On This Page – Quick Medical Summary
A lung cancer CT scan — specifically a low-dose CT (LDCT) — is a painless, 10–30 minute imaging test that can detect lung nodules as small as 3mm, often years before symptoms appear. Your results are scored using the Lung-RADS system (0–4X). A score of 1–2 means no immediate concern. A score of 3–4 requires follow-up action. This guide decodes exactly what happens before, during, and after your scan — in plain English.
Who Needs a Lung Cancer CT Scan in 2026?
The Case That Changed Everything
Marcus, a 57-year-old former factory worker from Ohio, had no symptoms. No cough, no chest pain — nothing. His doctor recommended an annual lung cancer CT scan based on his 25-year smoking history. The scan revealed a 9mm solid nodule in his right lower lobe. Six weeks later, a biopsy confirmed Stage IA non-small cell lung cancer. He underwent surgical resection. Three years later, he is cancer-free.
This is exactly why screening exists.
Who Qualifies for a Lung Cancer CT Scan?
According to the U.S. Preventive Services Task Force (USPSTF), annual low-dose CT screening is recommended for adults who meet all three of these criteria:
- Age: 50 to 80 years old
- Smoking history: 20 or more pack-years (e.g., 1 pack/day for 20 years, or 2 packs/day for 10 years)
- Current smoker OR quit within the last 15 years
Medicare covers annual LDCT screening at $0 cost for qualifying individuals.
Eligibility by Country: 2026 Comparison
| Country | Age Range | Smoking Criteria | Cost Coverage |
|---|---|---|---|
| USA | 50–80 | 20 pack-years; quit ≤15 yrs ago | Medicare: $0 cost-share |
| UK (NHS) | 55–74 (pilot areas) | High-risk score (LLP tool) | Free via NHS |
| Canada | 55–74 | 30 pack-years; quit ≤15 yrs ago | Covered in select provinces |
| Australia | 50–70 | Pilot programme (expanding 2026) | Partially subsidised via MBS |
Know the difference: A lung cancer screening LDCT is a low-radiation, preventive scan for high-risk individuals with no symptoms. A diagnostic chest CT is ordered when symptoms already exist — it uses standard radiation doses and looks for a wider range of conditions. They are not interchangeable. If you are unsure which applies to you, use our Genetic Risk Assessment Tool to evaluate your personal risk profile before speaking with your doctor.
The CDC confirms that annual LDCT screening reduces lung cancer mortality by up to 20% in high-risk adults — a finding from the landmark National Lung Screening Trial (NLST).
What Happens During a Lung Cancer CT Scan?
Before Your Scan
Preparation is minimal — which surprises most patients.
- No fasting required. Eat and drink normally.
- No contrast dye is used for screening LDCT (unlike some diagnostic CT scans).
- Wear comfortable, metal-free clothing. You will not need to change into a gown in most centres.
- Reschedule if you have a respiratory infection. Active infections can appear as nodules and skew results.
- Inform your technologist if you are pregnant or may be pregnant.
If you are already tracking symptoms that brought you to this point, our Symptom Checker can help you document them clearly for your care team.
During the Scan: Step by Step
- You lie flat on your back on a sliding CT table.
- The table moves slowly through a large, doughnut-shaped scanner.
- You will be asked to hold your breath for 5–10 seconds — this prevents blurring.
- The scan itself takes less than 2 minutes. The full visit is typically 10–30 minutes.
- No injections. No pain. No claustrophobia risk (the scanner is open, not a closed tube like an MRI).
After the Scan
- You can resume all normal activities immediately — no recovery time needed.
- Results are typically available within 1–2 business days.
- Your results may appear on your patient portal before your doctor calls — don’t panic if you see them early without context.
LDCT vs. Standard CT vs. Chest X-Ray: Key Differences
| Feature | Screening LDCT | Diagnostic Chest CT | Chest X-Ray |
|---|---|---|---|
| Radiation dose | ~1.5 mSv (up to 90% less) | ~7 mSv | ~0.1 mSv |
| Nodule detection | ≥3mm | ≥5mm | ≥10mm |
| Contrast dye | No | Sometimes | No |
| Purpose | Preventive screening | Symptom investigation | Initial assessment |
| Cost (uninsured) | $200–$500 | $800–$2,500 | $100–$300 |
According to RadiologyInfo.org, the low-dose format uses X-ray beams to produce cross-sectional images while exposing patients to a fraction of conventional CT radiation.
How to Read Your Lung Cancer CT Scan Radiology Report
This is the section no competitor adequately covers — and the one that causes patients the most anxiety.
