On This Page – Quick Medical Summary
If you’ve landed here, you’re likely trying to answer one of two questions: is the pain I’m feeling a sign of pancreatic cancer, or I’ve been diagnosed — so why does it hurt where it does? This guide answers both, in plain language, with every fact tied to a named medical source.
Here’s how to find your part quickly. If you have new or persistent upper-abdominal or back pain and you’re worried, the sections on where the pain sits and how it differs from an ordinary sore back are for you. If you or someone you love was recently diagnosed, the sections on why the pain travels to the back and how it’s managed will help most. If you’re a caregiver, the management and warning-sign sections give you concrete things to watch for and ask about.
One honest starting point: most upper-abdominal and back pain is not pancreatic cancer. But pain that is persistent and unexplained deserves attention. The short answer on pancreatic cancer pain location is that it usually sits in the upper abdomen and often radiates straight through to the mid-back — and there’s a clear anatomical reason, which the rest of this guide explains alongside the full picture of pancreatic cancer symptoms and stages.
ℹ️ Medical Disclaimer: This article is general education about pancreatic cancer symptoms and pain. It is not a substitute for professional medical advice, diagnosis, or treatment, and it does not diagnose any condition, recommend specific medications or doses, or replace evaluation by a qualified clinician. Decisions about pain, imaging, medication, and procedures such as a nerve block should be made with a board-certified physician — a gastroenterologist, medical oncologist, or pain-medicine specialist — who knows your full history. If your symptoms are severe or worsening, or you develop yellowing of the skin or eyes, seek prompt medical care.
Where pancreatic cancer pain is usually felt
Pancreatic cancer pain is felt most often in the upper-middle abdomen — below the breastbone and above the navel, the area clinicians call the epigastric region — and it commonly radiates straight through to the mid-back.
Pain in the upper abdomen
The pancreas sits deep in the upper belly, so pain that originates there tends to feel deep and dull rather than sharp or surface-level. Many people describe a gnawing ache rather than a stabbing pain. According to the American Cancer Society, abdominal or back pain is common with pancreatic cancer, though it is far more often caused by something else.
Why it often wraps around to the back
A hallmark pattern is a band-like or belt-like ache that seems to wrap from the upper abdomen around to the mid-back, often described as running from one side of the back to the other. Some people feel it under the shoulder blades. Johns Hopkins Medicine notes that pain may begin in the middle of the abdomen and radiate into the back.
Where else it can show up
The location is not identical for everyone. Some people feel the ache mainly in the back, some mainly in the belly, and some report discomfort with no single, clear location at all. That variability is normal and is part of why this pain is easy to mistake for other problems.
Why pancreatic cancer pain reaches the back
Pancreatic cancer causes back pain because the pancreas sits deep in the upper abdomen, just in front of the spine, and tumors there tend to grow into and irritate the nerves that carry pain signals toward the back.
The pancreas sits deep, near the spine and major nerves
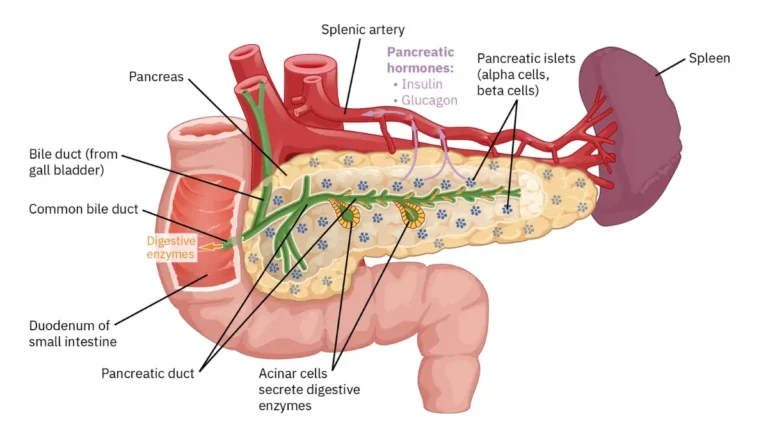
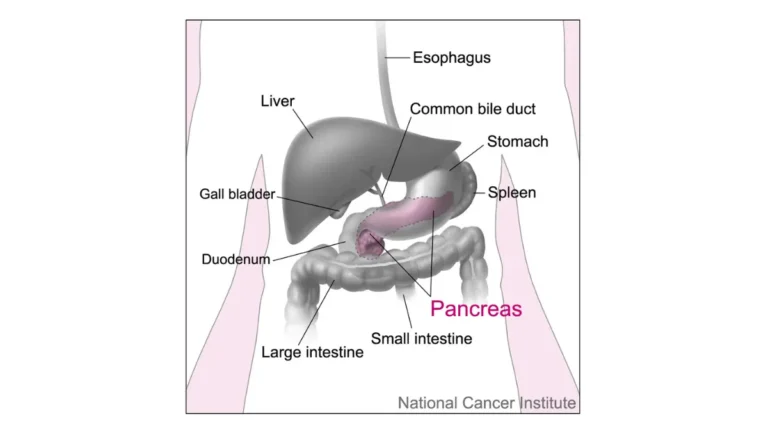
The pancreas is a retroperitoneal organ — it lies behind the stomach, crossing the midline, close to the spinal column and to a dense bundle of nerves. Because it sits so far back, a growing tumor can press toward the spine and the surrounding nerve network, which is why the back is so often involved.
