On This Page – Quick Medical Summary
How Is Lung Cancer Diagnosed? (The Short Answer)
Lung cancer is diagnosed through a three-phase process: imaging scans, tissue biopsy, and biomarker/genomic testing. No single test confirms lung cancer alone — doctors use a combination based on your symptoms, risk factors, and tumor location.
Here is the statistic that should alarm every American: according to the American Lung Association’s 2026 diagnostic campaign, only 16% of eligible Americans are getting the recommended lung cancer screening scan. Yet catching it early raises the five-year survival rate from just 9% to 65%.
If you are experiencing unexplained symptoms, track them immediately using our Symptom Checker and speak with your doctor without delay. Before diving into tests, read our comprehensive guide on what lung cancer is to understand what doctors are actually looking for.
What Triggers Lung Cancer Testing? Symptoms vs. Screening Explained
Not everyone gets tested the same way. There are three distinct pathways to a lung cancer diagnosis — and most articles online fail to explain the critical difference between them.
| Pathway | Who It’s For | First Test Ordered |
|---|---|---|
| Symptom-based | Persistent cough, coughing blood, unexplained weight loss | Chest X-ray → CT scan |
| Screening-based | Ages 50–80, 20+ pack-year smoking history, no symptoms | Low-Dose CT (LDCT) |
| Incidental finding | Abnormal spot found during an unrelated scan | Diagnostic CT + pulmonologist referral |
Who Qualifies for Lung Cancer Screening in 2026?
Per the CDC’s current LDCT screening guidelines and the American Cancer Society’s updated eligibility criteria, yearly low-dose CT screening is recommended for adults who:
- Are 50 to 80 years old
- Currently smoke, or have quit within the last 15 years
- Have a 20 pack-year smoking history (example: 1 pack per day for 20 years, or 2 packs per day for 10 years)
⚠️ The gap no competitor covers: Approximately 20% of lung cancer patients have never smoked. Non-smokers are rarely screened proactively, meaning their cancer is often caught at a later, harder-to-treat stage. If you are a non-smoker with persistent respiratory symptoms, learn about the causes of lung cancer beyond smoking — including radon gas, asbestos, air pollution, and inherited gene mutations.
If you’ve been experiencing any of the early warning signs of lung cancer, do not wait for annual screening — request a diagnostic CT scan from your physician.
At a physical exam, your doctor will specifically look for:
- Abnormal breathing sounds (wheezing, crackling)
- Clubbing or swelling of the fingertips
- Swollen lymph nodes in the neck or collarbone area
- Unexplained weight loss or facial swelling (superior vena cava syndrome)
Assess your hereditary risk factors using our Genetic Risk Assessment Tool to better understand your baseline lung cancer susceptibility.
Lung Cancer Scans Explained: CT, X-Ray, PET, MRI & Bone Scan (Compared)
Imaging is the first line of investigation in diagnosing lung cancer. These tests do not confirm cancer — they identify suspicious areas that require tissue analysis. Here is the master comparison table that no competitor publishes:
| Scan | What It Shows | Invasive? | Radiation | Duration | Best Used For |
|---|---|---|---|---|---|
| Chest X-Ray | Large masses only | No | Minimal | 10 min | First-line abnormality flag |
| Low-Dose CT (LDCT) | Nodules ≥4mm | No | Low | 5–10 min | High-risk annual screening |
| Standard CT Scan | Tumor size, lymph nodes, spread | No | Moderate | 15–20 min | Diagnostic confirmation |
| PET Scan | Metabolically active cancer cells | No (injection) | Moderate | 2–3 hrs | Spread detection, staging |
| PET/CT Combined | Most complete whole-body picture | No | Moderate | 2–3 hrs | Gold standard for staging |
| MRI | Brain and spinal cord spread | No | None | 30–60 min | CNS metastasis check |
| Bone Scan | Bone metastasis | No (injection) | Low | 3–4 hrs | Stage IV investigation |
Can a CT Scan Miss Lung Cancer?
