On This Page – Quick Medical Summary
If you searched this question, you are probably frightened, and you want a straight answer. Here it is, honestly: pancreatic cancer grows on two very different clocks. At the cellular level it usually develops slowly, often over a decade or more — but it is typically found late and can move quickly once detected, which is why it feels so fast.
Where you are matters, so this guide takes you straight to what you need. If you or someone you love was just diagnosed, the section on what growth speed means for the outlook will help most. If you are here because of a symptom, the parts on why this cancer is missed and which warning signs deserve quick attention are written for you. If you have a family history, there is a section on risk. And if you came for the numbers, they are all here, each tied to its source.
We will not give you false comfort, and we will not feed your fear.
ℹ️ Medical Disclaimer: This article is general health education, not medical advice, and does not diagnose disease, recommend treatment, or replace care from a qualified professional. Survival statistics describe groups of people, not your individual situation. For any diagnosis, staging, prognosis, screening decision, or symptom that worries you, consult a board-certified oncologist, gastroenterologist, or your primary care physician.
What “growth” actually means for pancreatic cancer
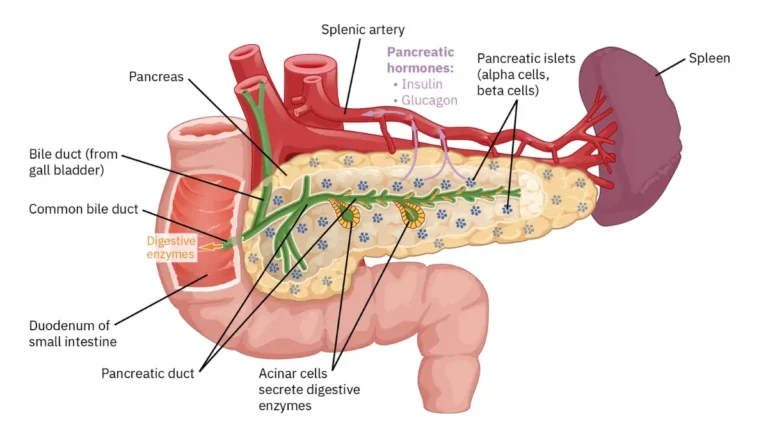