How the tumor irritates nerves (perineural invasion)
Pancreatic tumors have a strong tendency to grow along and into nearby nerves, a process called perineural invasion. This nerve involvement is a major reason the pain can be persistent and is often described as a deep, neuropathic (nerve-type) ache rather than a simple muscular soreness.
📊 Clinical Data Point: Perineural invasion — cancer growing into surrounding nerves — is reported in roughly 80–100% of pancreatic cancers across published surgical series. Source: Journal of Pancreatology, review of pancreatic cancer-related pain (2021).
Referred pain — why the brain misreads the location
Internal organs don’t have the precise location “mapping” that skin and muscle do, and the organs and the back share overlapping nerve pathways. So when nerves near the pancreas are irritated, the brain can interpret the signal as coming from the back — a phenomenon called referred pain.
🔬 How It Works: Pain signals from the pancreas travel along nerves that pass through the celiac plexus, a control-center bundle of nerves sitting behind the pancreas, and continue up the splanchnic nerves to the spinal cord and brain. Because those nerves enter the spine at the same levels that serve the mid-back, the brain often “places” the pain in the back even though the source is the pancreas. This shared wiring — plus the tumor’s tendency to invade the nerves directly — is why upper-abdominal and back pain so often occur together here.
How pancreatic cancer pain differs from ordinary back pain
The most useful question is rarely “where exactly does it hurt?” but “how is this pain behaving?” Several features can help separate a likely muscle or joint problem from pain that deserves a closer look.
What the pain tends to feel like
Pancreatic pain is usually a deep, dull, gnawing ache rather than a sharp, localized twinge. It may be worse after eating or when lying flat, and some people find it eases when they lean or curl forward. It tends to build steadily over weeks rather than flaring and settling with activity.
🩺 Physician Note: The pattern of pain that worsens lying down and improves when leaning forward is a recognized clinical clue for pancreatic pain, because position changes alter pressure on the structures behind the pancreas. It does not confirm cancer — but combined with persistence and other symptoms, it’s a pattern worth raising with a clinician.
Clues that point away from a simple muscle strain
Ordinary mechanical back pain usually starts after a clear trigger — lifting, twisting, a bad night’s sleep — improves with rest, and responds to over-the-counter pain relief within days to weeks. Pain with no mechanical trigger that persists despite those measures is more notable.
| Feature | Ordinary (mechanical) back pain | Pancreatic-cancer pain | Key Clinical Detail |
|---|---|---|---|
| Onset | Often after lifting, twisting, or poor sleep | No clear injury; simply appears and stays | Pain with no mechanical trigger is more notable |
| Course over time | Flares, then eases with rest/activity | May come and go early; later tends to be steady and progressive | Steady worsening over weeks warrants evaluation |
| Position | Often eased by rest or lying down | Can worsen lying down; sometimes eased by leaning forward | The “leaning-forward relief” pattern is a known clue |
| Response to OTC relief | Usually responds to rest and OTC pain relievers | Tends to persist despite usual measures | Persistence despite self-care is a flag |
| Other symptoms | Usually occurs on its own | Often joined by weight loss, jaundice, appetite/digestive change, or new diabetes | The combination matters more than any single sign |
Source note: synthesized from American Cancer Society, Johns Hopkins Medicine, and Cancer Research UK descriptions of pancreatic cancer pain; mechanical-pain features per standard clinical guidance.
