On This Page – Quick Medical Summary
When David, a 61-year-old former firefighter from Chicago, heard the words “non-small cell lung cancer, Stage IIIA,” he assumed there was one treatment: chemotherapy and then hope for the best.
His oncologist corrected him immediately. There were seven treatment pathways available — and two of them had only been FDA-approved in the past eight months.
That gap between what patients assume and what science actually offers is costing lives. This guide closes that gap entirely.
In 2026, lung cancer treatment options include surgery, chemotherapy, radiation therapy, targeted therapy, immunotherapy, antibody-drug conjugates (ADCs), and clinical trials. The right option — or combination — depends entirely on your cancer type, stage, and molecular profile. Here is everything you need to know.
Why Your Lung Cancer Type Determines Everything
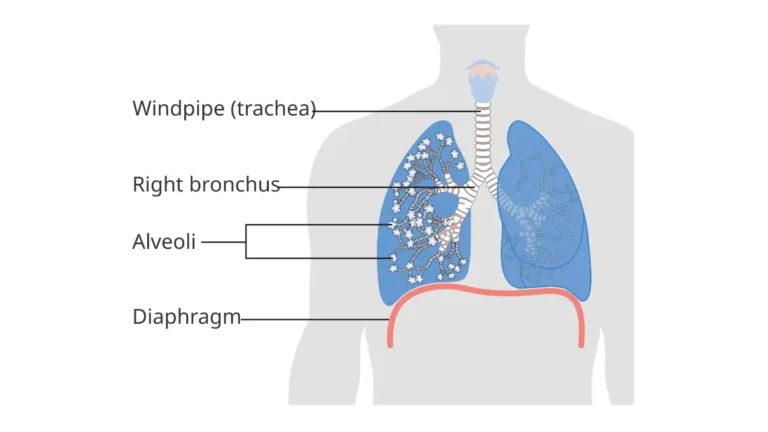
Before any lung cancer treatment plan is created, your oncologist must identify which type of lung cancer you have. This single factor drives nearly every decision that follows. If you are still in the diagnostic phase, our detailed guide on how lung cancer is diagnosed walks through every test step-by-step.
NSCLC vs. SCLC — The Critical Divide
There are two primary categories of lung cancer, and they are treated very differently.
| Feature | Non-Small Cell (NSCLC) | Small Cell (SCLC) |
|---|---|---|
| Frequency | ~85% of all cases | ~15% of all cases |
| Growth Rate | Slower | Extremely fast |
| Surgery option? | Yes (early stages) | Rarely |
| Biomarker testing needed? | Always — mandatory | Less common |
| Responds to immunotherapy? | Yes (PD-L1 dependent) | Yes (limited options) |
| 5-year survival (Stage I) | 68–92% | 20–30% |
| Key 2026 drug | Zongertinib (HER2+) | Tarlatamab (recurrent) |
NSCLC includes adenocarcinoma, squamous cell carcinoma, and large cell carcinoma. For a deeper breakdown of the differences, read our full NSCLC vs SCLC comparison guide.
The Step You Cannot Skip: Biomarker Testing
This is the most important pre-treatment step most patients don’t know to demand.
Before any lung cancer treatment begins, complete molecular profiling of your tumor must be done. Oncologists test for mutations in these genes:
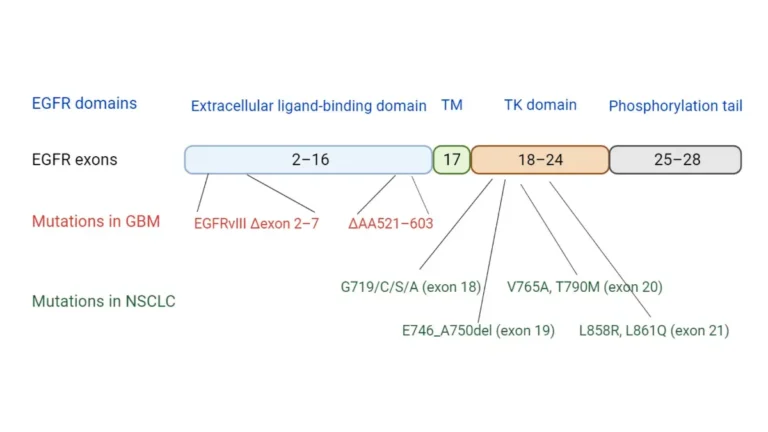
- EGFR (most common — found in ~15% of NSCLC in the US)
- ALK rearrangements (~5%)
- KRAS G12C (~13%)
- HER2 mutations (~3%)
- ROS1, MET, BRAF, RET, NTRK (less common but highly targetable)
- PD-L1 expression (determines immunotherapy eligibility)
If your oncologist hasn’t ordered comprehensive biomarker testing, ask for it immediately. You can also use our Genetic Risk Assessment Tool to understand your hereditary risk profile. The NCI’s patient guide on NSCLC treatment confirms that all newly diagnosed NSCLC patients should undergo molecular testing as standard of care.
