On This Page – Quick Medical Summary
If you or someone you love has been told they have pancreatitis, the fear that it might be — or might become — pancreatic cancer is one of the most common reasons people search for answers. The two conditions involve the same organ and share several symptoms, which is exactly why they get confused. They are not the same thing: one is inflammation, the other is cancer.
This guide is written for three situations. If you have unexplained upper-abdominal or back pain and want to understand which condition fits, start with the symptom comparison below. If you already have chronic pancreatitis and worry about your cancer risk, the section on whether pancreatitis can turn into cancer is written for you. And if you are facing tests, or supporting someone who is, the section on how doctors tell the two apart will help you ask sharper questions.
Here is the honest, sourced picture — what each condition is, how they differ, and when symptoms mean it is time to act.
ℹ️ Medical Disclaimer: This article is general health education, not a diagnosis or a treatment plan, and it cannot tell you which condition you have. Distinguishing pancreatitis from pancreatic cancer — and any decision about testing, imaging, biopsy, medication, or treatment — requires a board-certified gastroenterologist or pancreatic specialist who can examine you and review your results. If you have severe abdominal pain, yellowing of the skin or eyes, or other warning signs described below, seek medical care promptly.
What pancreatitis and pancreatic cancer actually are
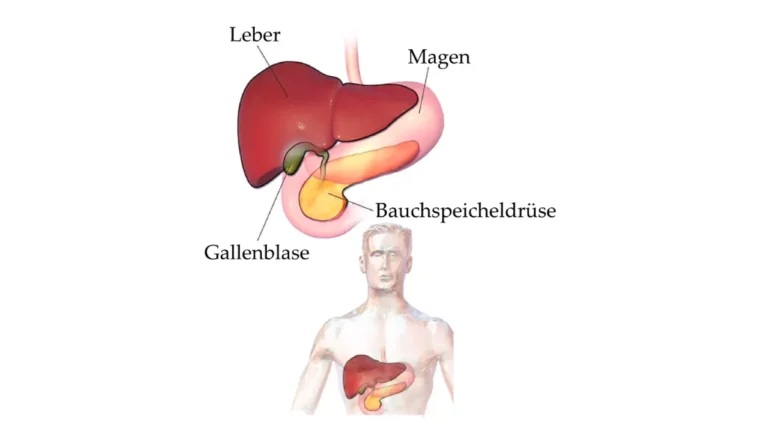
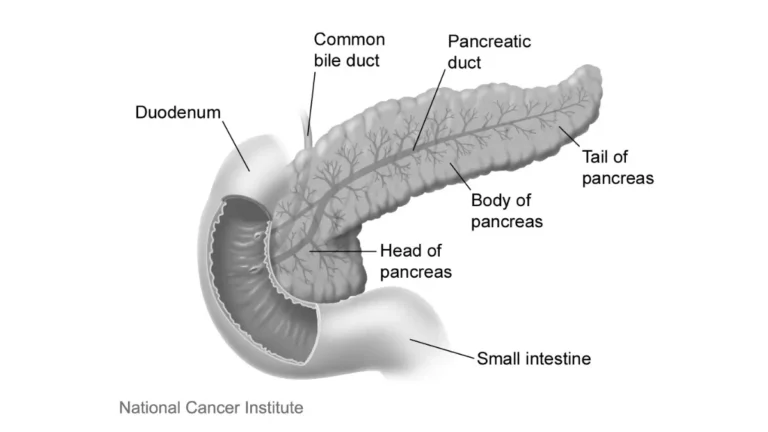
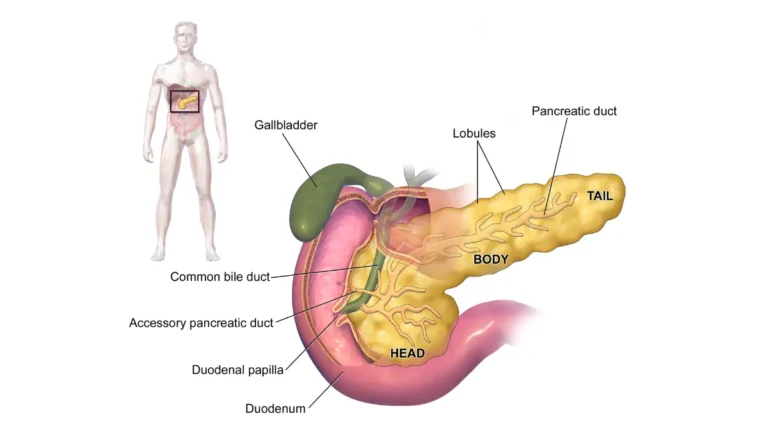
The clearest way to separate the two is by what is physically happening in the gland. Pancreatitis is inflammation of the pancreas, while pancreatic cancer is a malignant growth in the pancreas. Inflammation means irritation and swelling — not a tumor; cancer means pancreatic cells have begun to grow uncontrollably.