When people ask how fast pancreatic cancer grows, they are really asking two questions at once: how quickly do the cancer cells multiply, and how quickly does the disease become dangerous. Those are not the same thing, and separating them is the key to an honest answer.

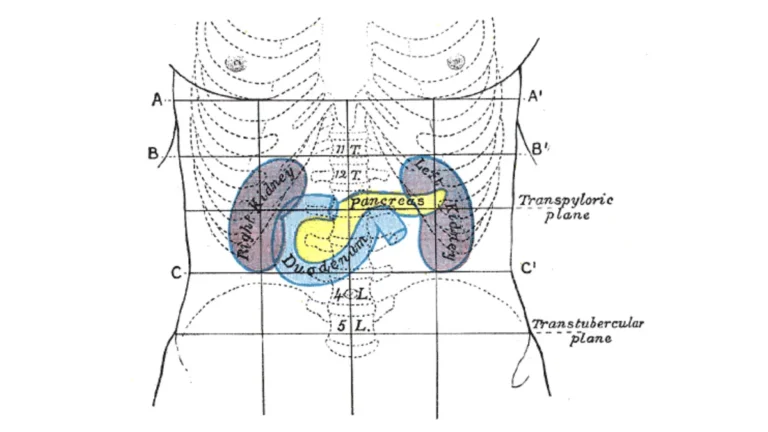
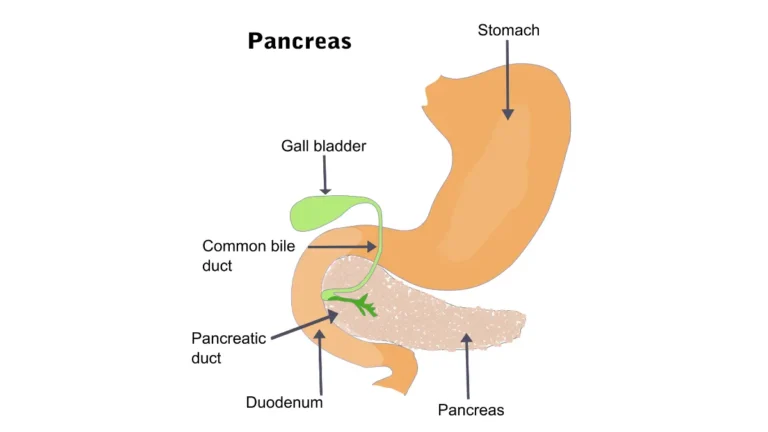
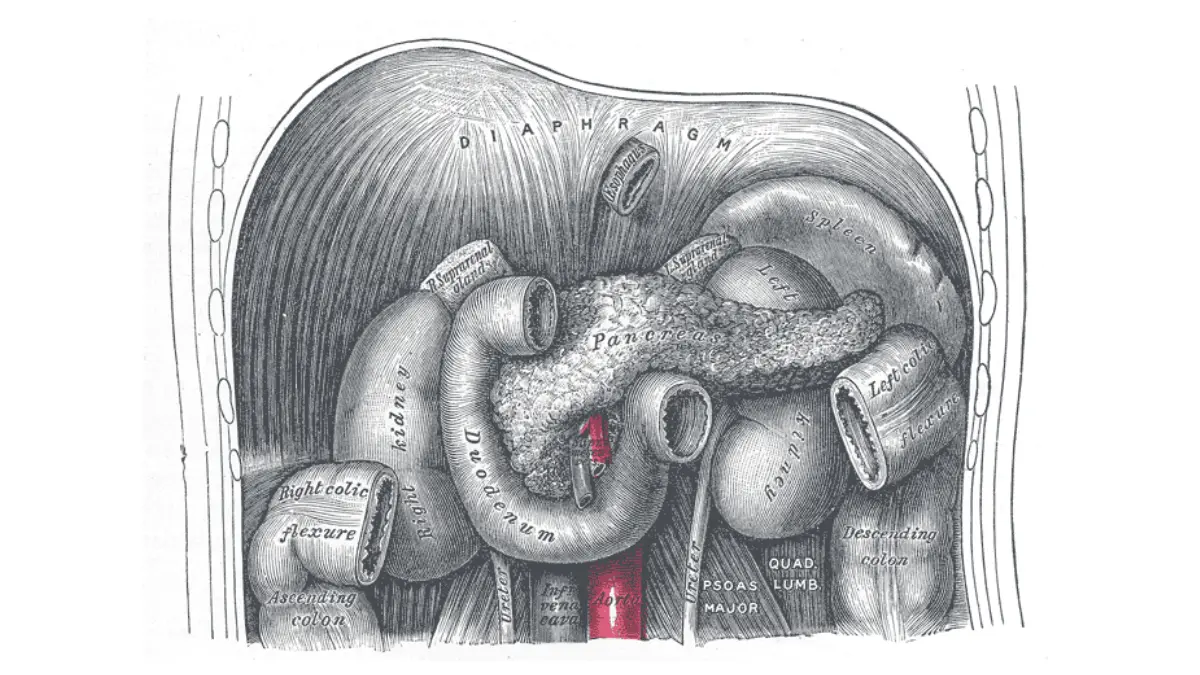
Adapted from Wikimedia Commons Pancreas 2.png, licensed under CC BY-SA 3.0.
Ductal adenocarcinoma versus neuroendocrine tumors
More than nine in ten pancreatic cancers are pancreatic ductal adenocarcinoma, or PDAC — the aggressive form most people mean by the term. A smaller share are pancreatic neuroendocrine tumors (PNETs), which often grow far more slowly and carry a very different outlook. Most pages blur these together, but the distinction genuinely changes what “fast” means.
Why “fast” usually describes the clinical course
PDAC cells do not divide dramatically faster than other cancers. What makes it feel explosive is that it is usually discovered late and tends to spread early, so the time from diagnosis to advanced disease is often short. The speed you experience is mostly about when it is caught — not unusually rapid cell division.
🔬 How It Works: Pancreatic tumors invade nearby veins earlier in their course than most other cancers. This early access to the bloodstream is one reason cells can seed distant sites while the primary tumor is still small and silent.
