm | 90% | Usually none | Surgery alone |
| 1A2 | 1-2 cm | 85% | Often none | Surgery ± surveillance |
| 1A3 | 2-3 cm | 80% | Mild/intermittent | Surgery + close monitoring |
| 1B | 3-4 cm | 73% | More frequent | Surgery + possible adjuvant therapy |
The Silent Killer: Asymptomatic Presentation
25% of all lung cancer cases produce zero symptoms at diagnosis, according to research published in the U.S. Pharmacist. For stage 1 specifically, that percentage climbs higher—with studies showing 54-60% of early-stage patients reporting no warning signs.
This asymptomatic period creates a dangerous illusion of health. You might feel energetic enough to maintain your normal workout routine using a heart rate zone calculator, yet harbor a growing tumor visible only on imaging.
Korean research tracking 3,000+ patients found that asymptomatic lung cancer patients were:
- More likely to be younger and female
- Three times more likely to receive curative surgery (60% vs 20%)
- More frequently diagnosed with adenocarcinoma subtype
- Significantly more likely to survive five years
When Symptoms Do Appear
The most common early lung cancer symptoms include:
- Persistent cough lasting 3+ weeks (not typical cold/flu pattern)
- Chest discomfort that worsens with deep breathing
- Shortness of breath during activities previously manageable
- Unexplained fatigue despite adequate sleep
- Recurrent respiratory infections in the same lung area
If you’re experiencing any combination of these symptoms, use our symptom checker as a starting point, but schedule an appointment with your doctor immediately—not next month, this week.
NSCLC Subtypes Matter for Stage 1 Prognosis
Non-small cell lung cancer encompasses three primary histologic types, each carrying different survival implications even at stage 1.
Adenocarcinoma (Most Common):
- Represents 60-70% of stage 1 NSCLC cases
- Five-year survival: 72.4% for early-stage disease
- More common in never-smokers and women
- Tends to grow slower than other subtypes
Squamous Cell Carcinoma:
- Accounts for 25-30% of cases
- Five-year survival: 62.6% for early-stage disease
- Strongly linked to smoking history
- More likely to be centrally located in airways
Large Cell Carcinoma (Rare):
- Less than 5% of cases
- Tends to grow and spread more aggressively
- Often requires more intensive treatment even at stage 1
Research comparing these subtypes found that adenocarcinoma patients with T1-T2N0M0 disease achieved significantly better long-term survival than squamous cell carcinoma patients, even after controlling for tumor size and other prognostic factors.
What This Means For You: Your pathology report’s histologic subtype isn’t just medical jargon—it directly influences your treatment plan and surveillance schedule. Adenocarcinoma patients might qualify for less aggressive follow-up, while squamous cell patients often need more frequent imaging.
Understanding your precise stage 1 subcategory transforms your diagnosis from a scary label into actionable information. A 1A1 adenocarcinoma warrants an entirely different conversation with your oncologist than a 1B squamous cell carcinoma—and recognizing that distinction empowers you to ask the right questions about your specific prognosis.
How Early Detection Saves Lives—2025 Screening Guidelines
The Low-Dose CT Revolution
Low-dose computed tomography (LDCT) lung cancer screening has transformed early detection, catching 80% of lung cancers at stage 1 when survival rates exceed 85%. The technology uses 90% less radiation than traditional chest CT scans while producing detailed cross-sectional images that reveal nodules as small as 3 millimeters—roughly the size of a pencil eraser tip.
A single 15-minute scan can detect tumors years before symptoms appear, making it the most powerful tool in lung cancer early detection. Yet only 5.8% of eligible Americans get screened annually, leaving millions at unnecessary risk.
Who Should Get Screened? 2025 Updated Guidelines
The U.S. Preventive Services Task Force expanded screening eligibility in 2021, and Medicare followed suit in February 2022. These changes make 15 million more Americans eligible for potentially life-saving screening.
Current USPSTF Screening Criteria (Grade B Recommendation):
- Age: 50-80 years old
- Smoking history: At least 20 pack-years (equivalent to 1 pack daily for 20 years, or 2 packs daily for 10 years)
- Current status: Currently smoking OR quit within past 15 years
- Health status: Healthy enough to undergo curative surgery if cancer detected
Medicare Coverage Expanded Criteria (Ages 50-77):
Medicare beneficiaries now qualify with just 20 pack-years instead of the previous 30 pack-year requirement. This expansion disproportionately benefits women and Black Americans, who historically developed lung cancer with lower smoking exposure.
