On This Page – Quick Medical Summary
Targeted therapy for lung cancer is one of the most transformative medical breakthroughs of the 21st century. Unlike chemotherapy — which attacks all rapidly dividing cells — targeted therapy works like a guided missile, identifying and destroying only cancer cells that carry specific genetic mutations. In 2026, nine druggable mutations in non-small cell lung cancer (NSCLC) now have FDA-approved treatments, turning what was once a near-certain death sentence into a manageable, long-term condition for many patients.
David, a 47-year-old non-smoker from Houston, was diagnosed with Stage IV NSCLC in 2023. His oncologist ordered comprehensive biomarker testing and discovered an EGFR exon 19 deletion. Within three weeks of starting targeted therapy with osimertinib, his tumor had shrunk by 40%. Two and a half years later, he still coaches his daughter’s soccer team. David’s story is now the new normal in precision oncology.
What Is Targeted Therapy for Lung Cancer?
Targeted therapy is a precision medicine approach that uses drugs to block specific proteins, genes, or receptors that drive cancer cell survival and growth. It is not chemotherapy, and it works very differently inside the body.
Before starting any treatment, your oncologist must test your tumor for genetic mutations that make it vulnerable to specific targeted drugs. Understanding how lung cancer is diagnosed — including biopsy and molecular testing — is the essential first step every patient should take.
How Targeted Therapy Differs from Chemotherapy
| Feature | Targeted Therapy | Chemotherapy | Immunotherapy |
|---|---|---|---|
| Mechanism | Blocks specific cancer gene/protein | Kills all fast-dividing cells | Activates immune system vs. cancer |
| Who benefits | Patients with specific mutations | Broad NSCLC population | Patients with high PD-L1 expression |
| Administration | Oral pill (mostly) | IV infusion | IV infusion |
| Common side effects | Skin rash, diarrhea, fatigue | Nausea, hair loss, infection risk | Fatigue, immune-related reactions |
Key Takeaway: Targeted therapy only works if your tumor carries a specific, testable genetic mutation. Without comprehensive biomarker testing, there is no way to know whether these drugs will help.
The 3 Main Types of Targeted Drugs in Lung Cancer
- Tyrosine kinase inhibitors (TKIs): Oral pills that block signaling proteins driving cancer growth — e.g., osimertinib (EGFR), alectinib (ALK)
- Bispecific monoclonal antibodies: IV or subcutaneous drugs that simultaneously target two proteins — e.g., amivantamab targeting EGFR + MET
- Antibody-drug conjugates (ADCs): Lab-made antibodies that deliver chemotherapy directly to cancer cells — e.g., trastuzumab deruxtecan for HER2-mutant NSCLC
