On This Page – Quick Medical Summary
What Are STI Test Results? (Understanding Your Report)
You just got your STI test results back and stared at a page full of numbers, abbreviations, and medical terms that might as well be written in another language. You’re not alone.
Over 2.2 million Americans received STI test results in 2024 alone, according to the CDC’s latest surveillance data. Most had the same question: “What do these numbers actually mean?”
Your Test Report: The Basics
STI test results arrive in three main formats. Each uses different terminology that can confuse even the most health-literate patients.
Lab report formats you’ll see:
- Qualitative results: Shows “Positive,” “Negative,” “Reactive,” or “Non-Reactive”
- Quantitative results: Displays numerical values with reference ranges (example: <0.90 index value)
- Descriptive results: Uses terms like “Detected,” “Not Detected,” or “Indeterminate”
Here’s what makes STI results different from other lab tests. Unlike your standard CBC blood test results, STI tests specifically look for bacterial DNA, viral antibodies, or active infections.
The Three Result Categories Explained
Negative (Non-Reactive) Results This means the test did not detect the STI in your system at the time of testing. The infection was not found based on current testing methods and timing.
Positive (Reactive) Results
The test detected the presence of the STI. This requires immediate follow-up, treatment planning, and partner notification protocols.
Indeterminate (Equivocal) Results The test results fall in a gray zone between positive and negative. This happens in 3-8% of cases due to early infection, recent treatment, or insufficient sample quality.
Understanding Index Values and Reference Ranges
Many STI tests report results as numerical index values. Here’s how to read them.
Herpes (HSV-1/HSV-2) Example:
- Index value <0.90 = Negative
- Index value 0.90-1.09 = Equivocal (retest needed)
- Index value ≥1.10 = Positive
These cutoff points are established through population studies involving thousands of tested individuals. Labs determine what values indicate infection versus normal antibody levels.
How to Read Each STI Test Result (Complete Breakdown)
Different STIs require different testing methods and produce different result formats. Let’s decode each one with precision.
Chlamydia Test Results
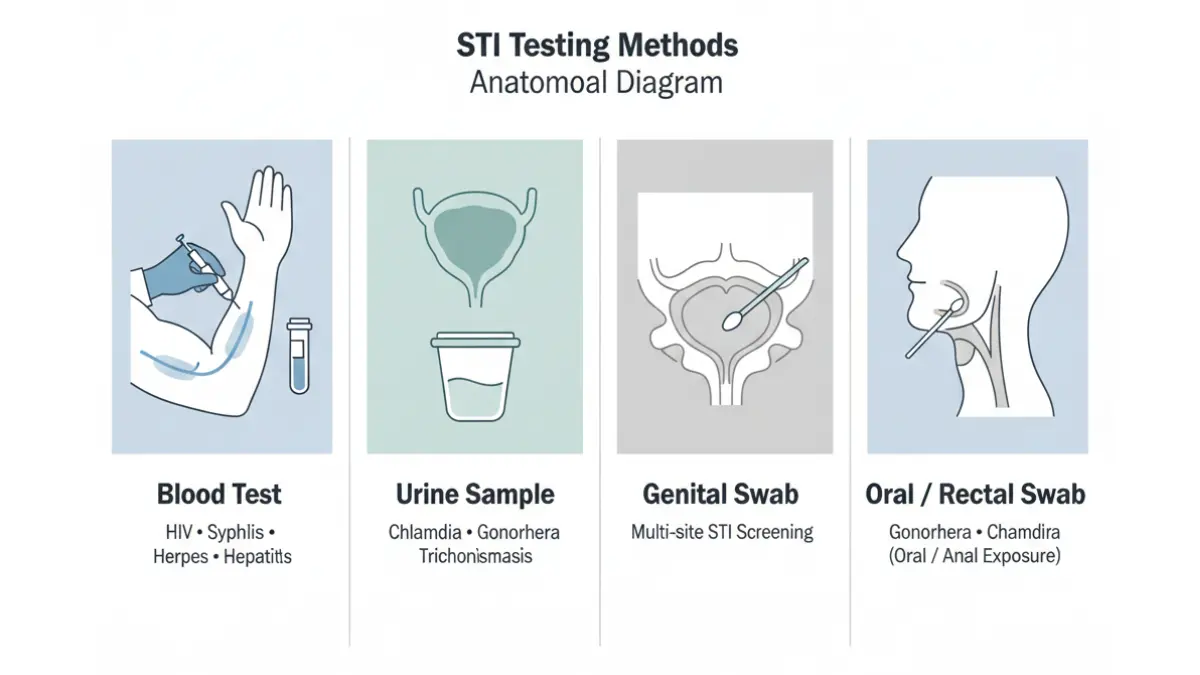
Test Type: Nucleic Acid Amplification Test (NAAT)
Sample: Urine or genital swab
Result Format: Detected / Not Detected
Turnaround Time: 1-3 days
Chlamydia results are binary—either the bacterial DNA was detected or it wasn’t. There’s no numerical value here.