What About Never-Smokers?
While traditional guidelines focus on smoking history, emerging research shows 10-20% of lung cancer patients never smoked. Risk factors for never-smokers include:
- Secondhand smoke exposure (living with smoker for 20+ years)
- Occupational exposures (asbestos, radon, diesel fumes)
- Family history of lung cancer (first-degree relative diagnosed before age 60)
- Chronic lung diseases like COPD or pulmonary fibrosis
Talk to your doctor about screening eligibility even without smoking history if multiple risk factors apply. Consider using a genetic risk assessment tool to evaluate your inherited cancer predisposition, especially if lung cancer runs in your family.
Understanding LDCT Scanning Process
What happens during screening:
- You lie on a table that slides through a donut-shaped CT scanner
- Hold your breath for 5-10 seconds while images are captured
- No injections, contrast dye, or needles required
- Total appointment time: 15-30 minutes including paperwork
- Results typically available within 7-10 business days
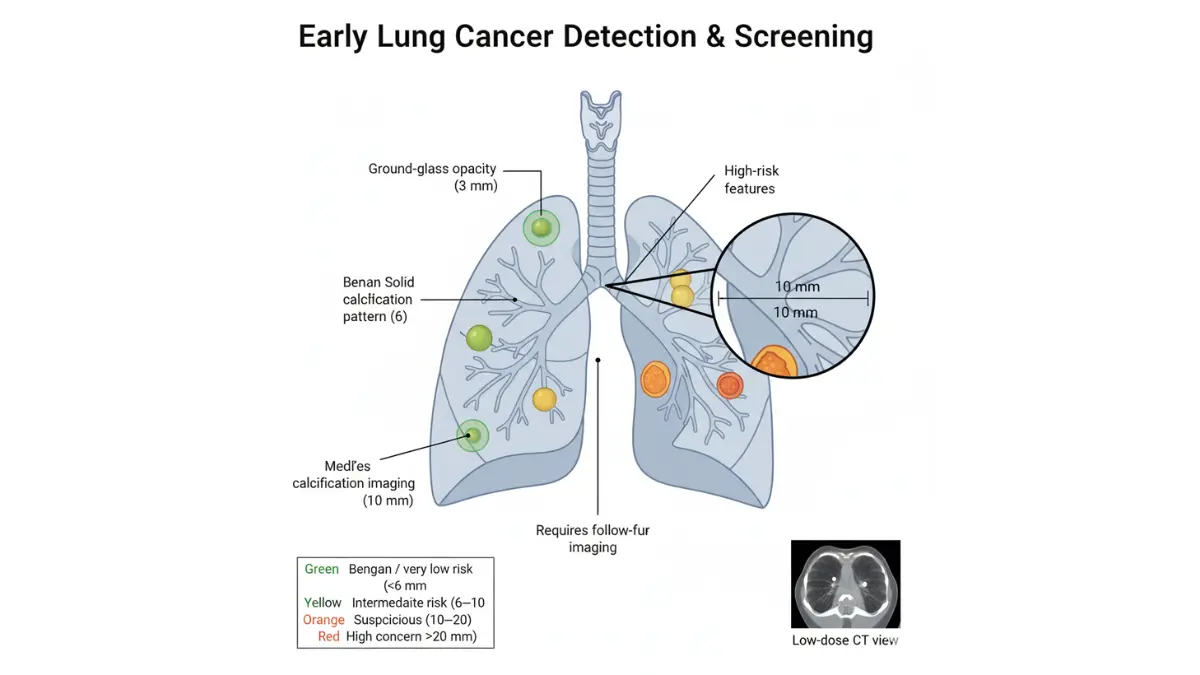
Lung-RADS scoring system interprets results:
- Category 1: Negative (no nodules) → continue annual screening
- Category 2: Benign findings → continue annual screening
- Category 3: Probably benign → 6-month follow-up CT
- Category 4: Suspicious findings → diagnostic workup recommended
AI Technology Reducing False Positives
Artificial intelligence algorithms now assist radiologists in detecting lung nodules with remarkable accuracy. Research published in 2025 shows AI systems achieve over 95% sensitivity in pulmonary nodule detection while reducing false-positive rates to fewer than one per scan.