The 7 Core Lung Cancer Treatment Options — Explained Clearly
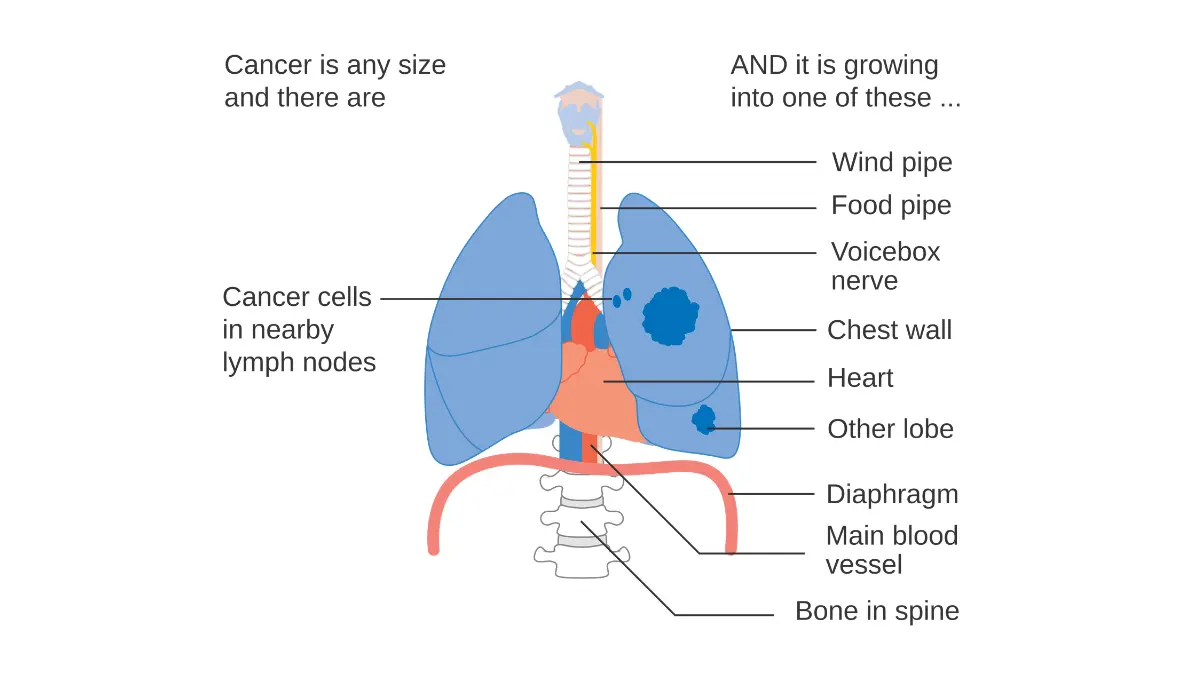
1. Surgery — The Gold Standard for Early-Stage Lung Cancer
Surgery offers the highest chance of cure when lung cancer is caught early (Stage I–II NSCLC). The goal is complete removal of the tumor with clear margins.
