On This Page – Quick Medical Summary
What Is Rheumatoid Factor & Why Your RF Levels Matter
Sarah, a 42-year-old teacher from Denver, woke up one morning unable to make a fist. Her hands felt stiff, swollen, and painful—symptoms that wouldn’t go away after an hour like typical morning stiffness. After weeks of struggling to button her blouse and grip a coffee mug, her doctor ordered a rheumatoid factor test. The results showed RF levels of 78 IU/mL—nearly four times the normal range. That single blood test changed everything, leading to an early rheumatoid arthritis diagnosis and treatment that preserved her joint function.
Rheumatoid Factor Levels: Normal <20, High >60 & What It Means
Rheumatoid factor levels measure the concentration of RF autoantibodies in your blood, typically expressed in international units per milliliter (IU/mL). Normal rheumatoid factor levels fall below 20 IU/mL, while levels exceeding 60 IU/mL indicate significantly elevated RF that strongly suggests autoimmune disease. Understanding these numbers helps doctors diagnose conditions like rheumatoid arthritis and predict disease severity, making RF level interpretation crucial for your health journey.
What Is Rheumatoid Factor?
Rheumatoid factor is an autoantibody—a protein your immune system produces by mistake that attacks your body’s own tissues instead of foreign invaders. Specifically, RF targets the fragment crystallizable (Fc) region of immunoglobulin G (IgG), which is one of your body’s most common antibodies designed to fight infections. While your immune system normally creates antibodies to protect you from bacteria and viruses, rheumatoid factor turns against healthy cells in a process called autoimmunity.

The presence of rheumatoid factor isn’t always abnormal. Research from the National Institutes of Health shows that up to 14% of healthy people over age 70 test positive for low levels of RF without having any autoimmune disease. However, when RF levels climb above normal ranges—especially above 60 IU/mL—they become clinically significant markers of inflammatory conditions.
Why Rheumatoid Factor Levels Matter for Diagnosis
The specific rheumatoid factor levels in your bloodstream tell a more complete story than simply “positive” or “negative” results. According to MedlinePlus, higher RF concentrations correlate with increased likelihood of rheumatoid arthritis and predict more aggressive disease progression. About 70-80% of people with rheumatoid arthritis test positive for elevated RF, and those with RF levels exceeding 60 IU/mL face greater risks of joint erosion, extra-articular manifestations, and disability.
Understanding your RF measurement in IU/mL units is essential. Most laboratories use the international unit per milliliter (IU/mL) standard to quantify rheumatoid factor levels, though some may report results in units per milliliter (U/mL)—functionally the same measurement. This standardization allows doctors worldwide to compare results and make consistent treatment decisions based on your specific numbers.
If you’re experiencing unexplained joint pain, stiffness, or swelling, using our Symptom Checker can help identify whether your symptoms warrant a rheumatoid factor test. Early detection makes a profound difference—patients diagnosed and treated within the first six months of symptom onset have significantly better long-term outcomes than those who delay.
What This Means For You
Your rheumatoid factor levels aren’t just numbers—they’re predictive markers that guide diagnosis and treatment intensity. While RF below 20 IU/mL is considered normal, levels between 20-40 IU/mL require monitoring, and anything above 60 IU/mL demands comprehensive evaluation by a rheumatologist. The higher your RF levels, the more aggressive your treatment approach should be to prevent irreversible joint damage.
Rheumatoid Factor Normal Range & Complete RF Level Chart
Rheumatoid Factor Normal Range: Understanding Your Numbers
The standard rheumatoid factor normal range falls below 20 IU/mL in most clinical laboratories across the United States, though some facilities use a stricter cutoff of 14 IU/mL or lower. According to the University of Florida Pathology Laboratories, RF levels at or below 14 IU/mL are definitively considered negative, while the University of Rochester Medical Center uses the 20 U/mL threshold as their upper limit of normal.
Understanding these reference ranges is crucial because rheumatoid factor levels exist on a continuum, not simply as positive or negative results. Research published by the National Institutes of Health demonstrates that RF specificity increases dramatically with higher titers—from 89% at 20 IU/mL to 97.1% at 60 IU/mL and above. This means that higher rheumatoid factor levels provide more diagnostic certainty for autoimmune conditions like rheumatoid arthritis.
Laboratory methods vary slightly between facilities, with some using nephelometry and others employing immunoturbidimetric assays to measure rheumatoid factor test results. Despite these methodological differences, the IU/mL unit standardization allows physicians to interpret RF levels consistently worldwide and compare your results across different testing locations throughout your treatment journey.