What “Detected” means: Chlamydia trachomatis bacteria is present. Treatment with antibiotics (typically azithromycin or doxycycline) is needed immediately.
Critical timing note: Testing too early after exposure can produce false negatives. The window period for chlamydia is 7-14 days after potential exposure.
Gonorrhea Test Results
Test Type: NAAT or culture
Sample: Urine, throat swab, rectal swab, or genital swab
Result Format: Detected / Not Detected (or Positive/Negative for culture)
Turnaround Time: 1-3 days
Gonorrhea testing through NAAT has 95% sensitivity. This test looks for Neisseria gonorrhoeae DNA.
Multi-site testing importance: If you’ve had oral or anal sex, testing only urine or vaginal samples misses up to 30% of infections. Request pharyngeal (throat) and rectal swabs when appropriate.
HIV Test Results
HIV testing comes in multiple formats with different window periods.
Rapid Antibody Tests:
- Result time: 20 minutes
- Window period: 23-90 days
- Format: Positive/Negative with confirmation needed for positives
4th Generation Antigen/Antibody Tests:
- Result time: 1-3 days
- Window period: 18-45 days
- Format: Reactive/Non-Reactive with numerical values
HIV Result Example: HIV-1/2 Ag/Ab Combo: Non-Reactive (index <1.00)
Any reactive result requires immediate confirmatory testing with HIV-1/HIV-2 differentiation and viral load. Our complete HIV test results guide covers next steps.
Syphilis Test Results (Two-Step Process)
Syphilis testing uses a two-tier approach that can confuse patients.
Step 1: Screening Test (RPR or VDRL)
- Result format: Non-Reactive or Reactive with titer (1:2, 1:4, 1:8, etc.)
- What titers mean: Higher numbers indicate higher antibody levels
Step 2: Confirmatory Test (TP-PA or FTA-ABS)
- Result format: Reactive / Non-Reactive
- Purpose: Confirms true syphilis infection vs. false positive
Result interpretation:
- Screen Reactive + Confirmatory Reactive = Syphilis confirmed
- Screen Reactive + Confirmatory Non-Reactive = Likely false positive
- Screen Non-Reactive = No current infection detected
Herpes (HSV-1 and HSV-2) Test Results
Test Type: IgG Antibody Blood Test
Result Format: Index value with interpretation
Turnaround Time: 2-3 days
Reading your herpes results:
HSV-1 IgG: 0.45 index value = Negative
HSV-2 IgG: 3.22 index value = Positive
Critical distinction: HSV-1 typically causes oral herpes (cold sores) but can cause genital herpes. HSV-2 primarily causes genital herpes. Your result will specify which type was detected.
Important note: Blood tests detect antibodies, not active infection. A positive result means you’ve been exposed at some point but doesn’t indicate when infection occurred.
HPV (Human Papillomavirus) Test Results
Test Type: DNA test (women only)
Sample: Cervical swab during pelvic exam
Result Format: Positive/Negative for high-risk HPV types
HPV result categories:
- Negative for all HPV types
- Positive for low-risk types (6, 11 – cause warts)
- Positive for high-risk types (16, 18 – linked to cervical cancer)
Note: There is no approved HPV test for men. Diagnosis in men typically occurs through visual examination of warts.
Hepatitis B and C Test Results
These tests measure different markers of infection and immunity.
Hepatitis B Panel:
- HBsAg (surface antigen): Positive = Current infection
- Anti-HBs (surface antibody): Positive = Immunity (vaccine or past infection)
- Anti-HBc (core antibody): Positive = Past or current infection
Our detailed hepatitis panel results guide explains each marker.