Yes — and this is something patients urgently need to understand. Chest X-rays miss up to 25% of early lung tumors. Nodules smaller than 4mm can be difficult to identify even on CT scans.
The American Cancer Society and the American Lung Association both recommend CT over X-ray for any high-risk patient. The Mayo Clinic describes how CT combines hundreds of X-ray images into a three-dimensional view — significantly more detailed than a single-plane chest X-ray.
2026 Update: AI-Assisted CT Scanning
This is the advancement that zero competitors are writing about. FDA-cleared AI tools are now helping radiologists detect lung nodules that human eyes miss — particularly in the 4–6mm range. Research published in 2025 shows that AI-assisted CT reading reduces missed early-stage diagnoses by up to 17%.
What This Means For You: If your doctor ordered only a chest X-ray and dismissed your concerns, you have the right to ask for a CT scan. CT is significantly more accurate, especially for lung cancer diagnosed before symptoms even appear.
If you’ve already received a CT result, our guide on CT scan abnormalities and what to do next will help you understand your report and your next steps.
Lung Cancer Biopsy Types: Which One Will You Need?
When James, a 63-year-old retired utility worker from Ohio, was told his CT scan showed a 2.3cm nodule in his right upper lobe, his pulmonologist recommended an EBUS-guided biopsy. He had never heard the term. Within three weeks, he had a confirmed non-small cell lung cancer diagnosis — and a personalized treatment plan already in motion.
A biopsy is the only definitive way to confirm lung cancer. It involves removing a small sample of tissue or cells from the lung and examining it under a microscope. The type of biopsy recommended depends on the tumor’s location, size, and how easily it can be accessed.
| Biopsy Type | How It’s Done | Best For | Recovery | Accuracy |
|---|---|---|---|---|
| CT-Guided Needle (FNA) | Needle through chest wall, CT-guided | Peripheral tumors | Same day | ~90% |
| Core Needle Biopsy (CNB) | Larger sampling needle | More tissue needed for biomarkers | Same day | ~92% |
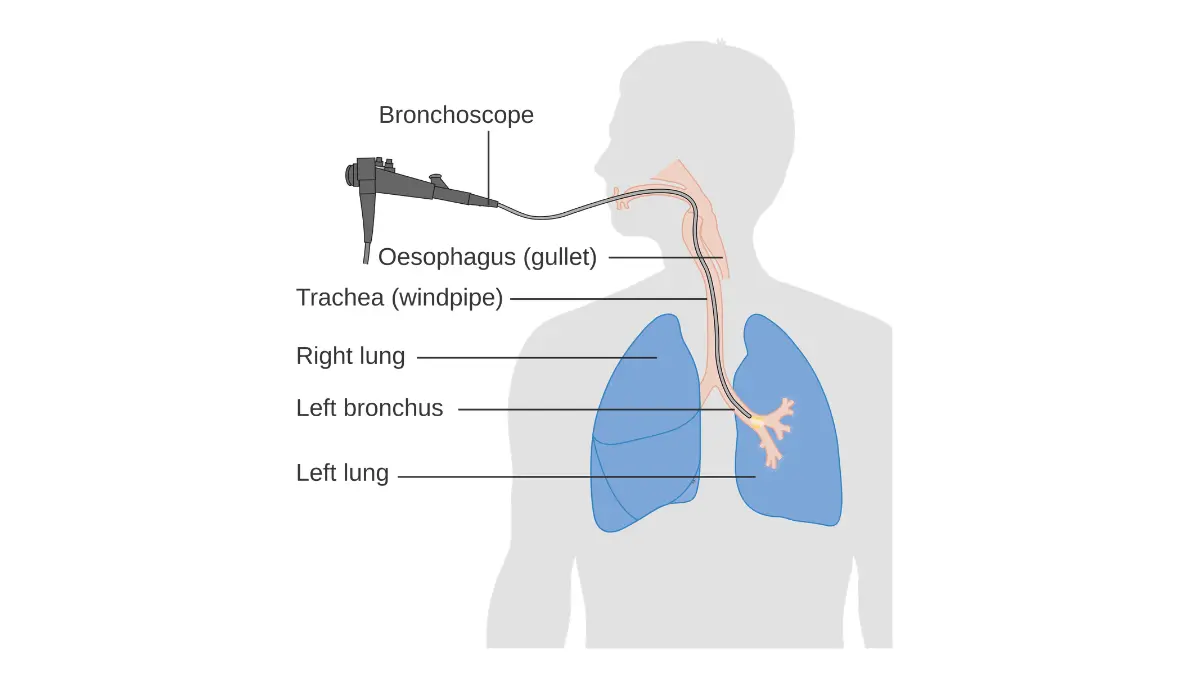
| Bronchoscopy | Flexible tube via nose/mouth into airways | Central airway tumors | 1–2 hrs | ~70–88% |
| EBUS (Endobronchial Ultrasound) | Bronchoscopy + real-time ultrasound | Lymph node sampling | Same day | ~89–93% |
| EUS (Endoscopic Ultrasound) | Flexible tube through esophagus | Mediastinal lymph nodes | Same day | ~85–90% |
