On This Page – Quick Medical Summary
What does it mean when lung cancer has spread?
Learning that lung cancer metastasis has occurred — that the disease has traveled beyond the original tumor in your lung — is one of the most difficult moments in a cancer diagnosis. This guide is written for the patient who just received that news, the caregiver researching from home after a difficult phone call, and the person waiting for imaging results who wants to be prepared before the next appointment.
Our complete guide to lung cancer explains how this disease begins. This article covers where it goes, how to recognize the warning signs, and what current treatments can offer even at stage 4.
Is this the same as stage 4 lung cancer?
Yes — by definition, metastatic lung cancer has reached a distant organ, and that finding places the disease in stage 4. Stages 1 through 3 involve the lung and regional lymph nodes. Stage 4 means the cancer has arrived somewhere beyond the chest — the brain, bones, liver, adrenal glands, or other distant sites.
How to use this guide based on your situation
- Stage 4 diagnosis just confirmed: Sections 3 and 6 cover the most common metastatic organs and the treatment options targeting each.
- Experiencing new or worsening symptoms: Section 4 maps each symptom cluster to its likely organ source — including when to go to the emergency department.
- Awaiting imaging or biopsy results: Section 5 walks through the full diagnostic sequence your oncologist will follow.
- Caregiving for a family member: Sections 4 and 7 include caregiver-specific guidance throughout.
ℹ️ Medical Disclaimer: The diagnostic criteria, staging classifications, treatment protocols, medication information, and survival data discussed in this article reflect current clinical standards and are provided for educational purposes only. Individual diagnostic conclusions, treatment decisions, drug selection, and prognosis depend on tumor histology, biomarker profile, performance status, organ function, comorbidities, and specialist evaluation. Consult a board-certified oncologist before acting on any clinical information in this article.
How lung cancer spreads through your body
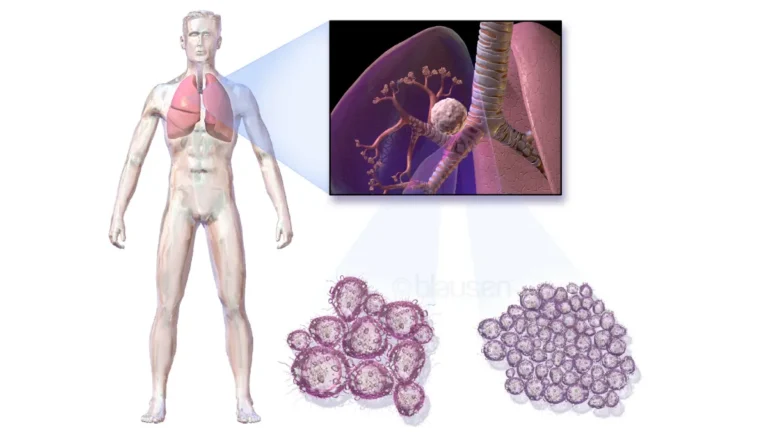
Lung cancer spreads through the body via two primary pathways: the bloodstream (hematogenous spread) and the lymphatic system.