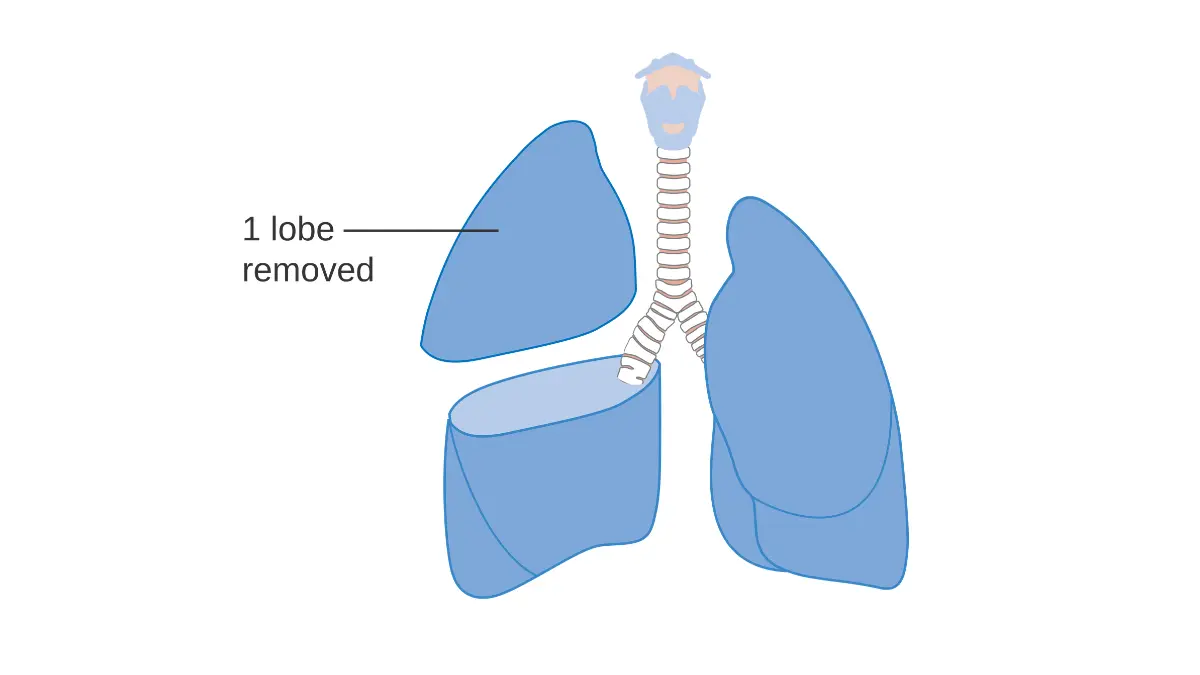
Adapted from Wikimedia Commons Diagram_showing_the_removal_of_one_lobe_of_the_lung_(lobectomy)_CRUK_366.svg, licensed under CC BY-SA 4.0.
Types of lung cancer surgery:
- Wedge resection — Removes tumor plus a small surrounding margin. Used for very small tumors or patients with limited lung reserve.
- Lobectomy — Removes the entire lobe containing the tumor. Considered the standard of care for most operable cases.
- Sleeve lobectomy — Removes the affected lobe plus part of the bronchus. Preferred over pneumonectomy when feasible.
- Pneumonectomy — Full removal of one lung. Reserved for centrally located tumors.
- VATS / Robotic-assisted surgery — Minimally invasive approach now standard at major centers including MD Anderson, reducing recovery time significantly.
Who qualifies: Patients with Stage I–II NSCLC in adequate general health with sufficient lung function.
Before surgery, many patients undergo a lung biopsy for cancer to confirm diagnosis and subtype.
2. Radiation Therapy — Precision Energy Against Tumors
Radiation therapy uses high-energy beams to destroy cancer cells. In 2026, it is far more precise than patients expect.
Key types:
- Stereotactic Body Radiation Therapy (SBRT/SABR) — Delivers high-dose radiation in 3–5 sessions. For inoperable Stage I patients, SBRT achieves cure-equivalent outcomes to surgery.
- Conventional radiation — Used over 5–6 weeks, often combined with chemotherapy.
- Proton therapy — Available at select NCI-designated centers; reduces radiation dose to surrounding healthy tissue.
Primary use cases: Inoperable early-stage NSCLC, Stage III chemoradiation, palliative pain control in Stage IV, brain metastases (whole brain or stereotactic radiosurgery). Our broader guide on radiation therapy covers the full mechanism and side effects.
3. Chemotherapy — Systemic Treatment That Still Plays a Vital Role
Chemotherapy remains a backbone of lung cancer treatment, particularly for Stage III–IV disease and SCLC.
Common regimens:
- Carboplatin + Paclitaxel — Standard for NSCLC
- Cisplatin + Pemetrexed — Preferred for non-squamous NSCLC
- Cisplatin + Etoposide — First-line SCLC standard
- Carboplatin + Etoposide + Atezolizumab — First-line extensive-stage SCLC (immunotherapy added)
Roles chemotherapy plays:
- Neoadjuvant (before surgery) — Shrinks the tumor to improve surgical outcomes
- Adjuvant (after surgery) — Kills remaining microscopic cancer cells
- Concurrent chemoradiation — Used for unresectable Stage III NSCLC
- Palliative — Controls disease and symptoms in Stage IV
For a complete breakdown of drug cycles, anti-nausea strategies, and hair loss timelines, see our 2026 chemotherapy guide with side effects.
4. Targeted Therapy — The Precision Revolution
Targeted therapy is the most transformative development in NSCLC lung cancer treatment of the past decade. These drugs attack specific genetic mutations in tumor cells rather than all fast-growing cells — meaning fewer side effects and higher response rates for the right patients.