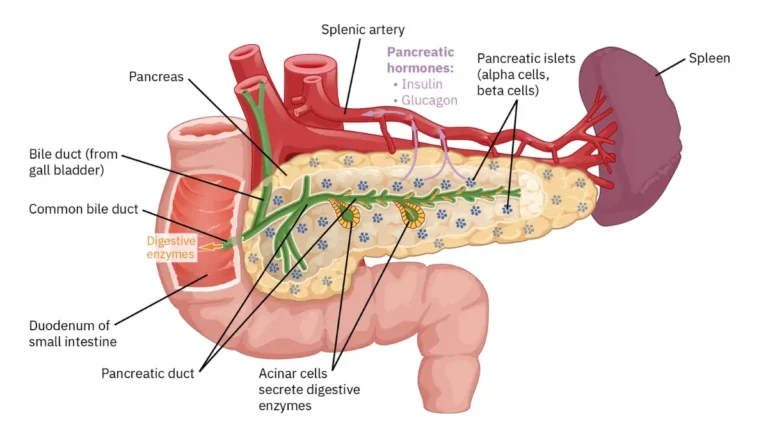
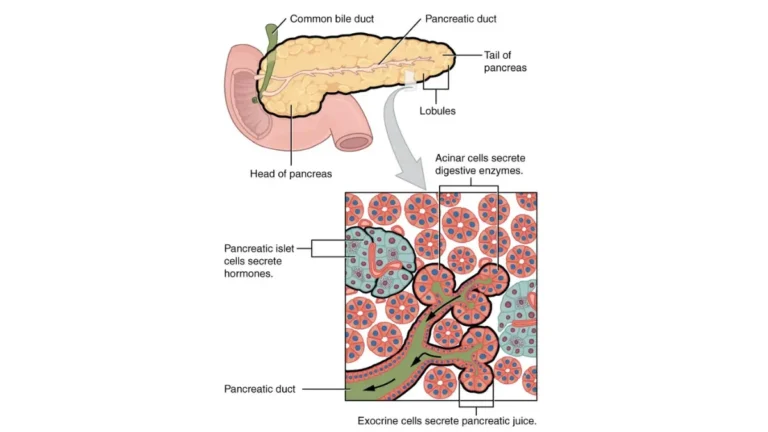
🔬 How It Works: Your pancreas makes digestive enzymes. In pancreatitis, those enzymes can activate too early and start to irritate and damage the gland itself, setting off inflammation. In cancer, a change in pancreatic cells causes them to multiply and form a tumor — most often a type called pancreatic ductal adenocarcinoma.
Pancreatitis: when the pancreas becomes inflamed
Acute pancreatitis comes on suddenly and is usually short-term; most people recover within several days with treatment, according to the NIDDK’s overview of pancreatitis. Chronic pancreatitis is long-lasting and can cause permanent damage over time. The most common triggers are gallstones and heavy alcohol use, which together account for most acute cases.