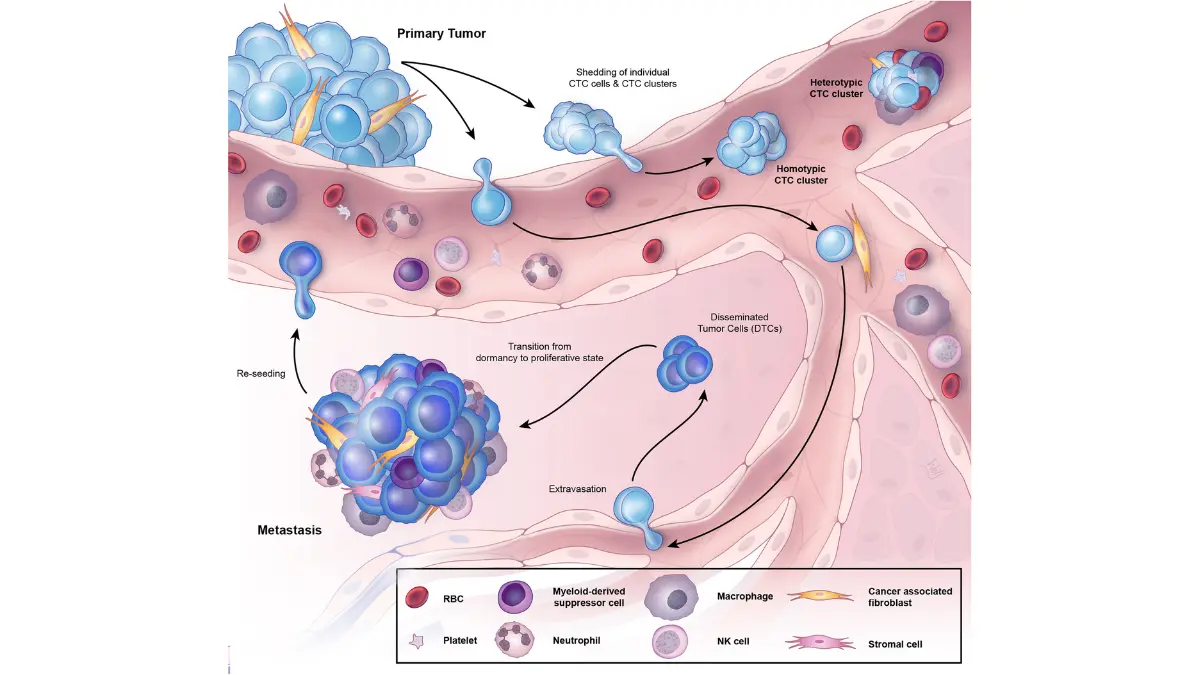
Tumor cells undergo a process called epithelial-mesenchymal transition (EMT) — they shed the adhesion proteins that anchor them to the primary tumor, enter circulation as free-floating circulating tumor cells (CTCs), and travel throughout the body. The immune system destroys the vast majority. The fraction that survives exits at distant organs, reactivates adhesion properties, and establishes secondary tumors.
🔬 How It Works: A lung cancer cell detaches from the primary mass → enters a blood vessel or lymphatic channel → survives immune surveillance in circulation → exits through a distant organ’s vessel wall → reanchors and begins dividing. This step-by-step process — the metastatic cascade — is what transforms a localized lung tumor into systemic disease.
The two routes: bloodstream and lymphatic system
Hematogenous spread — via the bloodstream — drives distant metastasis to the brain, liver, bone, and adrenal glands. Lymphatic dissemination moves tumor cells through the lymphatic system toward regional lymph nodes first, then progressively to more distant sites. Both pathways can operate simultaneously, which is why a newly staged patient can present with metastases in multiple organ systems at the same time.
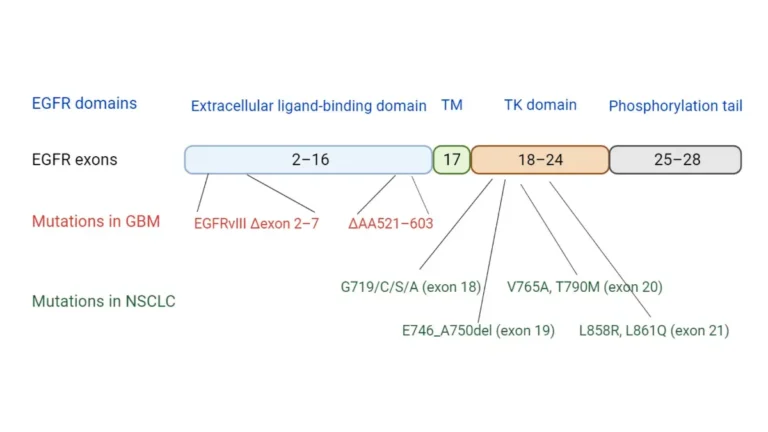
Why biomarker profile affects where cancer spreads
Driver mutation status influences not just which treatments work — it influences where the cancer travels. EGFR-mutant NSCLC shows a documented higher propensity for brain colonization. KRAS-mutant tumors more frequently seed the liver and adrenal glands. SCLC disseminates earlier and more widely than NSCLC, often before the primary diagnosis is confirmed, because of its neuroendocrine biology and rapid cell division rate. The biological and clinical differences between NSCLC and SCLC explain why two patients at the same stage can have completely different patterns of organ involvement.
