On This Page – Quick Medical Summary
If you’re reading this, you or someone you love has likely heard the words stage IV, advanced, or no longer curable — and you want an honest picture of what comes next. End-stage pancreatic cancer means the disease has spread beyond the pancreas, and the focus of care shifts from cure toward comfort and time.
This page is written for three readers. If you’re newly facing a stage IV diagnosis and want to understand the outlook, start with the next section; if you’re caring for someone whose symptoms are changing, the sections on symptom relief and palliative care are for you; and if you’re sitting with a loved one in their final days, you can go straight to what those days tend to look like.
None of this replaces your care team. But knowing what to expect can make a frightening time feel a little less unknown — you are not navigating this blindly, and you are not navigating it alone.
ℹ️ Medical Disclaimer: This article is general education, not medical advice for any individual. It does not diagnose disease, recommend treatment or medication, guide any procedure, or determine hospice or insurance eligibility. Survival statistics are population estimates and cannot predict one person’s course. Decisions about treatment, symptom relief, palliative care, and hospice belong with your oncology, palliative care, or hospice team. If a loved one is in uncontrolled pain or distress, contact your hospice or medical team right away.
What end-stage pancreatic cancer means
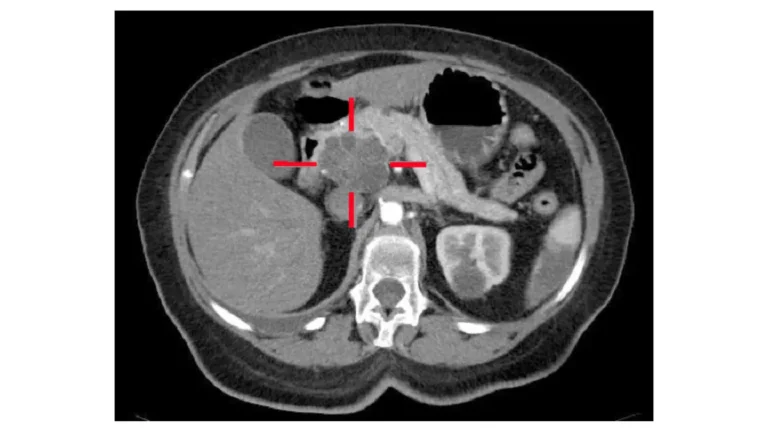
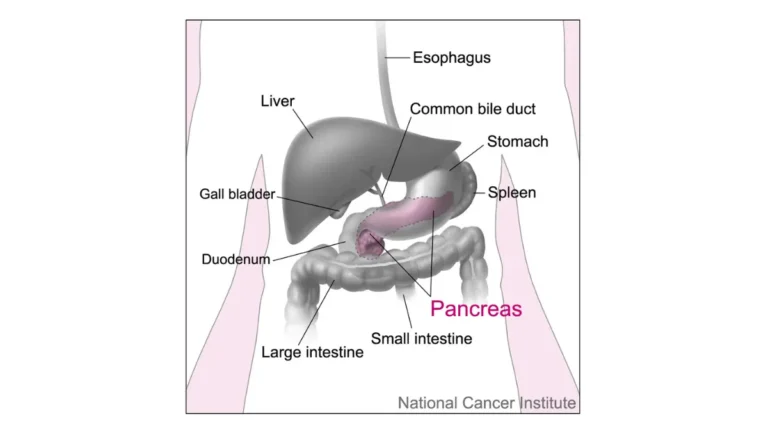
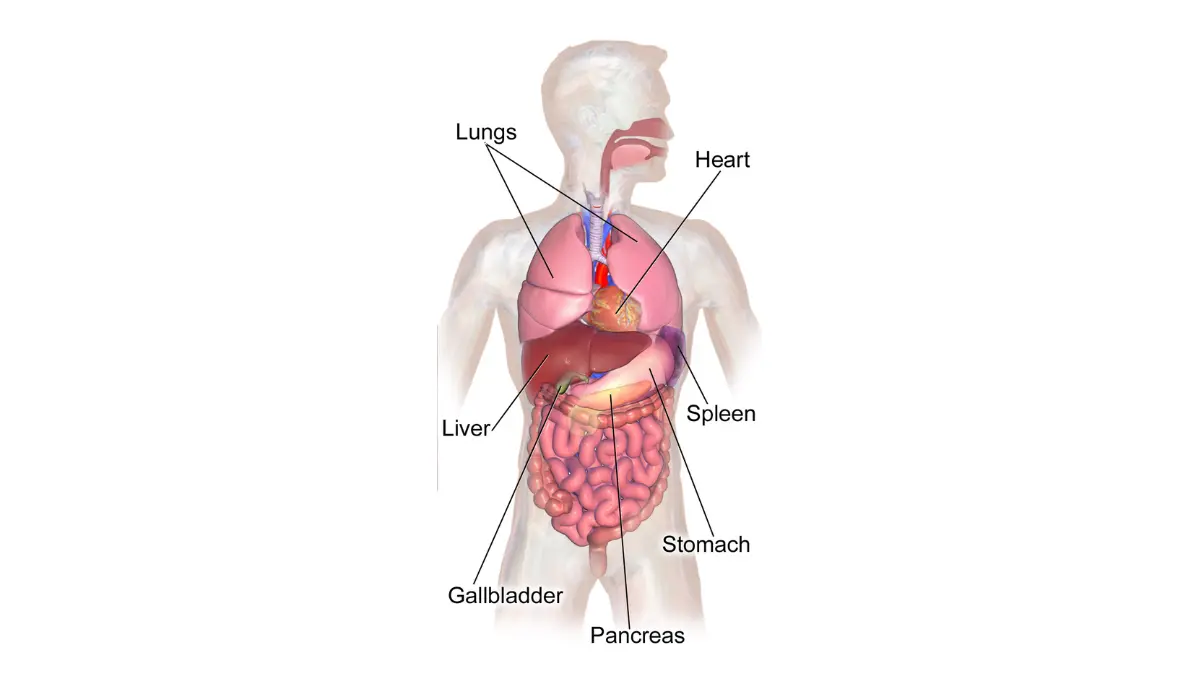
When clinicians call a cancer end-stage, they usually mean stage IV pancreatic cancer — the disease has metastasized beyond the pancreas to distant organs, most often the liver, the lungs, or the lining of the abdomen.
Stage IV and distant spread
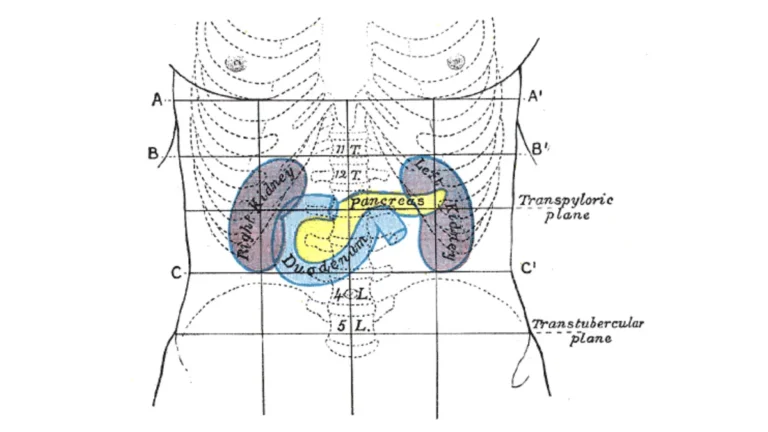
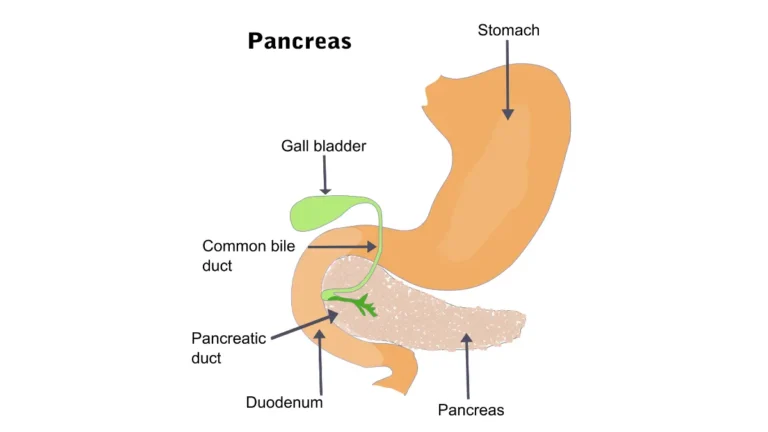
Pancreatic cancer is often found late because its early signs — fatigue, weight loss, vague abdominal or back discomfort — are easy to overlook, and there is no routine screening test for the general population. Understanding how pancreatic cancer is staged helps explain why “end-stage” and “stage IV” are often used to mean the same thing.
