On This Page – Quick Medical Summary
Could you be eligible for a lung cancer screening CT scan?
Find your starting point: If you have an active symptom — a persistent cough, blood in your sputum, or unexplained weight loss — check your symptoms with our Symptom Checker before continuing. Screening is designed for people without current symptoms. If you want to know whether your age and smoking history qualify you, start with Section 3. If you have already had a scan and are trying to understand your results, go directly to Section 5. If you are researching this for a family member, Section 6 covers insurance and costs.
Every year, thousands of lung cancer cases in the United States are diagnosed at a late stage — when treatment options are substantially more limited. Lung cancer screening with an annual low-dose CT scan changes that trajectory. Early detection, before symptoms develop, significantly expands what treatment can accomplish.
Dr. Nathaniel J. Hargrove, MD, a board-certified oncologist and member of the mymedicineadvisor.com Global Medical Advisory Board, authored this guide. It covers who qualifies, what the scan involves, what your results mean, and how to get it covered by insurance.
ℹ️ Medical Disclaimer: The eligibility criteria, screening procedures, results interpretation frameworks, insurance coverage details, and clinical guidance discussed in this article reflect current medical guidelines and are provided for educational purposes only. Individual eligibility assessments, diagnostic conclusions, follow-up decisions, and coverage determinations depend on factors including age, smoking history, comorbidities, plan type, and specialist assessment. Consult a board-certified pulmonologist, oncologist, or your primary care physician before making any decision about lung cancer screening, nodule follow-up evaluation, or treatment based on information in this article.
What is a low-dose CT scan and how does it work?
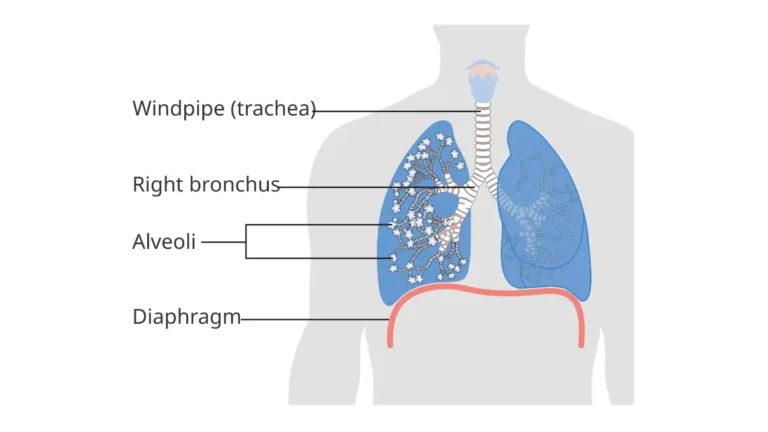
A low-dose CT (LDCT) scan is an FDA-cleared imaging test that produces detailed, three-dimensional cross-sectional images of the lungs using a fraction of the radiation dose delivered by a standard diagnostic chest CT. It requires no injection, no fasting, and no complete change of clothing. A board-certified radiologist reviews the images for pulmonary nodules — small areas of abnormal tissue density — that may warrant monitoring or further evaluation.
🔬 How It Works: During an LDCT scan, a motorized table moves your body through a large, open, ring-shaped scanner. The scanner rotates around your chest while you hold your breath for approximately 5 to 10 seconds, capturing hundreds of thin image slices. A computer reconstructs those slices into a three-dimensional view of your lungs that a radiologist can examine at any angle and magnification.

LDCT vs. chest X-ray: why the difference matters for detection
A standard chest X-ray produces a flat, two-dimensional projection of the chest cavity. This format cannot reliably detect pulmonary nodules smaller than approximately 1 centimeter — the size range where most early-stage lung cancers begin. Current guidelines from the USPSTF, NCI, and NCCN are aligned: chest X-ray has not been shown to reduce lung cancer mortality and is not recommended as a screening tool for any risk group.
LDCT detects nodules as small as 4 to 6 millimeters. That detection window is the entire clinical rationale for using it over X-ray for screening purposes.
📊 Clinical Data Point: The NCI’s lung cancer screening clinical evidence summary confirms that low-dose CT is the only imaging modality with demonstrated efficacy for lung cancer mortality reduction in high-risk adults — Source: National Cancer Institute (verify at publish for current 2026 version).