How fast does pancreatic cancer grow? What the data shows
Pancreatic cancer grows on two timescales: a long, silent molecular phase measured in years, and a faster clinical phase measured in months once a tumor is large enough to find. Both are real, and both come from published research.
The slow part: years before it can be detected
A landmark genomic study reconstructed how these tumors actually develop over time, drawing on a study that sequenced primary tumors and their metastases.
📊 Clinical Data Point: Researchers estimated roughly 11.7 years from the first cancer-causing mutation to a founding tumor cell, about 6.8 more years to develop the ability to spread, and around 2.7 more years to death — close to two decades at the cellular level. Source: Yachida et al., Nature, 2010.
🔬 How It Works: A tumor about one centimeter across already contains roughly one billion cells, which takes many doublings to reach. Only a few more doublings are needed to progress from there into advanced disease — so most of the growth happens silently, before anything is detectable.
The faster part: doubling time once it can be seen
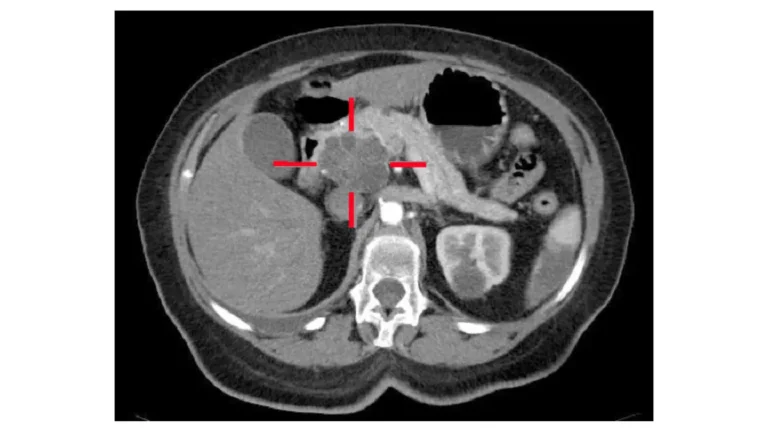
Once a tumor is visible on a scan, its growth can be measured. In untreated patients followed with serial CT imaging over time, the pace becomes clearer.
📊 Clinical Data Point: Primary pancreatic tumors had a median volume-doubling time of about 144 days (mean 159, range 64–255). In advanced disease, tumor-marker estimates put doubling as fast as roughly 40–60 days. Source: Furukawa et al., 2001; progression analysis, 2015.
Size and the jump to spreading
Growth matters most because of what it unlocks — the ability to spread to distant organs. Computational modeling suggests the risk of metastasis rises steeply with size, from roughly 28% at one centimeter to about 94% at three. That is why catching it while small is everything, and why advanced, distant disease carries such a different outlook.
✅ Patient Action: Ask your medical oncologist what stage and growth pattern your specific tumor shows, and whether its size and location make surgery possible.
Why pancreatic cancer is usually found late
If pancreatic cancer grows silently for years, why isn’t it caught earlier? The answer is a mix of where the pancreas sits, how vague the early signs are, and the lack of a routine screening test for most people.