Pancreatic cancer: when cells grow out of control
Pancreatic cancer is far less common than pancreatitis but much more serious. It often grows quietly, which is part of why it is so frequently found late. That contrast in behavior — loud and sudden versus quiet and gradual — is the foundation for everything that follows.
How the symptoms differ — and where they overlap
Both conditions can cause upper-abdominal pain, back pain, and nausea — the overlap that drives the confusion. The pattern, though, usually points one way or the other.
Pancreatitis symptoms: usually sudden and severe
A pancreatitis attack tends to announce itself: sudden, severe pain high in the abdomen that often radiates to the back, frequently with nausea and vomiting. Many people describe it as among the worst pain they have felt, and it can worsen after eating. You can read more about where pancreatic-related pain tends to be felt if you are trying to make sense of your own symptoms.
Pancreatic cancer symptoms: often quiet until later
Pancreatic cancer is often the opposite — quiet early, with little or no pain until the disease is more advanced. Telltale features include painless jaundice (yellowing of the skin and eyes without pain), unexplained weight loss, and sometimes new-onset diabetes. Our guide to the early signs of pancreatic cancer covers these in more detail.
| Feature | Typical in pancreatitis (esp. acute) | Typical in pancreatic cancer |
|---|---|---|
| Onset of pain | Sudden | Gradual, or absent early |
| Pain severity | Often severe | Mild/vague early, or none |
| Jaundice | Less typical; if present, with pain | Classic — and usually painless |
| Weight loss | Possible with chronic disease | Common, often unexplained |
| Nausea / vomiting | Common during an attack | Possible, often later |
Patterns summarized from Johns Hopkins Medicine, the NCI, and the Merck Manual. These are typical tendencies, not diagnostic rules — only testing can confirm a cause.
If your symptoms are hard to place, a symptom checker can help you organize what to tell your clinician.
How doctors tell pancreatitis and pancreatic cancer apart
Doctors rarely rely on a single test. They combine three kinds of evidence:
- Blood tests — lipase, amylase, and CA 19-9
- Imaging — CT, MRI/MRCP, and endoscopic ultrasound
- A biopsy — when a tumor needs to be confirmed
Blood tests: what lipase, amylase, and CA 19-9 can show
In acute pancreatitis, the digestive enzymes lipase and amylase typically rise sharply — a level at least three times the upper limit of normal is one of the standard diagnostic criteria, and lipase is the more specific of the two. The CA 19-9 tumor marker is associated with pancreatic cancer, but it is not a diagnostic or screening test. It can be raised by pancreatitis, jaundice, and other conditions, and roughly 1 in 10 people cannot produce it at all — more on what the CA 19-9 test can and cannot tell you.
🩺 Physician Note: A common point of confusion is treating CA 19-9 as a yes-or-no cancer test. Current guidance does not recommend it to diagnose or screen for pancreatic cancer, precisely because inflammation alone can raise it. It is most useful after a diagnosis is made, to help monitor treatment.