| Robotic Bronchoscopy | Robot-navigated scope to deep nodules | Small, peripheral, deep-access nodules | Same day | ~85–96% |
| VATS / Thoracoscopy | Small chest incision, surgical camera | Pleural spread, outer lung tumors | 1–3 days | ~98% |
| Thoracentesis | Needle drains pleural fluid | Fluid accumulation around lungs | Same day | Variable |
According to Johns Hopkins Medicine, biopsies are the most critical confirmatory tool in lung cancer diagnosis — and selecting the right type is essential to getting sufficient tissue for both diagnosis and downstream biomarker analysis.
Robotic Bronchoscopy: The 2025/2026 Diagnostic Game-Changer
Robotic bronchoscopy systems — including Intuitive’s Ion platform and the Monarch system — allow surgeons to navigate to small, deep, peripheral nodules that traditional bronchoscopes cannot safely reach. As annual LDCT screening increases, more tiny, hard-to-access nodules are being found. These robotic systems have demonstrated diagnostic yields up to 96% in published 2025 clinical data, compared to roughly 70% with conventional bronchoscopy.
Ask your medical center: “Do you offer robotic bronchoscopy for peripheral nodule biopsy?” Not all facilities have it — but NCI-designated cancer centers and major academic hospitals increasingly do.
Is a Lung Biopsy Painful?
Most patients report mild to moderate discomfort, not severe pain. CT-guided needle biopsies use local anesthesia. Bronchoscopy uses IV sedation. The most cited complication is pneumothorax — a small air leak around the lung — occurring in 2–5% of needle biopsies. It is almost always manageable without surgery.
Once your biopsy is complete, read our expert guide on biopsy results timelines and how to decode your pathology report. To understand the critical difference between the two main cancer types confirmed at biopsy, our full breakdown of NSCLC vs SCLC is essential reading.
Liquid Biopsy & Biomarker Testing: The Future of Lung Cancer Diagnosis Is Already Here
This is the section that no competitor’s diagnosis article properly covers — and it may be the most important for your treatment outcome.
After tissue is confirmed as lung cancer, doctors must determine its molecular identity. This is done through biomarker testing — also called genomic testing or molecular profiling — and it directly determines which treatments will work best for you.
What Is a Liquid Biopsy for Lung Cancer?
