On This Page – Quick Medical Summary
You pulled up your blood test results, and two similar-looking numbers are sitting there — MCH and MCHC — maybe one or both flagged. They sound almost identical, and your report probably didn’t explain either one. Here’s the short version first: MCH is how much hemoglobin is packed into each red blood cell, and MCHC is how concentrated that hemoglobin is inside the cell.
Both are part of your complete blood count, and both describe the hemoglobin in your red cells — just from slightly different angles.
Where you go next depends on what you’re looking at:
- If your value is low, the section on low results explains what that usually points to.
- If your value is high, skip ahead — the answer is often less alarming than it looks.
- If a number is flagged but you feel completely fine, the section on reading these results together explains why that happens.
Neither number is meant to be read alone, and a single flag rarely tells the whole story. Let’s make each one make sense.
ℹ️ Medical Disclaimer: This article explains what MCH and MCHC mean and is for general education. It does not diagnose anemia or any blood disorder, interpret your specific results, or replace testing and evaluation. Reference ranges and the meaning of an abnormal value depend on your full blood count, your health history, and your symptoms. Before acting on any result, review your complete blood count with your primary care physician or a hematologist, who can order the right follow-up tests and confirm what your numbers mean for you.
What MCH and MCHC actually measure
The difference between MCH and MCHC comes down to two words: amount versus concentration. MCH measures the average amount of hemoglobin inside a single red blood cell; MCHC measures how tightly that hemoglobin is packed into the space the cell provides.
MCH: the amount of hemoglobin in each red cell
Mean corpuscular hemoglobin is the average mass of hemoglobin carried by one red blood cell, reported in picograms. It’s one of your red blood cell indices, the calculated values that describe red-cell size and hemoglobin content. Because a larger cell can hold more hemoglobin, MCH tends to rise and fall along with cell size, which is why it tracks closely with your MCV — how big your red cells are.
MCHC: how concentrated that hemoglobin is
Mean corpuscular hemoglobin concentration measures the concentration of hemoglobin per unit of red-cell volume, reported in grams per deciliter. Unlike MCH, it controls for cell size. A bigger cell holding proportionally more hemoglobin can still have a perfectly normal concentration.
Why the two can disagree
Picture a small glass and a large glass, each with sugar dissolved in water. The large glass can contain more total sugar (higher MCH) while tasting exactly as sweet as the small one (same MCHC). That’s why one value can be flagged while the other looks normal — they answer different questions.
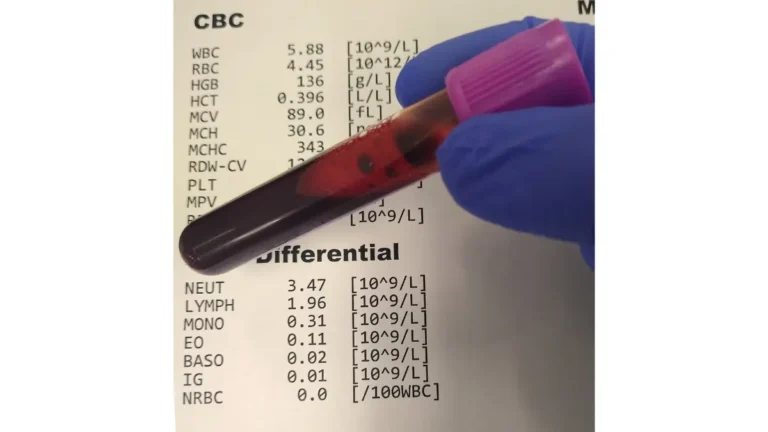
🔬 How It Works: MCH and MCHC aren’t measured directly. An analyzer measures your hemoglobin, hematocrit, and red cell count, then calculates MCH (hemoglobin divided by red cell count) and MCHC (hemoglobin divided by hematocrit). Because they’re derived from those inputs, anything that throws off the underlying measurements shifts these indices too.
Normal ranges for MCH and MCHC
Most labs use similar reference ranges for these two indices, though the exact cutoffs differ slightly from one lab to the next.
| Red cell index | Typical adult reference range | What it measures |
|---|---|---|
| MCH (mean corpuscular hemoglobin) | about 27–33 pg per cell | Amount of hemoglobin per red cell |
| MCHC (mean corpuscular hemoglobin concentration) | about 32–36 g/dL | Concentration of hemoglobin in red cells |
Ranges vary by laboratory and analyzer — always compare against the reference range printed on your own report. MCH interval per NCBI StatPearls (updated 2024); the MCHC figure shown is the commonly reported interval and is lab-dependent.