FDA-approved targeted therapies by mutation (2026):
| Mutation | FDA-Approved Drugs |
|---|---|
| EGFR (exon 19/21) | Osimertinib (Tagrisso), erlotinib, gefitinib, afatinib |
| ALK rearrangement | Alectinib (Alecensa), brigatinib, lorlatinib |
| KRAS G12C | Sotorasib (Lumakras), adagrasib (Krazati) |
| HER2 mutation | Zongertinib (Hernexeos) — FDA accelerated approval Q1 2026 |
| MET exon 14 | Tepotinib (Tepmetko), capmatinib (Tabrecta) |
| RET alteration | Selpercatinib (Retevmo), pralsetinib (Gavreto) |
| ROS1 rearrangement | Crizotinib, entrectinib, repotrectinib |
| BRAF V600E | Dabrafenib + Trametinib |
| NTRK fusion | Larotrectinib (Vitrakvi) |
Bold Takeaway: Targeted therapy only works if your tumor carries the matching mutation. This is why biomarker testing isn’t optional — it’s the gateway to your most effective treatment. The AACR’s January–March 2026 FDA oncology approvals document these new additions in full.
For the complete list of FDA-approved lung cancer drugs in 2026, see our dedicated lung cancer FDA drugs and treatment guide.
5. Immunotherapy — Activating Your Own Immune System
Immunotherapy for lung cancer works by releasing the “brakes” on your immune system, allowing it to recognize and destroy cancer cells. It has changed the survival outlook for thousands of Stage III and IV patients.
FDA-approved checkpoint inhibitors for lung cancer:
- Pembrolizumab (Keytruda) — First-line monotherapy for NSCLC with PD-L1 ≥50%; also used in combinations
- Nivolumab (Opdivo) — Neoadjuvant use with chemotherapy (pre-surgery); second-line treatment
- Atezolizumab (Tecentriq) — Used in SCLC combinations; adjuvant use after surgery in select NSCLC
- Durvalumab (Imfinzi) — Consolidation therapy after Stage III chemoradiation (PACIFIC trial); also used in limited-stage SCLC
Who benefits most: NSCLC patients with PD-L1 expression ≥50% show the strongest response to immunotherapy monotherapy. Lower PD-L1 patients benefit from immunotherapy combined with chemotherapy. For a full overview of how immunotherapy works across cancer types, visit the NCI’s lung cancer research advances page.
6. Antibody-Drug Conjugates (ADCs) — The Smart Bomb Class
ADCs are the newest class of lung cancer treatment and arguably the most exciting development of 2025. They combine a targeted antibody (that finds the cancer cell) with a chemotherapy payload (that kills it) — delivering maximum toxicity directly to the tumor while sparing healthy tissue.
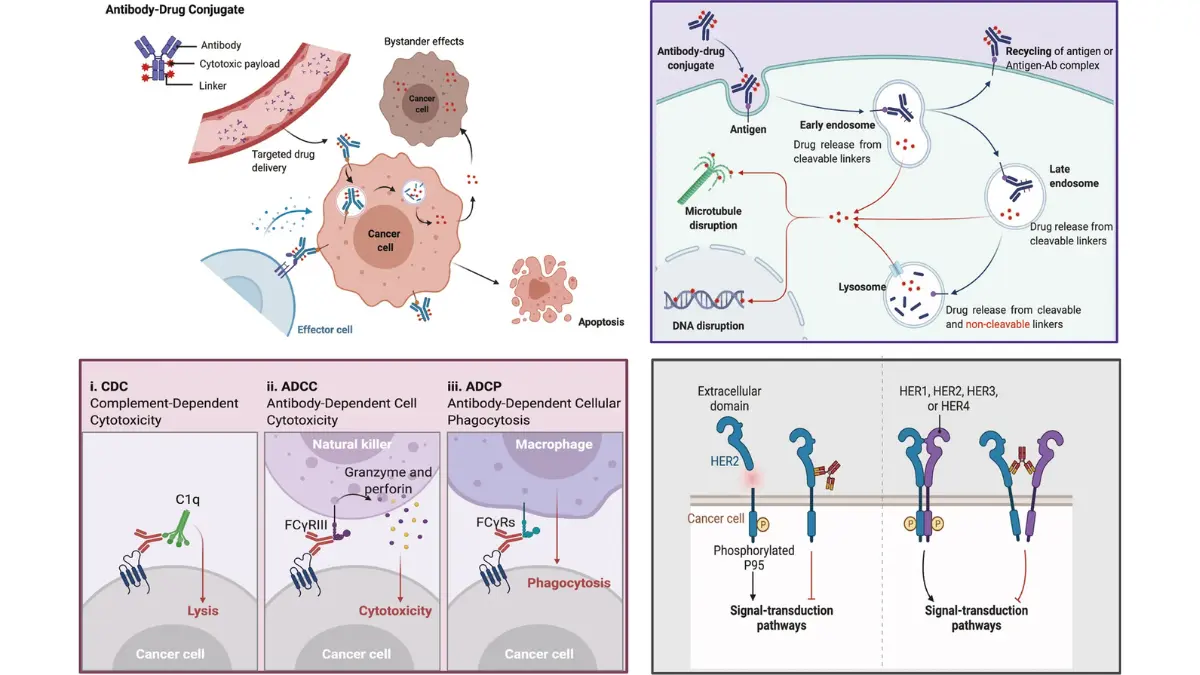
Adapted from Wikimedia Commons The_overview_of_the_mechanisms_of_ADC_for_killing_cancer_cells_via_different_approaches.webp, licensed under CC BY 4.0.