How AI improves screening:
- Identifies subtle nodules human eyes might miss
- Analyzes growth patterns by comparing previous scans
- Prioritizes suspicious findings for radiologist review
- Reduces radiologist workload by 30-40%, speeding up results
This technology is particularly valuable for detecting ground-glass opacities—hazy lung areas that often indicate early adenocarcinoma but are notoriously difficult to spot.
Cost Transparency: What You’ll Actually Pay
Medicare Coverage (Ages 50-77):
- Annual deductible: $240 (2026 rate)
- After deductible met: Medicare pays 80%, you pay 20%
- Out-of-pocket cost: $0-$60 per scan if deductible already met
- Shared decision-making visit: Fully covered with no copay
Private Insurance:
Most plans cover annual LDCT screening at 100% with no copay under the Affordable Care Act’s preventive services mandate. Verify coverage by calling the number on your insurance card and asking specifically about “low-dose CT lung cancer screening under USPSTF guidelines.”
Self-Pay Rates (Without Insurance):
- Hospital outpatient: $250-$600 per scan
- Freestanding imaging centers: $99-$300 per scan
- Average U.S. cost: $300
Many facilities offer cash-pay discounts or payment plans. Ask about pricing transparency before scheduling.
Finding Accredited Screening Centers
Not all CT scans meet lung cancer screening standards. Only facilities designated by the American College of Radiology (ACR) as “Lung Cancer Screening Centers” should perform these specialized scans.
To find accredited centers near you:
- Search the ACR’s online directory (filter by “Lung Cancer Screening”)
- Ask your primary care physician for referrals to ACR-accredited facilities
- Check your insurance provider’s website for in-network screening locations
- Call local hospitals and specifically ask: “Are you ACR-accredited for lung cancer screening?”
What makes ACR accreditation matter:
- Radiologists trained specifically in lung nodule detection
- CT equipment calibrated for low-dose protocols
- Standardized Lung-RADS reporting system
- Established protocols for following suspicious findings
Understanding other cancer warning signs can complement your screening strategy—learn about early warning signs across multiple cancer types to develop comprehensive cancer awareness.
What This Means For You: If you’re 50+ with 20+ pack-years of smoking history, screening eligibility isn’t theoretical—it’s a concrete action item for this month. The difference between a stage 1 diagnosis (90% survival) and stage 4 diagnosis (10% survival) often comes down to whether you scheduled that annual CT scan.
Don’t let cost concerns delay screening. With Medicare covering 80-100% and many imaging centers charging under $200 for self-pay patients, the financial barrier has largely disappeared. The biggest obstacle isn’t money—it’s awareness and action.
Treatment Options That Achieve 90%+ Cure Rates
Surgery: The Gold Standard for Stage 1
Surgical removal remains the most effective treatment for stage 1 lung cancer, with curative intent achieved in 85-92% of cases when performed within optimal timeframes. The National Cancer Institute recommends surgery as first-line treatment for all stage IA and IB patients healthy enough to undergo the procedure.
Most stage 1 patients undergo lobectomy—removal of the entire lobe containing the tumor. This approach provides the best chance of eliminating all cancer cells while preserving maximum lung function.
VATS: The Minimally Invasive Revolution
Video-assisted thoracoscopic surgery (VATS) has transformed lung cancer treatment. A landmark 2025 meta-analysis presented at the World Conference on Lung Cancer revealed that VATS reduces overall mortality by 21% compared to traditional open surgery—without compromising cancer-free survival rates.
