On This Page – Quick Medical Summary
If your complete blood count lists hemoglobin and hematocrit one after the other, you may wonder whether they mean the same thing — and which to worry about. They’re closely related, but they measure two different things.
How to use this page: if your results are normal, the next two sections give the plain difference and typical ranges. If a value is flagged high or low, the sections on abnormal results and when to call a clinician are for you. If you want to know which number is more reliable, jump to the accuracy section.
The short version of the hematocrit vs hemoglobin question: hemoglobin measures the oxygen-carrying protein in your blood, while hematocrit measures the share of your blood made of red cells. Because red cells carry hemoglobin, the two usually move together — which is why your lab reports both.
ℹ️ Medical Disclaimer: This article explains what hemoglobin and hematocrit measure, for general education only — not diagnosis, treatment advice, or a substitute for personalized care. Have a licensed physician interpret your ranges, abnormal results, or anemia for your situation, and bring your actual lab report before making decisions.
What’s the actual difference between hematocrit and hemoglobin?
The difference is what each one counts. Hemoglobin measures the oxygen-carrying protein inside your red blood cells, reported as a concentration in grams per deciliter (g/dL). Hematocrit measures how much of your blood volume is red cells, reported as a percentage.
| Feature | Hemoglobin | Hematocrit |
|---|---|---|
| What it measures | The oxygen-carrying protein in red cells | The share of blood volume that is red cells |
| Reported as | Concentration (g/dL) | Percentage (%) |
| Also called | Hb, Hgb | HCT, packed cell volume (PCV) |