The signs that rarely appear alone
Pancreatic pain seldom shows up by itself. The combinations that matter most include pain plus unexplained weight loss, pain plus yellowing of the skin or eyes (jaundice), or pain alongside newly diagnosed diabetes. You can read more about other early warning signs of pancreatic cancer, and the American Cancer Society’s overview of pancreatic cancer signs is a reliable plain-language reference.
✅ Patient Action: If you’ve had unexplained upper-abdominal or back pain for more than a couple of weeks with any weight loss or appetite change, ask your primary-care physician directly: “Could this pain have a pancreatic cause, and do I need imaging such as a CT scan?”
Does the tumor’s location change where the pain is felt?
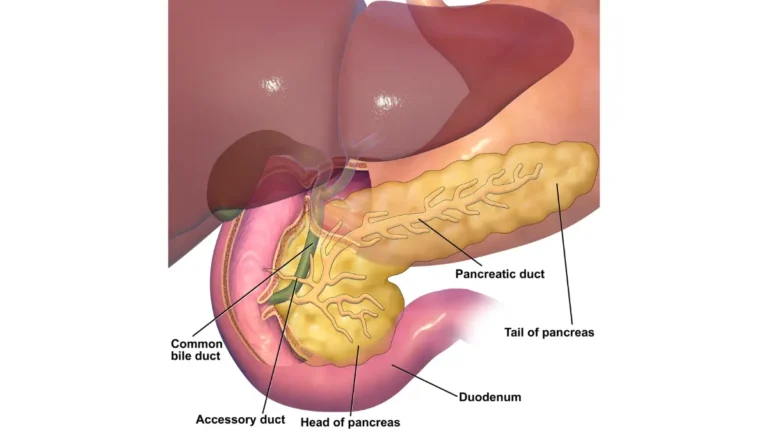
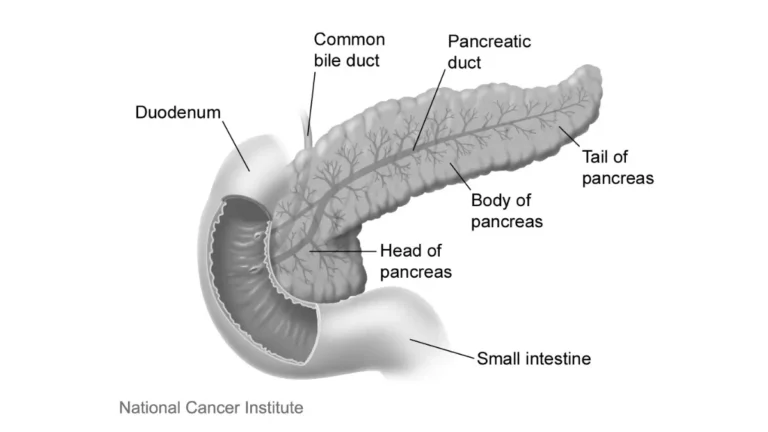
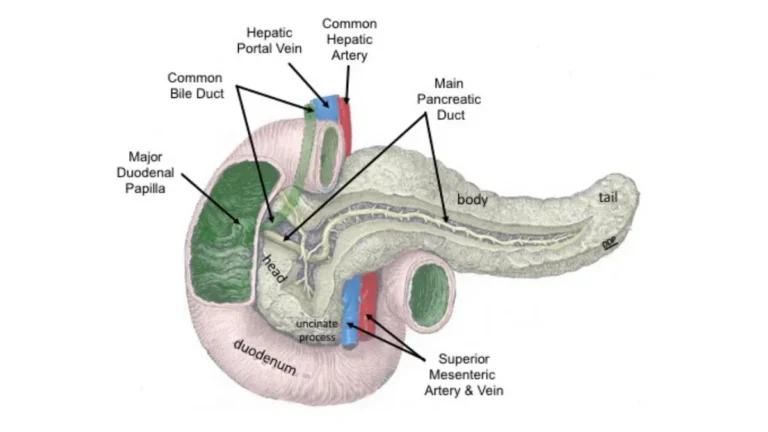
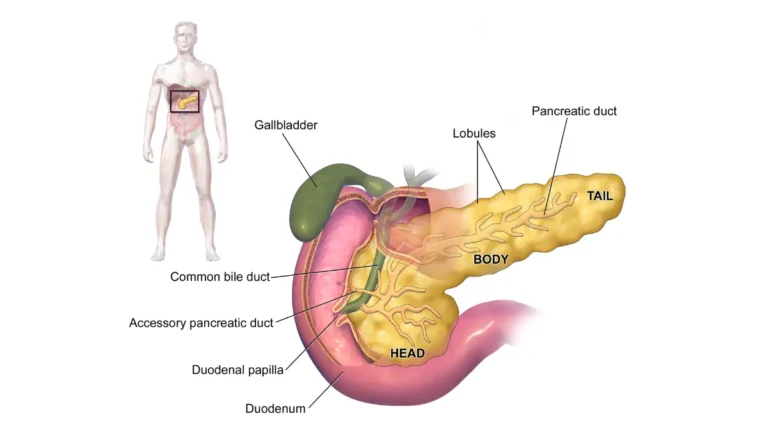
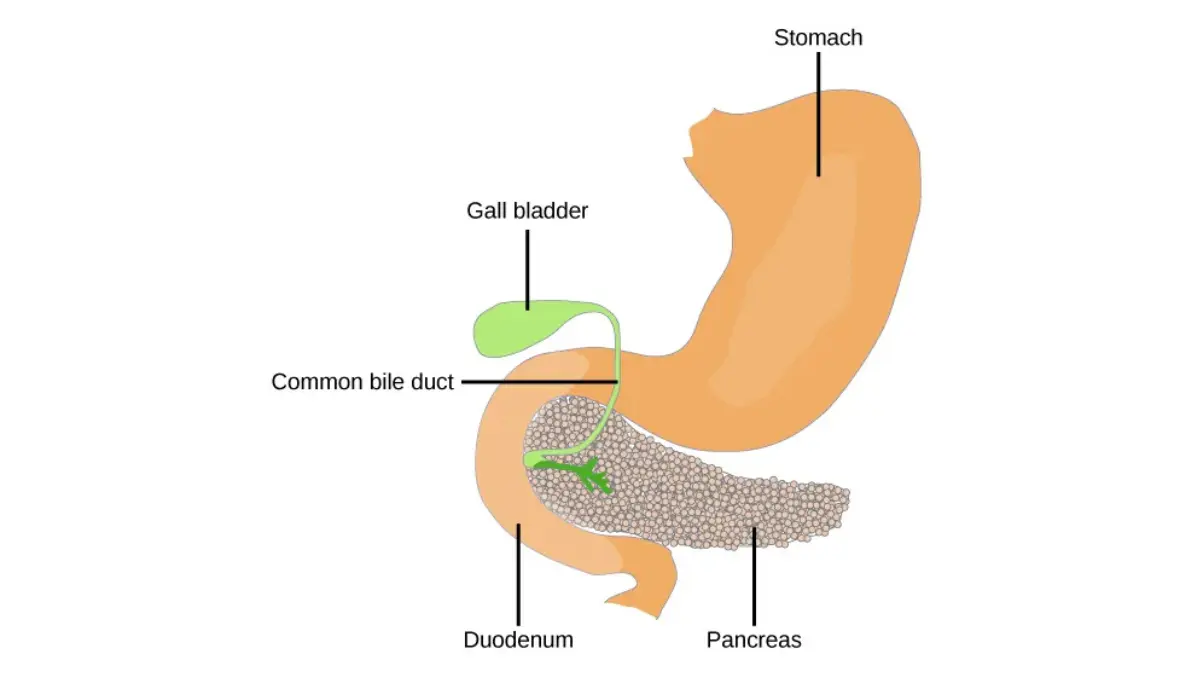
Where a tumor sits within the pancreas influences which symptoms appear first — and how much pain there tends to be. The pancreas has three parts: the head (on the right, where it meets the small intestine), the body (behind the stomach), and the tail (on the left, near the spleen).