Why VATS beats open surgery:
- 3-5 small incisions (each 1-2 inches) vs. 6-8 inch chest-splitting incision
- Hospital stay: 3-5 days vs. 7-10 days for open surgery
- Recovery time: Return to normal activities in 4-6 weeks vs. 8-12 weeks
- Pain levels: Significantly reduced postoperative discomfort
- Complication rates: 21% lower risk of death at 10-year follow-up
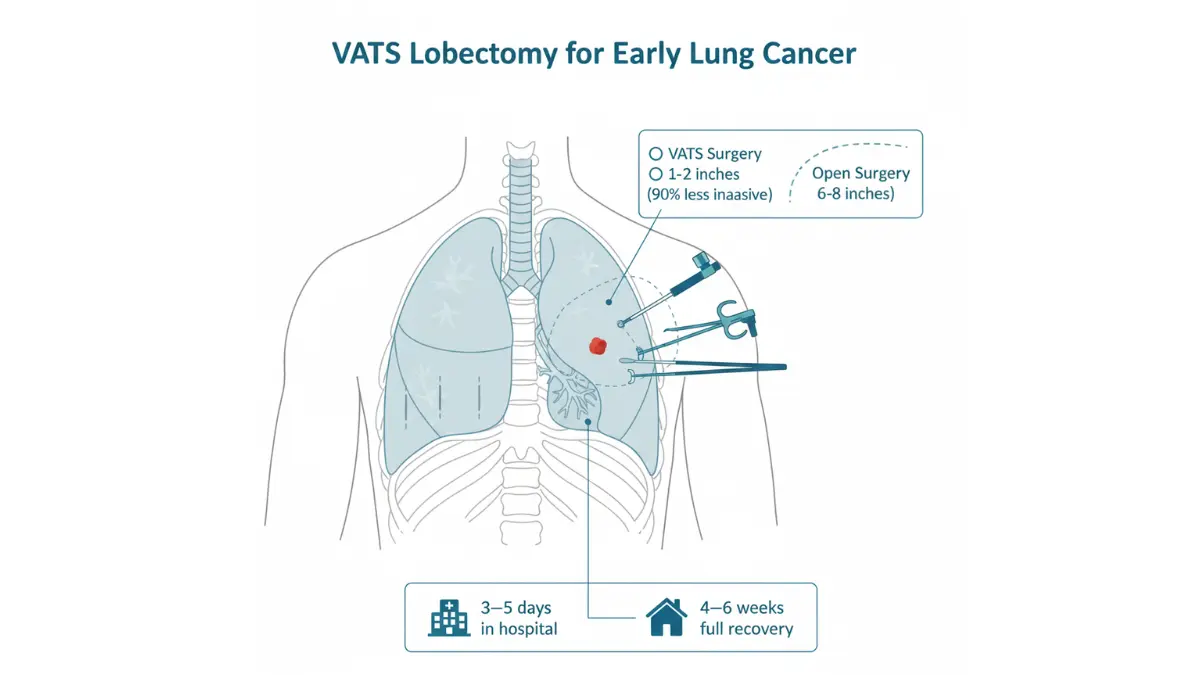
Ten-year data shows VATS patients maintain a 77.1% survival rate compared to 68.4% for open surgery patients—a compelling 9-point survival advantage.
Surgical Options by Tumor Size
| Procedure | Tumor Size | Lung Tissue Removed | Recovery Time | 5-Year Survival |
|---|---|---|---|---|
| Wedge/Segmental Resection | ≤2 cm | Small portion of lobe | 3-4 weeks | 85-90% |
| Lobectomy | Any stage 1 size | Entire lobe (1 of 5 sections) | 4-6 weeks (VATS) | 85-92% |
| Sleeve Resection | Airway involvement | Portion of bronchus + tumor | 6-8 weeks | 80-85% |
Research from the National Cancer Institute suggests that sublobar resection (wedge or segmental) works just as well as lobectomy for tumors 2cm or smaller—offering faster recovery without sacrificing cure rates.
When Surgery Isn’t an Option: SBRT
Stereotactic body radiation therapy (SBRT) delivers precisely targeted, high-dose radiation beams that destroy tumors without incisions. For patients who can’t undergo surgery due to poor lung function, heart disease, or age-related factors, SBRT provides a legitimate curative alternative.
10-year survival data released in 2025 shows:
- Overall survival rate: 70.7% for SBRT patients
- Comparable to surgery outcomes for tumors ≤2cm
- Treatment completed in 3-5 outpatient sessions over 1-2 weeks
- No anesthesia, no hospital stay, no surgical recovery
Game-Changing Immunotherapy Advances
The biggest treatment breakthrough for stage 1 lung cancer in 2025 involves perioperative immunotherapy—using immune checkpoint inhibitors before and after surgery to prevent recurrence.