Complete Rheumatoid Factor Levels Chart
Research from the NIH National Library of Medicine confirms that patients with rheumatoid factor levels exceeding 245 IU/mL face significantly higher risks of extra-articular rheumatoid arthritis manifestations, including lung involvement, vasculitis, and rheumatoid nodules.

What Does Rheumatoid Factor 20 Mean?
A rheumatoid factor 20 result sits precisely at the diagnostic threshold, representing a borderline positive finding that requires careful clinical interpretation. According to Hospital for Special Surgery, RF levels at 20 IU/mL alone aren’t sufficient to diagnose rheumatoid arthritis—physicians must consider your symptoms, physical examination findings, and additional blood tests like anti-CCP antibodies.
If you’re experiencing joint stiffness lasting more than 30 minutes each morning, swelling in multiple small joints, or symmetrical pain patterns, a rheumatoid factor 20 result warrants further investigation even though it’s technically at the normal-abnormal boundary. Your doctor should order complementary tests and potentially use our Blood Sugar Converter to rule out metabolic conditions that can mimic RA symptoms.
What Does Rheumatoid Factor 60 Mean?
Rheumatoid factor 60 represents a high positive result that strongly suggests rheumatoid arthritis, with specificity reaching 97.1% according to NIH-published research. At this rheumatoid factor level, patients face increased risk of aggressive joint erosion, higher disease activity scores, and greater likelihood of requiring biologic disease-modifying drugs.
Studies show that RF levels exceeding 60 IU/mL correlate with more rapid radiographic progression and worse functional outcomes without prompt treatment. The three-times-upper-limit threshold (3xULN) that a rheumatoid factor 60 result represents earns the highest scoring in the 2010 ACR/EULAR diagnostic criteria for RA classification.
What Does Rheumatoid Factor 100 Mean?
A rheumatoid factor 100 result indicates very high positive RF levels associated with severe rheumatoid arthritis requiring immediate aggressive intervention. Patients with rheumatoid factor levels in the 100-200 IU/mL range demonstrate significantly elevated risk for extra-articular manifestations affecting the lungs, heart, blood vessels, and skin.
Clinical data from multi-center European studies reveal that RF levels above 100 IU/mL predict longer disease duration, more joint damage, and greater functional disability without early combination therapy using conventional synthetic disease-modifying antirheumatic drugs. If your RF test results show levels at or above 100 IU/mL, consulting a rheumatologist within two weeks maximizes your chance of preventing irreversible joint destruction.
International Rheumatoid Factor Reference Ranges
While North American laboratories predominantly use the 14-20 IU/mL cutoff for rheumatoid factor normal range, international standards show slight variations. European laboratories following EULAR guidelines often employ similar thresholds but emphasize the importance of tiered RF level interpretation rather than simple positive/negative categorization. Asian-Pacific regions may use different assay methodologies, though results remain comparable when standardized to IU/mL units.
These international consensus panels agree that rheumatoid factor levels above 60 IU/mL warrant identical aggressive treatment approaches regardless of geographic location, reflecting the universal prognostic significance of high-titer RF in predicting severe rheumatoid arthritis outcomes.
High Rheumatoid Factor & Elevated RF: Causes & Interpretation
High Rheumatoid Factor: What Elevated RF Levels Really Mean
High rheumatoid factor levels—defined as RF values exceeding 60 IU/mL—signal significant autoimmune activity in your body, but contrary to popular belief, they don’t always indicate rheumatoid arthritis. Elevated rheumatoid factor appears in approximately 5-10% of healthy individuals over age 65, and up to 20% of people with other chronic conditions test positive despite never developing RA. Understanding what drives your high rheumatoid factor helps distinguish between various diagnoses and guides your physician toward the most appropriate treatment strategy.
The critical insight: rheumatoid factor positive results demand comprehensive evaluation, not immediate panic. Your doctor must correlate elevated RF levels with clinical symptoms, imaging findings, and complementary blood tests to determine the underlying cause.