🩺 Physician Note: In my clinical practice, the patients most blindsided by a new metastatic site are those whose molecular testing was incomplete at initial staging. Comprehensive biomarker profiling — EGFR, ALK, ROS1, KRAS, PD-L1, MET — belongs at the start of the workup. It tells you not just what to treat, but where to watch most carefully.
For the current clinical framework of lung cancer dissemination, the National Cancer Institute’s lung cancer resources provide physician-reviewed overviews updated with emerging 2026 evidence (verify specific page at publish).
The five organs lung cancer most commonly targets
Lung cancer does not spread randomly. It follows predictable anatomical and molecular pathways that oncologists have mapped across thousands of cases. The five most common destination sites — and what each one means clinically — are outlined below.
The five primary metastatic sites
The following table maps each common metastatic site to its clinical significance, key warning symptoms, NSCLC vs. SCLC pattern differences, and treatment implications. Incidence estimates should be verified against the American Cancer Society’s 2026 lung cancer statistics at publish time.
| Metastatic Site | Why Lung Cancer Targets It | Key Warning Symptoms | NSCLC vs. SCLC Pattern | Treatment Implication |
|---|---|---|---|---|
| Brain | Rich blood supply; EGFR-mutant tumors show documented CNS tropism | Morning headaches, confusion, seizures, one-sided weakness | NSCLC (EGFR-mutant especially); SCLC also common — prophylactic cranial irradiation used in limited-stage SCLC | SRS for 1–3 lesions; osimertinib has CNS penetration in EGFR-mutant disease |
| Bone | Bone marrow vascularity; metabolic environment supports tumor seeding | Deep bone pain worse at night, pathological fractures, hypercalcemia | Most common distant site in both types | Bone-modifying agents (denosumab, zoledronic acid); SRS for isolated lesions |
| Liver | Portal circulation; metabolic environment | Often asymptomatic early; right-upper-quadrant pain, jaundice, weight loss at higher burden | Both types; may alter chemotherapy dosing due to impaired drug metabolism | Systemic therapy; liver function must be monitored for dosing adjustments |
| Adrenal Glands | High vascularity and adrenocortical environment | Usually asymptomatic — detected incidentally on CT staging | More common in NSCLC; frequently bilateral | Systemic therapy; adrenalectomy considered in selected oligometastatic cases |
| Distant Lymph Nodes | Lymphatic drainage patterns from primary tumor site | Often asymptomatic; supraclavicular or cervical nodes may be palpable | Both types | Systemic therapy; radiation in selected oligometastatic presentations |
Source: Verify 2026 incidence figures at publish time from NCI SEER lung cancer statistics.
📊 Clinical Data Point: Population-level 5-year survival for distant-stage lung cancer continues to improve with biomarker-matched therapies. Verify the most current stage-specific survival estimates from the NCI SEER database (2026) at publish time — do not substitute 2025 or earlier figures. Source: NCI SEER, 2026 (verify at publish).
Understanding the lung cancer staging system provides the clinical framework for interpreting what each metastatic site means for treatment eligibility and prognosis. For a complete breakdown of stage-specific survival data, our lung cancer statistics and survival rates guide covers the current population-level data in full.