Pembrolizumab: FDA-Approved Adjuvant Therapy
In January 2023, the FDA approved pembrolizumab (Keytruda) as adjuvant therapy following surgical resection and chemotherapy for certain stage IB-IIIA patients. The groundbreaking KEYNOTE-671 trial demonstrated that adding perioperative pembrolizumab to chemotherapy:
- Improved event-free survival by 42% (hazard ratio 0.58)
- Achieved 30% major pathologic response rate vs. 11% with chemotherapy alone
- Delivered 18% complete pathologic response (no viable cancer cells remaining) vs. 4%
- Showed significant overall survival benefit at second interim analysis
Who qualifies for immunotherapy:
- Stage IB tumors ≥4cm or stage II-IIIA disease
- PD-L1 expression testing (higher expression = better response)
- No EGFR or ALK mutations (these patients benefit more from targeted therapy)
- Adequate organ function and performance status
For patients with targetable genetic mutations like EGFR, ALK, or ROS1, precision medicine offers even better outcomes. Learn about the latest FDA-approved lung cancer drugs and targeted therapies transforming treatment options.
Treatment Cost Reality Check
Stage 1 Lung Cancer Surgery Costs (United States, 2026):
With Insurance:
- Medicare: $240 deductible + 20% coinsurance = $1,500-$3,000 out-of-pocket for surgery
- Private insurance: Typically $1,000-$5,000 after deductible, depending on plan
- High-deductible plans: Expect $3,000-$7,500 until deductible met
Without Insurance (Self-Pay):
- VATS lobectomy: $25,000-$45,000 (hospital charges)
- Open lobectomy: $30,000-$55,000
- SBRT radiation: $30,000-$50,000 for complete course
- Hospital stay: $2,000-$4,000 per day
Immunotherapy Costs:
- Pembrolizumab: $9,000-$15,000 per infusion (every 3 weeks for up to 1 year)
- Total adjuvant immunotherapy: $135,000-$225,000 for full course
- Medicare Part B coverage: Typically covers 80% after deductible
These figures represent facility charges before negotiation. Many hospitals offer financial assistance programs that can reduce self-pay costs by 40-70% based on income. Cash-pay discounts of 20-30% are common if you negotiate upfront payment.
Recovery Timeline and Expectations
Post-Surgery Milestones:
- Days 1-3: Hospital stay with chest tube drainage
- Week 1-2: Pain management, breathing exercises, short walks
- Week 3-4: Gradual activity increase, no heavy lifting (>10 lbs)
- Week 6-8: Return to desk work, light exercise approved
- Month 3: Resume normal activities including exercise
- Month 6: Full recovery achieved for most patients
Maintaining optimal nutrition accelerates healing—use a protein intake calculator to ensure you’re consuming adequate protein (1.2-1.5g per kg body weight) during recovery.
What This Means For You: Stage 1 lung cancer treatment has never been more effective or less invasive. The combination of VATS surgery achieving 90%+ survival rates, SBRT offering a no-surgery alternative, and immunotherapy preventing recurrence creates a treatment landscape where cure is the expected outcome—not the exception. Cost remains a significant barrier, but Medicare covers most treatments at 80%, and hospital financial assistance programs can reduce bills substantially for those without insurance.
Life After Treatment—Staying Cancer-Free
Understanding Your Recurrence Risk
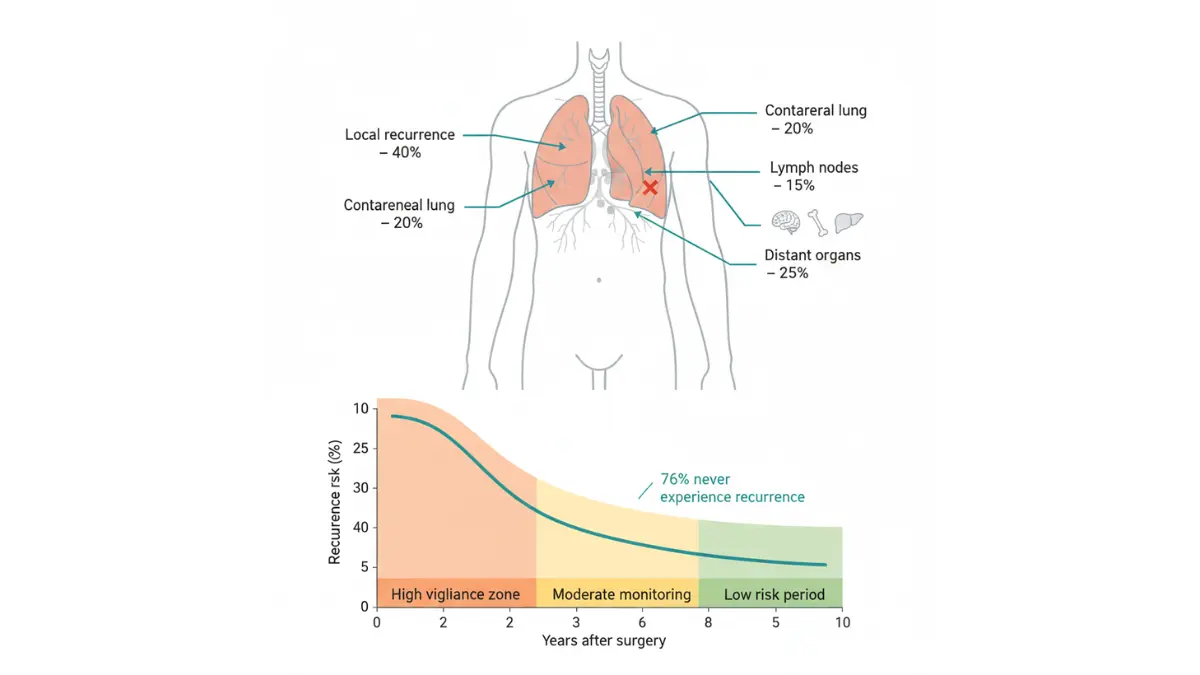