The 5 Sections of Every Radiology Report
| Report Section | What It Contains |
|---|---|
| Clinical History | Why you had the scan (age, smoking history) |
| Comparison/Priors | How results compare to your previous scans |
| Technique | Type of scan performed, radiation parameters |
| Findings | Objective description of everything the radiologist saw |
| Impression | The radiologist’s summary — read this first |
💡 Pro Tip: Skip to the “Impression” section first. It contains the radiologist’s most important conclusions in 2–4 sentences.
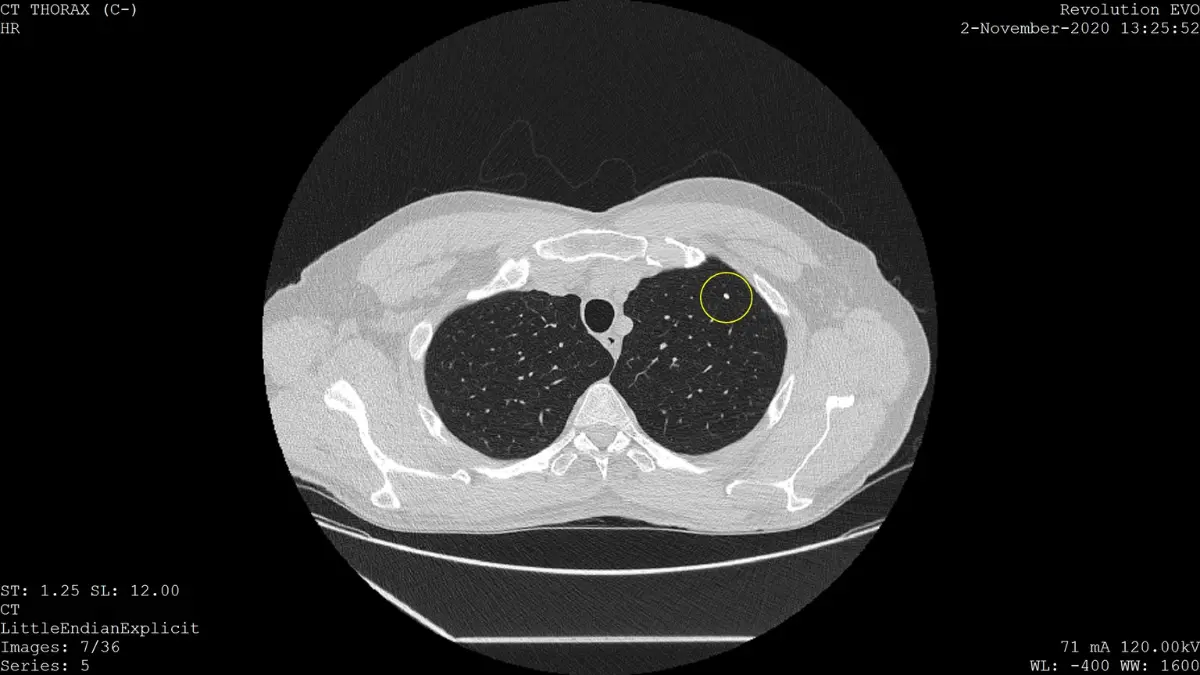
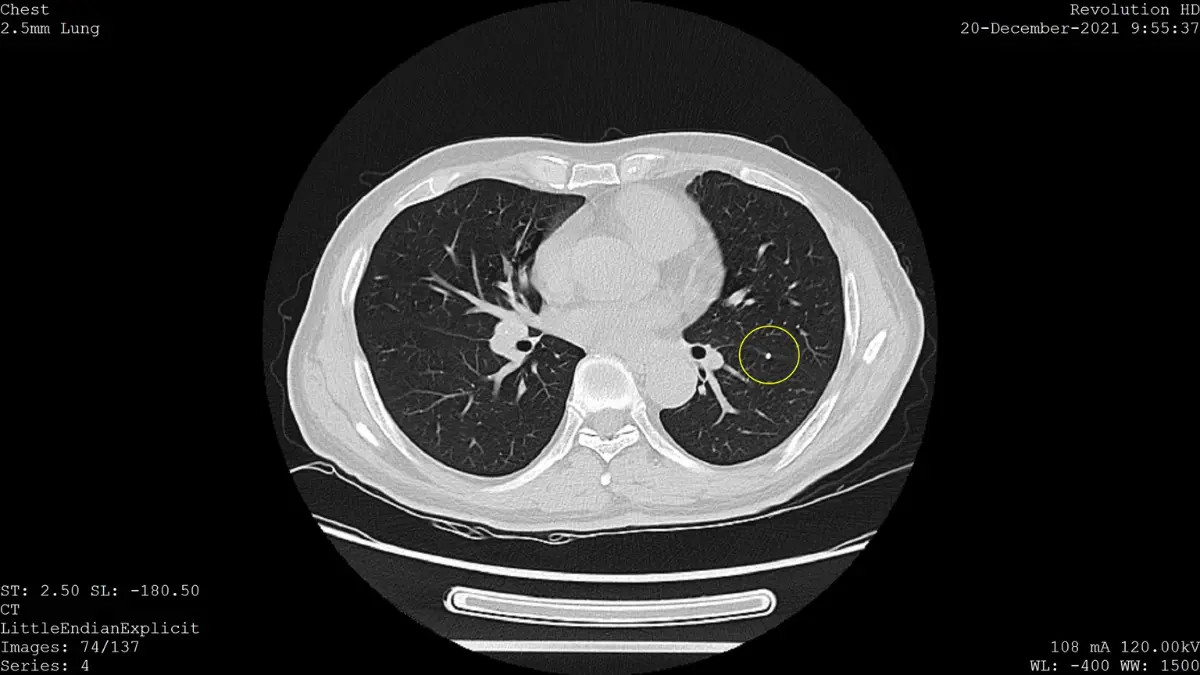
Understanding Lung Nodules on CT Scan
A pulmonary nodule is a spot on the lung smaller than 3cm. Nodules larger than 3cm are called masses and are treated with higher urgency.
Most nodules are not cancer. According to research published via PMC/NIH, over 96% of positive LDCT screens do not result in a lung cancer diagnosis.
Nodule Type Comparison Table
| Nodule Type | CT Appearance | Malignancy Risk | Typical Next Step |
|---|---|---|---|
| Solid | Fully opaque, uniform density | Varies by size (higher if >6mm) | 6–12 month follow-up or biopsy |
| Part-Solid (Semi-Solid) | Mixed: solid core + hazy outer ring | Higher risk per mm than solid | Closer surveillance; possible biopsy |
| Ground-Glass Opacity (GGO) | Hazy, cloud-like; vessels visible through it | Usually lower, but requires monitoring | Annual LDCT |
| Calcified | Bright/white on CT | Almost always benign | No follow-up needed |
Medical Jargon Decoder
These terms appear in nearly every radiology report — decoded here:
- “Unremarkable” = Normal; nothing concerning found
- “Spiculated margins” = Irregular, star-like edges = higher cancer concern
- “Atelectasis” = Partial collapse of lung tissue (often benign)
- “Lymphadenopathy” = Enlarged lymph nodes (may indicate spread or infection)
- “Consolidation” = Lung tissue filled with fluid or cells instead of air
- “Emphysema” = Damage to air sacs — graded mild, moderate, or severe
- “Coronary artery calcification” = Plaque in heart arteries — an incidental finding flagged even on lung scans