Currently approved ADCs for lung cancer:
- Datopotamab deruxtecan (Dato-DXd) — FDA approved 2025. Targets TROP-2. Indicated for EGFR-mutant NSCLC patients who progressed after a TKI and platinum-based chemotherapy.
- Trastuzumab deruxtecan (Enhertu) — Approved for HER2-mutant NSCLC (advanced).
ADCs are now embedded in ASCO 2026 guidelines as standard second-line or later-line options for select NSCLC patients. The LUNGevity Foundation’s treatment navigator provides an excellent patient-friendly overview of emerging options.
7. Clinical Trials — Access to Tomorrow’s Treatments Today
Every Stage III or Stage IV patient should ask about clinical trials at the time of diagnosis — not as a last resort.
Why clinical trials matter:
- Access to drugs 2–4 years before public approval
- Often fully covered, including travel costs at major centers
- Bispecific antibody trials currently enrolling for NSCLC and SCLC show early response rates above 50%
How to find trials: Search clinicaltrials.gov by zip code, cancer type, and mutation status. Ask your oncologist specifically about trials at NCI-designated cancer centers.
Lung Cancer Treatment by Stage — The 2026 Decision Matrix
Your treatment plan is built around your stage. Here is what NCCN guidelines and ASCO 2026 recommendations support for each stage:
| Stage | Type | Primary Treatment | Additional Options |
|---|---|---|---|
| Stage 0 | NSCLC | Surgery (curative) | — |
| Stage I | NSCLC | Surgery ± adjuvant osimertinib / atezolizumab | SBRT if inoperable |
| Stage II | NSCLC | Neoadjuvant chemo ± immunotherapy → Surgery | Adjuvant targeted therapy |
| Stage IIIA | NSCLC | Chemoradiation → Durvalumab consolidation | Surgery in select cases |
| Stage IIIB/C | NSCLC | Chemoradiation → Durvalumab | Clinical trials |
| Stage IV | NSCLC | Targeted therapy (mutation+) OR Immunotherapy ± chemo | ADCs, clinical trials |
| Limited | SCLC | Chemo + Radiation → Durvalumab | Prophylactic cranial irradiation |
| Extensive | SCLC | Chemo + Atezolizumab → Lurbinectedin + Atezolizumab maintenance | Tarlatamab (post-progression) |
To understand what stage you or a loved one is at, our lung cancer stages explained guide breaks down every stage with survival context.
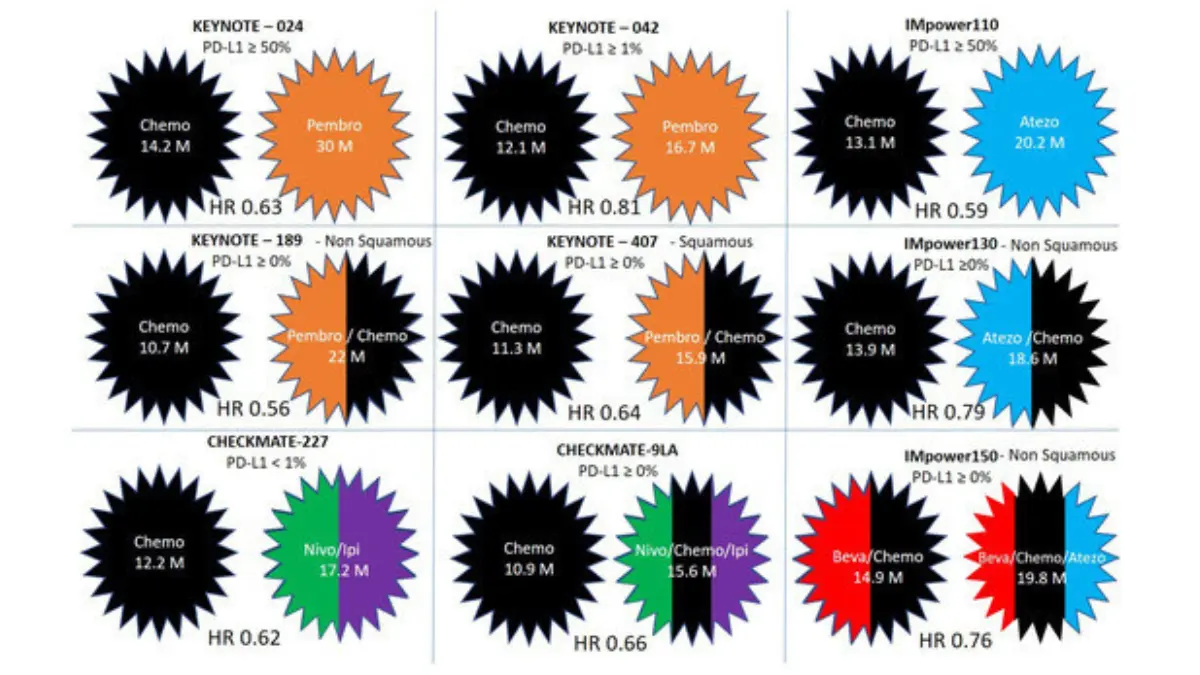
Adapted from Wikimedia Commons Overall_survival_in_non-small_lung_cancer_patients_treated_with_modern_immunotherapy_in_the_first_line_for_advanced_or_metastatic_disease.jpg, licensed under CC BY 4.0.