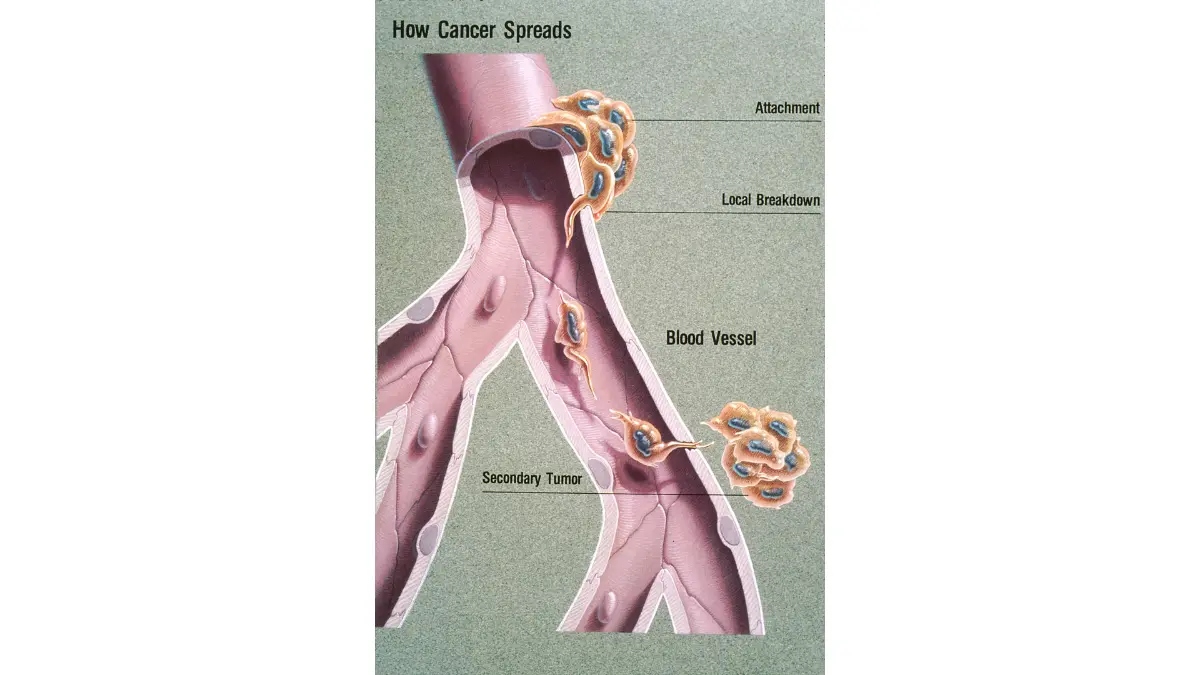
Adapted from Wikimedia Commons Metastasis Illustration, licensed under public domain.