| On the CBC | Measured directly | Often a calculated value |
| Key clinical detail | The more direct measure of oxygen-carrying capacity | Also reflects red cell size |
Sources: NIH Clinical Methods; MedlinePlus. Reported together on a CBC as “H and H.”
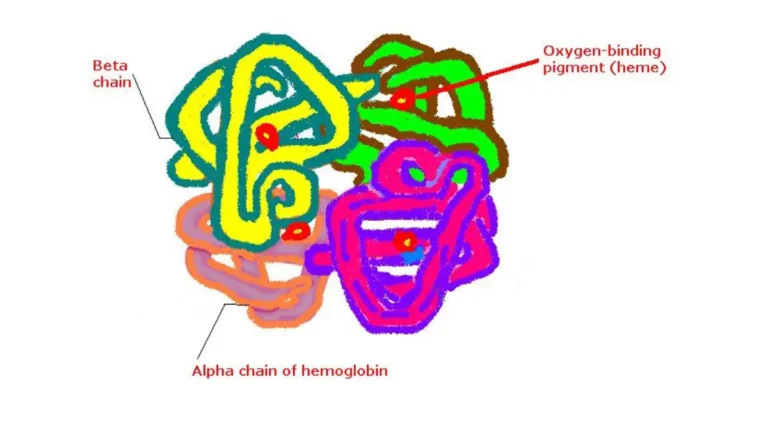
Hemoglobin: the oxygen-carrying protein
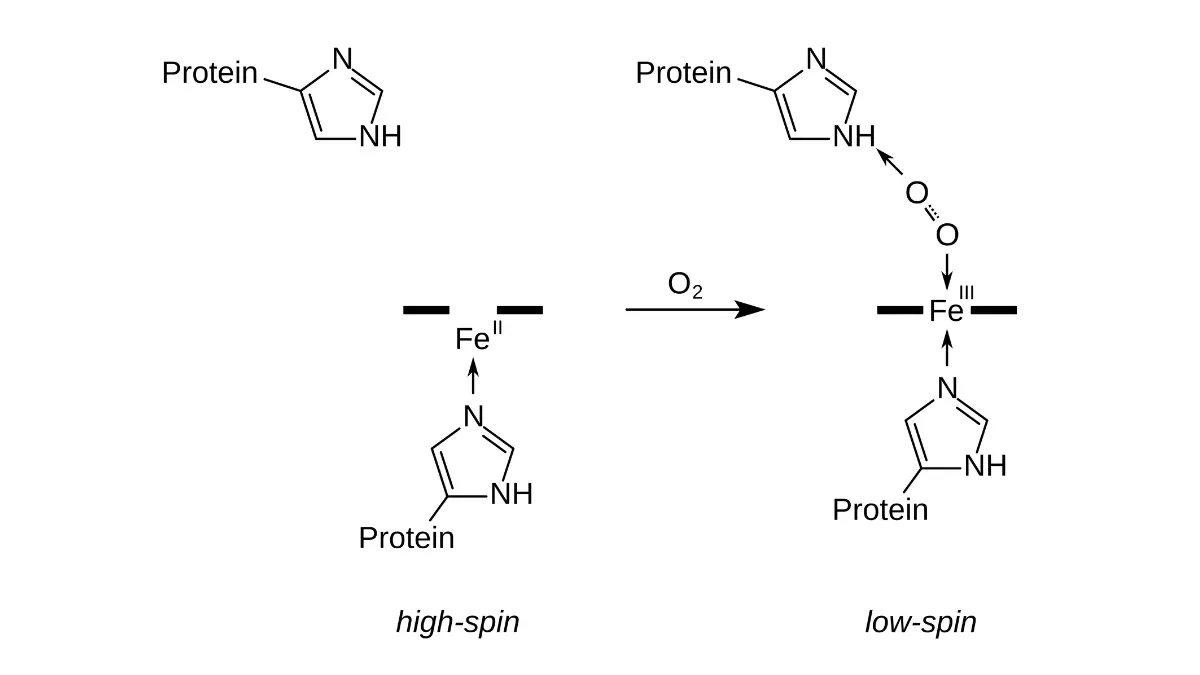
Hemoglobin is the iron-containing protein red cells use to carry oxygen from your lungs to your tissues. It’s measured directly, in g/dL.
🔬 How It Works: Each red cell is packed with hemoglobin. Oxygen binds to its iron in the lungs and releases into tissues — so the hemoglobin number is a direct read on how much oxygen your blood can carry.
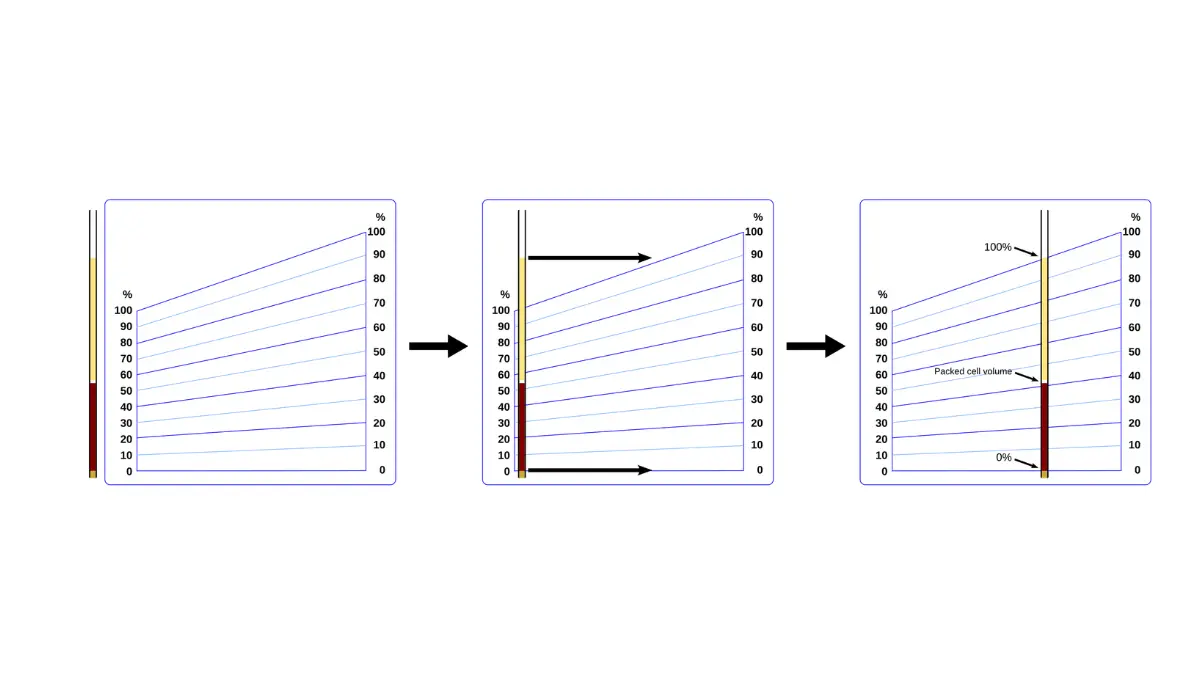
Hematocrit: the percentage that’s red cells
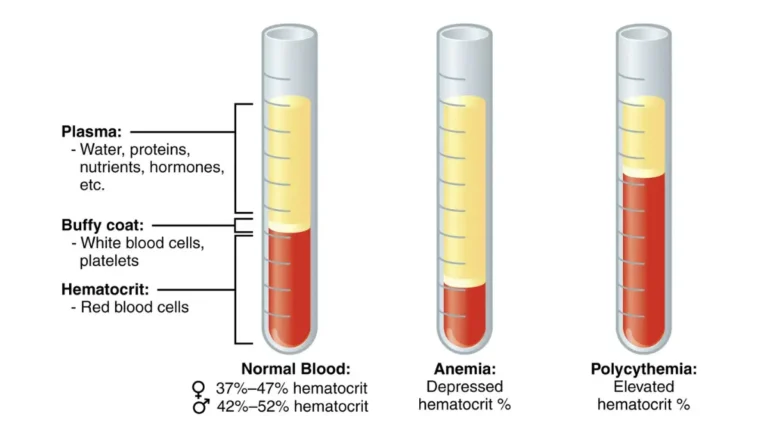
Hematocrit is the proportion of whole blood that is red cells — also called packed cell volume, because spinning a sample packs the red cells into a measurable column. MedlinePlus explains what a hematocrit test measures in plain terms.
What are normal hemoglobin and hematocrit levels?
Reference values give a rough frame, but the range on your own report is what matters. Using NIH reference data, typical adult figures look like this.
| Measure | Typical adult men | Typical adult women | Key clinical detail |
|---|---|---|---|
| Hemoglobin | ~14–18 g/dL | ~12–16 g/dL | Below range often suggests anemia |
| Hematocrit | ~40–54% | ~36–48% | Runs near three times the hemoglobin |
Reference values from NIH Clinical Methods. Ranges vary by laboratory.
Normal hemoglobin range (by sex)
Men typically sit higher than women, largely due to hormonal differences in red cell production. A hemoglobin below your lab’s range is the usual first clue of anemia.