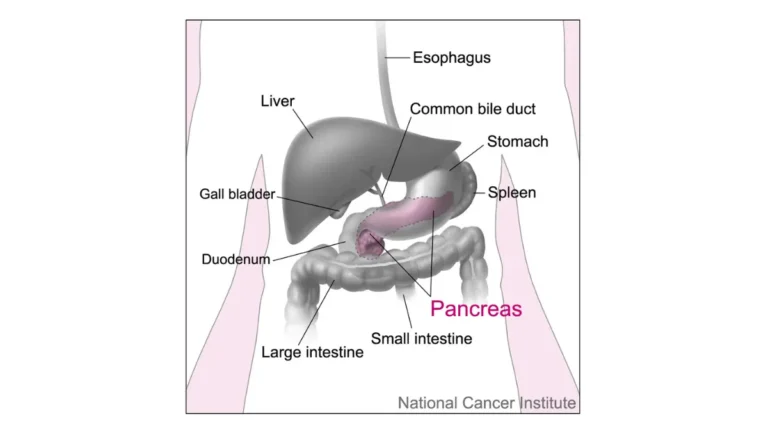
A hidden organ and quiet early symptoms
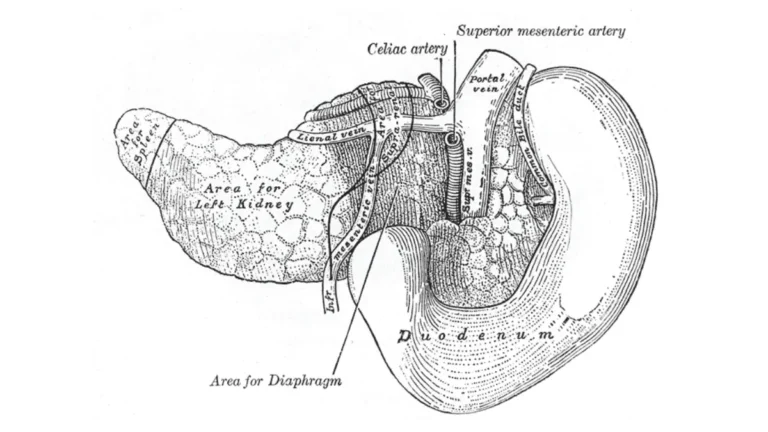
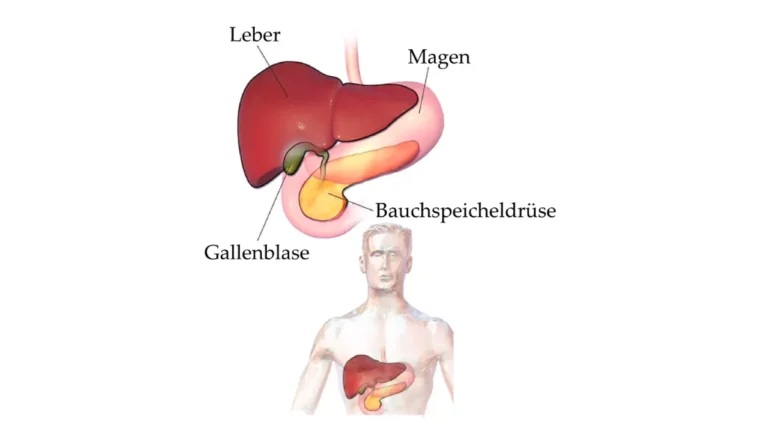
The pancreas lies deep in the abdomen, behind the stomach, where a small tumor causes no pressure and no obvious symptom. Early signs — mild back or belly discomfort, appetite changes, gradual weight loss — are easy to attribute to something else, which is part of why the early symptoms are so easy to miss.
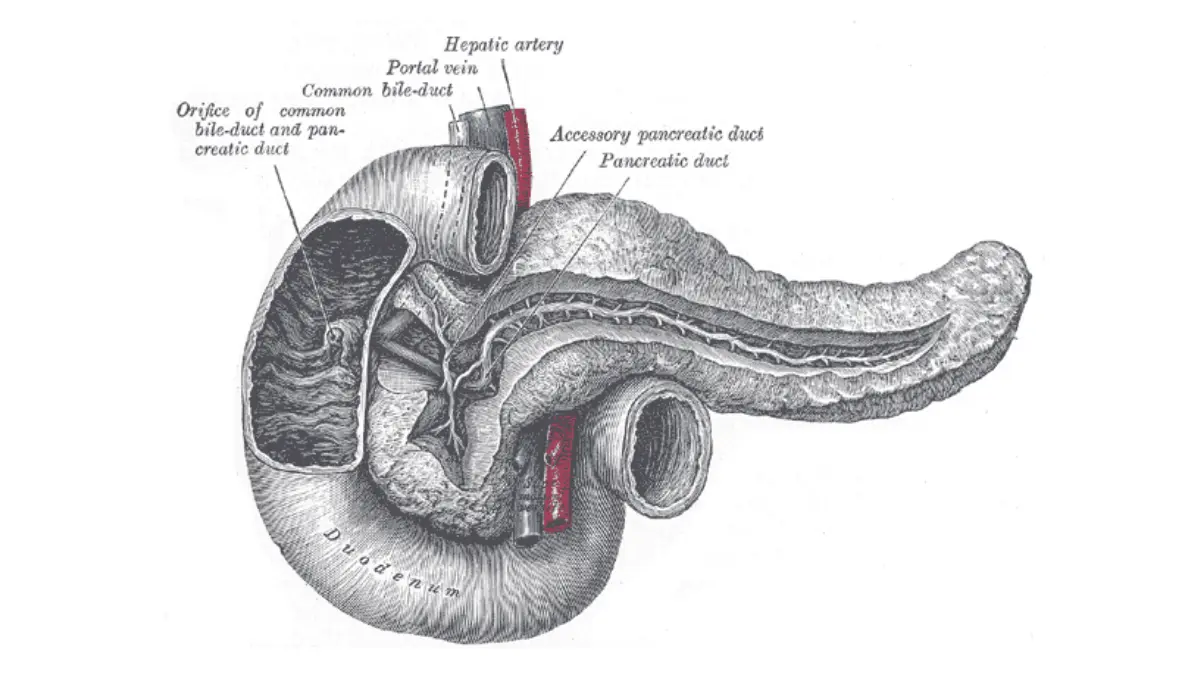
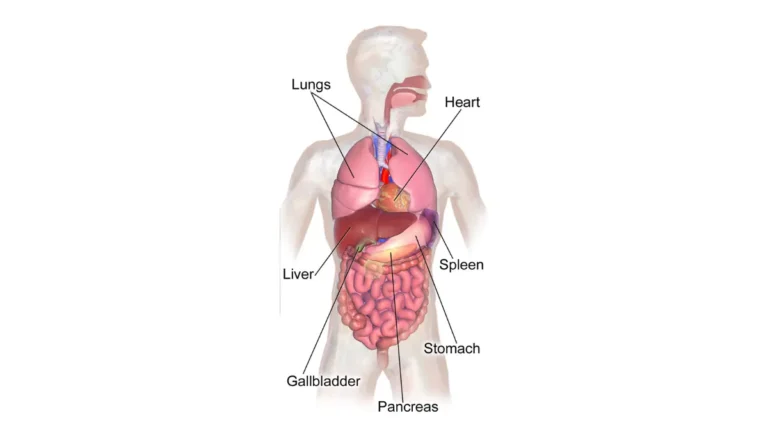
Adapted from Wikimedia Commons Gray1100.png, licensed under Public Domain.
📊 Clinical Data Point: Only about 15% of pancreatic cancers are found while still confined to the pancreas; most are regional or distant at diagnosis. Source: NCI SEER.
No routine screening for average-risk adults
There is no recommended screening test for pancreatic cancer in people at average risk — nothing like a mammogram or colonoscopy. That is a major reason it is usually advanced when found, and it is why knowing your personal risk matters. A general symptom checker can help you organize what to raise with a clinician, but it is educational, not diagnostic.
🩺 Physician Note: A common point of confusion is assuming that because there is no screening test, nothing can be done. For people at high inherited risk, specialists do offer surveillance — the issue is that it is not appropriate or available for everyone.
Does growth speed change the outlook?
Growth speed influences the outlook, but the single biggest factor is how far the cancer has spread when it is found. Stage at diagnosis shapes whether surgery — the main path to long-term survival — is even possible.
Why stage at diagnosis matters more than raw speed
A faster-growing tumor is generally associated with a worse course, but two people with the same growth rate can have very different outlooks depending on how the cancer is staged. Whether a tumor can be removed surgically often matters more than its speed.
Current survival by stage
These figures describe groups of people diagnosed in the past, not your personal odds — read them with that in mind, alongside the American Cancer Society’s stage-based survival data.
📊 Clinical Data Point: Five-year relative survival is about 44% when pancreatic cancer is localized, 17% when regional, 3% when distant, and 13% across all stages combined. Source: American Cancer Society, 2026 (SEER 2015–2021).