Stage 1 lung cancer recurs in approximately 24-26% of patients after surgical resection, according to multi-institutional studies tracking outcomes over five years. This means 74-76% of patients never experience recurrence—a reassuring majority that represents the new reality of early-stage lung cancer survival.
Recurrence timing follows predictable patterns. Most recurrences develop within the first two years post-surgery, with a median recurrence time of 22 months. After five years, recurrence risk drops dramatically—and after ten years, the risk approaches nearly zero for many patients.
Factors that influence recurrence risk:
- Tumor size: Larger stage 1 tumors (3-4cm) recur more frequently than smaller ones
- Surgical margins: Positive margins increase risk 3-fold
- Lymph node sampling: Comprehensive lymph node dissection reduces recurrence by 18%
- Continued smoking: Doubles recurrence risk compared to quitting
- Sublobar resection: Shows 38% recurrence rate vs. 20% for lobectomy
Your Surveillance Schedule
Consistent follow-up imaging catches 80-85% of recurrences when they’re still treatable. The American College of Chest Physicians and European Society of Medical Oncology recommend this evidence-based surveillance protocol:
Years 1-2 Post-Surgery:
- Chest CT scan with IV contrast every 6 months
- History and physical exam at each visit
- PET scan only if concerning findings appear on CT
Years 3-5 Post-Surgery:
- Annual low-dose chest CT (same technology used for screening)
- Annual clinical exam
- Symptom assessment at every visit
After 5 Years:
- Continue annual low-dose CT screening indefinitely
- Risk of new primary lung cancer remains 13% over lifetime
For patients who received radiation therapy instead of surgery, more frequent surveillance continues—CT scans every 3-6 months for the first three years before transitioning to annual screening.
Lifestyle Changes That Cut Recurrence Risk
Smoking cessation delivers the single most powerful recurrence prevention benefit. Research published in 2024 demonstrates that patients who quit smoking after surgery achieve 80% five-year survival compared to just 64% for those who continue smoking—a 16-point survival advantage.
Quitting reduces:
- Recurrence risk by 48%
- Secondary lung cancer development by 57%
- Overall mortality by 69% (hazard ratio 2.31 for continued smoking)
Evidence-based lifestyle modifications:
Exercise (150 minutes weekly):
- Improves lung function recovery by 15-20%
- Reduces cancer-related fatigue
- May lower recurrence risk by up to 30%
- Use a pace calculator to gradually build endurance safely
Nutrition priorities:
- High-protein diet (1.2-1.5g per kg body weight) supports tissue healing
- Antioxidant-rich foods (berries, leafy greens, cruciferous vegetables)
- Omega-3 fatty acids reduce inflammation
- Avoid processed meats and excessive red meat consumption
Weight management:
- Maintaining BMI 18.5-24.9 optimizes outcomes
- Obesity increases recurrence risk and complicates surveillance imaging
- Underweight status (<18.5 BMI) correlates with worse survival
Quality sleep (7-9 hours nightly):
- Supports immune system recovery
- Reduces inflammatory markers
- Improves treatment tolerance and energy levels
New Primary Lung Cancer Risk
Even with successful stage 1 treatment, 13% of patients develop a second primary lung cancer within their lifetime—a separate tumor unrelated to the original cancer. This elevated risk justifies lifelong annual CT screening.
