On This Page – Quick Medical Summary
Anti-CCP Test Positive? What It Really Means for RA
When Maria, a 34-year-old graphic designer, received her anti-CCP test positive result, her rheumatologist explained what thousands of patients need to hear: A positive anti-CCP test means your immune system is producing cyclic citrullinated peptide antibodies that attack joint tissue, indicating a 95-98% likelihood of having rheumatoid arthritis (RA) or developing it in the future. This highly specific biomarker helps doctors diagnose RA earlier and more accurately than older tests, often detecting the disease years before joint pain even begins.
Maria’s journey began six months earlier with unexplained morning stiffness in her hands. After tracking her symptoms with our Symptom Checker, she consulted her doctor who ordered comprehensive blood work. The anti-CCP antibody test would become the decisive factor in her diagnosis.
What Is the Anti-CCP Test?
The anti-CCP test is a blood test that measures levels of anti-cyclic citrullinated peptide antibodies in your bloodstream. According to the National Institutes of Health, these autoantibodies specifically target proteins in joint tissue that have undergone citrullination—a chemical modification that occurs during inflammation. Unlike normal antibodies that protect your body from viruses and bacteria, anti-CCP antibodies mistakenly attack your own healthy tissues, particularly the synovial lining of joints.
Doctors order the CCP antibody test when patients present with joint symptoms like swelling, warmth, or persistent stiffness, especially if these symptoms last more than six weeks. The Centers for Disease Control and Prevention emphasizes that early RA diagnosis and treatment can prevent permanent joint damage. The anti-CCP test has largely replaced rheumatoid factor testing as the primary diagnostic tool because of its superior specificity.
Understanding Your Positive Anti-CCP Test Result
A positive anti-CCP test result typically means your blood contains more than 20 units per milliliter (EU/mL) of these antibodies, though normal ranges may vary slightly between laboratories. Research from the University of Iowa Hospitals & Clinics confirms that anti-CCP positivity indicates greater than 95% specificity for rheumatoid arthritis. This exceptional accuracy means that if you test positive for the anti-CCP antibody, you almost certainly have RA or will develop it.
Key Takeaway: The anti-CCP test is 95-98% specific for rheumatoid arthritis, making it one of the most reliable diagnostic markers in autoimmune disease testing.
What makes the anti-CCP test particularly valuable is its predictive power. Studies published by MedlinePlus, a service of the National Library of Medicine, show that anti-CCP antibodies can appear in your blood up to 10 years before you experience any joint symptoms. For Maria, this early detection meant she could begin disease-modifying antirheumatic drugs (DMARDs) immediately, potentially preventing the joint erosion that affects untreated RA patients. Understanding your anti-CCP levels helps predict disease severity—higher antibody concentrations often correlate with more aggressive rheumatoid arthritis and increased risk of joint damage.
If you’re concerned about autoimmune conditions or have a family history of rheumatoid arthritis, assessing your overall health with tools like our BMI Calculator can help you track risk factors, since maintaining a healthy weight reduces inflammatory stress on joints.
Medical Disclaimer: This article is for educational purposes and does not constitute medical advice. Always consult a board-certified rheumatologist for diagnosis and treatment of rheumatoid arthritis. Information current as of December 2025.
Anti-CCP Test Results: What Your Numbers Mean
Understanding your anti-CCP test results requires knowing what the numbers represent and how they translate to rheumatoid arthritis risk. Most laboratories use a threshold of 20 units per milliliter (U/mL or EU/mL) to distinguish negative from positive results, though this can vary slightly between testing facilities.
Anti-CCP Normal Range and Result Categories
Your anti-CCP antibody levels fall into specific categories that help predict both the likelihood of RA and potential disease severity. Here’s what different anti-CCP test results mean for your diagnosis:
Research from the National Institutes of Health demonstrates that anti-CCP positivity correlates significantly with more severe joint damage at diagnosis, making higher antibody levels an important prognostic indicator. If you’re tracking multiple health markers for autoimmune conditions, our Genetic Risk Assessment Tool can help you understand hereditary factors that may influence your RA risk.