Reviewing your full lung cancer treatment options alongside targeted therapy helps ensure you and your care team are evaluating every available pathway. If you have a family history of lung cancer, our Genetic Risk Assessment Tool can help clarify your inherited risk profile before your next oncology appointment.
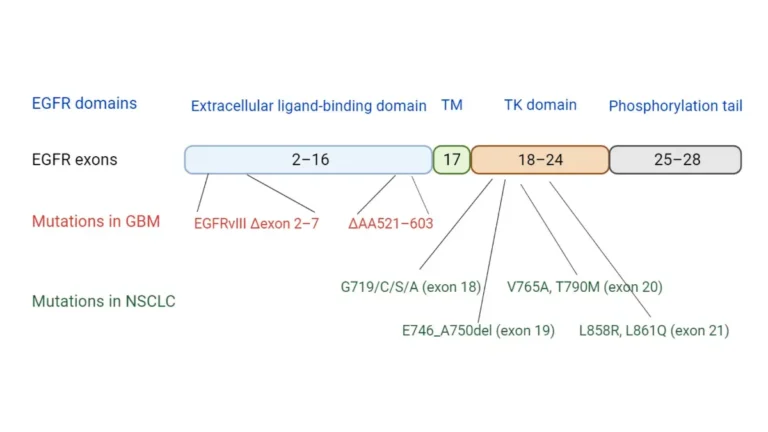
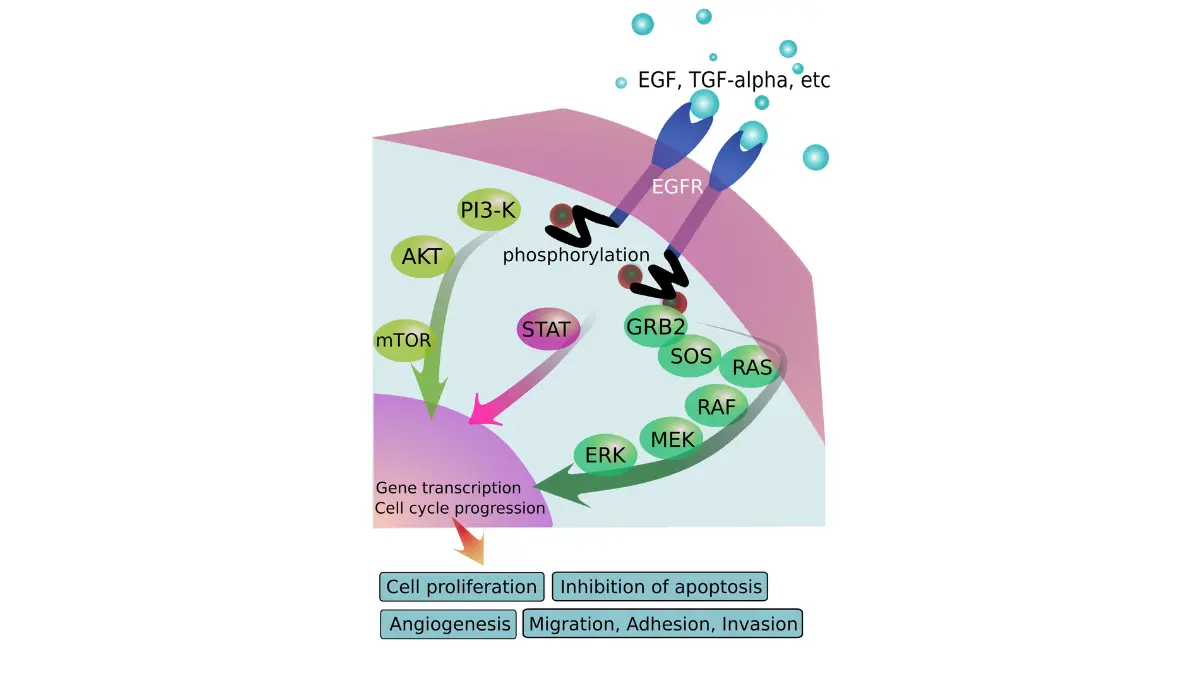
EGFR Mutations — The Most Common Targetable Driver
EGFR (epidermal growth factor receptor) mutations are the most prevalent actionable genomic driver in NSCLC. According to the National Cancer Institute’s lung cancer research page, EGFR mutations occur in 10–15% of NSCLC patients in the United States and up to 40% of patients in some Asian countries — a critical ethnic variation that directly affects screening decisions.
Who Gets EGFR-Mutant Lung Cancer?
EGFR mutations most commonly occur in:
- Non-smokers and light smokers
- Women more frequently than men
- Patients of East Asian descent (up to 40% prevalence)
- Adenocarcinoma subtype of NSCLC
The two most actionable EGFR mutations are exon 19 deletions and the L858R point mutation (exon 21). A third mutation — T790M — typically develops later as a resistance mechanism against first- and second-generation EGFR inhibitors.
FDA-Approved EGFR Inhibitors — 2026 Comparison Table
| Drug (Brand Name) | Generation | Primary Use | Key 2026 Update |
|---|---|---|---|
| Osimertinib (Tagrisso) | 3rd gen | 1st-line + adjuvant Stage IB–IIIA | LAURA trial: 84% reduced progression risk in Stage III unresectable |
| Amivantamab (Rybrevant Faspro) | Bispecific (EGFR+MET) | EGFR exon 20 insertions, post-chemo | NEW: Subcutaneous every-4-weeks dosing FDA-approved February 2026 |
| Erlotinib (Tarceva) | 1st gen | Metastatic NSCLC | Largely replaced by 3rd-gen agents in standard practice |
| Gefitinib (Iressa) | 1st gen | Metastatic NSCLC | Less used since FLAURA trial data established osimertinib superiority |
| Dacomitinib (Vizimpro) | 2nd gen | Selected 1st-line EGFR profiles | Used in specific patient subpopulations |
The landmark LAURA trial demonstrated that osimertinib reduces the risk of cancer progression or death by 84% in patients with Stage III unresectable EGFR-mutated NSCLC after chemoradiotherapy — a result the American Cancer Society calls a practice-changing milestone.
When EGFR Therapy Stops Working — Understanding Resistance
Most patients on EGFR targeted therapy eventually develop resistance — typically within 12–18 months on earlier-generation drugs, and often considerably longer on osimertinib. The T790M mutation is the most common acquired resistance mechanism. Osimertinib was specifically engineered to overcome T790M, which is why it is now the globally preferred first-line EGFR inhibitor.