The distinction matters: Recurrence means the original cancer returned, while a new primary represents a completely different tumor. New primaries often occur in different lung locations and may have different histology (adenocarcinoma vs. squamous cell).
When to Call Your Doctor Immediately
Don’t wait for scheduled appointments if you experience:
- New persistent cough lasting 3+ weeks
- Chest pain that worsens with breathing
- Unexplained weight loss of 5+ pounds in one month
- Hemoptysis (coughing up blood, even small amounts)
- Shortness of breath with minimal exertion
- Bone pain (potential metastasis site)
- Severe headaches or neurological changes
Early detection of recurrence significantly improves re-treatment success rates. Most recurrences caught on surveillance imaging before symptoms appear remain potentially curable with additional therapy.
What This Means For You: Life after stage 1 lung cancer treatment isn’t just about surviving—it’s about thriving. With 75% never experiencing recurrence, consistent surveillance catching most recurrences early, and lifestyle modifications cutting risk nearly in half, you hold substantial control over your long-term outcome. Quitting smoking alone delivers a 16-point survival advantage. Combined with regular CT surveillance and healthy lifestyle choices, you’re stacking the odds overwhelmingly in your favor.
Your Action Plan—Getting Screened This Month
Stop Waiting: Schedule Your Screening Today
The best time to get screened was five years ago. The second best time is this week. With 90%+ survival rates for stage 1 lung cancer and Medicare covering screening at minimal or no cost, financial and logistical barriers have largely disappeared.
Only inaction stands between you and potentially life-saving early detection.
Step 1: Determine Your Eligibility
You qualify for Medicare-covered lung cancer screening if you meet ALL these criteria:
- Age 50-77 years old
- Current smoker OR quit within past 15 years
- At least 20 pack-year smoking history
- No current lung cancer symptoms
- Order from your healthcare provider
Medicare Part B covers annual LDCT screening with zero copay after you complete a shared decision-making visit with your doctor. This counseling session discusses your individual risk, screening benefits, and what happens if abnormalities are found.
Private insurance coverage: The Affordable Care Act requires most plans to cover USPSTF Grade A and B preventive services with no cost-sharing. Lung cancer screening qualifies, meaning you shouldn’t pay copays or coinsurance—but verify your specific plan’s terms before scheduling.
Step 2: Talk to Your Doctor
Many primary care physicians aren’t proactively recommending lung cancer screening despite eligibility expansion in 2021. You may need to initiate the conversation.
What to say: “I’m [age] with [X] years of smoking history. Based on the 2021 USPSTF guidelines, I believe I qualify for lung cancer screening. Can you write me an order for a low-dose CT scan?”
Questions to ask:
- Which ACR-accredited facilities do you recommend?
- Will my insurance cover this screening with no copay?
- How will I receive my results, and what’s the typical turnaround time?
- If they find something suspicious, what are the next steps?
- Should I have any baseline testing done before the CT scan?
Step 3: Find ACR-Accredited Screening Centers
Search for “ACR-accredited lung cancer screening centers” plus your city/state to find qualified facilities near you. Major hospital systems like Mayo Clinic, Cleveland Clinic, Johns Hopkins, Duke Cancer Institute, and regional cancer centers typically offer designated lung cancer screening programs.
What makes a facility qualified:
- American College of Radiology Lung Cancer Screening Center designation
- Radiologists trained in Lung-RADS interpretation
- Established protocols for managing suspicious findings
- Access to thoracic surgery and pulmonology specialists if needed
Insurance Navigation Made Simple
If you have Medicare:
- Part B covers screening after your $240 annual deductible (2026 rate)
- Once deductible met, you pay 20% coinsurance (typically $0-$60)
- Shared decision-making visit fully covered
If you’re uninsured:
- Cash-pay costs: $99-$300 at most imaging centers
- Hospital charity care programs can reduce bills by 40-70% based on income
- Ask about self-pay discounts (often 20-30% off) before scheduling
Smoking Cessation Resources
If you currently smoke, quitting dramatically improves treatment outcomes and reduces recurrence risk by 48%. The CDC’s tobacco quitline (1-800-QUIT-NOW) connects you with free telephone counseling, a personalized quit plan, and FDA-approved cessation medications at no cost.