Anti-CCP vs Rheumatoid Factor: The Key Differences
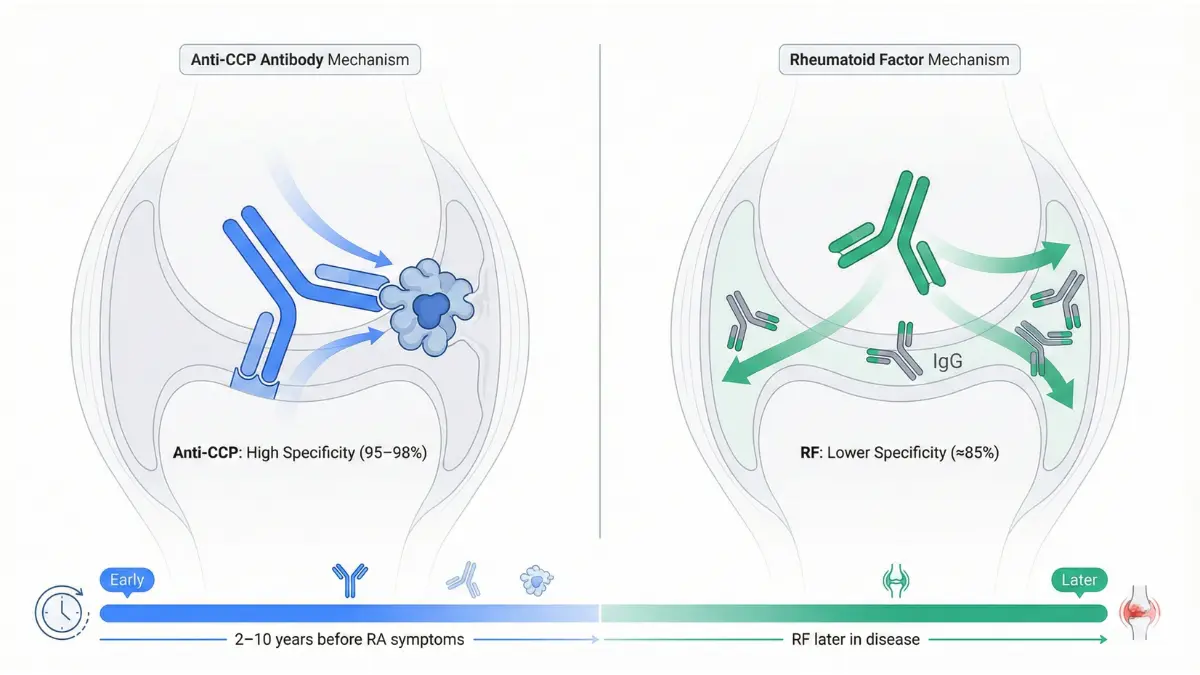
For decades, doctors relied on rheumatoid factor testing for RA diagnosis, but the anti-CCP test has proven superior in multiple ways. According to studies published in the British Journal of Pain, anti-CCP antibodies demonstrate 95% specificity compared to rheumatoid factor’s 85% specificity. Here’s how these two rheumatoid arthritis tests compare:
The anti-CCP test is approximately 25% more specific than rheumatoid factor for RA diagnosis, making it the preferred first-line serological marker according to Hospital for Special Surgery rheumatology experts.
When both anti-CCP and RF tests are positive together, the specificity for rheumatoid arthritis diagnosis increases to 98%. However, anti-CCP antibody testing alone provides more reliable diagnostic information than RF testing, particularly for predicting erosive joint disease.
What If You’re Anti-CCP Negative But Have RA Symptoms?
Approximately 20% of rheumatoid arthritis patients are seronegative, meaning both their RF and anti-CCP test results remain negative despite having active disease. According to University of Central Florida Health, seronegative RA diagnosis relies heavily on clinical examination, imaging studies like X-rays and MRI, and elevated inflammatory markers such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR).
The National Institutes of Health explains that seronegative rheumatoid arthritis patients may actually require more severe clinical and inflammatory symptoms to meet the 2010 ACR/EULAR diagnostic criteria, since they cannot accumulate points from serological markers. If you’re experiencing persistent joint stiffness, swelling in multiple joints symmetrically, or morning stiffness lasting more than 30 minutes, use our Symptom Checker to document your symptoms before consulting a rheumatologist.
Key Insight: A negative anti-CCP test does not rule out rheumatoid arthritis. Some patients develop positive results later in their disease course, while others remain persistently seronegative throughout. The diagnosis ultimately depends on combining laboratory results with physical examination findings, imaging evidence, and symptom patterns.
For seronegative patients, maintaining overall health becomes particularly important. Tools like our BMR Calculator can help you optimize metabolic health, which plays a role in managing inflammatory conditions.
Anti-CCP Test Procedure, Cost & What to Expect
Getting the Anti-CCP Test: Procedure and Preparation
The anti-CCP test procedure is straightforward and requires minimal preparation, making it accessible for patients with joint concerns. Understanding what happens before, during, and after testing helps reduce anxiety and ensures accurate results.
Anti-CCP Test Procedure Step-by-Step
Your journey to getting an anti-CCP antibody test typically follows these stages:
- Doctor’s Referral and Clinical Assessment – Your physician orders the CCP blood test based on symptoms like persistent joint swelling, morning stiffness lasting over 30 minutes, or family history of rheumatoid arthritis. According to MedlinePlus, a service of the National Library of Medicine, doctors most commonly order this test when RA is suspected but diagnosis needs confirmation.