What the scanner actually does to your lungs
The scanner does not touch you. It emits a narrow, rotating beam of X-rays at significantly reduced intensity compared to a standard diagnostic CT. The radiation dose is low — though the exact figure varies by scanner model and facility protocol and should be discussed with your imaging center at the time of scheduling.
The scanner itself is open on both ends. Most patients with mild claustrophobia tolerate it without significant difficulty. There is no enclosed tube, no loud noise, and no vibration.
Who qualifies for lung cancer screening in 2026?
Adults who meet all three of the following criteria qualify for annual low-dose CT lung cancer screening under the current USPSTF recommendation:
- Age 50 to 80 years old at the time of screening
- A smoking history of at least 20 pack-years — defined as one pack of cigarettes per day for 20 years, or any equivalent combination
- Currently smoke, or have quit within the past 15 years
All three criteria must be met simultaneously. A 75-year-old non-smoker does not qualify. A 52-year-old with a 25-pack-year history who quit 18 years ago does not qualify. Meeting two of three is not sufficient.
📊 Clinical Data Point: The current USPSTF Grade B recommendation for lung cancer screening — specifying age 50–80, a minimum 20-pack-year smoking history, and current or recent smoking status — is published at the USPSTF lung cancer screening recommendation page — Source: U.S. Preventive Services Task Force (verify at publish for any 2026 updates to this recommendation).
📊 Clinical Data Point: The American Cancer Society’s lung cancer early detection guidelines support annual LDCT in adults aged 50 to 80 with a 20 pack-year history, aligned with USPSTF criteria — Source: American Cancer Society (verify at publish for 2026 update).
🩺 Physician Note: “Before the 2021 threshold revision, the eligibility criteria required patients to be 55 years old with a 30-pack-year history. The updated recommendation — age 50 and 20 pack-years — materially changed my clinical practice. Patients in their early 50s with 22-pack-year histories now qualify who would have been excluded before. This change has an outsized impact on Black patients and women, who tend to start smoking later and in smaller quantities but face equivalent or higher lung cancer risk per pack-year smoked. If you checked eligibility before 2021 and were told you didn’t qualify, check again.” — Dr. Nathaniel J. Hargrove, MD, Oncology
The three criteria you must meet to qualify
The 15-year quit window is among the most frequently misunderstood element of the eligibility criteria. The clock starts on the date of your last cigarette. If you quit exactly 15 years ago today, you are at the edge of eligibility — confirm the date precisely with your physician rather than estimating.
⚠️ Clinical Warning: Do not self-exclude from screening based on a rough estimate of your pack-year total or quit date. Patients who smoke intermittently, who smoke pipe or cigar tobacco in addition to cigarettes, or who stopped and restarted multiple times frequently miscalculate their totals. An undercount can result in a missed screening window. Ask your physician to confirm eligibility using your exact history.
What counts as a pack-year — and how to calculate yours
A pack-year equals one pack of 20 cigarettes smoked per day for one full year. The formula:
Pack-years = packs smoked per day × years smoked
| Smoking Pattern | Calculation | Pack-Year Total | Qualifies? |
|---|---|---|---|
| 1 pack/day × 20 years | 1.0 × 20 | 20 pack-years | ✓ Yes |
| 2 packs/day × 10 years | 2.0 × 10 | 20 pack-years | ✓ Yes |
| ½ pack/day × 30 years | 0.5 × 30 | 15 pack-years | ✗ No |
| ½ pack/day × 40 years | 0.5 × 40 | 20 pack-years | ✓ Yes |
| 1 pack/day × 15 years + 1 year quit | 1.0 × 15 | 15 pack-years | ✗ No |
If your smoking history included multiple distinct periods at different rates, calculate each period separately and add the results.

Do you still qualify if you quit smoking?
Yes — provided you quit within the past 15 years. The day you reach 15 years since your last cigarette, the third eligibility criterion is no longer met. If you fall outside the standard criteria but have a family history of lung cancer, radon or asbestos occupational exposure, or other risk factors, assess your personal lung cancer risk profile using our Genetic Risk Assessment Tool — then bring those results to a physician for an individualized discussion.