Normal hematocrit range (by sex)
The same pattern holds for hematocrit. One point most sources skip: reference intervals are lab-specific in practice and shift with age and population — so compare against your own lab’s printed range, not a number from the internet. For the rest of the panel, see our full CBC normal range chart.
Why do you get both numbers, and how are they linked?
Red cells contain hemoglobin, so the two are tied together — and your lab reports both plus a set of calculated indices. That link is why they normally move in step.
The rule of three (and its limits)
The rule of three is a quick consistency check: your hematocrit percentage should be about three times your hemoglobin value — a hemoglobin of 13 g/dL pairs with a hematocrit near 39%. It holds only when red cells are normal in size and hemoglobin content, so a mismatch usefully flags that something about the cells is unusual.
🔬 How It Works: Analyzers measure hemoglobin directly and calculate hematocrit from the number of red cells and their average size — which is why hematocrit reflects both how many red cells you have and how big they are, and why what MCV measures feeds into it.
What MCHC tells you
The reason the rule works is a value called MCHC, which links hemoglobin to hematocrit. How MCH and MCHC differ is worth a look if your report flags either.
📊 Clinical Data Point: The normal MCHC — hemoglobin divided by hematocrit — is about 34 g/dL (roughly 32–36). Source: NIH Clinical Methods, Red Cell Indices. Because that ratio is near one-third, hematocrit lands near three times hemoglobin.
Is hematocrit or hemoglobin more accurate?
This is the question most people actually have, and it has a real answer: hemoglobin is generally the more direct measure, because it counts the protein that carries oxygen.