Imaging and biopsy: the real differentiators
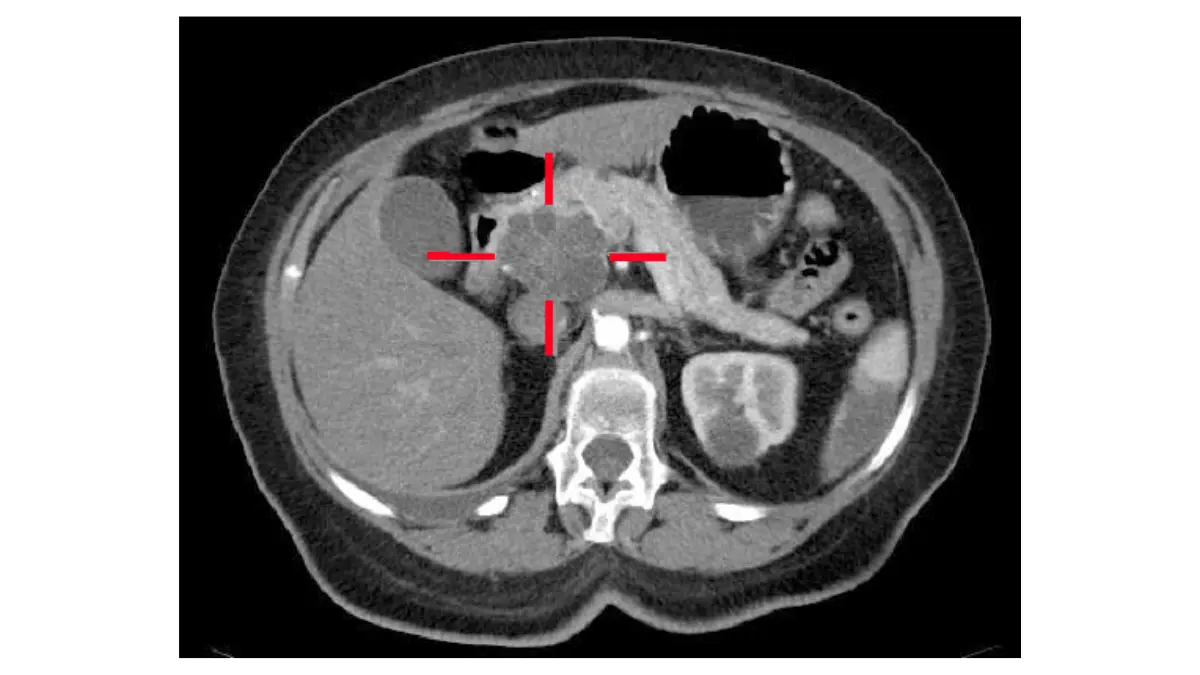
Imaging does the heavy lifting. A contrast-enhanced CT scan, an MRI/MRCP, or an endoscopic ultrasound can reveal a mass, and endoscopic ultrasound can guide a needle to take a tissue sample. A biopsy confirms cancer — blood tests alone cannot, which is covered further in our guide to how pancreatic cancer is diagnosed.
Adapted from Wikimedia Commons MBq cystic-carcinoma-pancreas, licensed under public domain.
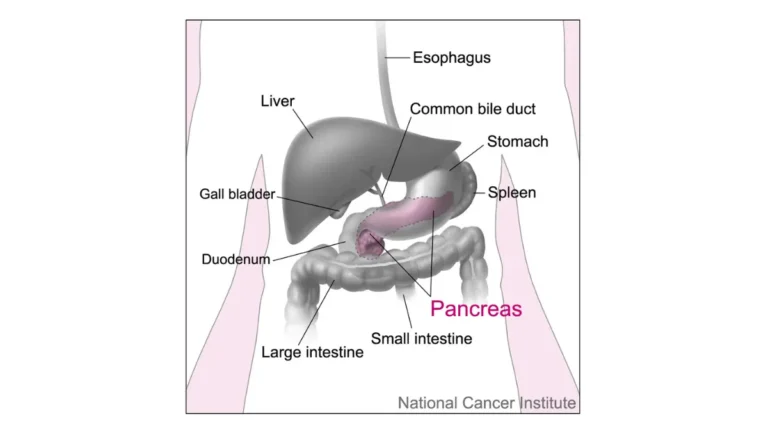
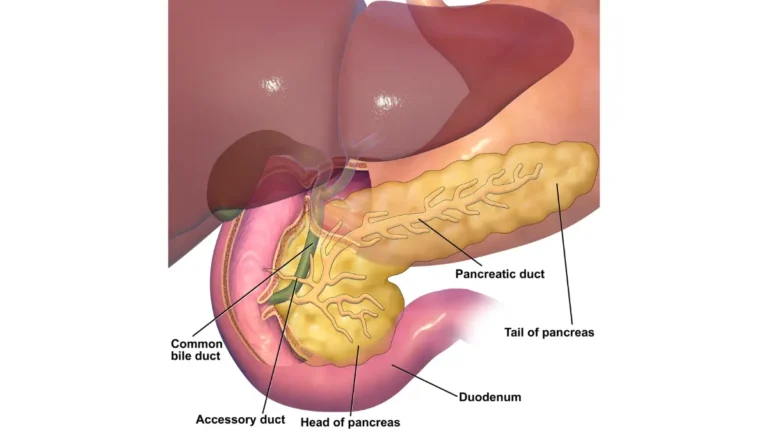
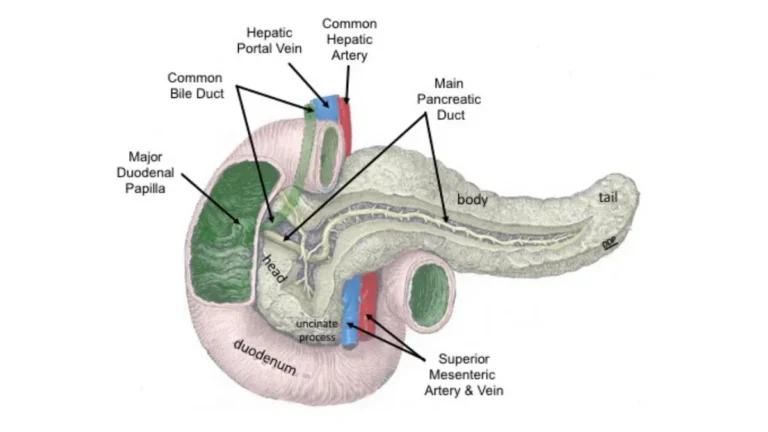
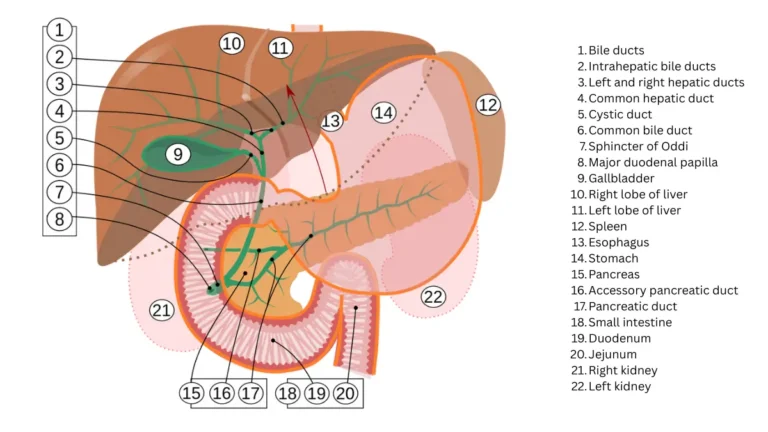
🔬 How It Works: When a tumor sits in the head of the pancreas, it can press on the bile duct and block bile from draining. That backup is what turns the skin and eyes yellow — the painless jaundice that often first signals pancreatic cancer.
Why it can be hard to tell them apart
Even with these tools, the two can be genuinely difficult to separate. A focal, mass-forming type of pancreatitis can look like a tumor on scans, and pancreatitis and cancer can occur together.
✅ Patient Action: If you have ongoing symptoms and your enzyme or marker results are unclear, ask a gastroenterologist or pancreatic specialist directly: “Do I need cross-sectional imaging — a CT or MRI — or an endoscopic ultrasound to rule out a pancreatic mass?”
Can pancreatitis turn into pancreatic cancer?
Chronic pancreatitis does raise the risk of pancreatic cancer — but most people with it never develop cancer. Both halves of that sentence are true, and both matter.
What the research shows
📊 Clinical Data Point: A 2022 systematic review and meta-analysis found that chronic pancreatitis was associated with a standardized incidence ratio of about 22.6 for pancreatic cancer — roughly 21.8 even after excluding cancers found within two years of the pancreatitis diagnosis — and about 63 in hereditary pancreatitis. Source: Gandhi et al., 2022 (PubMed).