Hepatitis C:
- HCV Antibody: Reactive/Non-Reactive
- If reactive, reflex HCV RNA (viral load) confirms active infection
Trichomoniasis Test Results
Test Type: NAAT or wet mount microscopy
Result Format: Detected / Not Detected
Turnaround Time: 1-2 days
Trichomoniasis (caused by Trichomonas vaginalis parasite) produces straightforward results. Detection means treatment with metronidazole or tinidazole is needed.
What Do Positive STI Test Results Mean? (Immediate Action Steps)
Finding out you have a positive STI result triggers a cascade of emotions: shock, fear, anger, shame, confusion. Take a breath. More than 1 in 5 Americans has an STI at any given time, based on CDC estimates.
Your First Hour After a Positive Result
Minute 1-15: Process the information Do not panic. Most STIs are completely curable with antibiotics. Even chronic viral STIs (herpes, HIV, HPV) are manageable with modern treatments.
Minute 15-30: Understand your specific diagnosis Re-read your results. Note which STI was detected and the specific values if provided. Understanding exactly what you’re dealing with reduces anxiety.
Minute 30-60: Contact your healthcare provider Call immediately if results came from a lab without physician follow-up. If your doctor ordered the test, they should contact you directly for positive results.
Treatment Timelines by STI Type
Bacterial STIs (Cured with Antibiotics):
Chlamydia:
- Treatment: Single dose azithromycin (1g) or doxycycline 100mg twice daily for 7 days
- Cure rate: 95-97%
- Retest: 3 months after treatment
- Sexual activity: Abstain for 7 days after treatment starts
Gonorrhea:
- Treatment: Ceftriaxone 500mg injection
- Cure rate: 99%+ with proper treatment
- Concern: Antibiotic-resistant strains emerging
- Partner treatment: All partners from past 60 days need testing and treatment
Syphilis:
- Early syphilis: Benzathine penicillin G 2.4 million units (single injection)
- Late syphilis: Three weekly injections
- Cure rate: >95% if caught early
- Follow-up: Titer monitoring at 6 and 12 months
Trichomoniasis:
- Treatment: Metronidazole 2g single dose or 500mg twice daily for 7 days
- Cure rate: 84-98%
- Important: No alcohol for 72 hours after treatment (severe reaction)
Viral STIs (Managed, Not Cured):
Herpes (HSV-1/HSV-2):
- No cure available
- Antiviral medications: Acyclovir, valacyclovir, famciclovir
- Suppressive therapy: Reduces outbreaks by 70-80%
- Transmission: Can still occur during asymptomatic shedding
HIV:
- Treatment: Antiretroviral therapy (ART) – combination of 2-3 medications
- Goal: Undetectable viral load (<200 copies/mL)
- U=U concept: Undetectable = Untransmittable
- Life expectancy: Near-normal with consistent treatment
HPV:
- No specific antiviral treatment
- Immune system clears most infections within 2 years
- Warts: Treated with topical medications or procedures (freezing, laser)
- Cancer prevention: Regular cervical cancer screening crucial
Hepatitis B:
- Chronic infection: Antiviral medications (tenofovir, entecavir)
- Acute infection: Usually resolves on own in 90% of adults
- Monitoring: Liver function tests every 6-12 months
The Partner Notification Process
This is where many people freeze. How do you tell someone they may have been exposed?
Who needs to be notified:
- All sexual partners from the past 60 days (for chlamydia, gonorrhea)
- All partners from past 3 months (for syphilis, depending on stage)
- All partners if you have HIV (regardless of timeframe)
Three notification methods:
- Direct conversation (most effective for current/recent partners)
- Anonymous notification through health department partner services
- Digital notification through services like inSPOT or TellYourPartner.org
What to say: “I recently tested positive for [STI name]. My doctor said anyone I’ve been with should get tested. I wanted you to know so you can take care of your health.”
Keep it factual. Avoid blame. Focus on health, not fault.
Insurance and Confidentiality
Will insurance notify anyone? Insurance companies send Explanation of Benefits (EOB) to the policyholder. If you’re on a parent’s or partner’s insurance, they may see that STI testing occurred but not the specific results.
Confidential testing options:
- Title X funded clinics (income-based free/low-cost)
- Planned Parenthood
- County health departments
- Self-pay at private labs (LabCorp, Quest)
Cost without insurance:
- Single STI test: $50-$100
- Full panel: $150-$350
- Treatment: $50-$200 for bacterial STIs
What Do Negative STI Test Results Mean? (Window Periods Explained)
A negative result doesn’t always mean you’re in the clear. Understanding window periods is critical.