Liquid biopsy — a blood test detecting circulating tumor DNA — can identify resistance mutations early, before a tumor is large enough to appear on imaging. Understanding what happens during a lung biopsy for cancer — including both tissue and liquid biopsy options — helps patients ask the right questions at each oncology visit.
What This Means For You: Ask your oncologist about liquid biopsy testing if you have been on EGFR-targeted therapy for more than 12 months. Early resistance detection opens new treatment options before symptoms progress.
ALK-Positive Lung Cancer — Targeted Therapy’s Greatest Success Story
ALK (anaplastic lymphoma kinase) fusions occur in 3–7% of NSCLC patients, according to NCI’s comprehensive NSCLC treatment guidelines. Despite their lower frequency compared to EGFR mutations, ALK-positive lung cancers have seen some of the most dramatic survival improvements of any cancer subtype in medical history.
What ALK-Positive Lung Cancer Means
ALK-positive NSCLC typically affects:
- Younger patients, often under 50 at diagnosis
- Never-smokers or very light smokers
- Adenocarcinoma subtype almost exclusively
- Patients with a higher baseline risk of brain metastases
The EML4-ALK gene fusion creates an abnormal protein that drives continuous, uncontrolled cancer cell growth. Targeted ALK inhibitors block this protein with extraordinary precision.
Before ALK inhibitors existed, patients with advanced ALK+ NSCLC survived a median of under two years. In 2026, patients on lorlatinib in clinical trials are reaching five-year survival milestones routinely.
ALK Inhibitors — Generation-by-Generation Progress
| Drug (Brand) | Generation | CNS Coverage | Key Trial/Approval |
|---|---|---|---|
| Crizotinib (Xalkori) | 1st | Limited | PROFILE 1014 |
| Ceritinib (Zykadia) | 2nd | Moderate | ASCEND-4 |
| Alectinib (Alecensa) | 2nd/3rd | Strong | ALEX trial; adjuvant FDA-approved 2024 (ALINA trial) |
| Brigatinib (Alunbrig) | 3rd | Strong | ALTA-1L |
| Lorlatinib (Lorbrena) | 3rd | Strongest blood-brain barrier penetration | CROWN trial — preferred 1st-line for brain metastases |
Key Takeaway: Lorlatinib is the preferred first-line choice for ALK+ NSCLC patients with brain metastases because of its superior ability to cross the blood-brain barrier. Alectinib’s 2024 FDA adjuvant approval for early-stage ALK+ NSCLC following surgery represents a paradigm shift that most consumer health sites have not yet adequately communicated.
Track any new or worsening neurological symptoms between oncology appointments using our Symptom Checker. Always report sudden headaches, vision disturbances, or coordination changes to your care team immediately.
What This Means For You: If newly diagnosed with ALK+ NSCLC, request a baseline brain MRI and specifically ask your oncologist to compare lorlatinib versus alectinib based on your CNS involvement at diagnosis.
Beyond EGFR and ALK — 7 More Lung Cancer Mutations Now Treatable
This is the section that competitors have failed patients on most critically. Modern next-generation sequencing (NGS) can identify nine or more druggable mutations in NSCLC tumors. If your oncologist has only tested for EGFR and ALK — and nothing else — ask immediately for a comprehensive biomarker panel. You may be sitting on a targetable mutation that changes your entire treatment plan.
A 2025 peer-reviewed review in Current Oncology, available via PubMed Central, confirms that comprehensive molecular testing across all actionable genomic alterations is now the standard of care for NSCLC.
The 2026 Complete Targeted Mutation Map for NSCLC
| Mutation | Frequency in NSCLC | FDA-Approved Drug(s) | Critical 2026 Notes |
|---|---|---|---|
| EGFR | 10–40% | Osimertinib, amivantamab, erlotinib | Most common driver; subcutaneous amivantamab every-4-weeks approved Feb 2026 |
| ALK | 3–7% | Lorlatinib, alectinib, crizotinib | Adjuvant alectinib approved 2024 (ALINA trial) |
| KRAS G12C | ~12–13% | Sotorasib (Lumakras), adagrasib (Krazati) | First-ever druggable KRAS inhibitors — historic landmark |
| ROS1 | 1–2% | Entrectinib (Rozlytrek), repotrectinib (Augtyro) | Repotrectinib FDA-approved late 2023 as 1st and 2nd-line option |
| MET exon 14 | 3–4% | Capmatinib (Tabrecta), tepotinib (Tepmetko) | Common in older patients; co-occurring mutations frequent |
| RET fusion | 1–2% | Selpercatinib (Retevmo), pralsetinib (Gavreto) | Highly selective — minimal off-target effects |
| BRAF V600E | 1–3% | Dabrafenib + trametinib (combination) | Same drugs approved for melanoma now work in NSCLC |
| HER2 (ERBB2) | 2–4% | Trastuzumab deruxtecan (Enhertu) | ADC approach; major breakthrough 2023–2025 |
| NTRK fusion | <1% | Larotrectinib (Vitrakvi), entrectinib | “Tumor-agnostic” FDA approval — works across all solid tumor types |
Key Takeaway: KRAS G12C was considered scientifically “undruggable” for over 40 years. Two FDA-approved inhibitors now exist — and KRAS G12C is the third most common mutation in NSCLC at 12–13%.