Rheumatoid Arthritis – The Primary Cause
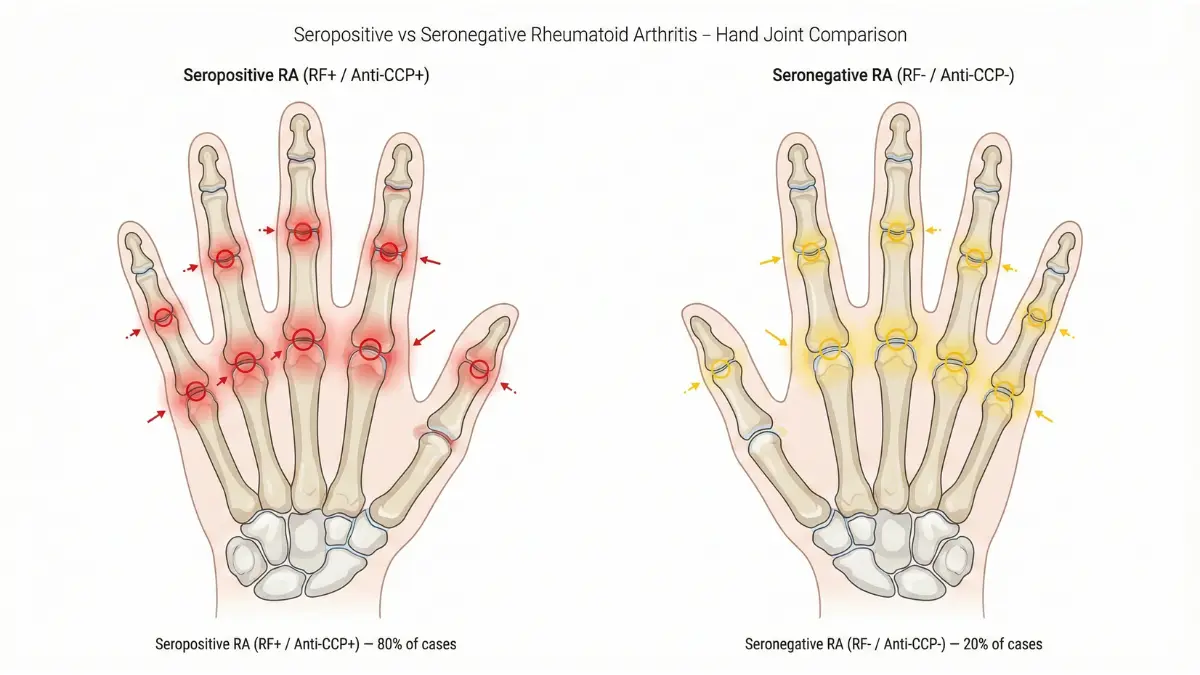
Rheumatoid arthritis remains the leading cause of high rheumatoid factor levels, accounting for 70-80% of elevated RF cases in symptomatic patients. According to research from the National Institute of Arthritis and Musculoskeletal and Skin Diseases, seropositive RA patients—those with rheumatoid factor positive and anti-CCP positive results—experience more aggressive disease progression compared to seronegative patients.
Higher rheumatoid factor levels in RA correlate directly with disease severity. Patients with RF exceeding 100 IU/mL demonstrate significantly increased risks of:
- Joint erosions visible on X-ray within the first two years of diagnosis
- Extra-articular manifestations affecting lungs, heart, and blood vessels
- Rheumatoid nodules developing on pressure points like elbows and fingers
- Accelerated disability requiring joint replacement surgery
Early diagnosis transforms outcomes—understanding your family history and genetic predispositions through tools like our Genetic Risk Assessment Tool helps identify elevated RA risk before symptoms become severe.
Other Autoimmune Conditions That Cause High RF
Elevated rheumatoid factor appears in multiple autoimmune diseases beyond rheumatoid arthritis, making differential diagnosis essential. Research published by the National Institutes of Health documents significant RF elevation in:
- Sjögren’s syndrome: 50-90% of patients test rheumatoid factor positive, often with RF levels between 40-100 IU/mL
- Systemic lupus erythematosus (SLE): 15-35% show elevated RF, typically lower titers (20-60 IU/mL)
- Mixed connective tissue disease: Nearly 60% demonstrate positive RF alongside other autoantibodies
- Systemic sclerosis (scleroderma): 20-30% exhibit rheumatoid factor positive results
- Polymyositis and dermatomyositis: Occasional RF elevation in 10-15% of cases
The rheumatoid factor test alone cannot distinguish between these conditions—physicians rely on symptom patterns, additional autoantibody testing, and physical examination findings to pinpoint the correct diagnosis.