📊 Clinical Data Point: Typical adult MCH is about 27–32 pg per red blood cell — Source: NCBI StatPearls (updated 2024). Some labs report a slightly higher upper limit (around 33 pg), which is exactly why the range on your own report matters most.
Why your lab’s numbers may differ
Reference ranges are set by each laboratory based on its equipment and the population it tests, so a value flagged at one lab may sit inside the range at another. You can see how these fit with the rest of your results in a full CBC reference-range chart. A result just outside the range is common and, on its own, rarely meaningful.
How these numbers are calculated
Your analyzer divides hemoglobin by red cell count to get MCH, and hemoglobin by hematocrit to get MCHC. Because both are calculated by clinical reference laboratories rather than measured directly, an error in the hemoglobin or hematocrit reading pushes the indices off too — a point that matters when a result looks surprising.
What a low MCH or low MCHC means
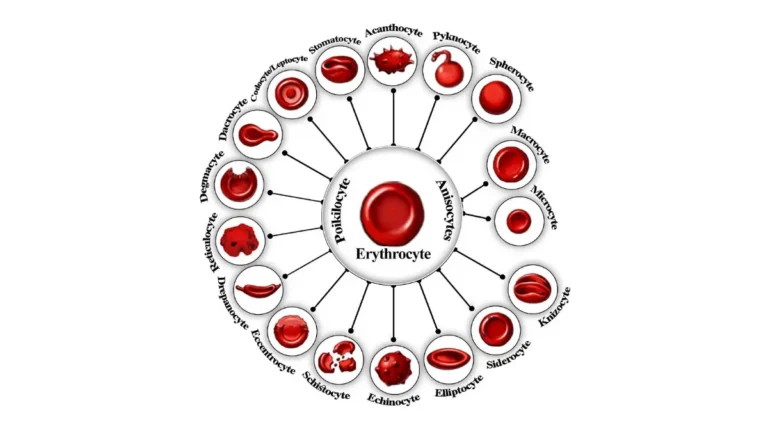
Low MCH or low MCHC usually means your red blood cells contain less hemoglobin than normal — a state doctors call hypochromia, literally “less color,” because hemoglobin gives red cells their color.
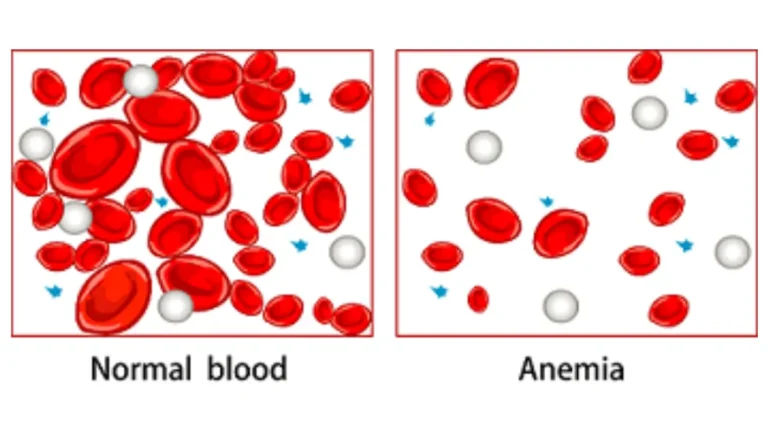
Low values and hypochromic anemia
When red cells are pale and under-filled with hemoglobin, the indices drop, and this pattern often accompanies certain types of anemia. These same cells are frequently small, so a low MCH often travels with a low MCV. Low indices point toward a type of anemia, not a specific diagnosis on their own.
Iron deficiency — the most common cause
Iron deficiency anemia is the most common cause of low, hypochromic red cell indices, and iron-deficiency anemia is the most common form of anemia overall. Without enough iron, the body can’t make enough hemoglobin, so cells end up smaller and paler. If your indices are low, checking iron studies, including ferritin, is a common next step, and low indices often go hand in hand with low hemoglobin.
When low MCH/MCHC isn’t iron
Iron isn’t the only explanation. Inherited conditions such as thalassemia also lower these indices, and so can anemia of chronic disease. That’s why a low value alone doesn’t confirm iron deficiency without further testing.