If you need help identifying a targeted therapy pill by its appearance, our Pill Identifier tool provides a reliable visual reference. For a complete breakdown of FDA-approved lung cancer drugs in 2026, including dosing schedules and recent approvals, read our dedicated companion article.
What This Means For You: Demand comprehensive NGS panel testing — not a two-gene EGFR/ALK test alone. One missing mutation result could mean missing an approved, effective targeted therapy entirely.
How to Access Targeted Therapy — Testing, Cost & Your Next Steps
Knowing a targeted therapy exists is only part of the equation. Accessing it requires understanding biomarker testing, navigating insurance prior authorizations, and knowing your financial assistance options.
Step-by-Step: How Biomarker Testing Works
- Diagnosis confirmed → Request comprehensive NGS testing of tumor tissue, liquid biopsy, or both simultaneously
- Tissue or blood sample collected → Sent to a molecular diagnostics lab (Foundation Medicine, Guardant Health, Tempus)
- Results returned in 7–21 days → Full genomic mutation panel report generated
- Oncologist interprets results → Matches identified mutations to FDA-approved targeted drugs or open clinical trials
- Treatment initiated → Oral TKI daily pill or IV/subcutaneous infusion on defined dosing schedule
Understanding your lung cancer stage is equally important, as staging affects which targeted therapy options and clinical trials you may qualify for.
How Much Does Targeted Therapy Cost in 2026?
Targeted therapy is highly effective — and among the most expensive treatment categories in all of oncology.
- Cost range: $50–$750 per pill, taken daily
- Osimertinib (Tagrisso): Total treatment course estimated at $556,720 (WebMD, March 2026)
- Insurance coverage: Most commercial plans and Medicare Part D cover FDA-approved TKIs with prior authorization
- Patient assistance programs include:
- AstraZeneca’s AZ&Me Program (osimertinib / Tagrisso)
- Genentech Access Solutions (alectinib, entrectinib)
- Pfizer’s Patient Assistance Program (lorlatinib, crizotinib)
Never stop or delay targeted therapy due to cost without first speaking with your oncology team’s dedicated social worker or patient financial navigator. Most patients never learn about assistance programs that could eliminate out-of-pocket costs entirely.
Clinical Trials for Targeted Therapy in 2026
For patients with rare mutations or acquired resistance, clinical trials are often the best available option — not a last resort. Search open studies at ClinicalTrials.gov using your specific mutation type as the search filter. The NCI’s landmark ALCHEMIST lung cancer trials specifically test targeted adjuvant therapies in early-stage NSCLC — a resource your oncologist may not proactively mention. The American Lung Association’s lung cancer treatment resources also include clinical trial navigation services available at no cost.
Side Effects, Quality of Life & Living on Targeted Therapy in 2026
The most common question patients ask after a targeted therapy recommendation is: “What will my daily life actually feel like?” For the majority of patients, the answer is significantly better than traditional intravenous chemotherapy.
Common Side Effects by Drug Class — Quick Reference
| Drug Class | Common Side Effects | Serious (Rare) Side Effects |
|---|---|---|
| EGFR TKIs (osimertinib) | Skin rash, diarrhea, dry skin, oral sores | Interstitial lung disease (ILD), cardiac QT prolongation |
| ALK inhibitors (alectinib, lorlatinib) | Vision changes, nausea, edema, weight gain | ILD/pneumonitis, bradycardia |
| KRAS inhibitors (sotorasib, adagrasib) | Diarrhea, nausea, fatigue, joint pain | Hepatotoxicity, pneumonitis |
| Bispecific antibodies (amivantamab) | Skin/nail changes, fatigue, infusion reactions | Cardiac events, severe rashes, ILD |
Most EGFR TKI side effects are manageable and do not require stopping treatment. Always report new breathing difficulty, skin rashes that spread, or vision changes to your oncologist without delay — some rare side effects require prompt dose modification to prevent serious complications.