What If Lung Cancer Comes Back?
Recurrence does not mean options are exhausted. Second-line treatments include:
- Switching targeted therapy (e.g., from erlotinib to osimertinib after EGFR T790M resistance mutation develops)
- Immunotherapy if not used in first-line
- Tarlatamab (Imdelltra) — FDA received full approval November 19, 2025, specifically for recurrent extensive-stage SCLC after platinum-based chemotherapy. Memorial Sloan Kettering reported this as a landmark approval for SCLC patients with limited prior options.
- ADCs as later-line NSCLC options
- Clinical trials for novel agents
Bold Callout: “Recurrence is not a dead end. More second-line lung cancer treatment options exist in 2026 than at any point in history.”
For stage-specific survival data, our lung cancer statistics and survival rates guide provides the most current SEER database figures.
2025–2026 FDA Approvals That Changed Lung Cancer Treatment
2025 was the single most productive year for lung cancer drug approvals in FDA history. Seven new agents were approved for NSCLC alone. Here are the most important developments for patients:
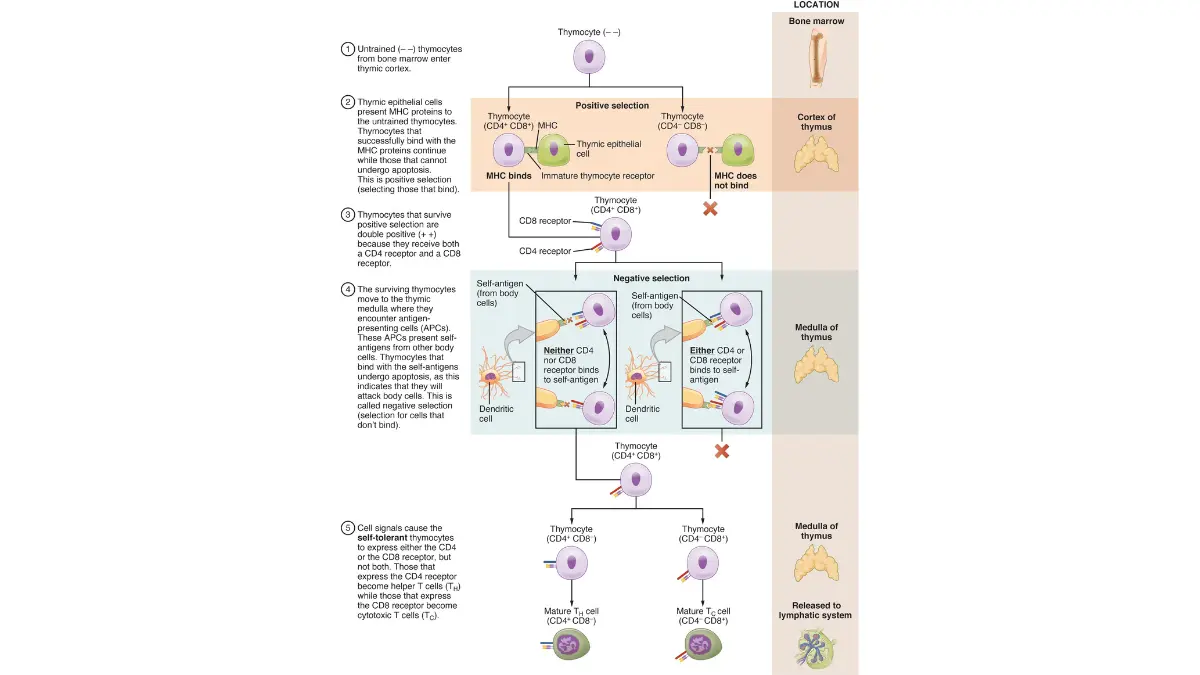
Adapted from OpenStax Anatomy and Physiology 2e, 21.3 The Adaptive Immune Response: T Lymphocytes and Their Functional Types, licensed under CC BY 4.0.