The Window Period Problem
Window period is the time between potential STI exposure and when a test can accurately detect infection. Testing too early produces false negatives—you have the infection but the test can’t detect it yet.
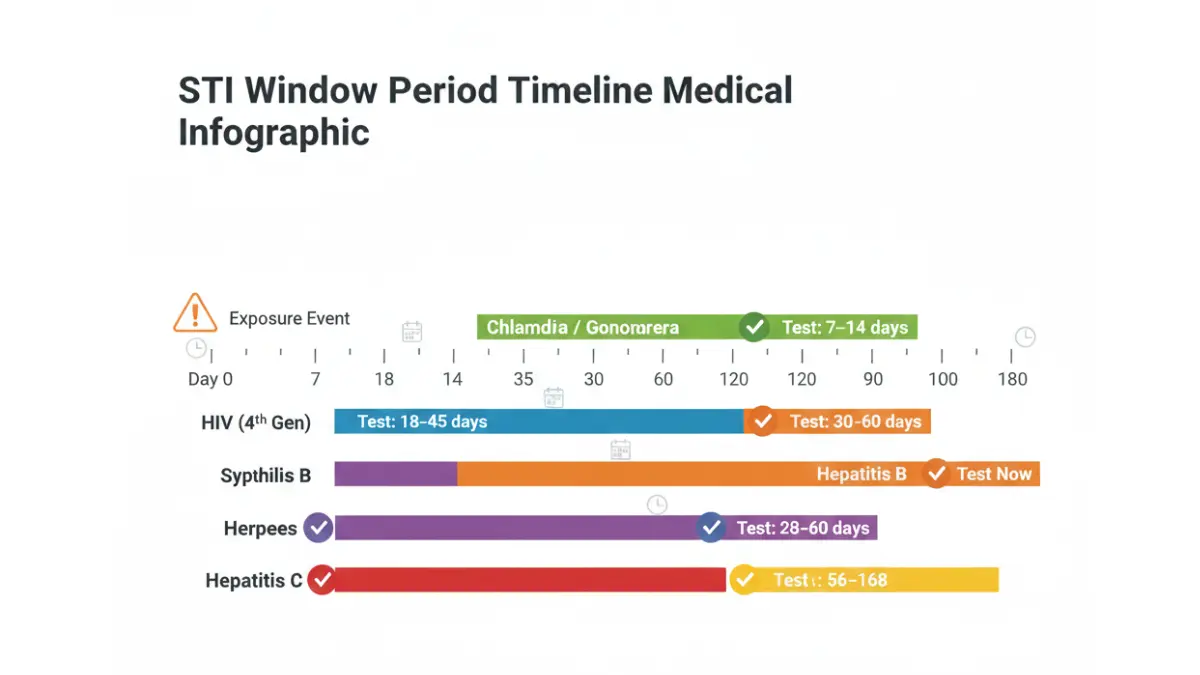
Window Periods by STI:
Chlamydia:
- Window: 7-14 days
- Optimal testing: 2 weeks after exposure
- Note: Can take up to 21 days for some individuals
Gonorrhea:
- Window: 7-14 days
- Optimal testing: 2 weeks after exposure
- Multi-site consideration: Different body sites may show positive at different times
Syphilis:
- Window: 21-90 days
- Initial test: 3 weeks post-exposure
- Confirmatory test: 6 weeks if initial negative but exposure suspected
HIV:
- 4th generation test: 18-45 days
- Antibody-only test: 23-90 days
- RNA test (not standard): 10-33 days
Herpes (HSV-1/HSV-2):
- Window: 4-12 weeks for IgG antibodies
- Optimal testing: 12-16 weeks post-exposure
- Early testing may miss infection
Hepatitis B:
- HBsAg: 30-60 days
- Anti-HBc: 45-70 days
- Full panel recommendation: 6 weeks minimum
Hepatitis C:
- Antibody test: 8-12 weeks
- RNA test: 1-2 weeks
- Confirmation: Repeat at 6 months if high-risk exposure
When to Retest After Negative Results
Scenario 1: Recent exposure (within window period) Retest at the appropriate interval based on the specific STI window periods above.