- No Fasting Required – Unlike some metabolic blood tests, the anti-CCP test requires no fasting or dietary restrictions. You can eat and drink normally before your appointment, though staying hydrated makes the blood draw easier. If you track your nutritional intake for overall inflammatory health, our Macro Calculator can help optimize your anti-inflammatory diet.
- Simple Blood Draw from Arm Vein – The actual CCP antibody test procedure takes only 5-10 minutes. A healthcare professional uses a small needle to collect blood from a vein in your arm, similar to routine blood work. The FDA-approved testing methodology analyzes your serum for the presence of anti-cyclic citrullinated peptide IgG antibodies.
- Lab Processing Timeline – After collection, your blood sample undergoes chemiluminescent immunoassay testing. Most laboratories return anti-CCP test results within 24 to 72 hours, though some facilities may take up to one week depending on whether testing is performed on-site or sent to reference laboratories.
- Results Delivery and Consultation – Your doctor will schedule a follow-up appointment to discuss your anti-CCP levels and what they mean for your diagnosis. Research published in the National Institutes of Health journals confirms that anti-CCP detection provides higher diagnostic specificity than rheumatoid factor testing.

Anti-CCP Test Cost and Insurance Coverage
Understanding the financial aspects of RA testing helps you plan accordingly. The anti-CCP test cost varies significantly based on location, insurance status, and testing facility:
United States Pricing:
- With insurance: $20-$60 copay after meeting deductible
- Without insurance: $100-$250 out-of-pocket
- Academic medical centers: $31.50-$45 (reference pricing from University of Nevada, Las Vegas contract rates)
International Cost Comparison:
- India: ₹779-₹1,479 ($10-$18 USD)
- United Kingdom: £40-£80 (NHS-covered when medically necessary)
- Australia: AUD $50-$120 (Medicare rebate available)
- Canada: CAD $60-$100 (provincial health coverage varies)
Medicare and Insurance Coverage:
According to Medicare.gov, Medicare Part B covers medically necessary clinical diagnostic laboratory tests, including the anti-CCP test, when ordered by your physician for RA diagnosis. After meeting your annual Part B deductible, you typically pay 20% coinsurance for laboratory services.
Most private insurance plans cover the CCP test for RA when your doctor documents clinical indications such as joint symptoms, positive rheumatoid factor, or family history. To verify coverage, contact your insurance provider before testing or ask your rheumatology practice to submit a pre-authorization request.
Preparing for Your CCP Blood Test
Preparation for the anti-CCP antibody test is minimal, but these steps ensure smooth testing:
- Medication Disclosure – Inform your healthcare provider about all medications, vitamins, and supplements you’re taking. While most medications don’t interfere with anti-CCP results, your doctor needs complete information for accurate interpretation. Use our Pill Identifier if you’re unsure about any medications you’re taking.
- Continue Current Medications – According to MedlinePlus guidelines, you should continue your regular medications unless specifically instructed otherwise by your physician. Stopping RA medications before testing doesn’t affect anti-CCP antibody levels.
- Hydration Matters – Drinking adequate water before your blood draw makes veins more accessible and the procedure easier. Our Water Intake Calculator can help you determine your optimal daily hydration.
- What to Bring – Bring your insurance card, photo identification, and a list of current symptoms with dates to help your doctor interpret results in clinical context.
Testing Risks are Minimal: The National Institutes of Health confirms that the anti-CCP test carries virtually no risk beyond slight pain or bruising at the needle insertion site, which resolves quickly.
What Positive Anti-CCP Means for Your RA Diagnosis & Future
If You Test Anti-CCP Positive: What Happens Next?
Receiving a positive anti-CCP test result marks the beginning of your diagnostic journey, not the end. Your rheumatologist will combine this blood marker with additional clinical assessments to confirm rheumatoid arthritis and develop a personalized treatment strategy.
Understanding Your Rheumatoid Arthritis Diagnosis
According to the National Center for Biotechnology Information, the 2010 ACR/EULAR (American College of Rheumatology/European League Against Rheumatism) classification criteria use a point-based system that incorporates anti-CCP test results, joint involvement, symptom duration, and inflammatory markers. Patients scoring 6 or more points out of 10 are classified as having definite rheumatoid arthritis.
Your doctor will likely order complementary tests to build a complete diagnostic picture. These include rheumatoid factor testing, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and imaging studies. Research from Stanford University Medical Center demonstrates that combining multiple autoantibodies improves diagnostic accuracy, particularly when detecting disease in its earliest stages.