“Incidental findings” are discoveries unrelated to lung cancer (e.g., an aortic aneurysm or coronary calcification) that appear because the scan covers a wide area of the chest. Always follow up on these with the appropriate specialist.
Understanding your lung cancer CT scan results is closely connected to knowing how lung cancer is first detected. Our article on how lung cancer is diagnosed walks through the full diagnostic journey.
Lung-RADS Score Explained — What Your Number Means in 2026
Lung-RADS (Lung CT Screening Reporting and Data System) is the standardised scoring system developed by the American College of Radiology. Every lung cancer CT scan report includes a Lung-RADS score. It tells you — and your doctor — exactly what happens next.
Think of it like the BI-RADS system used for mammograms, but for lungs.
Full Lung-RADS v2022 Reference Table
| Score | Category | Cancer Risk | What It Means | Recommended Action |
|---|---|---|---|---|
| 0 | Incomplete | N/A | Scan unclear; prior images needed | Repeat scan in 1–3 months |
| 1 | Negative | <1% | No nodules detected | Annual LDCT in 12 months |
| 2 | Benign Appearance | <1% | Nodule present but definitely benign | Annual LDCT in 12 months |
| 3 | Probably Benign | 1–2% | Small nodule; likely harmless | Follow-up LDCT in 6 months |
| 4A | Suspicious | 5–15% | Larger or growing nodule | LDCT in 3 months or PET/CT |
| 4B | Highly Suspicious | >15% | Highly concerning nodule features | Biopsy or surgical evaluation |
| 4X | Highly Suspicious + | >15% | 3 or 4 nodule + extra danger signs (spiculation, growth, lymph nodes) | Immediate biopsy or workup |
| S modifier | Other Significant Finding | N/A | Non-cancer finding (e.g., cardiac issue, emphysema) | Specialist referral for that finding |
| C modifier | Prior Cancer History | N/A | Individual has a history of lung cancer | Enhanced monitoring protocol |
✅ What This Means For You: A Lung-RADS 3 or 4A result does not mean you have cancer. It means your doctors are being appropriately thorough. The vast majority of follow-up findings turn out to be benign. Stay calm, keep your follow-up appointment, and ask your doctor exactly what they saw.