Non-Autoimmune Causes of Elevated Rheumatoid Factor
High rheumatoid factor doesn’t always signal autoimmune disease, making proper rheumatoid factor interpretation crucial for avoiding misdiagnosis. The MedlinePlus Medical Encyclopedia documents several non-rheumatic conditions that produce elevated RF levels:
- Chronic infections: Hepatitis C virus infection (up to 70% RF positive), tuberculosis, bacterial endocarditis, and parasitic diseases can trigger RF production
- Liver disease: Chronic hepatitis, cirrhosis, and primary biliary cholangitis elevate RF in 15-40% of patients
- Chronic lung disease: Interstitial pulmonary fibrosis, sarcoidosis, and silicosis occasionally cause positive RF
- Malignancies: Rare cases of lymphoma, leukemia, and solid tumors produce RF as a paraneoplastic phenomenon
- Normal aging: RF levels gradually increase with age—4% of healthy people under 60 and 10-14% over 70 test positive
Understanding False Positive RF Results
False positive rheumatoid factor results occur when RF levels exceed normal range without any underlying disease, affecting 5-15% of test results depending on the population studied. According to University of Rochester Medical Center clinical guidelines, RF specificity improves dramatically at higher titers—only 3% of people with RF above 60 IU/mL represent true false positives, compared to 15-20% at the 20-30 IU/mL borderline range.
Transient RF elevation can result from recent vaccinations, acute infections, or even strenuous exercise in susceptible individuals. If your rheumatoid factor positive result occurs without symptoms like joint pain, morning stiffness, or swelling, your doctor should retest in 6-12 weeks before pursuing aggressive diagnostic workup.
What This Means For You
High rheumatoid factor levels demand investigation but don’t guarantee a rheumatoid arthritis diagnosis. If your RF exceeds 60 IU/mL, insist on comprehensive evaluation including anti-CCP testing, inflammatory marker assessment (ESR and CRP), and thorough symptom review. Even with elevated RF, absence of joint symptoms may indicate a different condition or benign RF positivity that requires monitoring rather than immediate treatment.
Rheumatoid Factor Negative, Seronegative RA & Anti-CCP Testing
Rheumatoid Factor Negative: Can You Still Have Rheumatoid Arthritis?
Maria, a 38-year-old graphic designer from Chicago, spent eight months visiting different doctors for her painful, swollen wrists and ankles. Every rheumatoid factor test came back negative—RF levels consistently below 10 IU/mL—leading some physicians to dismiss her symptoms as “just stress”. Finally, a thorough rheumatologist ordered an anti-CCP antibody test, which revealed strongly positive results at 180 U/mL, confirming seronegative rheumatoid arthritis that had been silently damaging her joints for months.
Yes, you can absolutely have rheumatoid arthritis with rheumatoid factor negative results. Approximately 20-30% of all rheumatoid arthritis patients test negative for RF throughout their entire disease course, a condition clinically classified as seronegative rheumatoid arthritis. According to the National Library of Medicine, these patients experience genuine RA with joint inflammation, potential erosions, and disability despite their rheumatoid factor test showing normal ranges below 20 IU/mL.
This critical diagnostic gap means that rheumatoid factor negative results should never rule out RA when classic symptoms persist—morning stiffness lasting over 60 minutes, symmetrical small joint swelling, and progressive functional limitation all warrant comprehensive evaluation regardless of RF status.
What Is Seronegative Rheumatoid Arthritis?
Seronegative rheumatoid arthritis describes confirmed RA cases where patients test negative for both rheumatoid factor and anti-CCP antibodies, though the term often applies more broadly to anyone with rheumatoid factor negative status. Research from the Arthritis Foundation indicates that 20% of RA patients remain seronegative throughout their disease journey, presenting unique diagnostic and treatment challenges.
Seronegative RA typically follows a milder disease course than seropositive RA, with slower radiographic progression and fewer extra-articular manifestations. However, “milder” doesn’t mean “mild”—without proper treatment, seronegative patients still develop joint erosions, deformities, and significant functional impairment. The diagnostic challenge lies in distinguishing seronegative RA from other inflammatory arthritis conditions like psoriatic arthritis, reactive arthritis, or early ankylosing spondylitis when biomarkers remain absent.
If you’re experiencing unexplained joint symptoms despite rheumatoid factor negative results, our Symptom Checker can help document your symptom patterns to share with your rheumatologist.
RF vs. Anti-CCP: Understanding the Difference
| Characteristic | Rheumatoid Factor (RF) | Anti-CCP Antibody |
|---|---|---|
| Sensitivity for RA | 60-80% | 60-75% |
| Specificity for RA | 85% (at 60+ IU/mL) | 95-98% |
| Appears Before Symptoms | Occasionally (months before) | Often (up to 10 years before) |
| Predicts Disease Severity | Yes—higher RF = worse outcomes | Yes—higher anti-CCP = erosive disease |
| Found in Other Conditions | Common (infections, other autoimmune diseases) | Rare (highly specific to RA) |
| Best Clinical Use | Screening and diagnosis support | Definitive RA confirmation; early detection |
| False Positive Rate | 15-20% in general population | 2-5% in general population |
Data compiled from NIH research publications demonstrates that combining rheumatoid factor test results with anti-CCP antibody testing achieves 99% specificity for rheumatoid arthritis diagnosis when both are positive.