✅ Patient Action: If you are near the 20 pack-year threshold or uncertain about your quit timeline, ask a board-certified pulmonologist or your primary care physician this specific question before assuming you do or do not qualify: “Based on my exact smoking history and my quit date, do I currently meet the USPSTF criteria for annual LDCT lung cancer screening?”
What to expect on the day of your lung cancer CT scan
Preparing for an LDCT lung cancer screening scan requires almost no advance effort. There is no fasting requirement, no IV line, no contrast dye injection, and in most protocols, no need to fully undress. Remove metal objects near your chest — necklaces, underwire bras — before entering the scanner room, but most patients complete the appointment in their street clothing.
How to prepare before your appointment
Follow these steps on the day of your screening:
- Confirm your physician referral is in place. Your ordering physician must provide a written referral before the facility will schedule the scan. Medicare requires a completed shared decision-making counseling visit before your first covered scan — without it, the claim will be denied.
- Remove metal near your chest. Leave necklaces and metal-clasp bras at home. A front-hook sports bra or no bra is preferable for the appointment.
- Arrive 10 to 15 minutes early. Paperwork, consent forms, and positioning add time even though the scan acquisition itself is brief.
- Inform the technologist of prior lung surgery, implanted devices, or previous CT imaging. Prior comparison scans allow the radiologist to detect growth or change in a nodule — which significantly reduces false-positive rates in subsequent rounds.
- Bring your insurance card and referral documentation. Coverage verification happens at check-in, not in advance for most facilities.
What happens inside the scanner
The LDCT scanner is a large, open ring — not a closed tube. You will lie on a motorized table that slides through the ring while the scanner rotates around your chest. The entire active imaging sequence requires a single breath-hold of approximately 5 to 10 seconds.
The scan acquisition itself takes under five minutes. Total appointment time — including check-in, positioning, and post-scan instructions — is typically 15 to 30 minutes. Results are reviewed by a board-certified radiologist and returned to your ordering physician within several business days.
✅ Patient Action: Before scheduling, confirm with the imaging facility whether your physician’s referral has been received and whether your insurer requires prior authorization. A missing referral or unapproved prior authorization is the most common reason an LDCT appointment is cancelled or denied at check-in — catching it before the appointment saves weeks of rescheduling.
Understanding your lung cancer screening results: what Lung-RADS means
Lung-RADS (Lung CT Screening Reporting and Data System) is the standardized classification system radiologists use to report findings on a lung cancer screening CT scan. A score of 1 or 2 indicates no significant finding requiring follow-up action. A score of 3 or 4 indicates a finding that warrants monitoring, additional imaging, or further evaluation — and does not, by itself, mean cancer.
🔬 How It Works: Lung-RADS assigns a category based on the largest or most concerning nodule visible on the scan. The classification considers nodule size, density type (solid versus ground-glass opacity), and — in subsequent screening rounds — whether growth is detectable compared to the prior year’s scan. The category then determines the follow-up protocol: from routine annual screening to short-interval CT to tissue sampling evaluation.
The Lung-RADS scale explained: categories 1 through 4
| Lung-RADS Score | Description | Typical Characteristics | Recommended Next Step | Best For Patient Profile |
|---|---|---|---|---|
| 1 | Negative | No pulmonary nodules detected | Annual screening next year | Low-risk screening round; reassuring result |
| 2 | Benign appearance | Nodule with clearly benign features (e.g., calcified, stable) | Annual screening next year | Patient with prior scans showing no change |
| 3 | Probably benign | Solid nodule 6–7.9 mm; or new nodule <4 mm | 6-month follow-up LDCT | Patient with small finding requiring surveillance |
| 4A | Suspicious | Solid nodule ≥8 mm; or growing nodule | 3-month LDCT or PET-CT | Patient requiring closer monitoring |
| 4B | Highly suspicious | Solid nodule ≥15 mm or significant growth | Referral for tissue sampling evaluation | Patient requiring definitive diagnosis workup |
Source: American College of Radiology Lung-RADS criteria — verify for current version at publish.