Dr. V. Michael Holers, Director of the Autoimmune Disease Prevention Center at the University of Colorado Anschutz Medical Campus, explains that positive anti-CCP antibodies signal the immune system has already begun targeting joint tissue, even if inflammation isn’t yet visible. International consensus from European rheumatology experts confirms this preclinical phase offers the best opportunity for intervention.
Anti-CCP Antibody Positive: Predicting Disease Severity
The level of your anti-CCP antibodies doesn’t just confirm diagnosis—it predicts how aggressive your rheumatoid arthritis may become. A comprehensive meta-analysis published by the National Institutes of Health found that anti-CCP positivity increases the odds of developing joint erosions by 4.85 times compared to seronegative patients.
Higher anti-CCP levels correlate with more severe outcomes:
- Radiological Damage: Studies from NIH research archives demonstrate that anti-CCP positive patients showed significantly higher Larsen scores (a measure of joint destruction) at baseline and throughout follow-up periods. Patients with strongly positive results (>60 EU/mL) had mean Larsen scores of 28 after six years compared to 19 in anti-CCP negative patients.
- Erosive Disease Progression: Research published in NIH medical journals found that baseline anti-CCP positivity predicted erosive disease development with an odds ratio of 2.72. The presence of these antibodies was associated with greater extent of joint deformity and lower odds of achieving remission.
- Structural Joint Damage: A study from Taiwan medical research confirmed that higher anti-CCP antibody titers correlate with more severe synovitis on ultrasound and more frequent bone erosions. This correlation remained significant even when controlling for other inflammatory markers.
Patient Story: Robert, a 42-year-old teacher, tested positive for anti-CCP with a level of 68 EU/mL. His rheumatologist immediately started him on methotrexate, a disease-modifying antirheumatic drug (DMARD). Within six months, Robert’s joint swelling decreased dramatically, and follow-up imaging showed no new erosions. Early aggressive treatment based on his high anti-CCP levels likely prevented permanent disability. If you’re managing weight as part of your overall inflammatory health strategy, our BMI Calculator can help track this important risk factor.
Early Detection: When Anti-CCP Appears Before Symptoms
One of the most remarkable features of the anti-CCP test is its ability to detect rheumatoid arthritis years before joint pain begins. Research from the University of Colorado School of Medicine shows that anti-CCP antibodies appear in the blood an average of 3 to 5 years before the first synovitis symptoms develop.
Even more striking, studies documented in University of North Carolina research detected anti-CCP antibodies up to 14 years prior to RA onset, with gradually increasing prevalence and levels as diagnosis approached. During this preclinical phase, Stanford Medicine research indicates that cytokines, chemokines, and inflammatory markers like CRP also begin elevating, creating a detectable immunological signature of developing disease.
This window of opportunity is crucial. According to Hospital for Special Surgery experts, RA should be treated within 3 to 6 months after symptom onset, before irreversible joint damage occurs. Patients with shorter disease duration show significantly better treatment responses than long-term sufferers, supporting the concept of early intervention.
For asymptomatic individuals with positive anti-CCP antibodies, monitoring protocols may include:
- Regular rheumatology consultations every 3-6 months
- Periodic inflammatory marker checks (CRP, ESR)
- Joint ultrasound to detect subclinical synovitis
- Lifestyle modifications to reduce inflammatory triggers
- Consideration of preventive DMARD therapy in high-risk cases
If you’re experiencing unexplained joint symptoms, our Symptom Checker can help you document patterns before your rheumatology appointment.
Rheumatoid Arthritis Test: Beyond Anti-CCP
While the anti-CCP antibody test provides exceptional diagnostic specificity, comprehensive RA diagnosis requires multiple assessments. According to NIH clinical guidelines, no single biomarker captures all aspects of rheumatoid arthritis disease activity.
Complementary blood tests include:
- Rheumatoid Factor (RF) – Although less specific than anti-CCP (85% vs. 95-97%), RF testing remains valuable. When both tests are positive together, RA likelihood exceeds 98%. Research shows anti-CCP has greater predictive power for disease severity compared to rheumatoid factor.
- C-Reactive Protein (CRP) – This acute phase reactant rises quickly in response to inflammation. Studies from NIH medical archives confirm CRP levels correlate with active synovitis on ultrasound. However, research indicates normal CRP doesn’t exclude active disease in 20-40% of RA patients.
- Erythrocyte Sedimentation Rate (ESR) – ESR measures how quickly red blood cells settle, indicating inflammation levels. While useful, it’s influenced by factors unrelated to RA like age, anemia, and kidney function.
- Complete Blood Count – Anemia of chronic disease is common in active RA. Recent studies suggest neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio may serve as emerging inflammatory markers.