✅ Patient Action: If imaging has identified metastasis in a specific organ, ask your board-certified oncologist at your next appointment: “Given where the cancer has spread, am I eligible for site-directed therapy — such as stereotactic radiosurgery for a brain or bone lesion — in addition to systemic treatment?” The answer can change your treatment plan significantly.
Symptoms that may mean lung cancer has spread
New symptoms in a patient with lung cancer are not always easy to interpret. Some are dramatic and unmistakable. Others — particularly from liver or adrenal metastasis — are subtle enough to be mistaken for fatigue or side effects of treatment. Knowing which symptom cluster points to which organ site helps you act at the right speed.
Brain metastasis symptoms: headaches, confusion, and seizures
The symptom that most consistently signals brain metastasis is a headache that is worst when you first wake up and improves noticeably once you have been upright for 20 to 30 minutes. This positional pattern reflects raised intracranial pressure — the brain’s reaction to an expanding tumor inside a fixed skull. Other brain metastasis symptoms include confusion or personality changes noticed by a caregiver before the patient is aware of them, new visual disturbances, weakness affecting one side of the body, and first-time seizures in an adult with no prior history.
⚠️ Clinical Warning: A sudden severe headache unlike any previous headache, a first-time seizure, or acute confusion in a lung cancer patient is a neurological emergency. Go to the emergency department immediately — do not call the oncology office and wait for a callback. These symptoms can signal acute intracranial bleeding from a metastatic lesion and require same-day CT or MRI evaluation.
Bone metastasis: pain, fractures, and hypercalcemia
Bone metastasis produces a deep, persistent aching pain in the back, hips, ribs, or long bones that worsens at night and is not relieved by over-the-counter pain medication. Some patients experience a fracture from minimal trauma — a pathological fracture — before any pain has been recognized. The symptom cluster that most oncologists wish patients knew to watch for is hypercalcemia: fatigue, excessive thirst, constipation, and confusion appearing in a lung cancer patient on no new medications. This combination should prompt a same-day call to your oncologist for a serum calcium level, not a wait-and-see approach.
Liver and adrenal metastasis: the silent spreaders
Liver metastasis is often asymptomatic in its early stages and detected only on imaging. As tumor burden increases, right-upper-quadrant abdominal discomfort, unexplained weight loss, jaundice (yellowing of the skin or eyes), and loss of appetite can develop. Adrenal metastasis is almost always asymptomatic and found incidentally on CT staging scans — which is one reason routine complete staging imaging matters even when a patient feels well.
If you or a family member is experiencing any of these symptoms, the early warning signs of lung cancer guide provides additional clinical context on the full symptom spectrum. Use our Symptom Checker to log and organize new or changing symptoms before your next oncology appointment — a documented symptom timeline is one of the most useful tools you can bring to that visit.
✅ Patient Action: If you notice any of the brain symptoms described above — especially morning headaches, confusion, or one-sided weakness — contact your oncologist the same day. For neurological symptoms that appear suddenly, go directly to the emergency department. Do not self-diagnose or assume the symptom is medication-related without same-day evaluation.
How doctors confirm lung cancer has spread
Confirming lung cancer metastasis requires a sequence of imaging and molecular tests, typically in this order:
- CT scan of the chest, abdomen, and pelvis — the initial staging scan that identifies visible tumor deposits in the lungs, liver, adrenal glands, and lymph nodes
- Brain MRI with contrast — ordered for any neurological symptom, or when staging indicates a high probability of CNS involvement; MRI detects leptomeningeal disease and small parenchymal lesions that CT misses
- PET-CT scan — identifies metabolically active tumor deposits throughout the body, often revealing sites not visible on standard CT
- Tissue biopsy of a metastatic site — confirms spread histologically and enables molecular profiling of the metastatic lesion
- Liquid biopsy (ctDNA blood test) — detects circulating tumor DNA carrying driver mutations without requiring an invasive tissue sample
Imaging: CT, MRI, and PET-CT
The distinction between CT and MRI matters clinically. CT is faster and covers more anatomical territory; MRI with contrast has superior sensitivity for brain metastases, particularly small lesions and leptomeningeal spread — the involvement of the membranes lining the brain and spinal cord. Your oncologist may order both. The complete lung cancer CT scan guide explains what each imaging type detects and what the results mean for staging.