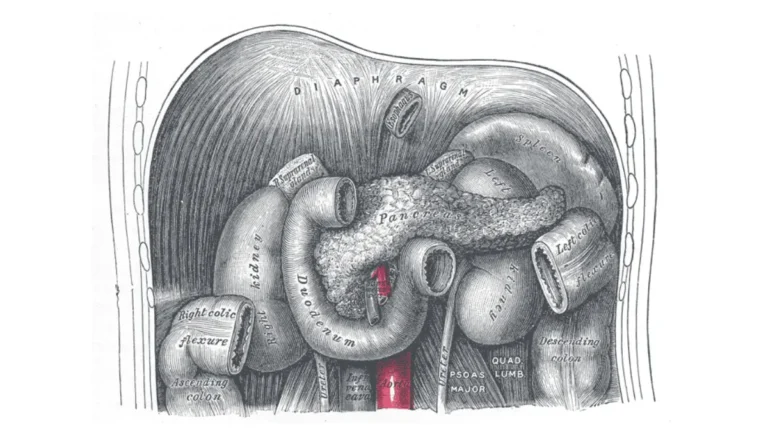
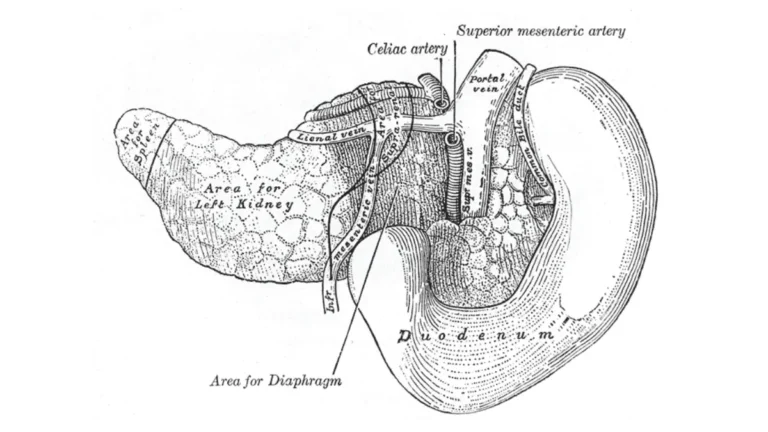
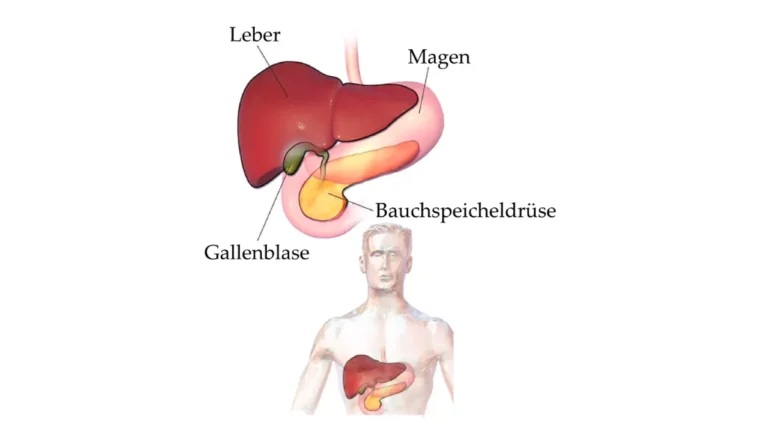
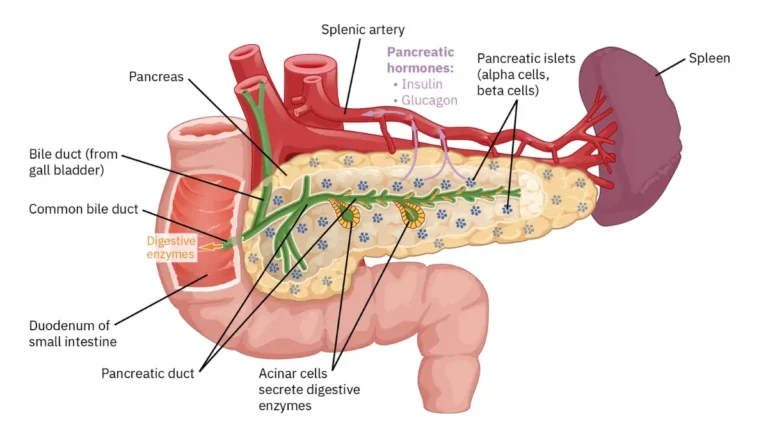
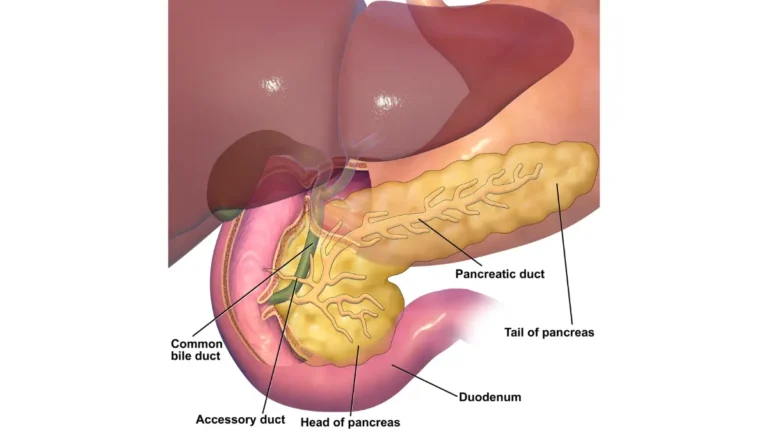
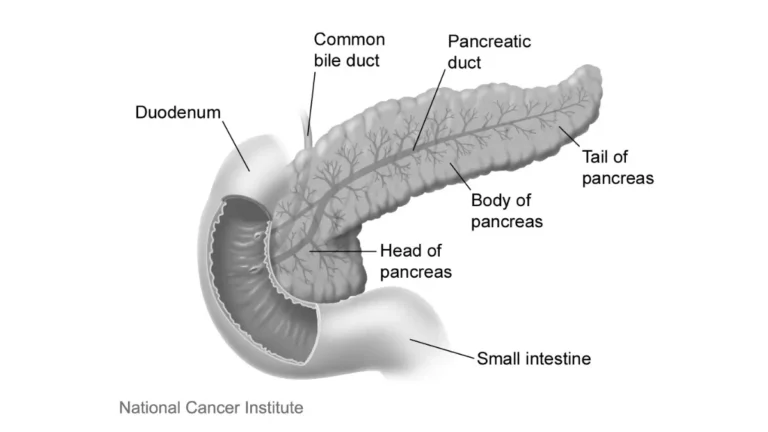
🔬 How It Works: The pancreas sits deep in the abdomen, behind the stomach. A tumor can grow there for months without obvious symptoms, which is why many cancers are diagnosed only after they have already spread to other organs.
What the survival statistics do — and don’t — tell you
For cancer that has spread to distant organs, the five-year relative survival rate is about 3%, based on the National Cancer Institute’s SEER data, compared with roughly 44% when the cancer is still confined to the pancreas.
📊 Clinical Data Point: Distant-stage pancreatic cancer — five-year relative survival ≈3% (vs ≈44% localized) — Source: NCI SEER Cancer Stat Facts, cases diagnosed 2015–2021.
These figures describe large groups of people diagnosed years ago — they are not a prediction or a deadline for any one person, a point the American Cancer Society’s stage-based figures also stress. Overall health, how the cancer responds, and supportive care all shape the time ahead; a closer look at what stage IV means for life expectancy can help you set expectations.
✅ Patient Action: Ask your oncologist what your specific scans, tumor markers, and overall health suggest about your individual situation — population statistics cannot predict one person’s course.
Common symptoms in the final stage
As pancreatic cancer advances, several symptoms tend to appear together — and nearly all of them can be eased, even when the cancer itself can no longer be cured.
Pain, jaundice, and digestive changes
Pain is one of the most common symptoms — clinical reviews report it affects the large majority of people with pancreatic cancer, often felt in the upper abdomen or radiating to the mid-back. Jaundice — a yellowing of the skin and eyes, with dark urine and pale stools — is also common, especially with tumors in the head of the pancreas.
🔬 How It Works: Jaundice develops when the tumor presses on or blocks the bile duct, so bilirubin (a yellow pigment the liver normally clears) builds up in the blood. You can read more about why pancreatic cancer causes jaundice and how it’s relieved.