Anti-CCP Antibody Test: The Missing Piece
Anti-cyclic citrullinated peptide (anti-CCP) antibodies represent highly specific biomarkers for rheumatoid arthritis, with 95-98% specificity compared to rheumatoid factor’s 85% specificity. According to MedlinePlus CCP Antibody Test guidelines, anti-CCP antibodies target citrullinated proteins—modified proteins found in inflamed joint tissue—making them remarkably specific for RA rather than other autoimmune conditions.
The anti-CCP test proves especially valuable for rheumatoid factor negative patients, detecting RA in 40-50% of seronegative cases. Research published by the National Institutes of Health shows that anti-CCP antibodies can appear up to 10 years before clinical RA symptoms manifest, offering a critical window for preventive intervention.
Normal anti-CCP levels fall below 20 U/mL, with values exceeding 60 U/mL strongly indicating rheumatoid arthritis regardless of rheumatoid factor status. Patients positive for both RF and anti-CCP face the highest risk for aggressive, erosive disease requiring intensive treatment with disease-modifying antirheumatic drugs and biologics.
Other Blood Tests for Rheumatoid Arthritis
When rheumatoid factor test results and anti-CCP antibodies remain negative despite persistent symptoms, physicians employ additional blood tests to support rheumatoid arthritis blood test diagnosis:
- Erythrocyte Sedimentation Rate (ESR): Measures inflammation levels; elevated ESR (>30 mm/hr) suggests active inflammatory arthritis
- C-Reactive Protein (CRP): Another inflammation marker that rises during RA flares; normal <10 mg/L
- Complete Blood Count (CBC): Detects anemia common in chronic RA; low hemoglobin indicates disease activity
- Antinuclear Antibodies (ANA): Helps distinguish RA from lupus; positive in 20-30% of RA patients
Managing overall health alongside RA treatment improves outcomes—tools like our BMI Calculator help monitor weight management crucial for reducing joint stress in arthritis patients.
What This Means For You
Rheumatoid factor negative results don’t exclude rheumatoid arthritis—they simply mean you need comprehensive evaluation including anti-CCP testing, inflammatory markers, and clinical assessment. If you have symmetrical joint pain, morning stiffness exceeding 30 minutes, and rheumatoid factor levels below 20 IU/mL, insist your doctor order anti-CCP antibodies and consider referral to a rheumatologist. Early seronegative RA diagnosis prevents irreversible joint damage even when traditional biomarkers remain absent.
The Rheumatoid Factor Test – Procedure, Results & What to Expect
Rheumatoid Factor Test: Everything You Need to Know
When Your Doctor Orders an RF Test
Your physician typically orders a rheumatoid factor test when you present with specific symptoms suggesting inflammatory arthritis or autoimmune disease. According to MedlinePlus, the most common triggers for RF testing include:
- Morning joint stiffness lasting 30 minutes or longer after waking
- Symmetrical joint swelling, especially in hands, wrists, or feet
- Persistent joint pain affecting multiple joints simultaneously for 6+ weeks
- Fatigue and low-grade fever accompanying joint symptoms
- Family history of rheumatoid arthritis or autoimmune conditions
- Unexplained inflammation markers (elevated ESR or CRP) on routine blood work
The rheumatoid factor test serves as a first-line screening tool that helps rheumatologists determine whether your symptoms stem from RA, another autoimmune condition, or non-inflammatory causes requiring different treatment approaches.
The RF Blood Test Procedure
The rheumatoid factor test involves a simple venipuncture blood draw identical to routine laboratory work, requiring no special preparation or fasting. A phlebotomist or nurse will:
- Clean the injection site (typically inside your elbow) with an antiseptic wipe
- Apply a tourniquet around your upper arm to make veins more visible
- Insert a small needle to collect 5-10 milliliters of blood (about 1-2 teaspoons)
- Remove the needle and apply pressure with gauze to prevent bruising
- Label your sample and send it to the laboratory for analysis
The entire rheumatoid factor test procedure takes less than 5 minutes and causes minimal discomfort—most patients describe it as a brief pinching sensation. Unlike some diagnostic tests, the RF blood test requires no fasting, medication adjustments, or activity restrictions before or after the procedure. You can eat, drink, take your regular medications, and resume normal activities immediately.