Tissue biopsy and liquid biopsy for biomarker testing
🔬 How It Works: A liquid biopsy is a standard blood draw that analyzes circulating tumor DNA (ctDNA) shed into the bloodstream by lung cancer cells. It can identify driver mutations — EGFR, ALK, ROS1, KRAS G12C, MET exon 14 — that determine which targeted therapies will work. Results are typically available within seven to fourteen days. Liquid biopsy does not replace tissue biopsy in all clinical situations, but it provides actionable molecular data when a tissue sample is not safely accessible.
Understanding how biopsies are performed and interpreted is covered in our guide to lung biopsy for lung cancer. For a full overview of all diagnostic tests used in lung cancer staging, our lung cancer diagnosis guide walks through each step in patient-accessible terms.
Patients whose biomarker results suggest eligibility for investigational agents can search active clinical trials in metastatic lung cancer on ClinicalTrials.gov by mutation profile and geographic location.
✅ Patient Action: Before your diagnostic workup is finalized, ask your board-certified thoracic oncologist: “Has comprehensive biomarker testing been ordered — including EGFR, ALK, ROS1, PD-L1, KRAS, and MET — alongside my imaging?” Biomarker results determine which systemic therapies are appropriate for your specific case. No treatment decision should be made before a complete molecular profile is available.
Treatment options when lung cancer has spread
Receiving a metastatic diagnosis is not a single event with a single treatment path. Metastatic lung cancer treatment is driven entirely by the molecular profile of the tumor — and two patients with stage 4 disease may receive entirely different first-line therapies because their biomarker results point in different directions.
Targeted therapy for EGFR, ALK, and ROS1 mutations
For patients with EGFR-mutant NSCLC, osimertinib (Tagrisso) is the established first-line targeted therapy. Its clinical significance extends beyond efficacy — osimertinib penetrates the blood-brain barrier, making it the preferred choice specifically when brain metastases are present in EGFR-positive patients. This CNS-penetrant pharmacology distinguishes it from earlier-generation EGFR inhibitors and reduces the need for immediate brain radiation in eligible patients. For ALK-positive NSCLC, alectinib (Alecensa) or brigatinib are first-line options with strong CNS activity. ROS1-rearranged NSCLC responds to entrectinib or crizotinib. All of these targeted options require confirmed biomarker status before prescribing — a full explanation of EGFR, ALK, and ROS1 testing and their treatment implications is covered in our guide to targeted therapy for EGFR and ALK lung cancer.
Immunotherapy: when PD-L1 expression drives the decision
Patients with PD-L1 expression ≥50% and no actionable driver mutation may receive pembrolizumab (Keytruda) monotherapy as first-line therapy. Those with lower PD-L1 expression typically receive pembrolizumab in combination with platinum-based chemotherapy. PD-L1 testing must be completed before initiating immunotherapy — the threshold determines whether monotherapy or combination is appropriate. A detailed overview of how these agents work is available in our guide to immunotherapy for lung cancer.
Site-directed therapy: treating brain and bone metastases
Metastatic lung cancer in the brain does not automatically mean whole-brain radiation therapy (WBRT). Patients with one to three discrete brain metastases are often candidates for stereotactic radiosurgery (SRS), which delivers high-dose, precisely targeted radiation to each lesion individually — preserving the surrounding healthy brain tissue and reducing the neurocognitive side effects associated with WBRT. Your oncologist will assess lesion number, size, and location to determine whether SRS is appropriate. For bone metastases, bone-modifying agents such as denosumab or zoledronic acid reduce the risk of skeletal complications including pathological fractures.