Imaging Studies for Joint Assessment:
- X-rays – Detect established erosions and joint space narrowing
- Ultrasound – The NIH validates ultrasound as highly sensitive for detecting subclinical synovitis and early erosions before they appear on X-ray
- MRI – Identifies bone marrow edema and early inflammatory changes
- Power Doppler Ultrasound – Visualizes active blood flow in inflamed joints
For patients managing chronic conditions, comprehensive health tracking extends beyond joint health. Our Health Tips section offers evidence-based guidance on anti-inflammatory lifestyles that complement medical treatment.
Evidence Strength: The predictive value of anti-CCP for joint erosions represents Level 1 evidence, supported by multiple systematic reviews and meta-analyses published in peer-reviewed medical journals.
False Positives, Special Cases & Advanced Insights
Beyond the Basics: False Positives and Complex Cases
While the anti-CCP test demonstrates exceptional specificity for rheumatoid arthritis, understanding rare false positives and special clinical scenarios ensures accurate interpretation of your results.
Can Anti-CCP Be a False Positive?
False-positive anti-CCP test results occur in fewer than 2-5% of cases, making this marker remarkably reliable. However, research published by the National Institutes of Health identified anti-streptavidin IgG antibodies as a rare but important cause of false-positive anti-CCP results in certain immunoassay platforms. These interfering antibodies can trigger erroneous readings in patients who don’t have rheumatoid arthritis.
When laboratories suspect a false positive, they typically:
- Retest using a different anti-CCP assay platform
- Confirm results with additional RA markers like rheumatoid factor
- Correlate findings with clinical symptoms and physical examination
- Monitor patients over time for development of joint symptoms
According to University of Rochester Medical Center clinical guidelines, testing positive for anti-CCP antibodies alongside symptoms strongly indicates RA, but a positive result might occasionally occur in other autoimmune conditions. If you’re experiencing confusing symptoms across multiple body systems, our Symptom Checker can help track patterns before discussing with your physician.
Interestingly, studies show that immunological factors including RF and anti-CCP antibodies may influence the screening of other conditions, occasionally producing unexpected cross-reactivity in certain laboratory tests.
Anti-CCP in Other Conditions
While anti-CCP antibodies are highly specific for rheumatoid arthritis, researchers have documented their presence in select non-RA conditions. A landmark study from the National Institutes of Health described patients with lung disease and anti-CCP positivity but no existing RA or connective tissue disease. These patients showed distinct radiographic phenotypes including isolated airways disease (54%), isolated interstitial lung disease (14%), and mixed patterns.
Research from the University of Colorado Anschutz Medical Campus explains that anti-CCP antibodies may develop in lung tissue before joints become affected, particularly in cigarette smokers. A NIH investigation confirmed that smoking increases the risk for anti-CCP antibodies only in patients with specific genetic markers (shared epitope positive).
Other conditions occasionally showing anti-CCP positivity include:
- Systemic Lupus Erythematosus (SLE) – Rare overlap, usually low titers
- Sjögren’s Syndrome – Occasional detection in secondary forms
- Chronic Lung Disease – May precede RA development
- Polymyalgia Rheumatica (PMR) – Studies show elderly PMR patients typically remain anti-CCP negative, helping distinguish from elderly-onset RA
According to NIH research archives, anti-CCP antibodies are rarely detectable in non-rheumatoid diseases, and when present, usually appear at low titers below 40 EU/mL. For comprehensive health risk assessment beyond rheumatoid arthritis, our Genetic Risk Assessment Tool analyzes hereditary factors for multiple autoimmune conditions.
Monitoring Anti-CCP Levels Over Time
The question of whether anti-CCP levels should be monitored during rheumatoid arthritis treatment remains debated. Research from the National Institutes of Health demonstrated that anti-CCP levels may change during RA course, regardless of the biological drug used. After one year of anti-TNF therapy, patients showed significant reduction in anti-CCP levels, while rituximab and tocilizumab also decreased antibody concentrations.
However, a 2023 study published in NIH medical journals concluded that anti-CCP is a more stable index compared to rheumatoid factor; its level changes only slightly during therapy and does not require routine monitoring. The concentration of anti-CCP in patients who responded to treatment remained high throughout rituximab therapy, with only 7-15% achieving negative seroconversion.
Current clinical consensus suggests:
- Anti-CCP levels at diagnosis help predict severity, not monitor treatment response
- Clinical symptoms, inflammatory markers (CRP/ESR), and imaging better track disease activity
- Repeat anti-CCP testing is generally not cost-effective for routine monitoring
For patients managing chronic inflammatory conditions, tracking overall wellness metrics remains important. Our BMI Calculator helps monitor weight, since obesity increases inflammatory burden in RA patients.