Scenario 2: Ongoing risk factors
- Multiple partners: Test every 3-6 months
- New partner: Test before becoming sexually active
- Partner diagnosed: Retest 2 weeks after completing treatment
Scenario 3: Symptoms despite negative result Some infections don’t show up immediately on tests but cause symptoms. Symptoms trumps a negative test—see a doctor for clinical evaluation.
False Negatives: How Common Are They?
Test sensitivity varies by STI and testing method.
NAAT tests (chlamydia, gonorrhea):
- Sensitivity: 90-95%
- Means: 5-10% chance of false negative even when infection is present
Antibody tests (HIV, syphilis, herpes):
- Sensitivity: 95-99% after window period
- Before window period: Much lower sensitivity
Factors increasing false negative risk:
- Testing too soon after exposure
- Improper sample collection (especially self-collected)
- Recent antibiotic use (can suppress bacterial STIs temporarily)
- Very early or very late infection stages
The “All Clear” Timeline
If you had a single exposure event, here’s when you can be reasonably confident you’re negative:
Week 2: Chlamydia and gonorrhea testing reliable
Week 4: HIV 4th generation testing 95% accurate
Week 6: Syphilis initial screening reliable
Week 12: HIV antibody testing 99% accurate, Herpes IgG testing reliable
Week 24: Hepatitis C antibody testing conclusive
Many doctors recommend a comprehensive STI panel at 2 weeks, 6 weeks, and 12 weeks post-exposure for complete peace of mind.
Indeterminate or Borderline Results (What Happens Next)
You got your results back and they say “equivocal,” “borderline,” or “indeterminate.” Now what?
Why Indeterminate Results Occur
Indeterminate results happen when test values fall in a gray zone between clearly positive and clearly negative. This occurs in 3-8% of STI tests.
Common causes:
Early infection (most common): Your body is just starting to produce antibodies. Levels are detectable but not yet high enough to definitively call positive.
Recent treatment: You were treated for an STI recently. Antibody levels or bacterial loads are declining but still show up on sensitive tests.
Cross-reactivity: Other infections or conditions trigger antibodies that interfere with STI test interpretation.
Sample quality issues: Insufficient sample volume, contamination, or improper handling affects result accuracy.
Very old infection: Antibody levels have declined over years but haven’t disappeared completely.
Interpretation by Test Type
Herpes IgG with index value 0.90-1.09: This is the classic equivocal range. You need a retest in 4-6 weeks or a Western Blot confirmatory test.
Western Blot is the gold standard for herpes but costs $200-$300 and isn’t routinely covered by insurance. It provides definitive positive or negative results.
HIV 4th Generation Reactive with Negative Differentiation: Initial screen showed reactive but follow-up HIV-1/HIV-2 antibody differentiation was negative or indeterminate.
Next step: HIV-1 RNA (viral load) test within 1-2 weeks. This detects actual virus and confirms whether infection is present.
Syphilis with Low Reactive Titer: RPR titer of 1:1 or 1:2 can be indeterminate, especially if confirmatory TP-PA is also weakly positive.
Requires: Clinical evaluation, detailed sexual history, and likely repeat testing in 2-4 weeks.
Chlamydia/Gonorrhea Indeterminate: Rare with NAAT testing but can occur. Usually requires repeat testing with fresh sample.
The Retest Protocol
Most indeterminate results require retesting within 2-6 weeks depending on the specific STI.
During the waiting period:
Sexual activity: Abstain or use barrier protection consistently. Treat yourself as potentially positive to protect partners.
Treatment consideration: Some doctors opt for presumptive treatment, especially for bacterial STIs where treatment is simple and side effects minimal.
Anxiety management: Indeterminate results create significant stress. Consider using our Symptom Checker to track any symptoms that develop while waiting.
When Presumptive Treatment Makes Sense
Doctors may treat before confirmatory results in these scenarios:
- High-risk exposure with symptoms present
- Sexual partner already diagnosed and treated
- Bacterial STI (chlamydia, gonorrhea) with low treatment risk
- Patient unlikely to follow up for retest
Presumptive treatment isn’t appropriate for:
- Viral STIs requiring long-term medication (HIV, herpes)
- Situations where confirmation affects partner notification requirements
- Cases where retest timing is critical for diagnosis
Next Steps After Receiving Your STI Test Results (Your 72-Hour Action Plan)
Whether your results were positive, negative, or indeterminate, here’s your systematic action plan.