What this means for acting quickly
The steep drop between localized and distant survival is the real argument for moving quickly — earlier detection means more people are eligible for surgery. Tumor markers like the CA 19-9 blood test can add information, but they do not replace staging.
⚠️ Clinical Warning: Do not use these population statistics to predict your own outcome or to make treatment decisions alone. Stage, tumor biology, overall health, and response to treatment all change the picture for an individual.
✅ Patient Action: Ask your surgical or medical oncologist directly — is my cancer resectable, and how do my stage and CA 19-9 level affect my treatment options?
Who is at higher risk — and the early-detection window
The long silent phase is mostly bad news, but it points to one genuine opportunity: people at higher-than-average risk may qualify for surveillance that can catch tumors earlier, inside that window.
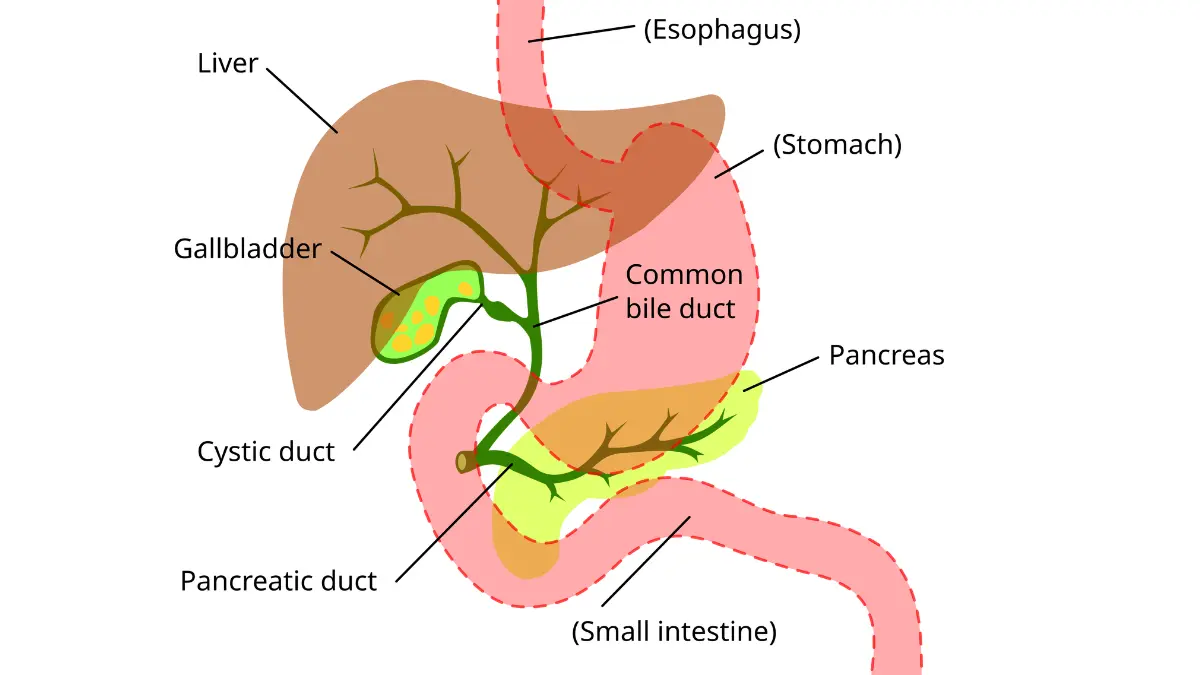
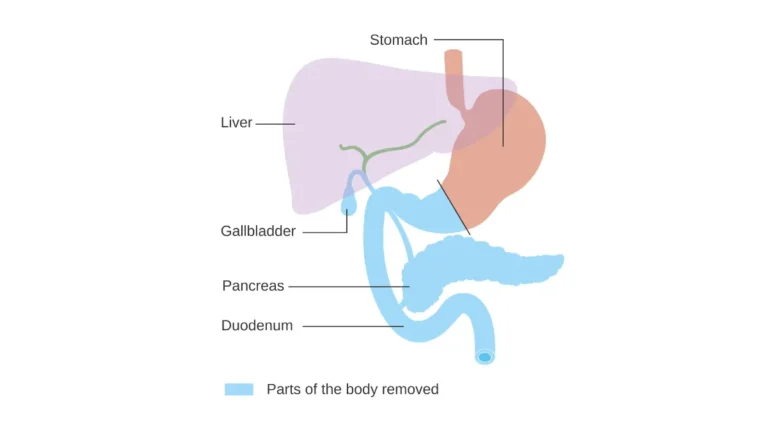
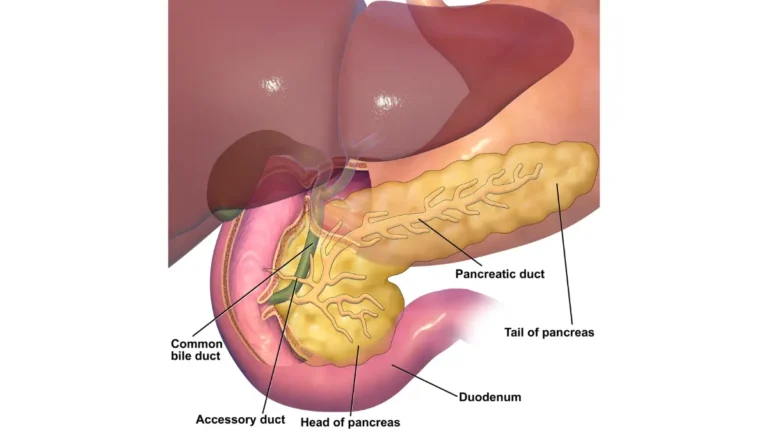
Adapted from Wikimedia Commons Digestive_system_showing_bile_duct.svg, licensed under CC BY-SA 4.0.
Inherited and family-history risks
Risk is elevated by certain inherited conditions and a strong family history. These include BRCA2 and related mutations, Lynch syndrome, familial atypical multiple mole melanoma (CDKN2A), Peutz-Jeghers syndrome, and hereditary pancreatitis, along with having several close relatives affected. A genetic risk assessment can help you organize your family history before a counseling visit. New-onset diabetes after age 50 can also, occasionally, be an early sign rather than a cause — a link explored in new-onset diabetes and pancreatic cancer.
When surveillance is recommended
For people at defined high risk, specialists may recommend surveillance with endoscopic ultrasound or MRI — but this is not recommended for the general public, as the national incidence figures help put in context.
📊 Clinical Data Point: Pancreatic cancer accounts for roughly 3% of new US cancer cases but ranks among the leading causes of cancer death — about 67,500 new diagnoses are expected in 2026. Source: American Cancer Society, 2026.