✅ Tarlatamab (Imdelltra) — Full Approval, November 2025
- What it is: First-in-class bispecific T-cell engager (BiTE) targeting DLL3 on SCLC tumor cells and CD3 on T cells
- Who it helps: Adults with extensive-stage SCLC who progressed on platinum-based chemotherapy
- Phase III result (DeLLphi-304): Statistically significant overall survival improvement vs. standard of care
✅ Lurbinectedin + Atezolizumab — Approved October 2025
- What it is: Maintenance immunotherapy combination for extensive-stage SCLC
- Based on: IMforte Phase III trial showing improved overall survival vs. atezolizumab alone
✅ Datopotamab Deruxtecan (Dato-DXd) — Approved 2025
- What it is: TROP-2-directed ADC
- Who it helps: EGFR-mutant NSCLC patients who already received a TKI and platinum chemotherapy
✅ Zongertinib (Hernexeos) — Accelerated Approval, Q1 2026
- What it is: First HER2-selective tyrosine kinase inhibitor for lung cancer
- Who it helps: Adults with unresectable or metastatic non-squamous NSCLC harboring HER2 tyrosine kinase domain mutations
✅ Amivantamab + Lazertinib (MARIPOSA trial)
- What it is: EGFR-MET bispecific antibody + 3rd-generation EGFR TKI combination
- Result: Superior progression-free survival vs. osimertinib monotherapy in first-line EGFR-mutant NSCLC — now incorporated into ASCO 2026 living guidelines
The NCI’s Cancer Trends Progress Report on lung cancer treatment tracks how these approvals are changing real-world treatment utilization nationally.
Survivorship — Life During and After Lung Cancer Treatment
Treatment is only part of the journey. Managing your body through therapy matters enormously for outcomes.
Nutrition and Weight During Treatment
Maintaining lean muscle mass during chemotherapy is directly linked to better tolerance and recovery. Use our Protein Intake Calculator to ensure you are meeting your daily protein targets during active treatment. Staying hydrated is equally critical — use the Water Intake Calculator to set daily hydration goals adjusted for your body weight and treatment schedule.
Exercise During Lung Cancer Treatment
Cardiopulmonary exercise is safe and recommended for most patients during treatment unless otherwise directed by your oncologist. Use our Heart Rate Zone Calculator to identify the safe aerobic zones for light walking or supervised exercise programs — a critical tool as surgery or chemo may reduce your baseline lung capacity.
Sleep and Recovery
Fatigue is the most commonly reported side effect across all lung cancer treatments. Our Sleep Calculator helps you optimize sleep timing around treatment days to improve recovery quality.
Monitoring Medications and Side Effects
If you are taking corticosteroids to manage immunotherapy-related inflammation, blood glucose monitoring is essential. Use our Blood Sugar Converter to interpret your glucose readings. If you are ever unsure about a medication you have been prescribed, our Pill Identifier can help you confirm the drug name and dosage.
Insurance and Financial Access to Treatment
Most FDA-approved targeted therapies are covered under Medicare Part B (infusion-based drugs) or Part D (oral targeted therapies like osimertinib). Major manufacturers offer patient assistance programs:
- AstraZeneca (Tagrisso/osimertinib): AZ&Me Prescription Savings Program
- Amgen (Imdelltra/tarlatamab): Amgen SupportPlus
- Merck (Keytruda/pembrolizumab): Merck Access Program
The American Cancer Society NSCLC treatment guide includes financial assistance resources for uninsured and underinsured patients.
Your Lung Cancer Treatment Action Plan — 5 Questions to Ask Your Oncologist
Most patients leave their first oncology appointment overwhelmed and underprepared. These five questions change that outcome.
1. “Have you ordered complete biomarker testing — including EGFR, ALK, KRAS G12C, HER2, ROS1, MET, BRAF, RET, and PD-L1?” If the answer is no, this must be done before any treatment begins.
2. “Based on my mutation profile, do I qualify for targeted therapy or a first-line immunotherapy regimen?” This question separates patients who receive generic chemo from those who get precision medicine.
3. “Am I eligible for any active clinical trials — including Phase II or III trials at NCI-designated cancer centers?” Trials are not a last resort. They are often the fastest path to the newest therapies.