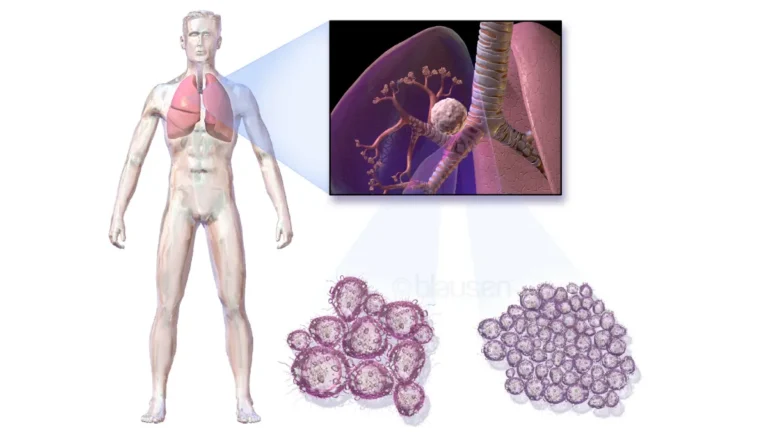
Most nodules found on screening are not cancer — here’s why
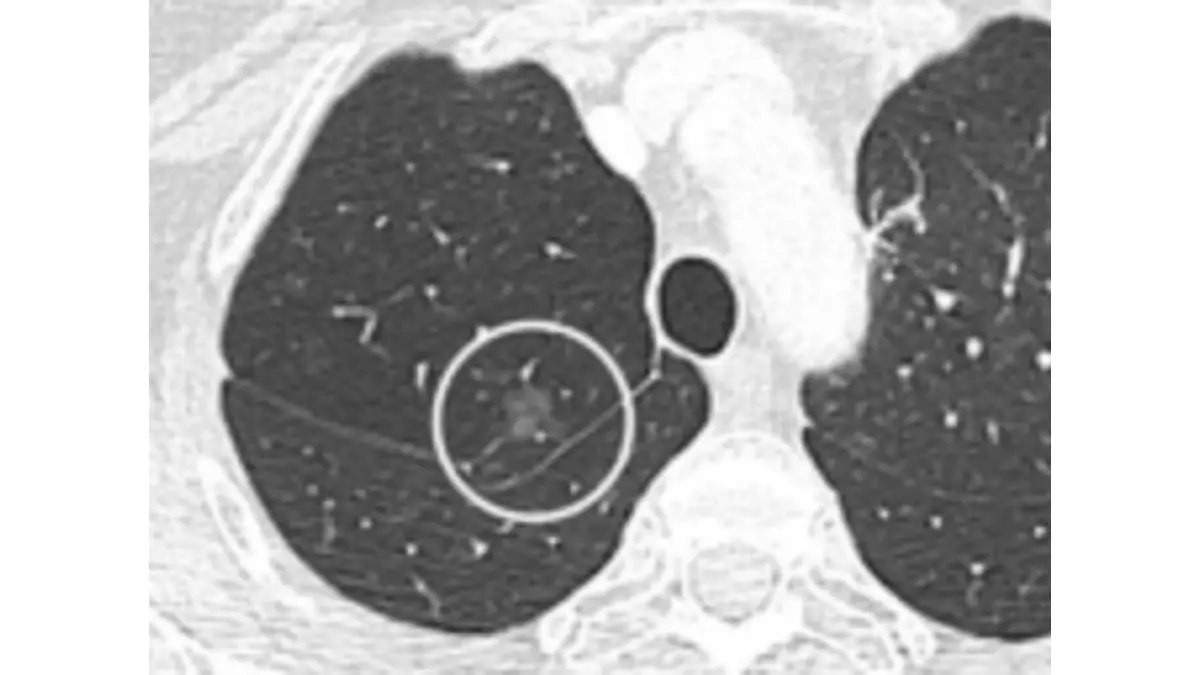
A pulmonary nodule is any small area of abnormal tissue density visible on a CT scan. The majority of nodules detected on LDCT screening are benign — caused by prior infections, scar tissue from healed inflammatory conditions, or calcified remnants of previous lung injuries. Most Lung-RADS 1, 2, and 3 results do not represent cancer.