Latest Research & Future of Anti-CCP Testing (2024-2025)
Cutting-Edge Developments:
Groundbreaking research published in August 2025 by the National Institutes of Health explored next-generation antibody detection methods using advanced electrochemical biosensors and artificial intelligence integration. These novel platforms promise improved sensitivity for detecting anti-CCP antibodies at even lower concentrations during preclinical disease phases.
A June 2025 NIH review outlined current applications of artificial intelligence for rheumatoid arthritis diagnosis, management, and prognosis. Machine learning algorithms combining anti-CCP levels with genetic markers, imaging findings, and cytokine profiles may soon enable personalized risk stratification and treatment selection.
Research from Stanford Medicine in 2025 confirmed that anti-CCP positivity correlates with higher cardiovascular disease risk in RA patients, independent of traditional risk factors. A May 2025 NIH publication reinforced anti-CCP’s role as both a diagnostic and prognostic biomarker, with higher titers predicting more severe joint damage and extra-articular manifestations.
Regional Testing Variations:
European rheumatology guidelines increasingly emphasize anti-CCP testing in the “window of opportunity”—the first 12 weeks of symptoms when aggressive treatment prevents irreversible damage. Asian medical centers have adopted combined anti-CCP and anti-MCV (mutated citrullinated vimentin) testing protocols for enhanced sensitivity in seronegative patients.
Action Plan & Living with Anti-CCP Positivity
Your Action Plan After a Positive Anti-CCP Test
Receiving a positive anti-CCP test result requires prompt action to preserve joint health and prevent irreversible damage. Research from Hospital for Special Surgery emphasizes that early treatment within 3 to 6 months of disease onset significantly improves long-term outcomes.
Immediate Next Steps
- Schedule Rheumatologist Consultation Within 2-4 Weeks – Early DMARD therapy can slow RA progression and prevent disability according to UCSF Medical Center clinical guidelines. Don’t delay this critical appointment.
- Gather Complete Medical History – Document family history of autoimmune diseases, previous joint symptoms, and current medications for your rheumatology visit.
- Track Symptoms Systematically – Use our Symptom Checker to log joint pain patterns, morning stiffness duration, and swelling locations with timestamps.
- Request Comprehensive Test Results – Obtain copies of your anti-CCP test results, rheumatoid factor, inflammatory markers (CRP/ESR), and any imaging studies for your records.
- Verify Insurance Coverage – Contact your insurance provider to confirm coverage for rheumatology visits, RA blood tests, and potential DMARD medications.
Critical Fact: Early treatment within 6 months improves long-term outcomes by approximately 40% compared to delayed intervention.
Lifestyle Modifications to Support Joint Health
A groundbreaking 2023 National Institutes of Health study demonstrated that a multidisciplinary lifestyle program combining whole-food plant-based diet, physical activity, and stress management significantly improved disease activity scores (DAS28) in rheumatoid arthritis patients.
Evidence-Based Lifestyle Strategies:
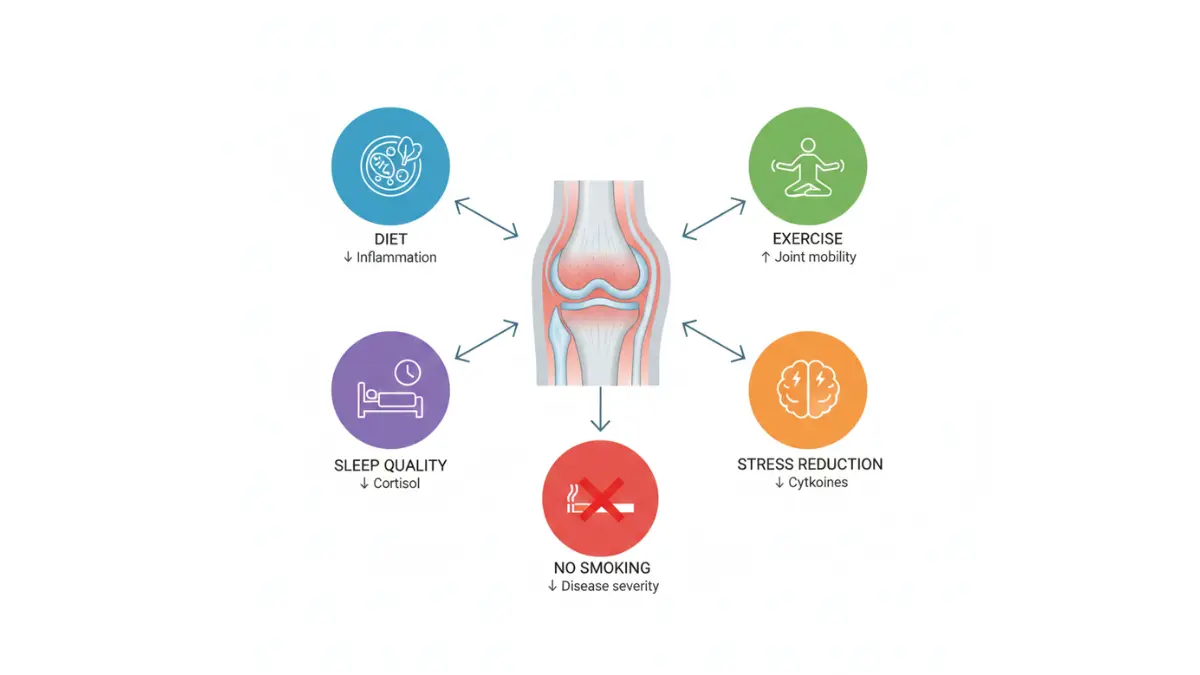
- Anti-Inflammatory Diet – Research published in NIH medical journals shows Mediterranean diets reduce inflammatory cytokines in RA patients. Focus on fish oil/omega-3, probiotics, vitamin D, and antioxidants to improve pain and functional ability. Our Macro Calculator helps balance nutrients for optimal anti-inflammatory nutrition.