Digestion often changes too, because the pancreas can no longer release enough enzymes — leading to greasy, pale stools, bloating, and poor absorption of food.
Ascites, weight loss, and fatigue
Other common features of advanced disease include:
- Ascites — fluid building up in the abdomen, causing swelling, tightness, and discomfort
- Cachexia — ongoing weight and muscle loss that happens even when a person is eating, driven by the cancer’s effect on metabolism
- Profound fatigue and increased sleep
- Nausea, early fullness, or bowel obstruction as the tumor affects the digestive tract
- Blood clots, which are more common in pancreatic cancer than in many other cancers
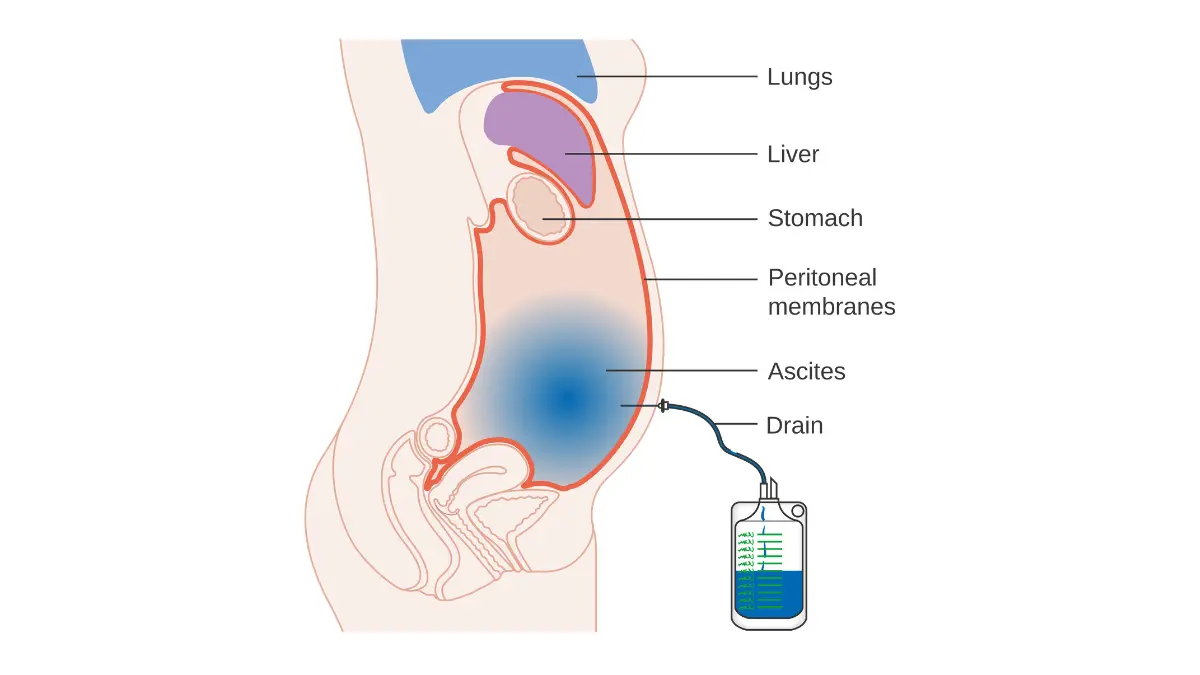
Adapted from Wikimedia Commons Diagram Showing Fluid (Ascites) Being Drained from the Abdomen CRUK 122, licensed under CC BY-SA 4.0.
✅ Patient Action: Report any new or worsening symptom to the palliative care team early — most, including pain, jaundice, and ascites, can be managed before they become severe.
How symptoms and pain are managed
Comfort at this stage is not only possible — it is the central goal of care, and there are well-established ways to relieve nearly every symptom above.
Controlling pain
Pain is treated in steps, usually starting with medication managed by the care team. When pain is hard to control, a celiac plexus block is a procedure that can bring lasting relief.