Understanding where your scan result fits into the overall staging picture is important. Our guide to lung cancer stages explained provides the full progression framework used by oncologists.
The American Lung Association confirms that regular annual screenings remain one of the most effective tools for catching lung cancer at its most treatable stage.
What Happens After an Abnormal Lung Cancer CT Scan Result?
Your Follow-Up Pathway by Lung-RADS Score
| Lung-RADS | Immediate Next Step |
|---|---|
| 1–2 | Return for annual LDCT in 12 months |
| 3 | Repeat LDCT in 6 months |
| 4A | Repeat LDCT in 3 months OR PET/CT scan |
| 4B / 4X | Biopsy (CT-guided or bronchoscopic) or surgical evaluation |
PET/CT vs. Biopsy — What Is the Difference?
Patients frequently confuse these two. Here is the distinction:
PET/CT Scan:
- Measures metabolic activity of a nodule
- Cancer cells use more glucose → they “light up” on a PET scan
- Non-invasive; helps avoid unnecessary biopsies
- Best for nodules ≥8mm solid component (per Lung-RADS 4A guidance)
Biopsy:
- A tissue sample is extracted from the nodule
- Methods include CT-guided needle biopsy or bronchoscopy
- Provides a definitive cancer diagnosis — only a biopsy can confirm malignancy
- Also determines cancer type: NSCLC vs. SCLC — which determines the entire treatment plan
Our guide on lung cancer statistics and survival rates shows clearly why early detection through CT scan dramatically improves outcomes: Stage I five-year survival rates exceed 85%, compared to under 10% for Stage IV. You can read more about Stage I outcomes specifically in our Stage 1 lung cancer survival article.
AI-Assisted Lung Cancer CT Analysis in 2026 — A Game Changer
This is the development no competitor is covering — and it directly affects your results.
FDA-cleared artificial intelligence tools are now integrated into many major radiology centres across the USA. These systems:
- Detect nodules as small as 2–3mm that human readers may miss
- Flag sub-centimetre ground-glass opacities for closer follow-up
- Reduce inter-radiologist variability in Lung-RADS scoring
- A 2024 study published in Nature Medicine found an AI system trained on 45,064 cases achieved a sensitivity of 87.1% vs. 63.3% for standard Lung-RADS alone
What this means for you in 2026: If your imaging centre uses AI-assisted reading, your lung cancer CT scan results may be more sensitive than scans read five years ago. Ask your radiologist whether AI-assisted detection was used.
Managing Scan Anxiety — The Emotional Reality
Waiting for lung cancer CT scan results is consistently ranked among the most stressful medical experiences. This is real, valid, and common.
- Write down 3 specific questions before your results call (e.g., “What is my exact Lung-RADS score?” and “When is my next scan?”)
- Bring a family member or trusted friend to your results consultation
- Remember: 96%+ of positive LDCT scans do not indicate cancer
- Avoid interpreting the raw radiology report alone — always wait for your doctor’s explanation
If you are noticing new or worsening symptoms after your scan, document them carefully using our Symptom Checker and bring that record to your next appointment.
For patients already navigating a diagnosis, our article on early signs of lung cancer and lung cancer FDA-approved drugs and treatments 2026 offer the next layer of evidence-based guidance.
After Your Lung Cancer CT Scan — Reducing Risk and Staying Ahead
Receiving your results — whether clear or concerning — is not the end of the process. It is the beginning of informed action.
Commit to Annual Screening
Skipping even one annual lung cancer CT scan can allow a slow-growing nodule to progress from Stage I to Stage II — a shift that can halve your survival odds. Consistency is not optional; it is life-saving.
Quit Smoking — Even During Screening
Current smokers are still eligible for and benefit enormously from LDCT screening. But cessation remains the single most powerful modifiable risk factor. According to Smokefree.gov, the risk of lung cancer drops by approximately 50% within 10 years of quitting.
Most LDCT screening programmes include integrated smoking cessation counselling — ask your screening coordinator to enrol you.