Free resources available:
- Smokefree.gov: Text message programs and mobile apps
- NCI quitSTART app: Games and daily tips for your quit journey
- State quitlines: Provide 4-8 counseling sessions plus nicotine replacement therapy
- Medicare tobacco cessation counseling: Covered up to 8 sessions per year
Taking the First Step Right Now
Don’t let this information become another article you read and forget. Your action item for today: Call your doctor’s office and request a lung cancer screening eligibility consultation. That single phone call could add decades to your life.
Understanding your overall health status helps contextualize cancer risk—consider using a sleep calculator to optimize recovery patterns that support immune function and healing.
The difference between stage 1 diagnosis (90% survival) and stage 4 diagnosis (10% survival) often comes down to whether you made that call this week or waited another year. Choose action over procrastination.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult with a qualified healthcare provider before making decisions about cancer screening, diagnosis, or treatment. Individual results may vary based on specific medical conditions, tumor characteristics, and treatment approaches.
Frequently Asked Questions About Stage 1 Lung Cancer
1. What is the survival rate for stage 1 lung cancer?
Stage 1 lung cancer has a 90% five-year survival rate for the smallest tumors (stage 1A1) and 73-85% for larger stage 1 tumors. Early detection through screening dramatically improves outcomes compared to later-stage diagnosis.
2. Can stage 1 lung cancer be cured?
Yes, stage 1 lung cancer is highly curable with surgery achieving 85-92% long-term disease-free survival. VATS minimally invasive surgery or SBRT radiation both offer curative treatment options depending on patient health status.
3. What are the early symptoms of stage 1 lung cancer?
Most stage 1 lung cancer patients (54-60%) experience no symptoms at all. When symptoms appear, they include persistent cough lasting 3+ weeks, chest discomfort, shortness of breath, and unexplained fatigue—but these are often absent in early stages.
4. How much does stage 1 lung cancer treatment cost?
With Medicare, expect $1,500-$3,000 out-of-pocket for surgery after meeting your deductible. Without insurance, VATS lobectomy costs $25,000-$45,000, though hospital financial assistance programs can reduce bills by 40-70% based on income.
5. What is the difference between stage 1A and 1B lung cancer?
Stage 1A tumors are 3cm or smaller (subdivided into 1A1, 1A2, 1A3 by size), while stage 1B tumors are 3-4cm. Stage 1A1 has 90% five-year survival versus 73% for stage 1B—tumor size directly impacts prognosis.
6. Who qualifies for lung cancer screening?
Adults aged 50-80 with at least 20 pack-years of smoking history who currently smoke or quit within the past 15 years qualify for annual low-dose CT screening. Medicare covers screening with minimal copay after a counseling visit.
7. How long is recovery after stage 1 lung cancer surgery?
VATS minimally invasive surgery requires 4-6 weeks recovery with most patients returning to desk work by week 6-8. Full recovery including exercise resumption typically occurs within 3 months, compared to 8-12 weeks for open surgery.
8. What is the recurrence rate for stage 1 lung cancer?
Stage 1 lung cancer recurs in 24-26% of patients, with most recurrences happening within the first two years post-surgery. Quitting smoking after treatment reduces recurrence risk by 48% and significantly improves overall survival.
9. Does Medicare cover lung cancer screening?
Yes, Medicare Part B covers annual low-dose CT lung cancer screening for eligible beneficiaries aged 50-77 with 20+ pack-year smoking history. After meeting your $240 annual deductible, you typically pay 20% coinsurance ($0-$60 per scan).
10. What is VATS surgery for lung cancer?
Video-assisted thoracoscopic surgery (VATS) uses 3-5 small incisions and a camera to remove lung tumors instead of large chest-opening incisions. VATS reduces mortality by 21% compared to open surgery while achieving identical cancer cure rates.
11. Can you have stage 1 lung cancer with no symptoms?
Absolutely—54-60% of stage 1 lung cancer patients are completely asymptomatic at diagnosis. This is why screening is critical for high-risk individuals, as waiting for symptoms to appear often means missing the most curable stage.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.