🔬 How It Works: A celiac plexus block interrupts the bundle of nerves around the pancreas that carry pain signals, using an injection to quiet them — often reducing the amount of pain medication a person needs. The pattern and location of pancreatic cancer pain helps the team decide whether this option fits.
⚠️ Clinical Warning: Severe pancreatic cancer pain should never be managed alone at home. Uncontrolled pain is a signal to contact the palliative or hospice team the same day, because it can almost always be brought down with the right plan.
Easing jaundice, ascites, and digestion
Jaundice from a blocked bile duct is often relieved with a small stent placed during an endoscopic procedure. Ascites can be drained for comfort through paracentesis, though the fluid may slowly return and need repeating. Digestive problems from low enzyme levels are eased with pancreatic enzyme replacement taken with meals.
✅ Patient Action: Ask your oncologist for a referral to palliative care, and ask specifically about a nerve block if pain is difficult to control.
When to consider palliative care and hospice
Two kinds of supportive care matter most at this stage, and they are not the same thing — knowing the difference helps families ask for the right help at the right time.
Palliative care vs. hospice
Palliative care focuses on comfort and quality of life, and it can be given at any stage, alongside treatments meant to control the cancer. Hospice care is for when the focus shifts fully to comfort — generally when a clinician estimates a prognosis of around six months — and it provides medical, emotional, and spiritual support for both the patient and the family.
🩺 Physician Note: Current oncology guidance emphasizes that palliative care started early — not only at the very end — improves quality of life and helps families plan. Choosing comfort-focused care is not giving up; it is a deliberate choice about how to spend the time ahead.
Knowing when it’s time — and what hospice provides
For families still weighing options, it can help to revisit whether the cancer can be removed or treated before shifting focus. When the goal becomes comfort, hospice brings a team — nurses, aides, social workers, and chaplains — to wherever the person lives, and hospice care from the NCI explains how it works.
✅ Patient Action: Ask your oncologist directly whether hospice is appropriate now, and how to begin it — many families later wish they had started sooner.
What to expect in the final days
This is the part most families fear, and an honest, gentle picture often brings more peace than not knowing. The signs below come from the National Cancer Institute’s summary on the last days of life, and they do not all happen to everyone.
In the final days, common signs include:
- Less interest in food and drink, and difficulty swallowing
- Sleeping much more, and becoming harder to wake
- Withdrawing from people and surroundings — a natural turning inward
- Changes in breathing — shallow breaths, long pauses, or noisy, rattling breathing
- Confusion, restlessness, or seeing people who aren’t there
- Cool, sometimes mottled skin in the hands and feet
🔬 How It Works: As the body slows, it needs less oxygen and energy, so breathing becomes irregular and appetite fades. These are signs of the body gently shutting down, not signs of suffering — and for most people in hospice, the end is calm and pain is well managed, as the NCI’s summary on the last days of life describes.
What caregivers can do is simple and deeply meaningful: offer (but never force) sips of fluid, keep the mouth moist, reposition gently if breathing sounds noisy, and speak softly — hearing is thought to remain even when a person can no longer respond.
✅ Patient Action: If breathing, restlessness, or secretions look distressing, call the hospice team — they can ease these quickly, day or night.
Caring for yourself and finding support
Caregivers carry an enormous weight, and the grief that begins before a loss — anticipatory grief — is real and exhausting. Your wellbeing matters here too.
Call the hospice team whenever pain, agitation, or a new symptom appears, or simply when you feel out of your depth — that is exactly what they are there for. Hospice also provides bereavement support for families, continuing after a loved one has died.
Some family members also begin to worry about their own risk, since a family history can raise the chance of pancreatic cancer. If that’s on your mind, you can check your own genetic risk profile and decide whether to speak with a genetic counselor.
✅ Patient Action: If close relatives have had pancreatic cancer, consider a genetic risk assessment and ask a genetic counselor whether testing for inherited risk makes sense for you.
Frequently asked questions about end-stage pancreatic cancer
1. What does end-stage pancreatic cancer mean?
End-stage pancreatic cancer usually refers to stage IV disease, meaning the cancer has spread beyond the pancreas to distant organs such as the liver, lungs, or abdominal lining. At this point, care focuses on comfort and quality of life rather than curing the cancer. Your oncology team can explain what your specific scans show.