A liquid biopsy is a simple blood draw that detects circulating tumor DNA (ctDNA) shed by cancer cells into the bloodstream. It cannot replace a tissue biopsy for initial diagnosis, but it is increasingly used when:
- Tumor tissue is unavailable or insufficient in volume
- Monitoring treatment response in real time
- Detecting cancer recurrence before imaging shows it
- Identifying resistance mutations after targeted treatment stops working
| Feature | Tissue Biopsy | Liquid Biopsy |
|---|---|---|
| Sample | Lung tissue | Blood draw |
| Invasiveness | Moderate to High | None |
| Turnaround Time | 7–14 days | 5–10 days |
| Confirms Cancer? | Yes (gold standard) | No — guides treatment decisions |
| Best For | Initial diagnosis | Monitoring, recurrence detection, insufficient tissue |
Biomarkers Your Oncologist Should Test For
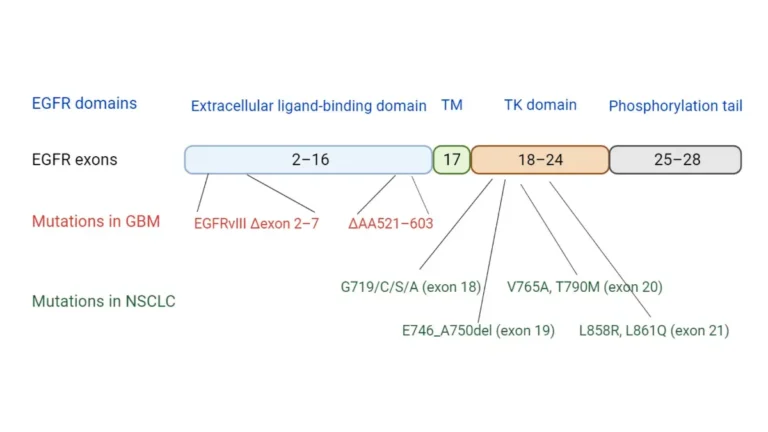
According to the American Lung Association’s biomarker testing guidelines and the National Cancer Institute, all NSCLC patients should receive comprehensive next-generation sequencing (NGS) testing for:
| Biomarker | Why It Matters |
|---|---|
| EGFR | Targeted therapy (osimertinib) available — most common mutation in non-smokers |
| ALK | ALK inhibitors (alectinib, brigatinib) significantly extend survival |
| ROS1 | Crizotinib- and entrectinib-sensitive — highly treatable |
| KRAS G12C | FDA-approved sotorasib (Lumakras) and adagrasib available |
| PD-L1 | Determines eligibility for immunotherapy (pembrolizumab) |
| MET exon 14 | Tepotinib and capmatinib are approved targeted options |
⚠️ The 2026 Statistic That Should Outrage You: The American Lung Association reports that 23% of lung cancer patients receive chemotherapy or radiation before completing full biomarker testing — potentially missing a more effective, less toxic targeted therapy.
What This Means For You: Before starting any treatment, insist on comprehensive NGS biomarker testing. It could mean the difference between chemotherapy and a once-daily oral targeted therapy with far fewer side effects.
Explore all current FDA-approved lung cancer drugs and treatment options for 2026 to understand what your biomarker results could unlock.
From First Symptom to Confirmed Diagnosis: A Real Patient Timeline
“How long does a lung cancer diagnosis take?” is one of the most searched and least-answered questions in this space. Here is the honest, step-by-step timeline — exclusive to this guide:
| Phase | What Happens | Typical Timeframe |
|---|---|---|
| Week 1 | GP visit, symptom review, chest X-ray ordered | Days 1–5 |
| Week 1–2 | CT scan performed if X-ray shows abnormality | Days 5–10 |
| Week 2–3 | Referral to pulmonologist or thoracic oncologist | Days 10–21 |
| Week 3–4 | Biopsy scheduled and completed | Days 14–28 |
| Week 4–6 | Biopsy pathology report + biomarker/NGS testing | Days 21–45 |
| Week 5–7 | Multidisciplinary tumor board case review | Days 35–50 |
| Week 6–8 | Staging confirmed, personalized treatment plan begins | Days 42–56 |
For a detailed explanation of what each stage means for your prognosis and treatment choices, read our complete guide on lung cancer stages explained.