🩺 Physician Note: “When I review a Lung-RADS 3 result with a patient, my message is consistent: a score of 3 means the radiologist identified something that warrants surveillance — not that you have cancer. A 6-month follow-up scan is a monitoring protocol. In my clinical experience reviewing these cases, the large majority of Lung-RADS 3 findings remain stable or resolve entirely on the next scan.” — Dr. Marcus A. Chen, MD, Pulmonology and Thoracic Radiology
When a finding leads to a biopsy or further testing
A Lung-RADS 4B result typically triggers a referral for tissue sampling — via bronchoscopy, CT-guided needle biopsy, or surgical resection depending on nodule location, size, and the patient’s overall health profile. This is not a cancer diagnosis. It means the finding has characteristics that require definitive tissue analysis to classify accurately.
✅ Patient Action: If your screening CT returns a Lung-RADS score of 3 or higher, ask a board-certified pulmonologist this specific question before your next appointment: “Based on this nodule’s size, density, and location, which follow-up protocol gives us the most diagnostic information with the lowest additional risk for my specific situation?”
Does insurance cover lung cancer screening — and what does it cost?
For most eligible Americans, annual LDCT lung cancer screening is covered at no out-of-pocket cost — but the pathway to that coverage differs depending on whether your plan is Medicare, private insurance, or an ACA marketplace plan. Understanding the specific requirement for each prevents the most common delay: arriving at the imaging center without the correct authorization in place.
Medicare coverage: what the shared decision-making visit requires
Medicare Part B covers annual LDCT screening for eligible beneficiaries at no cost-sharing — no copay, no deductible. One condition is mandatory before the first covered scan: the patient must complete a shared decision-making counseling visit with their ordering physician. This visit is a structured, documented appointment during which your physician discusses the benefits, limitations, and potential harms of screening. For current smokers, it includes cessation counseling. Without a completed and documented shared decision-making visit on record, Medicare will not reimburse the scan.
📊 Clinical Data Point: Medicare’s lung cancer screening benefit, including the shared decision-making visit requirement, age and smoking history eligibility criteria, and no-cost-sharing terms, is detailed on the Medicare preventive services lung cancer screening page — Source: Centers for Medicare and Medicaid Services (verify at publish for current 2026 coverage terms and reimbursement rules).
✅ Patient Action: Before scheduling your LDCT scan, ask your primary care physician or internist this specific question: “Can we complete the Medicare-required shared decision-making visit today and submit the LDCT order at the same appointment?” Completing both in one visit eliminates the most common scheduling barrier for Medicare beneficiaries.
Private insurance and ACA marketplace plans
All ACA-compliant private health insurance plans are required to cover USPSTF Grade B preventive services at no cost-sharing. Because lung cancer screening carries a current USPSTF Grade B recommendation, eligible adults with ACA-compliant plans receive the annual LDCT at no copay or deductible. Non-ACA-compliant plans, short-term health plans, and grandfathered plans may not carry this requirement — verify your plan type with your insurer directly before scheduling.
What if you don’t have insurance?
Federally Qualified Health Centers (FQHCs) provide preventive services including LDCT screening on a sliding-scale fee basis for uninsured and underinsured patients. Many NCI-designated cancer centers and major academic medical systems also operate financial assistance programs that can substantially reduce the cost of screening. Call the imaging center directly and ask specifically whether financial assistance is available for lung cancer screening — many facilities have social workers dedicated to navigating this process.
A lung cancer specialist’s perspective on who should not wait
🩺 Physician Note: “The patient I think about most is a 62-year-old man with a 38-pack-year history — a heavy smoker who had quit 12 years before we met. He had looked up his eligibility online and decided he was ‘probably fine’ because he hadn’t smoked in over a decade. He wasn’t experiencing symptoms. He felt well. He didn’t schedule a scan. Eighteen months later, he came to me with hemoptysis and imaging confirmed Stage IIIA disease. Under the current USPSTF criteria, he would have qualified for annual LDCT for the previous 12 years. That case changed how I open every shared decision-making conversation I have with a high-risk patient.” — Dr. Nathaniel J. Hargrove, MD, Oncology

The patients I wish I had seen sooner
The most consistent barrier I encounter is not a fear of the scan. It is self-exclusion — patients who apply the eligibility criteria themselves, apply them incorrectly, and conclude they don’t qualify when they do. The second most common barrier is the belief that quitting smoking eliminates the risk entirely. It substantially reduces risk over time. It does not eliminate it. Lung cancer risk in former heavy smokers remains elevated for decades after cessation — which is precisely why the USPSTF eligibility window extends 15 years beyond the quit date.