🩺 Physician Note: Current guidance reserves pancreatic surveillance for high-risk individuals identified through genetics or family history. If that describes you, a genetic counselor or gastroenterologist can help build a plan.
Warning signs that mean you should act quickly
Because this cancer is usually found late, recognizing the signs that deserve prompt attention can matter. None of these symptoms proves cancer — most have far more common, harmless causes — but when they are persistent or appear together, they are worth checking quickly.
Symptoms that warrant prompt evaluation
See a clinician promptly if you notice:
- Painless jaundice — yellowing of the eyes or skin, often with dark urine or pale stools, a sign explained in jaundice and pancreatic cancer
- Unexplained weight loss without trying
- New, persistent pain in the upper abdomen or mid-back, in the pattern this cancer often follows
- New-onset diabetes appearing without an obvious cause, especially after age 50
What to do and who to see
These are reasons to get evaluated, not to self-diagnose. Start with your primary care physician, who can order initial tests and refer you to a gastroenterologist or oncologist if needed.
⚠️ Clinical Warning: Painless jaundice in an adult should never be ignored — it warrants prompt medical evaluation, even though many causes are not cancer. Do not wait for it to clear on its own.
✅ Patient Action: If you have painless jaundice, or unexplained weight loss with new back pain, contact your primary care physician this week and ask specifically about pancreatic and biliary causes.
Frequently asked questions about pancreatic cancer growth
1. How fast does pancreatic cancer grow?
Pancreatic cancer grows on two timescales. At the cellular level it develops slowly — roughly two decades from the first mutation to advanced disease. Once a tumor is large enough to detect, growth is faster, with a median doubling time near 144 days. It feels rapid mainly because it is usually found late.