🩺 Physician Note: The single most consequential mistake I see in newly diagnosed metastatic lung cancer patients is beginning treatment before biomarker results are available. Administering chemotherapy to a patient who will respond to osimertinib is not a neutral choice — it delays effective therapy and may compromise organ function for subsequent targeted treatment. Wait for the molecular profile. That result changes everything.
Drug approval status for osimertinib, alectinib, and pembrolizumab should be verified against FDA-approved therapies for lung cancer at publish time to confirm current label indications (verify at publish).
✅ Patient Action: Before any systemic treatment begins, ask your board-certified thoracic oncologist: “Has my full biomarker panel — EGFR, ALK, ROS1, PD-L1, KRAS, MET, and RET — been completed? Which result is driving this treatment recommendation?” Treatment selection in metastatic NSCLC is biomarker-driven. No therapy should begin before that molecular profile is in hand.
What your oncologist wants you to know about metastatic lung cancer
Survival statistics: what they mean and what they miss
When I sit across from a patient who has just been told their lung cancer has spread, one of the most important things I can say is this: the survival statistics you find online are population averages. They are calculated from all patients with distant-stage lung cancer — including those diagnosed before targeted therapies existed, those with no actionable mutations, and those who were diagnosed late with high tumor burden.
Those numbers do not describe a patient with EGFR-mutant NSCLC on osimertinib, or a patient with ALK-positive disease on alectinib. Those patients, in clinical practice, can achieve disease control measured in years — not the months the raw statistics imply.
Palliative care is not giving up — it is expert symptom support
The other conversation I have at nearly every metastatic diagnosis is about palliative care. Most patients hear “palliative” and assume it means end-of-life. It does not. Palliative care is specialist-level symptom management — pain, fatigue, breathlessness, nausea, anxiety — that runs alongside active treatment, not instead of it. NCCN guidelines for stage 4 NSCLC specifically recommend early palliative care integration for all patients with metastatic disease (verify 2026 NCCN guidelines at publish). Research consistently shows that patients who receive concurrent palliative care alongside systemic therapy report better quality of life — and in some trials, longer survival.
If the emotional weight of a metastatic diagnosis is affecting daily life, our guide to lung cancer and mental health addresses the psychological dimension that clinical appointments often leave unaddressed.
✅ Patient Action: At your next oncology appointment, ask: “Can I be referred to a palliative care specialist now, while I am still on active treatment?” You do not need to be at end of life to benefit from expert symptom management. NCCN guidelines support this referral from the time of metastatic diagnosis.
Frequently asked questions about lung cancer metastasis
1. Where does lung cancer spread first?
Lung cancer metastasis most commonly reaches the brain, bones, liver, adrenal glands, and distant lymph nodes. The order varies by tumor biology. SCLC disseminates more rapidly and widely than NSCLC — often before the primary diagnosis is confirmed. EGFR-mutant NSCLC shows a higher propensity for early brain involvement than other NSCLC subtypes. Consult a board-certified oncologist to discuss which sites require monitoring based on your specific tumor profile.
2. What are the signs lung cancer has spread to the brain?
Brain metastasis from lung cancer metastasis produces headaches worst on waking that improve once upright, confusion, memory lapses, visual disturbances, weakness on one side, or a first-time seizure. These symptoms reflect raised intracranial pressure or focal neurological injury. If sudden confusion, acute severe headache, or a first seizure occurs, go to the emergency department immediately — this is a neurological emergency, not a symptom to monitor at home.
3. What is the survival rate for metastatic lung cancer?
Population-level survival for metastatic lung cancer (stage 4) is significantly lower than for localized disease — and improving with biomarker-matched therapies. Patients with EGFR or ALK driver mutations on targeted therapy show substantially better outcomes than population averages reflect. Verify the most current 5-year survival estimates from the NCI SEER 2026 database at publish time — do not substitute figures from 2025 or earlier. Consult a board-certified oncologist to interpret any statistic in the context of your molecular profile.