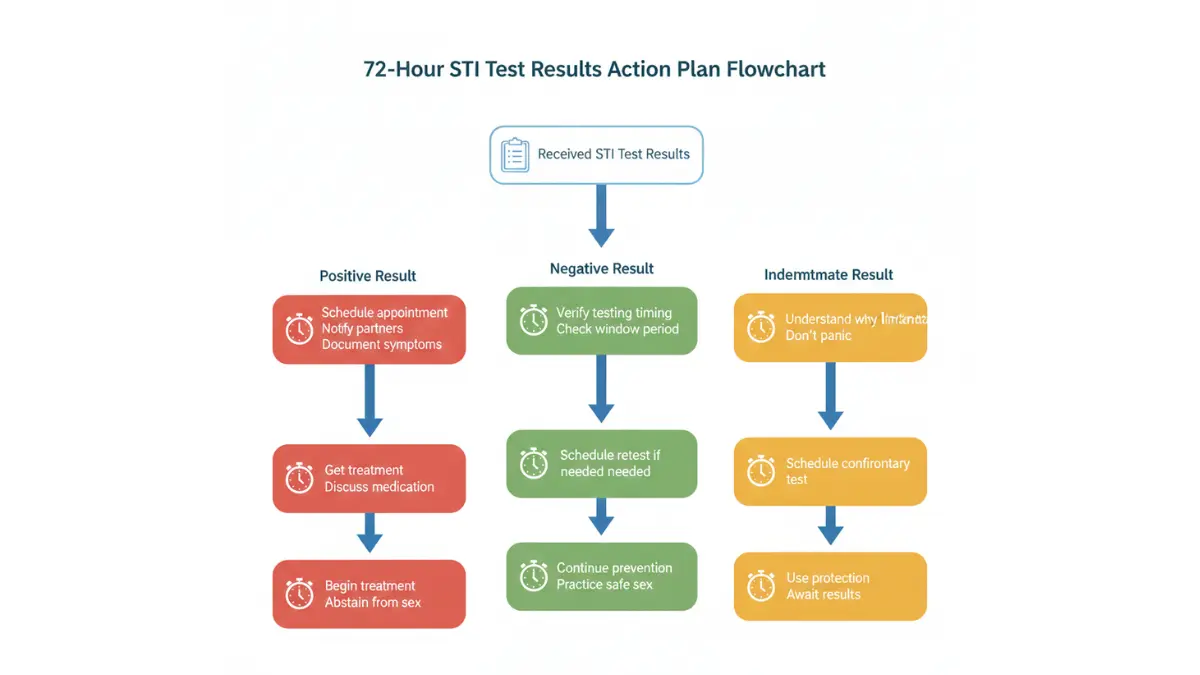
Hour 1-24: Immediate Response
Positive Results:
- Schedule follow-up appointment within 48 hours
- Start partner notification list (dates, contact information)
- Document symptoms if present (helps guide treatment)
- Avoid sexual contact until medical clearance
- Research treatment options but don’t self-medicate
Negative Results:
- Verify testing timing was appropriate based on exposure date
- Schedule retests if within window periods
- Review prevention strategies for ongoing protection
- Consider PrEP if at high risk for HIV
Indeterminate Results:
- Schedule retest within recommended timeframe
- Clarify with provider what specific follow-up is needed
- Practice safe sex until confirmation
- Track any symptoms that develop
Hour 24-48: Medical Follow-Up
For positive bacterial STIs: Most clinics can prescribe treatment via telemedicine within 24 hours. Some offer expedited partner therapy (EPT) where you receive medication for partners without them being examined.