Tumors in the head of the pancreas
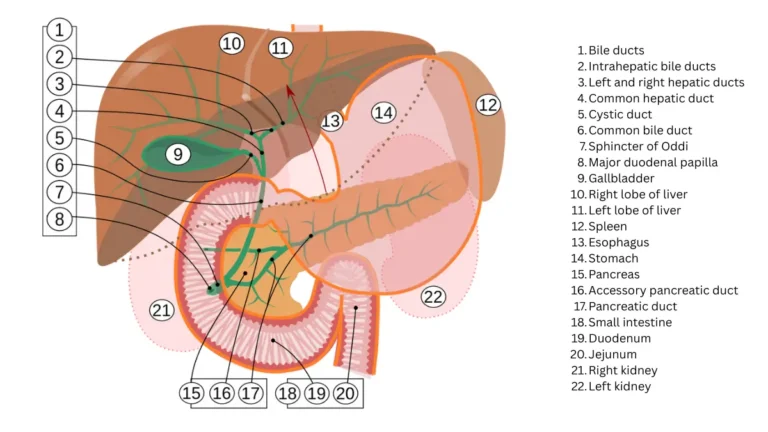
Tumors in the head of the pancreas often press on the nearby bile duct, which can cause jaundice — yellowing of the skin and eyes, dark urine, and pale stools — sometimes before pain becomes prominent. Because jaundice is hard to ignore, head tumors are occasionally found a little earlier.
Tumors in the body or tail
Tumors in the body or tail sit closer to the spine and have more room to grow before they obstruct anything obvious, so they more often present with pain and weight loss and can take longer to be found. Johns Hopkins Medicine notes that body or tail tumors can press toward the spine, contributing to back pain. You can see the full range of pancreatic cancer symptoms for how these patterns fit together.
How pancreatic cancer pain is managed
Pancreatic cancer pain can usually be controlled, and several approaches are used together: treating the tumor itself, pain medicines, nerve-targeted procedures, and supportive (palliative) care. This section is general education — the right plan is set by your own care team.
Treating the tumor and using pain medicine
Because the tumor is often the source of the pain, treatments aimed at it — chemotherapy, radiation, or surgery — can reduce pain as well. Pain medicines, including options for nerve-type pain, are tailored by a clinician. For pain that comes on after eating, prescription pancreatic enzymes sometimes help, which is a question for your team.
Celiac plexus block (a nerve block)
A celiac plexus block is a procedure that interrupts pain signals from the celiac nerves behind the pancreas. The National Cancer Institute notes that celiac-axis nerve blocks can provide effective, long-lasting pain control for some patients, and published reviews report meaningful relief and reduced opioid use in many people who have it.
🔬 How It Works: In a celiac plexus block, a clinician uses imaging or endoscopic guidance to reach the celiac plexus — the nerve bundle that relays pancreatic pain — and applies medication that quiets those nerves so they stop carrying pain messages to the brain. It targets the same nerve pathway described earlier, which is why it can help when standard pain medicines aren’t enough.
Supportive and palliative care
Supportive or palliative care — specialized help focused on symptoms and quality of life — is appropriate at any stage, not only late in the illness, and starting it early is associated with better quality of life. The NCI’s pancreatic cancer summary for patients and this review of celiac plexus block evidence are solid references to bring to an appointment.
✅ Patient Action: Ask your medical oncologist and a pain-medicine or palliative-care specialist: “Is a celiac plexus block appropriate for me, and what’s the plan if my current pain medicine isn’t controlling things?”
When pain means you should be checked promptly
Most upper-abdominal and back pain is not cancer — but certain combinations should be evaluated without delay. The point is not to alarm you; it’s to help you decide when “wait and see” isn’t the right call.
Combinations that warrant prompt evaluation
Seek medical evaluation soon if persistent upper-abdominal or back pain comes with any of these: yellowing of the skin or eyes, unexplained weight loss, a new diagnosis of diabetes, or ongoing nausea, appetite loss, or digestive changes. Pain that steadily worsens over weeks, or that wakes you from sleep, also deserves a look.
⚠️ Clinical Warning: Pain combined with jaundice (yellowing of the skin or eyes, dark urine, or pale stools) should be assessed urgently — jaundice is never normal and needs prompt medical attention to find the cause. The pairing of new back pain, unexplained weight loss, and newly diagnosed diabetes is also especially concerning and should be evaluated quickly.
What to do next
Start with your primary-care physician, who can examine you and arrange blood tests or imaging if needed. If you’re unsure whether your symptoms warrant a visit, you can check how your symptoms line up as a starting point — though only a clinician can diagnose the cause.