✅ Patient Action: If your MCH or MCHC is low, ask your primary care physician whether iron studies (including ferritin) should be checked — and if those come back normal, whether testing for thalassemia or another cause is the right next step.
What a high MCH or high MCHC means
A high result behaves very differently from a low one, and the two indices diverge here in an important way. High MCH and high MCHC are not two versions of the same thing.
High MCH — usually larger cells (macrocytosis)
A high MCH usually means your red cells are larger than average, a state called macrocytosis — bigger cells simply hold more total hemoglobin. Common reasons include vitamin B12 or folate deficiency, and this often shows up as a high MCV too. If your MCH is high, your provider may check your vitamin B12 level and folate.
High MCHC — uncommon, and often a lab artifact
A genuinely high MCHC is uncommon, because there’s a limit to how concentrated hemoglobin can get inside a cell. When it does occur, the classic true cause is hereditary spherocytosis, where red cells are shaped like small, dense spheres; autoimmune hemolytic anemia can produce a similar picture. Just as often, though, a high MCHC is a lab artifact rather than a disease — cold agglutinins (antibodies that clump red cells) and very fatty blood samples can both push the reading up falsely, which is why analyzers often flag a high MCHC for a second look.
🔬 How It Works: In hereditary spherocytosis, red cells lose surface area and become compact spheres, so the same hemoglobin is squeezed into less volume — driving the concentration (MCHC) up. With cold agglutinins, cells clump and the analyzer miscounts them, producing a falsely high concentration that a warmed, repeat sample or a blood smear can sort out.
Why there’s no true “hyperchromic anemia”
You may see high MCH loosely described as “hyperchromic anemia,” but that label is misleading. Because hemoglobin concentration has a natural ceiling, cells can’t truly be over-concentrated — a high MCH reflects bigger cells, not richer ones, which is why clinicians don’t recognize a true hyperchromic anemia.
✅ Patient Action: If your MCHC is flagged high, ask whether the result might be a lab artifact and whether a blood smear or repeat sample is warranted before any further work-up — and for a high MCH, ask whether B12, folate, and your MCV should be checked.
How doctors read MCH and MCHC together with MCV and RDW
A single flagged index rarely tells the whole story, which is why doctors read all the red cell numbers as a set.
Why one index is never read alone
MCH and MCHC are most useful alongside the other red cell indices and the rest of your blood count, not in isolation. Because they’re calculated values, an unusual number can reflect the sample or the math rather than a real problem. The pattern across several indices is what points toward a cause.
Reading MCH/MCHC against MCV and RDW
Your MCV (cell size) and red cell distribution width (RDW) — how much your cells vary in size — add the context these two numbers lack. Low MCH with a low MCV suggests one family of causes; a high MCH with a high MCV suggests another. Reading them together is how a clinician narrows the possibilities and decides how to interpret your full CBC.
When the numbers don’t add up
Sometimes the indices disagree in a telltale way. A low hematocrit alongside a normal hemoglobin and a high MCV and MCHC, for example, is a classic fingerprint of cold agglutinins in the sample rather than a disease. When results don’t fit the clinical picture, a blood smear or a repeat sample usually resolves it.
🩺 Physician Note: A common point of confusion is that these indices are calculated, not directly measured — so when a value looks surprising, clinicians check whether it fits the rest of the blood count and the peripheral smear before treating the number itself.
When abnormal MCH or MCHC needs follow-up
Most of the time, a mildly abnormal MCH or MCHC is something to raise at your next visit rather than a reason for alarm — but the right timing depends on your symptoms, not the number alone.
Values worth a routine conversation
A single index slightly outside the reference range, with no symptoms and an otherwise normal blood count, is usually worth a routine conversation rather than urgent action. Your provider will look at the whole picture — your MCV, RDW, hemoglobin, and how you feel — before deciding whether any follow-up test is needed.
Signs that warrant a prompt call
Abnormal indices paired with symptoms deserve quicker attention. Marked fatigue, shortness of breath, unusual paleness, or yellowing of the skin or eyes are worth calling about promptly rather than waiting.
⚠️ Clinical Warning: A high MCHC that looks like a lab artifact still shouldn’t be dismissed on your own — only your clinician can confirm whether it’s a harmless analyzer quirk or a sign of red-cell breakdown that needs testing. If you have significant symptoms of anemia, seek care rather than waiting for a scheduled appointment.