For positive viral STIs: Longer consultation needed to discuss:
- Medication options and side effects
- Suppressive therapy vs. episodic treatment
- Transmission risk reduction strategies
- Long-term management plan
For all results: Ask about:
- When you can safely resume sexual activity
- Retest timing and necessity
- Partner notification resources
- Support services available
Hour 48-72: Partner Notification and Prevention
Partner notification timeline:
Immediate notification needed for:
- Current sexual partner(s)
- Anyone within past 60 days for chlamydia/gonorrhea
- Anyone within past 90 days for early syphilis
- All partners for HIV regardless of timeframe
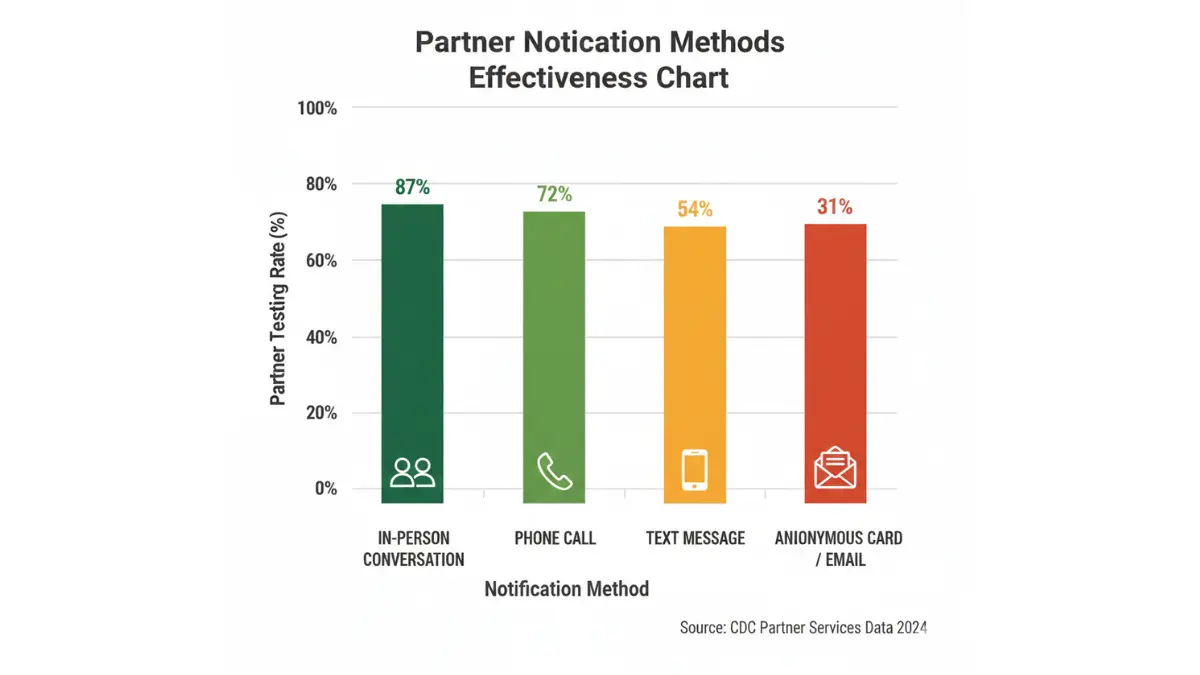
Notification methods ranked by effectiveness:
- Face-to-face conversation (87% partner testing rate)
- Phone call (72% partner testing rate)
- Text message (54% partner testing rate)
- Anonymous notification cards (31% partner testing rate)
Prevention strategy implementation:
Barrier methods:
- Condoms reduce STI transmission by 80-95% when used consistently
- Internal (female) condoms also effective
- Dental dams for oral sex on women or anal contact
Regular testing schedule:
- Every 3 months if multiple partners
- Every 6 months if monogamous but new relationship
- Annually for low-risk individuals
- Before each new partner ideally
Vaccination:
- HPV vaccine: Gardasil 9 (up to age 45)
- Hepatitis B vaccine: 3-dose series
- Hepatitis A vaccine: Recommended for MSM
PrEP (Pre-Exposure Prophylaxis) for HIV: Daily medication that reduces HIV acquisition risk by 99% when taken consistently. Candidates include:
- Anyone with HIV-positive partner
- Men who have sex with men with condomless sex
- People who inject drugs
- Anyone wanting extra protection
Understanding Treatment Success and Cure Rates
Bacterial STIs (curable):
Chlamydia: 97% cure rate with single-dose azithromycin, 98% with 7-day doxycycline
Gonorrhea: 99% cure rate with injectable ceftriaxone
Syphilis: >95% cure with appropriate penicillin treatment
Trichomoniasis: 90% cure with single-dose metronidazole, 95% with 7-day course
Important: “Cure” means the infection is eliminated. You can be reinfected immediately after successful treatment if exposed again.