Which one is the more direct measure
Hematocrit is often calculated and is more sensitive to cell size and sample handling. Both shift with hydration, but hemoglobin’s direct measurement is why clinicians usually lead with it to screen for anemia, reading it alongside hematocrit and the indices.
When the two disagree
Because they measure different processes, the two don’t always agree on who is anemic. When red cells vary widely in size — shown by a high RDW — they can tell slightly different stories.
📊 Clinical Data Point: In a CDC analysis of U.S. survey data from 1999–2020, hematocrit flagged more children and pregnant people as anemic than hemoglobin did, with only moderate agreement between the two. Source: NIH/CDC (PMC).
✅ Patient Action: If your two numbers point in different directions, ask your primary care clinician: “Which value are you using to guide my care, and do my red cell indices explain the difference?”
What do high or low hemoglobin and hematocrit mean?
An out-of-range result is a starting point, not a verdict — your clinician interprets it for your situation.
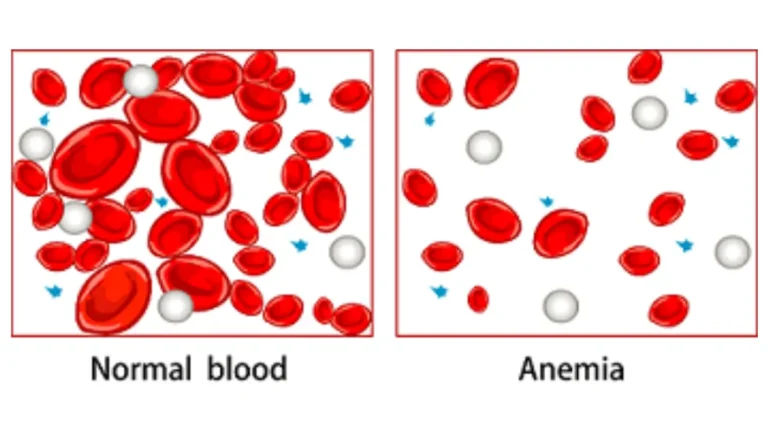
When the numbers are low (anemia)
Low values mean too few red cells or too little hemoglobin, which defines anemia. The WHO defines anemia as hemoglobin below 13 g/dL in men and below 12 g/dL in non-pregnant women. Anemia is a sign, not a diagnosis, so a low result points to a cause — iron deficiency, low B12, blood loss, or chronic disease — that needs working up. See low hemoglobin and anemia for the low end.
When the numbers are high
High values usually mean too many red cells, a state called polycythemia or erythrocytosis. But a high hematocrit can also reflect dehydration or high altitude rather than a red cell disorder, per MedlinePlus.
🩺 Physician Note: Current guidance treats anemia as a beginning, not an endpoint: the hemoglobin number says a problem may exist, but the cause — iron, B12, bleeding, or chronic disease — determines treatment, which is why a low value leads to more testing rather than a prescription.
When to call your clinician
Any result outside your lab’s range is worth a conversation, especially with fatigue, breathlessness, or dizziness. A quick symptom checker can help you gauge how soon.
⚠️ Clinical Warning: Some causes of very high or very low counts are serious — severe drops can follow internal bleeding, and very high counts can raise clot risk. Chest pain, severe shortness of breath, fainting, or signs of bleeding warrant urgent care, not a routine recheck.
✅ Patient Action: Bring your printed report and ask your primary care clinician: “Do these results suggest anemia or something else, and what’s the next test to find the cause?”
The dehydration trap: why your numbers can mislead
One common factor can push both numbers off without any real change in your red cells.
How dehydration inflates both numbers
Both are measured in whole blood, so both values depend on plasma volume. Dehydration concentrates the blood and pushes both readings higher; fluid overload dilutes it and pushes both lower.
🔬 How It Works: Blood is red cells suspended in plasma. When you’re dehydrated you have less plasma, so the same red cells make up a larger share — nudging both hematocrit and hemoglobin up even though the red cells haven’t changed.
Why one reading isn’t enough
So a single borderline result can mislead, and trends over time carry more weight than one snapshot.