Results typically return within 24-72 hours, though some facilities offer same-day rheumatoid factor test results for urgent cases. The laboratory measures RF levels using nephelometry or immunoturbidimetric methods that quantify antibody concentrations in IU/mL units.
RF Test Cost & Insurance Coverage
Rheumatoid factor test costs vary significantly based on your testing location and insurance coverage. According to healthcare pricing data:
- In-person laboratory testing: $15-$26 through Quest Diagnostics, LabCorp, or hospital labs with insurance
- Self-pay rates: $35-$75 without insurance at commercial laboratories
- At-home test kits: $39-$100 for mail-in rheumatoid factor testing services
- Hospital-based testing: $50-$150 when ordered during emergency or specialty visits
Most health insurance plans cover rheumatoid factor testing when medically necessary—meaning your doctor orders it based on symptoms or diagnostic workup rather than routine screening. Medicare Part B covers RF testing at 100% after deductible when ordered by your physician for diagnostic purposes, as outlined in Medicare coverage guidelines. Medicaid programs in all 50 states also cover medically necessary rheumatoid factor test costs with minimal or no copayment.
Understanding healthcare costs alongside your treatment plan is essential—our Health Tips section provides guidance on navigating insurance, managing medical expenses, and advocating for necessary testing coverage.
Understanding Your RF Test Results Report
Your rheumatoid factor test results report will display several key components that help interpret your RF levels:
- Your RF value in IU/mL or U/mL (functionally identical units)
- Reference range showing the laboratory’s normal threshold (typically <14-20 IU/mL)
- Flag indicators marking results as “negative,” “positive,” or “high”
- Testing methodology (nephelometry, immunoturbidimetry, or ELISA)
The report may use terminology like “normal,” “negative,” or “<20 IU/mL” interchangeably to indicate rheumatoid factor levels within the standard range. Conversely, “positive,” “elevated,” “high,” or any value exceeding 20 IU/mL signals abnormal RF requiring clinical correlation with your symptoms and additional testing.
Remember that rheumatoid factor interpretation requires clinical context—your doctor evaluates RF results alongside your physical examination, symptom duration, imaging studies, and other blood tests rather than treating the number in isolation.
What Happens After a Positive RF Test
When your rheumatoid factor test returns positive (RF >20 IU/mL), your physician initiates a systematic diagnostic workup to determine the underlying cause and appropriate treatment:
- Additional autoantibody testing: Anti-CCP antibodies, ANA (antinuclear antibodies), and other specific autoimmune markers
- Inflammatory markers: ESR and CRP to quantify inflammation levels
- Imaging studies: X-rays of affected joints to detect early erosions; ultrasound or MRI for detailed soft tissue assessment
- Rheumatology referral: Consultation with a board-certified rheumatologist specializing in autoimmune arthritis
- Joint examination: Detailed assessment of swelling, tenderness, range of motion, and functional limitations
According to National Institute of Arthritis and Musculoskeletal and Skin Diseases guidelines, patients with rheumatoid factor positive results exceeding 60 IU/mL should see a rheumatologist within 2-4 weeks to prevent irreversible joint damage through early treatment intervention.
What This Means For You
The rheumatoid factor test is a quick, painless, affordable screening tool that opens the door to proper diagnosis and treatment. If your RF levels exceed 20 IU/mL, don’t delay follow-up appointments—early rheumatoid arthritis treatment within the first 3-6 months of symptoms dramatically improves long-term outcomes and prevents disability. Even with normal rheumatoid factor test results below 20 IU/mL, persistent joint symptoms warrant comprehensive evaluation including anti-CCP testing to rule out seronegative RA.
Living with High RF Levels – Treatment, Monitoring & Lifestyle
Managing High Rheumatoid Factor Levels: Treatment & Lifestyle Strategies
Receiving high rheumatoid factor test results can feel overwhelming, but understanding that elevated RF levels respond to treatment offers hope and direction. Modern rheumatology has transformed rheumatoid arthritis from a progressively disabling disease into a manageable chronic condition when diagnosed early and treated appropriately. Your rheumatoid factor levels serve as both a diagnostic tool and a monitoring marker that helps physicians track treatment effectiveness and adjust therapeutic strategies over time.