- Regular Physical Activity – A September 2025 NIH publication confirmed that physical activity reduces disease activity and inflammation while improving RA symptoms. Aim for 150 minutes weekly of moderate-intensity exercise plus muscle-strengthening activities twice weekly.
- Stress Management – Chronic stress elevates cortisol, which exacerbates inflammation. Studies validate psychoeducation and stress reduction techniques as effective RA management tools.
- Quality Sleep – Adequate sleep (7-9 hours) supports immune regulation and reduces inflammatory responses. Use our Sleep Calculator to optimize your sleep schedule for maximum recovery.
- Smoking Cessation – According to NIH research, smoking dramatically worsens RA outcomes and should be discontinued immediately.
Questions to Ask Your Doctor
Treatment Options: What disease-modifying antirheumatic drugs (DMARDs) do you recommend as first-line therapy for my anti-CCP antibody positive status?
Monitoring Plan: How frequently will we assess disease progression through clinical exams, inflammatory markers, and imaging?
Prognosis: Given my specific anti-CCP level and clinical presentation, what’s my outlook for achieving remission or low disease activity?
Clinical Trials: Are there research opportunities I qualify for that might provide access to emerging RA therapies?
Lifestyle Impact: Which daily activities should I modify to protect my joints while maintaining quality of life?
Finding Support and Resources
The Arthritis Foundation provides comprehensive patient education, support groups, and advocacy for individuals with rheumatoid arthritis diagnosis. Their trained Helpline team answers questions about insurance enrollment, Medicare changes, treatment options, and navigating medical systems.
Veterans can access specialized resources through the VA-Arthritis Foundation partnership, which offers health education, exercise programs, and motivational strategies tailored to managing arthritis.
Living with a positive anti-CCP test result doesn’t mean accepting disability. With early aggressive treatment, evidence-based lifestyle modifications, and strong medical support, many patients achieve remission or maintain excellent quality of life. Your proactive response to this diagnosis today shapes your joint health for decades to come.
Medical Disclaimer: This article is for educational purposes and does not constitute medical advice. Always consult a board-certified rheumatologist for diagnosis and treatment of rheumatoid arthritis. Information current as of December 2025.
11 Frequently Asked Questions About Anti-CCP Test
1. What is an anti-CCP test?
The anti-CCP test is a blood test that measures antibodies (anti-cyclic citrullinated peptide) that attack joint tissue in rheumatoid arthritis. It’s one of the most specific and accurate diagnostic markers for RA, detecting the disease with 95-98% specificity.
2. What does a positive anti-CCP test mean?
A positive result (above 20 EU/mL) indicates a 95-98% likelihood you have or will develop rheumatoid arthritis. Higher levels often predict more aggressive disease and greater risk of joint damage.