✅ Patient Action: If a borderline result surprises you, ask whether it should be rechecked when you’re well-hydrated — and don’t load up on fluids to “fix” a number right before testing.
Frequently asked questions about hematocrit vs hemoglobin
1. What is the difference between hematocrit and hemoglobin?
Both describe your red blood cells but count different things. Hemoglobin measures the oxygen-carrying protein inside red cells, in grams per deciliter; hematocrit measures the percentage of blood volume that is red cells. Because red cells contain hemoglobin, the two normally rise and fall together, so both appear on a CBC.
2. Is hematocrit or hemoglobin more accurate?
Hemoglobin is generally more direct, since it counts the protein that carries oxygen, while hematocrit is often calculated and more sensitive to cell size. Clinicians usually lead with hemoglobin to screen for anemia but read both together. If your numbers disagree, ask which value is guiding your care.
3. What is the rule of three for hemoglobin and hematocrit?
The rule of three is a quick consistency check: your hematocrit percentage should be about three times your hemoglobin — a hemoglobin of 13 g/dL pairs with a hematocrit near 39%. It holds only when red cells are normal in size and hemoglobin content, so it can break with certain anemias.
4. What is a normal hemoglobin level?
Typical adult hemoglobin runs about 14–18 g/dL for men and 12–16 g/dL for women in NIH reference data. Ranges differ by lab, age, and population, so the most reliable comparison is the range printed on your own report. Below range often suggests anemia.
5. What is a normal hematocrit level?
Typical adult hematocrit is roughly 40–54% for men and 36–48% for women in NIH reference data. Exact cutoffs vary by lab, so use your own results’ range. Because hematocrit is about three times hemoglobin, the two normally track together, and a large mismatch is worth asking about.
6. Can hemoglobin be normal but hematocrit low?
It can, though usually the two move together. Because hematocrit is often calculated from red cell number and size, unusual cell sizes or lab factors can nudge them apart. A meaningful gap is a reason to review the red cell indices with your clinician.
7. What causes high hematocrit but normal hemoglobin?
A high hematocrit with normal hemoglobin can reflect dehydration, which concentrates the blood, or living at high altitude, rather than a red cell disorder. Larger red cells or calculation factors can also contribute. Because causes range from harmless to serious, ask your clinician what the pattern means.
8. Does dehydration affect hemoglobin and hematocrit?
Yes. Both are measured in whole blood and depend on your plasma volume. Dehydration reduces plasma, so red cells make up a larger share and both read higher; fluid overload dilutes the blood and both read lower — even when your red cell mass hasn’t changed.
9. Why are both hemoglobin and hematocrit on a CBC?
Red cells contain hemoglobin, so measuring both gives a fuller picture than either alone. Hemoglobin directly reflects oxygen-carrying capacity, while hematocrit shows the proportion of blood that is red cells and feeds the calculated indices. Together they help screen for and characterize anemia more reliably.
10. What hemoglobin level indicates anemia?
The WHO defines anemia as hemoglobin below 13 g/dL in men and below 12 g/dL in non-pregnant women, and below 11 g/dL in pregnancy. Anemia is a sign, not a diagnosis, so a low value points to a cause that needs investigating. Ask what testing comes next.
11. What is MCHC and how does it relate to hemoglobin and hematocrit?
MCHC — mean corpuscular hemoglobin concentration — is hemoglobin divided by hematocrit, averaging about 34 g/dL. It describes how much hemoglobin is packed into your red cells and is why hematocrit runs near three times hemoglobin. An abnormal MCHC helps clinicians narrow the type of anemia.
The bottom line on hematocrit vs hemoglobin
Hemoglobin and hematocrit are two views of the same red-cell picture: one counts the oxygen-carrying protein, the other the share of blood that’s red cells. Hemoglobin is the more direct measure and clinicians usually lead with it, but they read both together with the indices, because a mismatch is itself a clue. The most useful habit is to compare each number to your own lab’s range and weigh trends over any single reading. Both are just part of your complete blood count; to make sense of the rest of the panel, see how to read your CBC results, and bring the report to your next appointment.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.