5 Questions to Ask Your Doctor After a Lung Cancer Diagnosis
The National Cancer Institute’s treatment guidance consistently shows that patients who actively engage their care team achieve better outcomes. Ask these questions at every appointment:
- What exact type and stage is my lung cancer? NSCLC versus SCLC determines everything about your treatment path.
- Has full NGS biomarker testing been ordered? If not — demand it before any treatment begins.
- What biopsy method are you recommending, and why is it the best option for my case?
- Am I eligible for any clinical trials at this stage?
- Would you recommend I seek a second opinion at an NCI-designated comprehensive cancer center?
Getting a Second Opinion
You always have the right to a second opinion — and for lung cancer, it is strongly encouraged. Major centers including MD Anderson, Memorial Sloan Kettering, and Mayo Clinic offer rapid second opinion consultations, often within days of your initial diagnosis.
If you are still identifying your symptoms, review our detailed resource on lung cancer signs and early warnings to help you give your physician a complete picture.
Frequently Asked Questions About Lung Cancer Diagnosis
Q1. What is the first test done to diagnose lung cancer?
A chest X-ray is typically the first test ordered. If it shows anything abnormal, a CT scan is the immediate next step — and is significantly more accurate for detecting early-stage tumors.
Q2. Can a blood test detect lung cancer?
No standard blood test confirms lung cancer. A liquid biopsy can detect circulating tumor DNA in the blood, but it is used to guide treatment decisions — not to make an initial diagnosis.
Q3. Is a CT scan enough to diagnose lung cancer?
No. A CT scan identifies suspicious areas. A biopsy — removing actual tissue — is required to confirm cancer at the cellular level. CT alone is never sufficient for a definitive lung cancer diagnosis.
Q4. How long does it take to get lung cancer diagnosis results?
From your first GP visit to a confirmed diagnosis typically takes 6 to 8 weeks. Biopsy pathology takes 7–14 days; comprehensive biomarker testing adds another 5–14 days on top of that.
Q5. Is a lung biopsy painful?
Most patients describe mild to moderate discomfort — not severe pain. Local anesthesia is standard for needle biopsies. IV sedation is used for bronchoscopy. Pneumothorax, the most common complication, occurs in 2–5% of cases and is almost always treated without surgery.
Q6. Can lung cancer be diagnosed without a biopsy?
Rarely, and only in exceptional clinical situations such as highly advanced, widely metastatic disease. Tissue biopsy remains the gold standard for diagnosis in virtually all cases.
Q7. What does a liquid biopsy test for in lung cancer?
It analyzes circulating tumor DNA (ctDNA) in the bloodstream to identify actionable biomarkers, monitor treatment response in real time, and detect early signs of cancer recurrence.
Q8. Who should get low-dose CT lung cancer screening in 2026?
Adults aged 50–80 who currently smoke or quit within the last 15 years, and have a 20 pack-year smoking history. Check the CDC’s current eligibility guidelines for updated criteria.
Q9. Can lung cancer be missed on a CT scan?
Yes — particularly nodules smaller than 4mm. AI-assisted CT reading tools are now reducing missed diagnoses. Always follow up abnormal findings promptly with a pulmonologist or thoracic specialist.
Q10. What happens after lung cancer is diagnosed?
Staging is confirmed via PET/CT, comprehensive biomarker testing is completed, and a multidisciplinary tumor board — including oncologists, radiologists, and surgeons — reviews your case to create a personalized treatment plan.
Q11. Is lung cancer diagnosis different for non-smokers?
Yes. Non-smokers are rarely screened proactively, so their cancer is more often caught at an advanced stage. Non-smokers with NSCLC are also significantly more likely to carry EGFR or ALK mutations — making comprehensive biomarker testing especially critical for this group.
Disclaimer: This article is for educational and informational purposes only. It does not constitute medical advice, diagnosis, or treatment. Always consult a qualified and licensed healthcare provider regarding any medical symptoms, test results, or treatment decisions. If you are experiencing a medical emergency, call 911 immediately.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.