A standardized incidence ratio compares how often cancer occurs in this group versus the general population. A number like 22 sounds alarming, which is exactly why the absolute risk matters just as much.
Why most people with pancreatitis never get cancer
In a long-term study, the cumulative risk of pancreatic cancer after chronic pancreatitis was about 1.8% at 10 years and roughly 4% at 20 years. In plain terms, the large majority of people with chronic pancreatitis do not go on to develop pancreatic cancer.
Who is at higher risk
Risk is higher with hereditary pancreatitis, and it rises the longer chronic pancreatitis has been present; smoking adds further risk. A new diagnosis of diabetes in an older adult, especially alongside weight loss, is another clue worth raising with a doctor — see new-onset diabetes and pancreatic cancer. If you have a family history of pancreatic disease, a genetic risk assessment tool can help you frame that conversation.
✅ Patient Action: If you have chronic pancreatitis — especially the hereditary form or a strong family history — ask a gastroenterologist: “Do I meet the criteria for pancreatic cancer surveillance, and if so, how often?”
Red-flag symptoms: when to seek care
Understanding the difference is useful only if it leads to the right action at the right time.
Pancreatitis: when an attack is an emergency
⚠️ Clinical Warning: Severe, persistent upper-abdominal pain — especially with vomiting or an inability to keep fluids down — can signal acute pancreatitis and needs emergency evaluation. This is not something to wait out at home.
Pancreatic cancer: symptoms that need prompt evaluation
Some symptoms warrant prompt medical attention even when they are not an emergency. Painless jaundice in an adult should always be checked, because it is a classic sign of pancreatic cancer — see jaundice and pancreatic cancer. So should significant unexplained weight loss, and new-onset diabetes that appears alongside it.
✅ Patient Action: If your skin or the whites of your eyes turn yellow, or you are losing weight without trying, contact your primary care clinician promptly and ask: “These symptoms can point to a pancreatic problem — what is the fastest way to get imaging?”
For trusted background on the disease itself, the NCI’s pancreatic cancer information is a reliable next step.
What the outlook looks like for each condition
The outlooks for these two conditions are very different, and honesty here serves you better than either false reassurance or alarm.
Pancreatitis: usually manageable
Most acute pancreatitis resolves with supportive care, and the majority of people recover. Severe cases can be dangerous, but they are the exception. Chronic pancreatitis is managed over time with attention to diet, alcohol, and pain.
Pancreatic cancer: why early detection matters
📊 Clinical Data Point: Pancreatic cancer’s overall five-year relative survival is about 13.7%, but it rises to 43.6% when the cancer is found while still localized and falls to 3.4% once it has spread to distant sites. Source: NCI SEER Cancer Stat Facts (2016–2022 data).
These are population statistics, not a prediction for any one person — and the wide gap between localized and distant disease is exactly why the warning signs above matter. For the full picture of symptoms, stages, and treatment, see our complete guide to pancreatic cancer symptoms and stages.
Frequently asked questions
1. Can pancreatitis be mistaken for pancreatic cancer?
Yes. A focal, mass-forming type of pancreatitis can resemble a tumor on imaging, and the two can occur together. This is why doctors often need more than one test — combining imaging with, sometimes, a biopsy — to be certain. If your results are unclear, ask about endoscopic ultrasound or a specialist review.
2. Does chronic pancreatitis always lead to pancreatic cancer?
No. Chronic pancreatitis raises the risk of pancreatic cancer, but the large majority of people with it never develop cancer — cumulative risk was about 1.8% at 10 years in long-term data. Hereditary pancreatitis carries higher risk. Discuss your individual risk and any surveillance with a gastroenterologist.
3. What are the early warning signs of pancreatic cancer?
Early pancreatic cancer is often quiet, but watch for painless jaundice, unexplained weight loss, dull upper-abdominal or back pain, and sometimes new-onset diabetes. These can also have non-cancer causes, so they are reasons to get evaluated rather than to panic. See a clinician promptly if they appear.