2. How long can you live with end-stage pancreatic cancer?
For pancreatic cancer that has spread to distant organs, the five-year relative survival is about 3%, and many people live weeks to months — but this varies widely with overall health and treatment response. Statistics describe groups, not individuals. Ask your oncologist what your particular situation suggests.
3. Is end-stage pancreatic cancer painful?
Pain is one of the most common symptoms of end-stage pancreatic cancer, but it can almost always be controlled. Options range from medication to a celiac plexus nerve block for harder-to-treat pain. Uncontrolled pain is a reason to contact your palliative or hospice team the same day.
4. What are the most common symptoms in the final stage?
The most common symptoms of end-stage pancreatic cancer include pain, jaundice, ascites (fluid in the abdomen), ongoing weight loss, digestive changes, profound fatigue, nausea, and blood clots. Nearly all can be eased with supportive care. Report new or worsening symptoms to your care team early so they can be managed.
5. What is the difference between palliative care and hospice?
Palliative care focuses on comfort and can be given at any stage, even alongside cancer treatment. Hospice care is for when treatment to control the cancer stops and the focus is entirely on comfort, generally with a prognosis of around six months. Both support the patient and family.
6. When should someone start hospice for end-stage pancreatic cancer?
Hospice is generally appropriate when the focus shifts fully to comfort and a clinician estimates a prognosis of about six months, though eligibility is determined individually. Many families find that starting earlier brings more support, not less. Ask your oncologist whether hospice is appropriate now and how to begin.
7. What are the signs that death is near?
Common signs in the final days of end-stage pancreatic cancer include eating and drinking very little, sleeping much more, withdrawing from surroundings, irregular or noisy breathing, confusion, and cool skin. These signs don’t occur in everyone, and timing is hard to predict. They reflect the body slowing down, not suffering.
8. Is dying from pancreatic cancer painful at the very end?
For most people receiving hospice care, the final hours of end-stage pancreatic cancer are peaceful, and pain and other symptoms are actively managed. Breathing changes and restlessness can look distressing but usually do not mean the person is in pain. The hospice team can ease any discomfort that appears.
9. Can jaundice and ascites be treated at this stage?
Yes. Jaundice from a blocked bile duct can often be relieved with a stent placed during an endoscopic procedure, and ascites can be drained for comfort through paracentesis, though fluid may return. These are comfort measures, not cures. Your care team can advise which options fit your situation.
10. How can caregivers cope through this?
Caregiving alongside anticipatory grief is exhausting, and support is essential. Lean on the hospice team for both practical help and emotional support, accept help from others, and use the bereavement support hospice provides for families. Caring for yourself is not selfish — it is what allows you to keep showing up.
11. Where can families find support?
Families facing end-stage pancreatic cancer can find support through their hospice team, which offers medical, emotional, and spiritual care, and through trusted resources like MedlinePlus’s pancreatic cancer overview. Hospice bereavement programs continue supporting families after a loss. You do not have to manage this alone.
Facing what comes next
There is no version of this that is easy, and you don’t need to have all the answers today. The most useful next step is usually a single honest conversation with the care team about comfort, symptom relief, and whether hospice is the right support now.
Whatever time remains, it can be time made gentler — with pain controlled, dignity protected, and a loved one surrounded by people who care. For the bigger picture of how this disease develops and is treated, see the full pancreatic cancer guide, or read about the earlier signs of pancreatic cancer if you’re tracing how things began. The effort and love you’re bringing to this matters more than you know.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: Internal Medicine (2010); Clinical Pharmacology (2013) Experience: 15 years | Location: San Francisco, California Education: BS Molecular Biology, Caltech (2000); MD/PhD, UCSF School of Medicine (2007);…

Board Certifications: Preventive Medicine (2010); Public Health & General Preventive Medicine (2010) Experience: 15 years | Location: Washington, DC Education: BA Public Policy, Georgetown University (2001); MD, George…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.