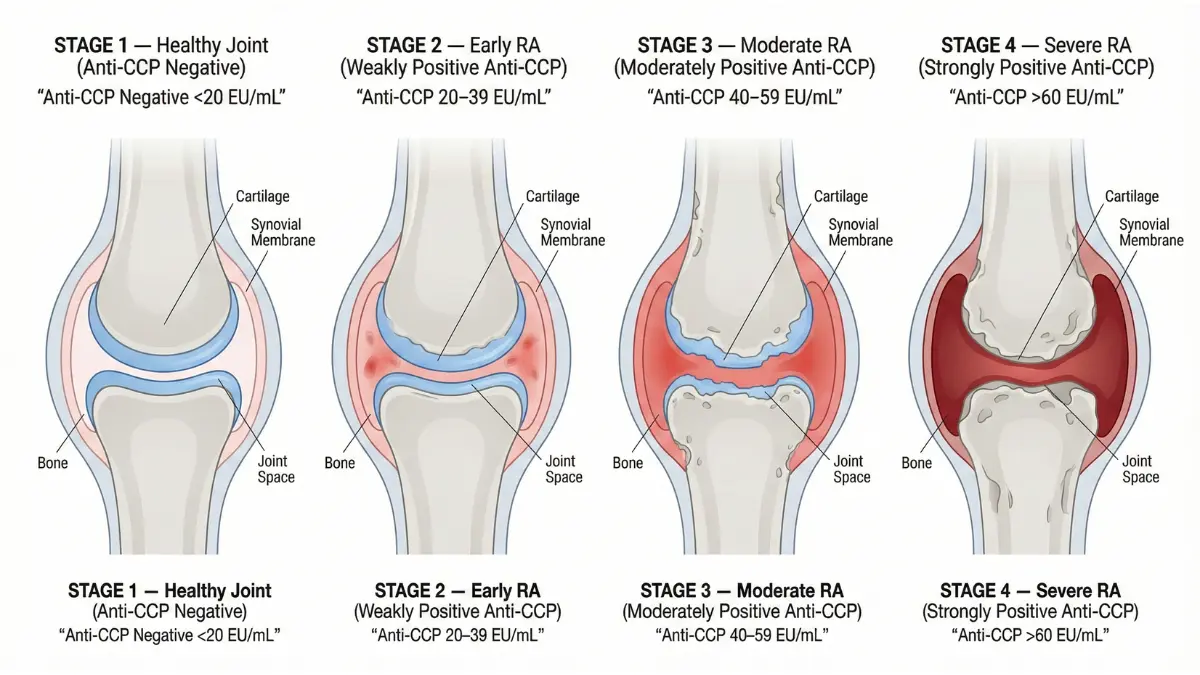
3. What is the normal range for anti-CCP?
Normal or negative anti-CCP levels are typically below 20 units per milliliter (EU/mL). Results between 20-39 EU/mL are weakly positive, 40-59 moderately positive, and above 60 strongly positive.
4. How much does the anti-CCP test cost?
In the United States, costs range from $20-$60 with insurance or $100-$250 without insurance. Medicare Part B typically covers the test when medically necessary after you meet your deductible.
5. Do I need to fast before an anti-CCP test?
No fasting is required for the anti-CCP antibody test. You can eat and drink normally before your blood draw, though staying hydrated helps make the procedure easier.
6. What’s the difference between anti-CCP and rheumatoid factor?
Anti-CCP is more specific (95-97%) than rheumatoid factor (85-90%) for diagnosing RA. Anti-CCP also appears earlier—sometimes years before symptoms—and better predicts disease severity and joint damage.
7. Can I have rheumatoid arthritis with a negative anti-CCP test?
Yes, approximately 20% of RA patients are seronegative (negative anti-CCP and RF). Diagnosis in these cases relies on clinical examination, imaging studies, and elevated inflammatory markers like CRP and ESR.
8. How long does it take to get anti-CCP test results?
Most laboratories return anti-CCP results within 24 to 72 hours. Some facilities may take up to one week depending on whether testing is performed on-site or sent to reference laboratories.
9. Is the anti-CCP test painful?
The test involves a simple blood draw from your arm vein, causing only brief discomfort similar to routine blood work. Risks are minimal—typically just slight pain or bruising at the needle site.
10. When should I get tested for anti-CCP?
Your doctor may order the test if you have persistent joint swelling, morning stiffness lasting over 30 minutes, family history of RA, or positive rheumatoid factor. Early testing enables prompt treatment before permanent joint damage occurs.
11. Do anti-CCP levels change with treatment?
Anti-CCP antibodies generally remain positive throughout the disease course, though levels may decrease slightly with some medications like rituximab or anti-TNF therapy. However, anti-CCP is not routinely monitored during treatment since clinical symptoms and inflammatory markers better track disease activity.
About this content
How this article was put together: researched from recognised health sources, drafted with the help of AI tools, and edited by hand, with sources linked throughout.

Sameer Patel is the founder and editor of My Medicine Advisor. He is not a doctor or medical professional — before starting this site he worked in banking,…
Medical disclaimer
The content on MyMedicineAdvisor is provided for general informational and educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Health information on this website should not be used to diagnose, treat, cure, or prevent any condition without guidance from a qualified healthcare professional. Always seek the advice of your doctor, physician, or another licensed healthcare provider with any questions you may have regarding a medical condition, symptoms, medications, or treatment decisions.