4. How does lung cancer spread through the body?
Metastatic lung cancer travels via the bloodstream (hematogenous spread) and the lymphatic system. Tumor cells undergo epithelial-mesenchymal transition — detaching from the primary mass, entering circulation, surviving immune clearance, and colonizing distant organs. This process can seed multiple organs simultaneously. SCLC spreads faster than NSCLC because of its aggressive neuroendocrine biology. Driver mutation status also influences which organs the cancer is most likely to target.
5. Can metastatic lung cancer be cured?
Metastatic lung cancer is not generally considered curable with current standard therapies, but it can be managed as a chronic condition in patients with actionable mutations. Those with EGFR-mutant NSCLC on osimertinib or ALK-positive disease on alectinib may achieve durable disease control lasting years. Clinical trials offer additional pathways beyond standard options. Consult a board-certified oncologist to determine whether your biomarker profile makes you eligible for therapies with prolonged response rates.
6. What does bone metastasis from lung cancer feel like?
Bone metastasis from lung cancer metastasis causes deep, persistent pain in the back, hips, ribs, or long bones — typically worse at night and unresponsive to standard over-the-counter pain relief. Pathological fractures can occur from minimal trauma. Hypercalcemia — elevated calcium from bone breakdown — produces fatigue, excessive thirst, constipation, and confusion. This symptom cluster in a lung cancer patient should prompt a same-day call to your oncologist for a serum calcium check.
7. How fast does lung cancer spread?
The pace of lung cancer metastasis depends on tumor subtype and driver mutation. SCLC can disseminate before the primary diagnosis is confirmed. NSCLC with aggressive histology — large cell neuroendocrine carcinoma — spreads faster than adenocarcinoma with an EGFR mutation. No single timeline applies across all cases. Ask your oncologist what imaging frequency is appropriate for your specific tumor biology to ensure new metastases are detected early, before they produce symptoms.
8. What happens when lung cancer spreads to the liver?
Liver metastasis from metastatic lung cancer is often asymptomatic in early stages, detected only on routine staging imaging. As tumor burden increases, right-upper-quadrant abdominal discomfort, unexplained weight loss, decreased appetite, jaundice, and fatigue can develop. Liver function tests typically show elevated AST, ALT, or bilirubin. Significant liver involvement can impair drug metabolism and affect chemotherapy dosing tolerability. Consult a board-certified oncologist to assess liver function and its impact on your treatment plan.
9. Is stage 4 lung cancer always metastatic?
Yes — by definition, stage 4 lung cancer metastasis has spread to a distant organ. Stage 4A indicates spread to a single distant organ, the opposite lung, or a malignant pleural or pericardial effusion. Stage 4B indicates metastases in two or more distant organs. Staging is determined through CT, brain MRI, and PET-CT imaging. Consult a board-certified oncologist to confirm your exact staging classification and discuss what it means for your treatment options.
10. How do doctors diagnose lung cancer metastasis?
Diagnosing lung cancer metastasis begins with a CT scan of the chest, abdomen, and pelvis, followed by a brain MRI with contrast. A PET-CT scan identifies additional sites of metabolic activity not visible on CT. Tissue or liquid biopsy of a metastatic site confirms spread and enables EGFR, ALK, ROS1, and PD-L1 biomarker testing. Consult a board-certified thoracic oncologist to determine the appropriate diagnostic sequence and confirm comprehensive molecular testing is included.
11. What treatments are available for metastatic lung cancer?
Treatment for metastatic lung cancer is determined entirely by biomarker results. EGFR-mutant NSCLC is treated with osimertinib (Tagrisso) as first-line therapy. ALK-positive NSCLC responds to alectinib (Alecensa) or brigatinib. PD-L1 ≥50% with no driver mutation may qualify for pembrolizumab (Keytruda) monotherapy. Chemotherapy combinations and clinical trials are additional options. Consult a board-certified oncologist to confirm your biomarker status before any treatment decision is made.