Treatment Approaches Based on RF Levels
Treatment intensity for rheumatoid factor positive patients correlates directly with RF levels, disease activity, and radiographic findings. According to American College of Rheumatology guidelines available through ACR.org, rheumatologists use a treat-to-target approach that adjusts medications based on achieving low disease activity or remission rather than simply managing symptoms.
| RF Range (IU/mL) | Typical Treatment Approach | Monitoring Frequency |
|---|---|---|
| 20-40 (Borderline/Mild) | Hydroxychloroquine or methotrexate monotherapy; NSAIDs for symptom relief; lifestyle modifications emphasized | Every 3-6 months; annual imaging |
| 40-60 (Moderate) | Methotrexate with or without combination DMARDs; corticosteroid bridge therapy during flares; aggressive PT/OT | Every 2-3 months; imaging every 6-12 months |
| >60 (High/Severe) | Combination DMARDs plus biologic agents (TNF inhibitors, IL-6 inhibitors, JAK inhibitors); intensive monitoring for complications | Monthly initially, then every 2-3 months; imaging every 6 months |
Disease-modifying antirheumatic drugs (DMARDs) like methotrexate, leflunomide, and sulfasalazine form the cornerstone of treatment for rheumatoid factor positive RA. These medications don’t just relieve symptoms—they actually slow disease progression, prevent joint erosions, and can reduce rheumatoid factor levels over time. Patients with rheumatoid factor levels exceeding 100 IU/mL often require biologic agents targeting specific immune pathways, including TNF-alpha blockers, B-cell depleting agents, or IL-6 receptor antagonists.
Experimental treatments currently in clinical trials include small molecule inhibitors, tolerance-inducing therapies, and personalized medicine approaches based on genetic profiling and autoantibody patterns, as documented in ongoing research at the National Institutes of Health.

Can Rheumatoid Factor Levels Decrease?
Yes, rheumatoid factor levels can and do decrease with effective treatment. Research demonstrates that successful DMARD therapy reduces RF levels in 30-50% of patients, with the greatest reductions occurring in those achieving clinical remission. Patients starting biologic therapies like rituximab (which depletes B-cells that produce RF antibodies) often see dramatic RF level drops within 3-6 months.
Monitoring RF trends over time provides more valuable information than single measurements. A patient whose rheumatoid factor levels decrease from 120 IU/mL to 45 IU/mL over six months demonstrates excellent treatment response, even if RF remains technically positive. Conversely, rising RF levels despite treatment may signal inadequate disease control requiring medication adjustments or switches to alternative therapeutic classes.
Your rheumatology team tracks rheumatoid arthritis blood test panels every 2-3 months during active treatment, measuring not just RF but also inflammatory markers (ESR, CRP), liver function (due to DMARD side effects), and complete blood counts to ensure treatment safety and effectiveness.
Lifestyle Modifications to Support Treatment
While medications form the foundation of rheumatoid factor positive RA management, evidence-based lifestyle modifications significantly enhance treatment outcomes and quality of life:
- Anti-inflammatory diet: Mediterranean-style eating patterns rich in omega-3 fatty acids, colorful vegetables, whole grains, and lean proteins reduce systemic inflammation and may modestly lower RF levels
- Regular low-impact exercise: Swimming, cycling, tai chi, and walking maintain joint mobility without excessive stress; aim for 150 minutes weekly
- Stress management: Chronic stress exacerbates autoimmune activity; mindfulness meditation, yoga, and cognitive behavioral therapy reduce inflammation and improve coping
- Quality sleep: 7-9 hours nightly supports immune regulation and reduces inflammatory cytokine production
- Smoking cessation: Cigarette smoking is the strongest environmental risk factor for RF-positive RA and dramatically worsens outcomes—quitting improves treatment response
Maintaining healthy body weight reduces mechanical stress on weight-bearing joints affected by RA. Our BMI Calculator and Macro Calculator help you establish appropriate caloric and nutritional targets that support both weight management and anti-inflammatory eating patterns essential for optimal rheumatoid factor level control.
International Treatment Guidelines
Global rheumatology organizations provide consistent guidance on managing high rheumatoid factor levels, though regional variations reflect healthcare system differences and medication availability. The European Alliance of Associations for Rheumatology (EULAR) emphasizes early aggressive treatment for RF-positive patients, recommending combination DMARD therapy within 3 months of diagnosis when RF exceeds 60 IU/mL.
United States guidelines from the American College of Rheumatology align closely with European protocols but offer more flexibility in biologic selection based on insurance coverage and patient preference. Asia-Pacific treatment recommendations incorporate traditional medicine approaches alongside conventional DMARDs, though evidence supporting complementary therapies remains limited for rheumatoid factor positive disease.
Long-Term Outlook with High RF Levels
High rheumatoid factor levels historically predicted poor prognosis, but modern treatment has transformed outcomes dramatically. Patients with RF exceeding 100 IU/mL who receive aggressive early treatment now achieve remission rates of 30-40% and low disease activity in another 30-40%—outcomes unthinkable two decades ago.