✅ Patient Action: Bring your full blood count to your primary care physician and ask which single next test — iron studies, B12 and folate, or a blood smear — makes the most sense given your specific pattern of results and any symptoms you have.
MCH vs MCHC — frequently asked questions
1. What’s the difference between MCH and MCHC?
MCH and MCHC both describe hemoglobin in your red blood cells but measure different things. MCH is the average amount of hemoglobin inside each red cell, reported in picograms. MCHC is how concentrated that hemoglobin is within the cell’s volume, reported in grams per deciliter. A bigger cell can hold more hemoglobin yet keep a normal concentration.
2. What is the normal range for MCH and MCHC?
For most adults, MCH runs roughly 27 to 33 picograms per cell and MCHC roughly 32 to 36 grams per deciliter. These ranges vary by laboratory, so the reference range printed on your own report is the one that applies to you. A result just outside the range is common and rarely meaningful on its own.
3. Which is more important, MCH or MCHC?
Neither MCH nor MCHC stands alone. Doctors read them with your MCV (cell size) and RDW (variation in cell size), plus hemoglobin and the rest of the blood count. The pattern across these values — not any single index — is what points toward a cause and guides what happens next.
4. What does a low MCH or low MCHC mean?
Low MCH or MCHC usually means your red cells carry less hemoglobin than normal, a pattern called hypochromia. The most common cause is iron deficiency anemia, though thalassemia and anemia of chronic disease can also lower these values. Low indices suggest a type of anemia, not a specific diagnosis — confirm the cause with your clinician.
5. What does a high MCH mean?
A high MCH usually means your red cells are larger than average, so each one holds more total hemoglobin. Vitamin B12 or folate deficiency is a common reason, and a high MCH often appears alongside a high MCV. Because several factors can raise it, ask your clinician whether B12, folate, and MCV should be checked.
6. What does a high MCHC mean?
A genuinely high MCHC is uncommon. When real, it can point to hereditary spherocytosis or autoimmune hemolytic anemia, where hemoglobin is packed into smaller or spherical cells. Just as often it’s a lab artifact from cold agglutinins or fatty blood samples. A blood smear or repeat test helps tell them apart — confirm the meaning with your clinician.
7. Can I have anemia if my MCH and MCHC are normal?
Yes. Some anemias — called normocytic anemias — involve red cells of normal size and normal hemoglobin content, so MCH and MCHC can look normal even when hemoglobin is low. That’s why these indices are read alongside your hemoglobin and the full blood count, not on their own.
8. Why is my MCHC high but I feel fine?
A high MCHC with no symptoms is often a lab artifact rather than a disease. Cold agglutinins and very fatty blood samples can both falsely raise the reading, which is why analyzers frequently flag high MCHC values. A warmed or repeat sample, or a blood smear, usually clarifies it — confirm the finding with your clinician.
9. Can MCH and MCHC be low without iron deficiency?
Yes. Iron deficiency anemia is the most common cause of low, hypochromic indices, but not the only one. Inherited conditions such as thalassemia lower MCH and MCHC, and so can anemia of chronic disease. Because a low value alone doesn’t confirm the cause, further testing — often starting with iron studies — is needed. Ask your clinician.
10. Do MCH and MCHC change with diet or supplements?
Indirectly, yes. MCH and MCHC reflect underlying factors like iron, vitamin B12, and folate status, so correcting a confirmed deficiency can move these values over time. This is general information, not a treatment plan — supplements should follow test results, since taking iron you don’t need carries its own risks. Discuss any supplement with your clinician first.
11. When should I see a doctor about abnormal MCH or MCHC?
A single index slightly outside the range, with no symptoms, is usually worth raising at your next routine visit. Abnormal values with marked fatigue, breathlessness, unusual paleness, or yellowing of the skin or eyes deserve a prompt call. Your clinician interprets the result alongside your full blood count and symptoms to decide the next step.
The bottom line on MCH vs MCHC
The difference between MCH and MCHC comes down to amount versus concentration: MCH is how much hemoglobin sits in each red cell, and MCHC is how concentrated it is. A single flagged value rarely settles anything on its own — these indices earn their meaning only when read alongside your MCV, RDW, hemoglobin, and how you actually feel.
If one of your numbers is outside the range, that’s a starting point for a conversation, not a diagnosis. Bring the full report to your provider, and see what your complete blood count shows as a whole to put these two numbers in context.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.