4. “What is the realistic goal of my treatment plan — cure, long-term control, or symptom management?” Knowing the goal shapes every decision about quality of life, side effects, and second opinions.
5. “Can you refer me to a thoracic oncology specialist or tumor board at a major cancer center for a second opinion?” Second opinions at NCI-designated centers regularly change treatment plans. This is especially true for Stage III and Stage IV NSCLC.
What This Means For You: If you haven’t been diagnosed yet but are experiencing persistent symptoms, use our Symptom Checker and read our guide on early signs of lung cancer immediately. Early detection is still the single most powerful factor in survival. The NCI’s small cell lung cancer treatment PDQ is also an essential resource for patients with SCLC seeking a government-level treatment reference.
To understand survival outcomes by stage, our Stage 1 lung cancer survival guide and small cell lung cancer survival rates articles provide current SEER data with 2026 updates.
Frequently Asked Questions About Lung Cancer Treatment
1. What is the most effective lung cancer treatment in 2026?
There is no single “best” treatment — it depends on your cancer type, stage, and molecular mutations. For EGFR-mutant NSCLC, osimertinib (Tagrisso) shows the highest documented response rates. For PD-L1 ≥50% NSCLC, pembrolizumab monotherapy outperforms chemotherapy in overall survival.
2. Can lung cancer be cured?
Yes — Stage I NSCLC has a 5-year survival rate of 68–92% after surgery. Cure is a realistic goal for early-stage disease. Stage III and IV focus on long-term control and quality of life, though some patients achieve durable remission.
3. What is the first-line treatment for Stage IV lung cancer?
For mutation-positive NSCLC: targeted therapy (e.g., osimertinib for EGFR, alectinib for ALK). For PD-L1 ≥50% without driver mutations: pembrolizumab alone. For others: pembrolizumab + platinum-based chemotherapy.
4. What are the main side effects of lung cancer treatment?
Side effects vary by treatment. Chemotherapy causes fatigue, nausea, and hair loss. Targeted therapy commonly causes skin rash and diarrhea. Immunotherapy can trigger immune-related reactions affecting the lungs, liver, or thyroid.
5. How long does lung cancer treatment last?
Surgery is a one-time procedure with a 4–6 week recovery. Chemotherapy typically runs 4–6 cycles (3 months). Targeted therapy is taken daily indefinitely until disease progression. Immunotherapy infusions are given every 3–6 weeks, often for 2 years.
6. Is immunotherapy better than chemotherapy for lung cancer?
For patients with high PD-L1 expression (≥50%) and no actionable mutation, pembrolizumab monotherapy shows superior overall survival compared to platinum-based chemotherapy. For lower PD-L1 patients, combination immunotherapy + chemotherapy outperforms chemo alone.
7. What is targeted therapy for lung cancer?
Targeted therapy uses drugs designed to attack specific genetic mutations in cancer cells — such as EGFR, ALK, or KRAS G12C — rather than all rapidly dividing cells. It requires biomarker testing to confirm eligibility.
8. What is the newest lung cancer treatment approved in 2026?
Zongertinib (Hernexeos) received FDA accelerated approval in Q1 2026 for adults with unresectable or metastatic non-squamous NSCLC with HER2 tyrosine kinase domain mutations. It is the first HER2-selective TKI approved for lung cancer.
9. Can small cell lung cancer be treated with immunotherapy?
Yes. Atezolizumab combined with carboplatin/etoposide is standard first-line treatment for extensive-stage SCLC. Tarlatamab (Imdelltra) received full FDA approval in November 2025 for patients with SCLC that progressed after prior therapy.
10. What happens if lung cancer stops responding to treatment?
If first-line treatment fails, second-line options include a different chemotherapy regimen, alternative targeted therapies (e.g., switching TKIs after resistance mutation develops), ADCs such as Dato-DXd, or enrollment in clinical trials. Palliative and hospice care are also important options focused on quality of life.
11. How do I find lung cancer clinical trials near me?
Visit clinicaltrials.gov, enter your zip code, select “Lung Cancer,” and filter by your cancer type and treatment history. Ask your oncologist to contact the trial team directly — patient advocates at NCI-designated cancer centers can also assist with enrollment navigation.
This article is reviewed and updated regularly to reflect the latest FDA approvals, NCCN guidelines, and ASCO living guideline updates. Last clinical review: May 2026.
For educational purposes only. Not a substitute for professional medical advice, diagnosis, or treatment. Always seek guidance from a qualified oncologist.
🔗 Continue Reading:
- What Is Lung Cancer? — Complete Pillar Guide
- Lung Cancer Stages Explained
- NSCLC vs SCLC — Full Comparison
- Lung Cancer FDA Drugs & Treatments 2026
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.