The quality of life for rheumatoid factor positive patients continues improving with each generation of therapeutics. Biologic agents and targeted synthetic DMARDs preserve joint function, prevent disability, and allow most patients to maintain employment and independent living. Early treatment within the first 3-6 months of symptoms—the “window of opportunity”—provides the best chance for excellent long-term outcomes regardless of initial rheumatoid factor levels.
What This Means For You
High rheumatoid factor levels demand action but shouldn’t inspire despair. With proper treatment, monitoring, and lifestyle optimization, most RF-positive patients achieve excellent disease control and maintain quality of life. Partner closely with your rheumatologist, adhere to prescribed medications despite the time required to see benefits (often 3-6 months), and embrace lifestyle modifications that complement medical therapy. Your rheumatoid factor levels may never normalize completely, but they can decrease substantially—and more importantly, you can prevent the joint damage and disability that elevated RF once inevitably predicted.
11 Frequently Asked Questions About Rheumatoid Factor Levels
1. What is a normal rheumatoid factor level?
A normal rheumatoid factor level is below 20 IU/mL in most laboratories, though some use a stricter cutoff of 14 IU/mL. Anything at or below these thresholds is considered negative and normal.
2. What does a rheumatoid factor of 60 mean?
A rheumatoid factor level of 60 IU/mL indicates high positive RF with 97% specificity for rheumatoid arthritis. This level suggests significant autoimmune activity requiring immediate rheumatology evaluation and likely aggressive treatment with DMARDs.
3. Can you have rheumatoid arthritis with negative RF?
Yes, 20-30% of rheumatoid arthritis patients have negative RF results throughout their disease course, called seronegative RA. These patients should be tested for anti-CCP antibodies, which can be positive when RF is negative.
4. What does a rheumatoid factor of 20 mean?
A rheumatoid factor of 20 IU/mL sits at the diagnostic threshold—borderline positive. This level requires clinical correlation with symptoms and additional testing like anti-CCP antibodies. It’s not diagnostic alone but warrants monitoring.
5. What causes high rheumatoid factor besides RA?
High RF can result from Sjögren’s syndrome (50-90% positive), lupus (15-35%), chronic infections like hepatitis C (up to 70%), liver disease, normal aging (10-14% over age 70), and rarely cancers.
6. How long does it take to get RF test results?
Rheumatoid factor test results typically take 24-72 hours from most laboratories. Some facilities offer same-day results for urgent cases. The actual blood draw takes less than 5 minutes.
7. What does a rheumatoid factor of 100 mean?
A rheumatoid factor level of 100 IU/mL indicates very high positive RF associated with severe rheumatoid arthritis, increased risk of joint erosions, extra-articular manifestations, and greater likelihood of requiring biologic medications.
8. Can rheumatoid factor levels go down?
Yes, rheumatoid factor levels decrease in 30-50% of patients with effective DMARD treatment, especially with biologic agents like rituximab. Declining RF levels indicate good treatment response, though levels may never completely normalize.
9. What is the difference between RF and anti-CCP?
RF has 85% specificity for RA and appears in other conditions, while anti-CCP has 95-98% specificity and is highly specific for RA. Anti-CCP can detect RA up to 10 years before symptoms, making it superior for early diagnosis.
10. Do I need to fast for a rheumatoid factor test?
No, you do not need to fast for a rheumatoid factor test. You can eat, drink, and take your regular medications before the blood draw. No special preparation is required.
11. What is considered a high rheumatoid factor level?
Rheumatoid factor levels exceeding 60 IU/mL are considered high positive, with levels above 100 IU/mL classified as very high. Higher RF levels correlate with more severe disease, aggressive joint damage, and worse prognosis without treatment.
About this content
This medical content is prepared through a structured publishing workflow with expert writing, clinical review and editorial quality checks.

Board Certifications: Internal Medicine (1995); Geriatric Medicine (2000); Hospital Medicine (2008) Experience: 30 years | Location: Dubai, UAE Education: MBBS, Cairo University Faculty of Medicine (1992); MD Internal…

Board Certifications: European Registered Toxicologist (2008); Clinical Pharmacology Certification (2010) Experience: 18 years | Location: Madrid, Spain Education: BSc Pharmacy, Complutense University of Madrid (2004); PhD Pharmacology, University…

Dr. Sameer Patel combines clinical expertise with technology innovation. After earning his MD in Internal Medicine, he spent a decade building AI-driven diagnostic systems before founding My Medicine…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.