4. Is pancreatitis pain the same as pancreatic cancer pain?
Usually not. Pancreatitis pain tends to be sudden and severe, often in the upper abdomen radiating to the back, with nausea. Pancreatic cancer pain is more often gradual, dull, or absent early on. Pain pattern alone cannot diagnose either, so persistent or worsening pain should be checked by a clinician.
5. Can a CT scan tell the difference between pancreatitis and pancreatic cancer?
Often, but not always. CT and MRI are central to telling pancreatitis from pancreatic cancer, yet a mass-forming pancreatitis can mimic a tumor. When imaging is uncertain, endoscopic ultrasound and a biopsy may be needed to confirm whether cancer is present. Ask your specialist which test fits your situation.
6. Does an elevated CA 19-9 mean pancreatic cancer?
No. CA 19-9 is associated with pancreatic cancer but is not a diagnostic or screening test. Pancreatitis, jaundice, and other conditions can raise it, and about 1 in 10 people cannot produce it. It is most useful for monitoring a known cancer. Interpret any result with your doctor, not on its own.
7. How long does chronic pancreatitis take to become pancreatic cancer?
There is no set timeline, and most cases never progress. When cancer does develop, it typically follows years to decades of chronic pancreatitis, and cumulative risk rises over 10 to 20 years. Longer-standing disease and hereditary pancreatitis carry more risk. Ongoing follow-up with a gastroenterologist is the safest approach.
8. Can you have pancreatitis and pancreatic cancer at the same time?
Yes. Pancreatitis and pancreatic cancer can coexist, and inflammation can even surround a tumor — one reason the two are sometimes hard to separate. A tumor can also block the pancreatic duct and trigger pancreatitis. If pancreatitis appears without an obvious cause, ask your doctor whether further imaging is warranted.
9. Is jaundice a sign of pancreatitis or pancreatic cancer?
Either can involve jaundice, but the pattern differs. Painless jaundice — yellowing without significant pain — is a classic red flag for pancreatic cancer in the head of the pancreas. Jaundice with sudden severe pain more often accompanies pancreatitis or gallstones. Any new jaundice should be evaluated promptly by a clinician.
10. What blood tests are used for pancreatitis vs pancreatic cancer?
For pancreatitis, lipase and amylase are the key enzymes; a level at least three times the upper limit of normal supports the diagnosis. For pancreatic cancer, CA 19-9 may be measured, but it is not diagnostic on its own. Imaging and sometimes a biopsy are needed. Your clinician interprets these together.
11. Should I be screened for pancreatic cancer if I have chronic pancreatitis?
Routine screening is not recommended for everyone with chronic pancreatitis, because the absolute risk is modest. Surveillance is generally reserved for defined high-risk groups, such as people with hereditary pancreatitis or certain genetic mutations. Ask a gastroenterologist whether your personal and family history meets the criteria for monitoring.
The bottom line
Pancreatitis and pancreatic cancer involve the same organ and share symptoms, but they are different conditions: one is inflammation, the other is cancer. Pancreatitis tends to be sudden and loud; pancreatic cancer tends to be quiet, which is why painless jaundice and unexplained weight loss deserve prompt attention.
If you have chronic pancreatitis, the honest message is balanced — your risk of cancer is higher than average, but most people with the condition never develop it. No symptom list or online guide can replace a proper evaluation. The most useful next step is a conversation with a gastroenterologist who can examine you, order the right imaging, and tell you what your specific results mean.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: Internal Medicine (2010); Clinical Pharmacology (2013) Experience: 15 years | Location: San Francisco, California Education: BS Molecular Biology, Caltech (2000); MD/PhD, UCSF School of Medicine (2007);…

Board Certifications: Preventive Medicine (2010); Public Health & General Preventive Medicine (2010) Experience: 15 years | Location: Washington, DC Education: BA Public Policy, Georgetown University (2001); MD, George…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.