12. Does lung cancer always spread?
Not all lung cancer metastasis is inevitable. Early-stage NSCLC detected before lymph node involvement can often be surgically resected with curative intent. However, lung cancer has high metastatic potential due to its proximity to major blood vessels and lymphatic channels. A significant proportion of US lung cancer cases are diagnosed at distant stage — verify the current NCI figure at publish time. Low-dose CT screening reduces the proportion of patients diagnosed at advanced stages.
13. What organs can lung cancer spread to?
Lung cancer metastasis most commonly involves the brain, bones, liver, adrenal glands, and distant lymph nodes. Less commonly, it spreads to the kidneys, skin (cutaneous metastasis), pericardium (causing malignant effusion), and the opposite lung. SCLC can involve the bone marrow. Imaging is the only reliable method for determining which organs are affected — metastasis to the liver and adrenal glands is often asymptomatic in early stages and discovered only on staging CT scans.
14. Can lung cancer spread to the heart?
Yes — lung cancer metastasis can reach the pericardium, the membrane surrounding the heart, causing a malignant pericardial effusion. This is less common than brain, bone, or liver involvement but clinically serious. Symptoms include shortness of breath, chest pressure, arrhythmia, and reduced exercise tolerance. Severe cases can cause cardiac tamponade, a life-threatening compression of the heart. If these symptoms appear, seek emergency evaluation immediately, and ask for joint management by your oncologist and a board-certified cardiologist.
15. What is the difference between local and distant metastasis?
In lung cancer metastasis, regional spread refers to nearby lymph nodes within the chest — this defines stage 3 disease, which may still be treated with curative intent using combined chemotherapy and radiation. Distant metastasis means cancer has traveled to an organ beyond the chest — the brain, liver, bones, or adrenal glands — defining stage 4 disease. The distinction is clinically critical because it determines whether the treatment goal is curative or disease-controlling.
16. What is a liquid biopsy and how is it used in metastatic lung cancer?
A liquid biopsy is a blood test that detects circulating tumor DNA (ctDNA) shed by metastatic lung cancer cells into the bloodstream. It identifies driver mutations — EGFR, ALK, ROS1, KRAS G12C, MET exon 14 — without requiring an invasive tissue biopsy. It also monitors treatment response and detects resistance mutations as they emerge. Consult a board-certified oncologist to determine whether liquid biopsy is the appropriate first step in your diagnostic workup or whether tissue biopsy is also needed.
17. What questions should I ask my oncologist about metastasis?
When discussing lung cancer metastasis, ask your oncologist: Has my tumor been fully tested for EGFR, ALK, ROS1, PD-L1, KRAS, MET, and RET mutations? Which organs are currently affected? Am I eligible for targeted therapy, immunotherapy, or stereotactic radiosurgery for specific lesions? Is palliative care available to me now, alongside active treatment? Are there clinical trials open for my biomarker profile? What imaging schedule will monitor for new metastatic sites?
Your next steps after a lung cancer metastasis diagnosis
The landscape of metastatic lung cancer treatment has changed profoundly. Biomarker-matched targeted therapies and immunotherapy have created patient subgroups whose outcomes bear little resemblance to the statistics of a decade ago.
Three actions matter most immediately. First: confirm all metastatic sites with complete staging imaging — CT of the chest, abdomen, and pelvis, plus a brain MRI with contrast. Second: ensure comprehensive molecular testing has been completed before any systemic treatment begins — EGFR, ALK, ROS1, PD-L1, KRAS, MET. Third: ask about a palliative care referral now, not at end of life.
The right oncology team, the right molecular results, and the right questions change what is possible. You are already asking them.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.