The patients who benefit most from this scan are the ones who feel fine right now.
One question to ask your doctor this week
If you are between 50 and 80 years old with a significant smoking history — current or former — there is one question that opens the right conversation with your physician:
✅ Patient Action: Ask your primary care physician or pulmonologist this week: “Based on my age and my exact smoking history, do I currently meet the USPSTF criteria for annual LDCT lung cancer screening — and if so, can we complete the shared decision-making visit and submit the referral today?” That question takes thirty seconds to ask. The answer can change your outcome.
Your next step toward lung cancer screening starts with one conversation
Annual LDCT lung cancer screening is among the most evidence-supported preventive tools available to high-risk adults in the United States. Eligibility is specific. The scan itself is brief. Coverage exists for most insured patients. The shared decision-making conversation with your physician is the entry point — and it takes one appointment.
If you are between 50 and 80 years old with a 20-pack-year or greater smoking history and you currently smoke or quit within the past 15 years, that conversation should happen at your next appointment.
Lung cancer screening: your most important questions answered
Q1: What is lung cancer screening?
Lung cancer screening is a preventive annual imaging test — specifically a low-dose CT scan — used to detect lung cancer in high-risk adults before symptoms develop. It produces detailed cross-sectional images that allow radiologists to identify small pulmonary nodules at early, more treatable stages. Consult a board-certified pulmonologist or primary care physician to determine whether lung cancer screening is appropriate for your specific situation.
Q2: Who should get screened for lung cancer?
Annual LDCT screening is recommended for adults aged 50 to 80 who have a smoking history of at least 20 pack-years and currently smoke or have quit within the past 15 years. These three criteria must all be met simultaneously under the current USPSTF recommendation. Consult a board-certified physician to confirm whether your age and exact smoking history meet the threshold for a covered screening referral.
Q3: At what age should you start lung cancer screening?
Annual lung cancer screening with LDCT is recommended beginning at age 50 for adults who meet both the pack-year and smoking status criteria. Screening continues through age 80, after which the risk-benefit ratio is reassessed individually. Consult a board-certified pulmonologist or your primary care physician to confirm eligibility based on your complete health history before scheduling.
Q4: How many pack-years do you need for lung cancer screening?
A minimum of 20 pack-years is required under current USPSTF criteria. Pack-years equal packs smoked per day multiplied by years smoked — one pack per day for 20 years equals 20 pack-years. Patients with intermittent smoking histories frequently underestimate their total. Consult a board-certified physician to confirm your exact pack-year calculation, particularly if your smoking pattern varied over time.
Q5: Is lung cancer screening covered by insurance?
Most ACA-compliant private health insurance plans cover annual LDCT lung cancer screening at no cost-sharing for eligible adults, as it carries a USPSTF Grade B recommendation. Non-ACA-compliant and grandfathered plans may not be required to cover it. Verify your specific plan type and current coverage terms directly with your insurer before scheduling your appointment.
Q6: Does Medicare cover lung cancer screening?
Medicare Part B covers annual LDCT lung cancer screening at no cost-sharing for eligible beneficiaries, provided the patient first completes a required shared decision-making counseling visit with their ordering physician. Without a completed and documented counseling visit, Medicare will not reimburse the scan. Contact your primary care physician to confirm eligibility and schedule the shared decision-making visit before the LDCT is ordered.
Q7: What is an LDCT scan?
An LDCT (low-dose computed tomography) scan is an FDA-cleared imaging test that produces three-dimensional cross-sectional images of the lungs using low-dose radiation. It requires no IV contrast, no fasting, and no undressing. The scan acquisition takes under five minutes. Consult a board-certified radiologist or pulmonologist to interpret your LDCT results within the full context of your clinical history.