2. Is pancreatic cancer always fast-growing?
No. More than 90% of cases are pancreatic ductal adenocarcinoma, the aggressive form. A smaller share are pancreatic neuroendocrine tumors, which often grow much more slowly and carry a different outlook. The growth speed of pancreatic cancer depends heavily on which type it is, so confirm the specific diagnosis with your care team.
3. How long can pancreatic cancer go undetected?
Often for years. Genomic research estimates roughly 11 to 15 years pass between the first cancer-causing mutation and the point where a tumor gains the ability to spread. Because the pancreas sits deep in the abdomen and early symptoms are vague, pancreatic cancer is usually undetectable, and unnoticed, for most of that time.
4. How quickly can pancreatic cancer spread to the liver?
Pancreatic cancer tends to spread early, and the risk rises sharply with tumor size — modeling suggests it climbs from about 28% at one centimeter to roughly 94% at three. The liver is a common first site. This is why finding pancreatic cancer while small matters so much for outcomes.
5. What is the doubling time of pancreatic cancer?
In untreated patients followed by CT, primary tumors had a median volume-doubling time of about 144 days, ranging from 64 to 255. In advanced disease, tumor-marker estimates suggest faster doubling, around 40 to 60 days. Doubling time for pancreatic cancer varies widely between individuals and tumor types.
6. Does a faster-growing tumor mean a worse prognosis?
Generally yes — faster growth is associated with a worse course. But stage at diagnosis matters more. Two tumors growing at the same rate can have very different outlooks depending on whether the cancer is localized or has already spread. Discuss your specific prognosis with your oncologist.
7. How fast does stage 1 pancreatic cancer progress?
It varies, and the key factor is whether the tumor can be removed before it spreads. Because the risk of spread rises steeply with size, a small stage 1 pancreatic cancer caught and treated early offers the best chance. Your surgical oncologist can assess whether your tumor is resectable.
8. Can pancreatic cancer grow in a few weeks?
Measurable change over weeks is possible in advanced disease, where doubling times can be as short as 40 to 60 days. But most growth happens slowly and silently over years before detection. A few weeks rarely transforms an early tumor, though pancreatic cancer can progress quickly once it is advanced.
9. Why is pancreatic cancer found so late?
The pancreas sits deep in the abdomen, so small tumors cause no symptoms. Early signs like back pain or weight loss are easily mistaken for other problems. And there is no routine screening test for average-risk adults, so pancreatic cancer is usually advanced by the time it is diagnosed.
10. Who should be screened for pancreatic cancer?
Routine screening is not recommended for average-risk adults. Surveillance with endoscopic ultrasound or MRI is offered only to people at high inherited risk — for example, certain BRCA2 or Lynch syndrome carriers, or those with a strong family history. A genetic counselor can help assess whether pancreatic cancer surveillance fits your situation.
11. What warning signs mean I should act quickly?
Painless jaundice, unexplained weight loss, new and persistent upper-abdominal or mid-back pain, and new-onset diabetes without a clear cause all warrant prompt evaluation. None proves pancreatic cancer, but when persistent or combined they should be checked. See your primary care physician quickly and ask about pancreatic and biliary causes.
The honest bottom line
Pancreatic cancer grows on two clocks — quietly for years at the cellular level, then quickly once it is found, because it is so often caught late. That combination, not unusually fast cell division, is what earns it such a fearsome reputation. The most useful response is not panic but timing: prompt evaluation of worrying symptoms, and for those at high inherited risk, a real conversation about surveillance. If you are facing this, understanding how pancreatic cancer develops and is staged can help you prepare for the next conversation with your care team.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: Internal Medicine (2010); Clinical Pharmacology (2013) Experience: 15 years | Location: San Francisco, California Education: BS Molecular Biology, Caltech (2000); MD/PhD, UCSF School of Medicine (2007);…

Board Certifications: Preventive Medicine (2010); Public Health & General Preventive Medicine (2010) Experience: 15 years | Location: Washington, DC Education: BA Public Policy, Georgetown University (2001); MD, George…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.