Viral STIs (manageable):
Herpes: Suppressive therapy reduces outbreaks by 70-80%, transmission risk by 50%
HIV: Antiretroviral therapy achieves undetectable viral load in 95% of adherent patients within 6 months
HPV: 90% of infections clear naturally within 2 years via immune response
Hepatitis B (chronic): Antiviral therapy suppresses virus, reduces liver disease progression, but rarely eliminates infection
When to Return to Sexual Activity
After bacterial STI treatment:
Wait 7 days after completing full antibiotic course AND:
- All symptoms resolved
- Partner(s) tested and treated
- For single-dose treatment: Wait full 7 days even though you took one pill
Returning too soon risks:
- Reinfection from untreated partner (30% risk)
- Treatment failure if infection not fully cleared
- Spreading infection to new partners
After viral STI diagnosis:
Herpes: Can resume with suppressive therapy and disclosure. Use condoms, avoid sex during outbreaks.
HIV: Safe to resume when viral load undetectable (typically 3-6 months on ART). Discuss U=U with partners.
HPV: Can resume but disclose if warts present. Protection is less effective due to skin-to-skin transmission.
Ongoing Monitoring and Retesting
Test of cure (confirm treatment worked):
Required for:
- Gonorrhea: Retest 7-14 days after treatment (resistance concerns)
- Chlamydia in pregnancy: Retest 3-4 weeks post-treatment
- Syphilis: Titer monitoring at 6, 12, 24 months
- HIV: Viral load monitoring every 3-6 months
Not typically needed for:
- Uncomplicated chlamydia in non-pregnant individuals (retest at 3 months for reinfection screening)
- Trichomoniasis (unless symptoms persist)
- Herpes (no cure, monitoring based on outbreaks)
3-month reinfection screening:
CDC recommends retesting 3 months after chlamydia or gonorrhea treatment because:
- 20% of patients get reinfected within 3 months
- Often from untreated partner
- Repeat infection increases complication risks (pelvic inflammatory disease, infertility)
Resources and Support
Free/low-cost testing:
- County health departments
- Planned Parenthood: plannedparenthood.org
- CDC testing locator: Available at CDC website
- Title X funded clinics
Emotional support:
- CDC-INFO: 1-800-CDC-INFO (232-4636)
- Planned Parenthood Chat
- STI support groups (in-person and online)
Educational resources:
- CDC STI Treatment Guidelines: Official 2021 guidelines
- Johns Hopkins STI Prevention Training Center
Related health tracking: Understanding your test results extends beyond STIs. Our Blood Sugar Converter and Health Risk Assessment Tool help you track overall wellness while managing sexual health.
2026 STI Statistics: The Encouraging News
For the first time in nearly two decades, combined STI cases declined 9% from 2023 to 2024, according to provisional CDC data released September 2025. This represents the third consecutive year of decline.
Specific decreases:
- Chlamydia: Down 8% (second consecutive year of decline)
- Gonorrhea: Down 10% (third consecutive year of decline)
- Primary/secondary syphilis: Down 22% (first significant drop since 2001)
These reductions demonstrate that increased testing, treatment access, and prevention efforts are working. However, over 2.2 million STIs were still reported in 2024, and congenital syphilis increased for the 12th consecutive year.
Continued vigilance, regular testing, and consistent prevention remain essential.
Final Thoughts: You’re Going to Be Okay
An STI diagnosis feels overwhelming in the moment. But here’s the truth: Most STIs are completely curable. Even the chronic ones are highly manageable with modern medicine.
You took the crucial step of getting tested. Now you have information, which means you have power to protect yourself and your partners.
Follow your treatment plan. Complete all medications. Get retested as recommended. Practice prevention going forward.
Your sexual health is a normal, important part of your overall wellbeing. Taking care of it is responsible, not shameful.
For additional guidance on interpreting medical results, explore our comprehensive guides on Hepatitis Panel Results, HIV Test Results, and other blood test interpretations.
Medical Disclaimer: This article provides educational information only and should not replace professional medical advice. Always consult with a healthcare provider for diagnosis and treatment decisions. If you need immediate medical assistance, call 911 or visit your nearest emergency room.
References:
- Centers for Disease Control and Prevention. (2025). Sexually Transmitted Infections Surveillance, 2024 (Provisional)
- Johns Hopkins Medicine STD Prevention Training Center. (2024). Clinical Guidelines
- American Sexual Health Association. (2025). STI Treatment and Prevention Resources
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.