Q8: How long does a lung cancer screening CT scan take?
The LDCT scan acquisition itself takes fewer than five minutes, with a single breath-hold of approximately 5 to 10 seconds during active imaging. Total appointment time — including check-in, positioning, and post-scan instructions — is typically 15 to 30 minutes. Results from the interpreting radiologist are generally available to your ordering physician within several business days.
Q9: What happens if a nodule is found during lung cancer screening?
A nodule finding is classified using the Lung-RADS scoring system. Lung-RADS 1 or 2 indicates no significant finding. Lung-RADS 3 typically requires a 6-month follow-up scan. Lung-RADS 4A or 4B warrants additional imaging or tissue sampling evaluation. Consult a board-certified pulmonologist or thoracic radiologist to understand what your specific Lung-RADS score means for your follow-up plan.
Q10: What is Lung-RADS and what do the numbers mean?
Lung-RADS is the American College of Radiology’s standardized system for classifying lung cancer screening CT findings. Scores range from 1 (no findings — continue annual screening) to 4B (highly suspicious — tissue sampling evaluation recommended). A score of 3 means a probably benign finding requiring a 6-month follow-up scan — not an immediate cancer diagnosis. Consult a board-certified pulmonologist to discuss the clinical meaning of your specific result.
Q11: What are the risks of lung cancer screening?
The primary risks of LDCT lung cancer screening include false-positive results requiring unnecessary follow-up procedures, overdiagnosis of clinically insignificant findings, cumulative radiation exposure from annual scanning, and psychological distress from uncertain results. These risks are weighed individually against the benefit of early detection. Consult a board-certified pulmonologist to evaluate your personal risk-benefit profile before beginning annual screening.
Q12: Can non-smokers get lung cancer screening?
Current USPSTF guidelines do not recommend routine LDCT lung cancer screening for non-smokers, as the clinical evidence was established in individuals with significant smoking histories. Non-smokers with substantial radon or asbestos exposure or a strong family history of lung cancer may benefit from an individualized risk discussion. Consult a board-certified pulmonologist to determine whether an off-guideline assessment is appropriate for your exposure profile.
Q13: How accurate is low-dose CT for detecting lung cancer?
LDCT is significantly more sensitive for early-stage lung nodule detection than chest X-ray, particularly for nodules in the 4–10 mm range where most early-stage cancers begin. It produces a meaningful false-positive rate, especially in the first screening round when no prior comparison scan is available. Accuracy improves in subsequent annual rounds. Consult a board-certified radiologist or pulmonologist to contextualize your specific findings accurately.
Q14: How do I prepare for a lung cancer screening CT scan?
LDCT screening preparation is minimal: wear comfortable, metal-free clothing on your chest; remove necklaces and underwire bras before the scan; no fasting is required; no IV will be placed. You will hold your breath for approximately 5 to 10 seconds during imaging. Confirm any facility-specific preparation requirements with the imaging center at the time you schedule your appointment.
Q15: Can LDCT lung cancer screening detect other conditions?
Yes — an LDCT scan designed for lung cancer screening can incidentally detect other clinically significant findings, including coronary artery calcification, aortic aneurysm, emphysema, and pleural abnormalities. Your radiologist will report significant incidental findings alongside the Lung-RADS result. Discuss any incidental finding with your ordering physician to determine whether additional evaluation is warranted and how urgently.
Q16: What is a shared decision-making visit for lung cancer screening?
A shared decision-making visit is a structured counseling appointment — required by Medicare before your first covered LDCT scan — in which your physician documents a discussion of screening benefits, limitations, potential harms, your personal risk factors, and cessation counseling if you currently smoke. Consult your primary care physician or a board-certified internist to schedule and document this required visit before submitting the LDCT order.
Q17: What is the difference between lung cancer screening and a chest X-ray?
A chest X-ray produces a two-dimensional image that cannot reliably detect pulmonary nodules smaller than approximately 1 centimeter. An LDCT scan produces three-dimensional cross-sectional images capable of detecting nodules as small as 4 to 6 millimeters. Current USPSTF, NCI, and NCCN guidance does not recommend chest X-ray as a substitute for LDCT in lung cancer screening for any eligible risk group.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.