Quality of Life — What Clinical Trials and Patients Report
Clinical trial data consistently shows better day-to-day functioning on oral TKIs compared to IV chemotherapy schedules. In the ALEX trial, patients receiving alectinib reported significantly higher quality-of-life scores than those on crizotinib, with fewer hospitalizations and lower fatigue burden.
Lifestyle factors meaningfully affect how well patients tolerate targeted therapy. Sleep quality directly influences immune function and treatment tolerance — use our Sleep Calculator to determine your optimal nightly sleep window based on your schedule. Hydration is equally critical, particularly when managing diarrhea-related side effects common to KRAS and EGFR inhibitors; our Water Intake Calculator generates personalized daily fluid targets.
For comprehensive, ongoing patient support, the American Cancer Society’s targeted drug therapy guide for NSCLC and ASCO’s cancer.net patient resources for NSCLC provide detailed side effect management guides and caregiver toolkits.
The bottom line: Targeted therapy has fundamentally redefined lung cancer from an acute emergency into a long-term, manageable condition for patients with qualifying mutations. In 2026, more mutations are druggable than at any prior point in oncology history — and the FDA pipeline includes even more approvals on the horizon. For patients already in treatment, understanding chemotherapy for lung cancer remains relevant, since some patients use targeted therapy and chemotherapy sequentially or in combination at different disease stages.
If you have been diagnosed with NSCLC, comprehensive biomarker testing is not optional — it is the most important step you can take toward the most effective, personalized treatment available today.
Frequently Asked Questions: Targeted Therapy for Lung Cancer
1. What is targeted therapy for lung cancer?
Targeted therapy uses drugs that block specific proteins or gene mutations driving cancer cell growth in NSCLC. It works only in patients whose tumors carry specific, testable genetic mutations — unlike chemotherapy, which works more broadly.
2. How do I know if I qualify for targeted therapy?
You qualify if comprehensive biomarker testing (NGS panel) identifies a druggable mutation in your tumor. Every NSCLC patient should receive this testing at diagnosis, before any treatment begins.
3. What is an EGFR mutation in lung cancer?
An EGFR mutation is a genetic change in the epidermal growth factor receptor gene that causes uncontrolled cancer cell growth. EGFR mutations occur in 10–40% of NSCLC patients and are the most common actionable genomic target in lung cancer.
4. Is targeted therapy better than chemotherapy for lung cancer?
For patients with qualifying mutations, yes — clinical trials consistently show higher tumor response rates, longer progression-free survival, and superior quality of life compared to standard chemotherapy.
5. Can targeted therapy cure lung cancer?
Targeted therapy can control advanced Stage IV lung cancer for extended periods but does not cure it. For early-stage patients (Stages IB–IIIA), adjuvant osimertinib and alectinib have significantly reduced recurrence rates following surgery.
6. How long does targeted therapy work before resistance develops?
This varies by drug and mutation. Osimertinib typically controls EGFR-mutant NSCLC for a median of 18–38+ months. ALK inhibitors like lorlatinib have demonstrated even longer control in clinical trial data.
7. What is a liquid biopsy and do I need one?
A liquid biopsy is a blood test that detects circulating tumor DNA without requiring a new tissue biopsy. It is particularly valuable for monitoring resistance mutations while you are actively on targeted therapy.
8. What does ALK-positive lung cancer mean?
ALK-positive NSCLC means your cancer carries a rearrangement in the ALK gene that creates an abnormal protein driving tumor growth. Multiple generations of targeted ALK inhibitors now exist, with lorlatinib offering the strongest response rates and brain metastasis coverage in 2026.
9. What targeted therapy is available for KRAS G12C mutations?
Sotorasib (Lumakras) and adagrasib (Krazati) are both FDA-approved for KRAS G12C-mutant NSCLC — a historic development since KRAS was considered scientifically undruggable for over four decades.
10. Does targeted therapy work for lung cancer that spread to the brain?
Yes — particularly third-generation ALK inhibitors like lorlatinib and the EGFR inhibitor osimertinib, both of which cross the blood-brain barrier effectively. Brain metastases are especially common in ALK+ NSCLC, making drug selection at diagnosis critically important.
11. How much does targeted therapy for lung cancer cost in 2026?
Costs range from $50–$750 per pill per day. Osimertinib’s estimated total treatment cost exceeds $500,000. Most insurance plans cover FDA-approved TKIs with prior authorization. Ask your oncology team about manufacturer patient assistance programs — many patients qualify for full or partial cost coverage.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.