Radon: The Hidden Risk Factor
After smoking, radon gas is the second-leading cause of lung cancer in the USA, responsible for approximately 21,000 deaths annually. Unlike smoking, radon exposure is invisible and odourless. The EPA recommends testing every home — particularly basements — using an inexpensive radon test kit. Our full article on radon gas and lung cancer home risk explains exactly what to do if your home tests positive.
Protect Your Cardiovascular Health
Lung cancer CT scans frequently reveal incidental coronary artery calcification — an early marker of heart disease. If your radiology report mentions this finding, monitor your cardiovascular health proactively. Use our Heart Rate Zone Calculator to optimise your exercise intensity and reduce cardiovascular risk alongside your lung cancer screening routine.
Know Your Family History
A family history of lung cancer — especially in a first-degree relative — increases your personal risk even if you are a non-smoker. Use our Genetic Risk Assessment Tool to evaluate your inherited risk and bring the results to your next preventive health appointment.
The American Cancer Society recommends that all high-risk individuals discuss a personalised screening plan with their physician — not a one-size-fits-all approach.
Frequently Asked Questions: Lung Cancer CT Scan
Q1. How long does a lung cancer CT scan take?
The scan itself takes under 2 minutes. The full appointment — including check-in and positioning — is typically 10 to 30 minutes.
Q2. Does a lung cancer CT scan hurt?
No. It is completely non-invasive and painless. No needles, no contrast dye, and no claustrophobia risk.
Q3. What does a Lung-RADS score of 3 mean?
A score of 3 means a probably benign nodule with a 1–2% cancer probability. A follow-up LDCT in 6 months is recommended — not a biopsy.
Q4. Can a CT scan tell if a lung nodule is cancerous?
No CT scan can definitively confirm cancer. It can only assess size, density, and growth. Only a biopsy provides a confirmed diagnosis.
Q5. What size lung nodule is concerning on a CT scan?
Solid nodules above 6mm typically require follow-up. Part-solid nodules above 6mm total / 4mm solid core are considered higher risk per Lung-RADS v2022 criteria.
Q6. How accurate is a lung cancer CT scan?
LDCT has a sensitivity of approximately 93–94% for detecting malignant nodules. AI-assisted reading in 2026 has pushed sensitivity above 87–94% in research settings.
Q7. What does ground-glass opacity mean on a lung CT scan?
A hazy, cloud-like area where underlying lung structures are still visible. Often benign or inflammatory, but monitored annually if persistent.
Q8. How often should I get a lung cancer CT scan?
Annually, if you meet USPSTF eligibility. More frequently (every 3–6 months) if a Lung-RADS 3 or 4A result is found.
Q9. Does insurance cover a lung cancer CT scan?
Medicare and most ACA-compliant plans cover annual LDCT screening at $0 cost-share for eligible individuals. Always verify with your insurer before scheduling.
Q10. What happens if my lung cancer CT scan result is abnormal?
Depending on your Lung-RADS score, next steps range from a 6-month follow-up scan (score 3) to biopsy or PET/CT (score 4A–4X). Your doctor will guide the specific pathway.
Q11. Is low-dose CT the same as a regular CT scan?
No. Low-dose CT (LDCT) uses up to 90% less radiation than a standard chest CT and is specifically designed for annual lung cancer screening in high-risk individuals.
Key Takeaways
- Annual lung cancer CT scans (LDCT) reduce lung cancer mortality by up to 20% in high-risk adults aged 50–80.
- Most scans are negative — and most abnormal findings are not cancer.
- Your Lung-RADS score (0–4X) determines your next steps — always ask for this number.
- AI-assisted CT analysis in 2026 is making scans more sensitive than ever before.
- Stop smoking, test your home for radon, and commit to annual screening — these three actions save lives.
Related Reading on mymedicineadvisor.com:
- How Is Lung Cancer Diagnosed?
- Early Signs of Lung Cancer
- Smoking and Lung Cancer: The Full Evidence
- Lung Cancer Stages Explained
- NSCLC vs. SCLC: What’s the Difference?
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (2005); Medical Oncology (2008); Hematology (2009) Experience: 20 years | Location: Houston, Texas Education: BS Biology, Duke University (1999); MD, Baylor College of Medicine…

Board Certifications: Diagnostic Radiology (2009); Neuroradiology (2011); Breast Imaging (2013) Experience: 16 years | Location: Rochester, Minnesota Education: BS Physics, MIT (2000); MD, Mayo Clinic Alix School of…

Board Certifications: Internal Medicine (1996); Pulmonary Disease (1999); Critical Care Medicine (1999); Sleep Medicine (2005) Experience: 29 years | Location: Sydney, Australia Education: MBBS, University of Sydney (1993);…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.