Pancreatic cancer pain: frequently asked questions
1. Where is pancreatic cancer pain usually located?
Pancreatic cancer pain location is typically the upper-middle abdomen, below the breastbone, and it often radiates straight through to the mid-back in a band-like pattern. Some people feel it under the shoulder blades, and some report no single clear spot. The deep, dull quality reflects how far back the pancreas sits.
2. Does pancreatic cancer pain radiate to the back?
Yes — radiating to the mid-back is one of the most common patterns of pancreatic cancer pain, often felt as a belt-like ache wrapping from the upper abdomen around to the back. It happens because the pancreas sits just in front of the spine and tumors there irritate nearby nerves.
3. Why does pancreatic cancer hurt in the back and not just the belly?
The pancreas lies deep in the abdomen, close to the spine and a major nerve bundle, and tumors tend to grow into those nerves. Because internal organs share nerve pathways with the back, the brain often interprets the signal as back pain — a phenomenon called referred pain.
4. What does pancreatic cancer back pain feel like?
It’s usually a deep, dull, gnawing ache rather than a sharp twinge, and it tends to be persistent and to build over weeks. It may be worse after eating or when lying down, and some people find it eases when leaning forward. It commonly appears alongside other symptoms.
5. Is pancreatic cancer pain constant or does it come and go?
Early on, the pain may come and go, which is part of why it’s easy to dismiss. Over time it more often becomes steady and progressive, sometimes severe enough to disturb sleep. A dull ache that keeps returning and slowly worsening over weeks is more concerning than a one-off flare.
6. Does the pain change depending on where the tumor is?
Yes. Tumors in the head of the pancreas often cause jaundice, sometimes before significant pain, while tumors in the body or tail sit closer to the spine and more often cause pain and weight loss. Location strongly influences which symptom appears first.
7. Is pancreatic cancer pain worse lying down or after eating?
It can be both. Many people notice the ache intensifies when lying flat and after meals, and that leaning or curling forward brings some relief. These position and meal-related patterns are recognized features, though they don’t by themselves confirm a pancreatic cause.
8. How is pancreatic cancer pain treated?
Pain is managed by treating the tumor (chemotherapy, radiation, or surgery), pain medicines tailored to nerve-type pain, a celiac plexus nerve block when appropriate, and supportive care, sometimes with pancreatic enzymes for post-meal pain. Your oncology and pain-management team should decide the specific plan for you.
9. What is a celiac plexus block?
It’s a procedure that quiets the celiac nerves behind the pancreas so they stop carrying pain signals to the brain, often using imaging or endoscopic guidance. The NCI notes it can give effective, long-lasting relief for some patients and may reduce the need for opioids. Ask your specialist whether it’s suitable for you.
10. When should back or abdominal pain be checked for cancer?
Have persistent or progressive upper-abdominal or back pain evaluated if it comes with jaundice, unexplained weight loss, new diabetes, or ongoing digestive symptoms — and seek urgent care for jaundice. Most such pain isn’t cancer, but these combinations warrant prompt assessment by a clinician.
11. Can you have pancreatic cancer with no pain?
Yes. Early pancreatic cancers often cause no symptoms at all, and pain may be absent until the tumor grows or affects nearby structures. That’s why other clues — jaundice, weight loss, new diabetes — matter, and why persistent unexplained changes are worth discussing with a clinician.
What to do with this
You now have the two answers most people come here for: pancreatic cancer pain is usually felt in the upper abdomen and radiates to the mid-back, and it reaches the back because the pancreas sits deep against the spine and its tumors grow into nearby nerves. You also have a sense of how this pain differs from an ordinary sore back, how it’s managed, and when a combination of symptoms means “get checked now.”
The most useful next step is rarely to worry alone. If your pain is persistent, unexplained, or paired with weight loss or jaundice, bring exactly that pattern to a clinician and ask whether imaging is warranted. Knowing where the pain comes from — and what to ask — puts you back in control.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: Internal Medicine (2010); Clinical Pharmacology (2013) Experience: 15 years | Location: San Francisco, California Education: BS Molecular Biology, Caltech (2000); MD/PhD, UCSF School of Medicine (2007);…

Board Certifications: Preventive Medicine (2010); Public Health & General Preventive Medicine (2010) Experience: 15 years | Location: Washington, DC Education: BA Public Policy, Georgetown University (2001); MD, George…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.